

Abstract
Environmental modifications have been shown to increase short-term stair use, longer-term success is unclear. This study assessed the 2-year effectiveness of an environmental intervention promoting worksite stair use. We assessed stair use at work by means of self-reports and infrared beam counters (which send a safe and invisible beam of infrared light from one side of a stairwell to a reflector on the other side; when an individual uses the stairs, the infrared beam is disrupted and an instance of stair use is recorded) at six worksites (three intervention, three control) in a group randomized, controlled worksite weight-gain prevention trial in Minneapolis/St. Paul, MN. Intervention modifications were signs encouraging stair use, music, and art posters in stairwells. We collected data before environmental modifications (2006–2007) and at the end of the 2-year intervention (2008–2009). The intervention had a significant positive effect on stair use measured both objectively and via self-report, with greatest increases reported among those participants who used the stairs least at baseline. Following 2-years of continuously-maintained stairwell modifications, increases in both objectively-measured and self-reported stair use were significantly larger at intervention than control worksites. Study findings suggest that the positive impact of environmental modifications on stair use persist over a longer time period than has been previously demonstrated. Results also indicate that infrequent stair users may be most amenable to the behavior changes encouraged by these environmental enhancements.
Keywords: Stair use, Worksite, Intervention, Environmental modification
Introduction
Over two-thirds of American adults are overweight or obese (Flegal, Carroll, Ogden, & Curtin, 2010), and insufficient physical activity is a key contributor to this energy surplus (Lee, Djousse, Sesso, Wang, & Buring, 2010; Troiano et al., 2008). Lack of time to engage in structured exercise is one of the most commonly cited reasons that individuals provide for leading a sedentary lifestyle (Brownson, Baker, Housemann, Brennan, & Bacak, 2001). However, because even brief bouts of physical activity can benefit health and contribute to the balancing of energy intake and expenditure (Dunn, Andersen, & Jakicic, 1998; Haskell et al., 2007), there has been a recent emphasis on incorporating more physical exertion into the many necessary activities of daily life (Dunn et al., 1998).
As most American adults are employed outside of the home (Porter, 2006), one of the necessary activities of daily life for many adults involves moving between floors at the workplace. Workplace stairwells thus offer an accessible setting for individuals to engage in daily physical activity. However, when stairwells and low-exertion forms of between-floor transportation (e.g., elevators, escalators) are available for employee use in multi-story workplaces, the low-exertion options tend to be used more often (Boutelle, Jeffery, Murray, & Schmitz, 2001; Kerr, Eves, & Carroll, 2001c; Webb & Eves, 2007). Because replacing elevator or escalator use with stair use enables individuals to engage in physical activity while accomplishing something they may need to do anyway (i.e., move from one level of a building to another), those individuals who were previously unaware or not focused on the health benefits of brief bouts of physical activity might increase their activity level if these benefits were made known or salient. Indeed, considerable prior research has demonstrated that rates of stair use increase when simple signage is posted near a stairwell encouraging stair use and/or describing the health benefits of taking the stairs (Andersen, Franckowiak, Snyder, Bartlett, & Fontaine, 1998; Blamey, Mutrie, & Aitchison, 1995; Boutelle et al., 2001; Brownell, Stunkard, & Albaum, 1980; Bungum, Meacham, & Truax, 2007; Coleman & Gonzalez, 2001; Engbers, van Poppel, & van Mechelen, 2007; Eves et al., 2008; Ford & Torok, 2008; Kerr, Eves, & Carroll, 2000, 2001a, b, c; Kerr, Yore, Ham, & Dietz, 2004; Marshall, Bauman, Patch, Wilson, & Chen, 2002; Webb & Eves, 2007). This body of research has also suggested that enhancing the attractiveness of stairwells, by such means as music or artwork, can increase rates of stair use.
Although these prior research studies have demonstrated that a range of inexpensive environmental modifications can produce significant short-term increases in stair use, it is not known whether these modifications are effective over longer periods (Kerr et al., 2001b; Matson-Koffman, Brownstein, Neiner, & Greaney, 2005). The present research investigates long-term change in stair use in the context of a 2-year worksite-randomized weight loss trial. We collected both objective (via infrared beam counters) and self-report stair use data at baseline and at 2-year follow-up. We hypothesized that stairwell modifications would result in increased stair use at intervention worksites compared with control worksites. In addition, we hypothesized that a subgroup of study participants would show greater increases in stair use, specifically those who were not using the stairs or using the stairs infrequently at baseline, compared with those who already used the stairs frequently at baseline. We based this latter hypothesis both on prior research findings (Kerr et al., 2000) and on the expectation that employees at a worksite are likely to make a relatively consistent number of daily trips from one floor of their building to another and that some individuals would already be making all or most of these trips via stairs at baseline; thus, these individuals would be unlikely to significantly increase their stair use even if signage, artwork and music made the stairwells more appealing.
Method
Study Design
We collected data as part of a group-randomized trial of six worksites in the Minneapolis/St. Paul, Minnesota metropolitan area. We obtained approval for all study procedures from the University of Minnesota Institutional Review Board. All worksites had at least two floors to ensure the presence of one or more stairwells. The mean number of stairwells per site was 3.5 (range 2–6), and the mean number of stories per building was 5.8 (range 2–11). In addition, we selected recruited sites based on the following criteria: size (250–1,000 employees), location (within the Twin Cities metropolitan area), minimal seasonal fluctuation of employees, projected stability of location and workforce over the course of the study period, and willingness to provide employees work contact information.
Participants
Employees at the six recruited worksites (three intervention and three control) were eligible to participate in the larger trial if they were employed at least 50 % time on-site during a daytime shift. There were 1,747 total participants enrolled in the study across the six worksites. Of these participants, 1,356 provided self-report data on their stair use at both baseline and 2-year follow-up. We display demographic characteristics of these 1,356 participants in Table 1 and the individual participant flow diagram in Fig. 1.
Table 1.
Baseline descriptive characteristics of worksites (N = 6) and participants (N = 1,356)
| Variable | All participants | Worksite 1 | Worksite 2 | Worksite 3 | Worksite 4 | Worksite 5 | Worksite 6 |
|---|---|---|---|---|---|---|---|
| Study condition | – | Control | Interv. | Interv. | Control | Control | Interv. |
| Floors in building | – | 5 | 5 | 5 | 3 | 11 | 7 |
| Stairwells with associated elevator (proportion) | – | 0a | 0.6 | 0.5 | 0.5 | 1.0 | 0.25 |
| Stairwells in building | – | 6 | 5 | 2 | 2 | 2 | 4 |
| Employees in building | – | 430 | 284 | 383 | 639 | 522 | 442 |
| Baseline stair use [objective counts per site; mean (SD)] | 1,704.1 (1,585.4) | 2,119.0 (661.0) | 4,672.4 (1,425.4) | 1,151.4 (186.7) | 795.0 (116.7) | 216.6 (44.7) | 1,270.7 (221.3) |
| Baseline stair use [self-report flights/day; mean (SD)] | 8.1 (8.9) | 12.0 (9.7) | 10.5 (9.1) | 11.0 (9.0) | 5.9 (8.9) | 2.3 (4.1) | 10.8 (8.0) |
| Total study participants (n) | 1,747 | 251 | 168 | 259 | 367 | 377 | 325 |
| Participants with baseline and follow-up self-reported stair use data (n) | 1,356 | 195 | 124 | 204 | 262 | 306 | 265 |
| Age (years) | |||||||
| Mean (SD) | 43.5 (10.4) | 46.5 (10.7) | 46.4 (10.5) | 44.4 (9.7) | 40.2 (10.1) | 45.3 (9.6) | 40.7 (10.5) |
| BMI (kg/m2) | |||||||
| Mean (SD) | 28.4 (6.3) | 28.4 (6.4) | 29.0 (5.9) | 29.3 (6.6) | 27.5 (5.6) | 28.7 (6.1) | 28.2 (7.0) |
| Sex (n (%)) | |||||||
| Female | 865 (63.8) | 114 (58.5) | 78 (62.9) | 121 (59.3) | 179 (68.3) | 181 (59.2) | 192 (72.5) |
| Male | 491 (36.2) | 81 (41.5) | 46 (37.1) | 83 (40.7) | 83 (31.7) | 125 (40.8) | 73 (27.5) |
| Race/ethnicity [n (%)] | |||||||
| White, non-Hispanic | 1,184 (88.4) | 152 (77.9) | 103 (83.1) | 189 (92.6) | 231 (88.1) | 277 (90.5) | 232 (87.5) |
| Black, non-Hispanic | 49 (3.6) | 16 (8.2) | 5 (4.0) | 4 (2.0) | 8 (3.1) | 8 (2.6) | 8 (3.0) |
| Other non-Hispanic | 79 (5.8) | 22 (11.3) | 10 (8.1) | 8 (3.9) | 11 (4.2) | 13 (4.2) | 15 (5.7) |
| Hispanic | 27 (2.0) | 4 (2.1) | 3 (2.4) | 1 (0.5) | 9 (3.4) | 3 (1.0) | 7 (2.6) |
| Educational attainment [n (%)] | |||||||
| High school or less | 136 (10.0) | 10 (5.1) | 1 (0.8) | 45 (22.1) | 56 (21.4) | 14 (4.6) | 10 (3.8) |
| Some (<4 year) college | 395 (29.1) | 59 (30.3) | 41 (33.1) | 70 (34.3) | 95 (36.3) | 71 (23.2) | 59 (22.3) |
| 4 year college degree | 508 (37.5) | 46 (23.6) | 33 (26.6) | 69 (33.8) | 86 (32.8) | 137 (44.8) | 137 (51.7) |
| Graduate degree | 316 (23.3) | 80 (41.0) | 48 (38.7) | 20 (9.8) | 25 (9.5) | 84 (27.5) | 59 (22.3) |
| Marital status [n (%)] | |||||||
| Married | 851 (62.8) | 109 (55.9) | 84 (67.7) | 145 (71.1) | 166 (63.4) | 203 (66.3) | 144 (54.3) |
| Cohabitating | 90 (6.6) | 17 (8.7) | 9 (7.3) | 7 (3.4) | 17 (6.5) | 18 (5.9) | 22 (8.3) |
| Never-married | 208 (15.3) | 28 (14.4) | 8 (6.5) | 23 (11.3) | 40 (15.3) | 45 (14.7) | 64 (24.2) |
| Divorced/separated | 185 (13.6) | 38 (19.5) | 20 (16.1) | 27 (13.2) | 33 (12.6) | 36 (11.8) | 31 (11.7) |
| Widowed | 19 (1.4) | 2 (1.0) | 3 (2.4) | 2 (1.0) | 4 (1.5) | 4 (1.3) | 4 (1.5) |
Stairwells and elevators were located in separate areas within this building
Fig. 1.
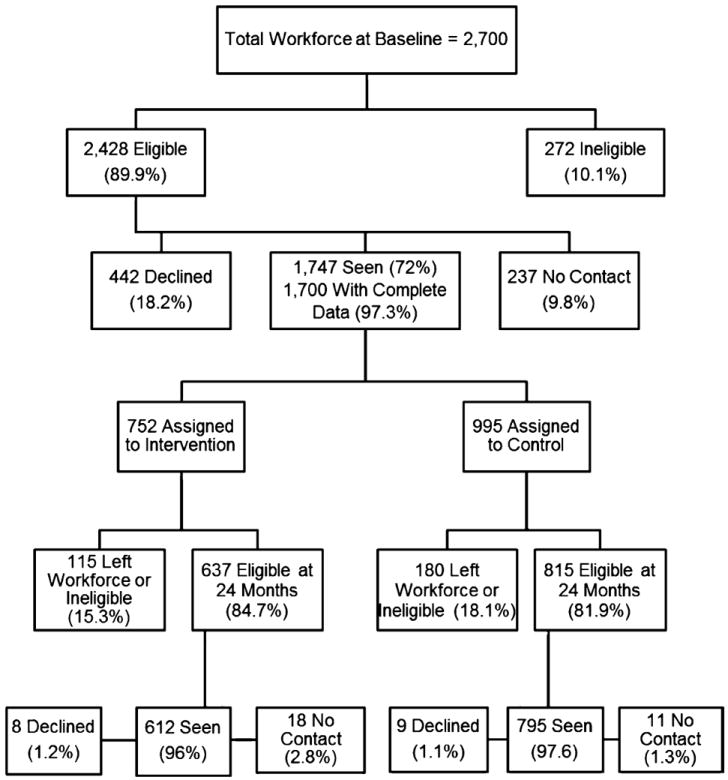
Individual participant recruitment flow diagram
Procedures
As part of a worksite weight gain prevention trial, modifications were made to all stairwells in the three intervention worksites in order to promote physical activity at work. The larger intervention focused on assessing the long-term effectiveness of environmental approaches to promoting healthy weight-related behaviors, including physical activity, diet (specifically increased fruit and vegetable consumption and decreased intake of high-fat foods), and increased weight self-monitoring. Key environmental change components included in this program were scales placed at intervention worksites to allow employees to monitor their bodyweight, changes to the food service environment (particularly an emphasis on offering a greater ratio of healthful to unhealthful food in worksite cafeterias and vending machines), and changes made to stairwells to promote greater physical activity at work (for complete details regarding the larger intervention, see Linde et al., 2012). To promote greater stair use by employees at intervention worksites, modifications were made to increase the attractiveness of stairwells (i.e., hanging decorative art posters and playing music) and to encourage the use of stairs (i.e., posting motivational signage outside of the stairwells as point-of-decision prompts to encourage use of stairs over lower-exertion automated forms of between-floor transportation, in particular elevators and escalators). Stair prompts included Blue Cross “DO” campaign posters featuring humorous messages about taking the stairs (such as “Don’t let the machines win. Take the stairs.”) and riddles placed on stair risers in the stairwells (these were introduced by 8.5 × 11 inch signs at stair entries, and then five clues to solve the riddles were positioned on stair risers). All study signage is available from the authors upon request or by accessing the supplemental materials link on the online version of this article.
Messages included in stair-use prompts were benefit/gain framed (e.g., “Raise your fitness level… one step at a time!”). Music played in the stairwells was selected by employees at their worksite. Art posters included modern or classical artists’ works, inspirational message posters, and movie posters. The stairwell modifications (i.e., signs, art, and music) remained in place at the intervention worksites continuously for 2 years. For a comprehensive compendium of intervention posters and signage, please see the electronic supplemental materials link on the title page.
Measures
We measured stair use objectively via infrared beam counters placed on the ground floors in stairwells at each worksite, using methodology adapted from procedures employed in a study of stair use conducted by the Centers for Disease Control and Prevention (CDC) within the CDC Rhodes building in Atlanta, Georgia (Kerr et al., 2004); specifically, study staff recorded daily counts of stair use for 20 consecutive work days both at baseline and at 2-year follow-up. We also assessed self-reported stair use subjectively by means of a questionnaire item which read “In the last month, how frequently did you use the stairs at work?” Response options ranged from “1 time a month or less” to “6 or more times per day.” We transformed all responses into number of times per week using the stairs.
Analyses
We fit generalized estimating equation (GEE) models to account for the nesting of participants within worksites. GEE modeling is a regression-based, non-parametric approach to account for dependency in measurements (e.g., Ballinger, 2004; Zeger, Liang, & Albert, 1988). GEE modeling produces more efficient and unbiased estimates when data are correlated than do ANOVA-based models (e.g., Zeger & Liang, 1986) and adjusts for within-cluster (i.e., worksite) correlations (Norton et al., 1998). This method is becoming widely used to examine effects of interventions when worksites or schools are randomly assigned to intervention and control conditions (e.g., Crespo, Sallis, Conway, Saelens, & Frank, 2011). Although ideally suited to comparing a larger number of groups, Horton and Lipsitz (1999) have reported that using model-based variance estimators can be helpful in situations like the present analyses, when the number of groups being compared is small. Therefore, the GEE analyses conducted in this study utilized model-based variance estimators. We performed these analyses to examine both objectively-measured and self-reported stair use, comparing intervention versus control change over time on each measure of stair use.
Analyses examining change over time in objectively-measured stair use (i.e., total stair use trips during the 20-day recording period at the end of the 2-year intervention minus total stair use trips during the 20-day baseline recording period) controlled for objectively-measured baseline stair use, number of floors in the worksite building, and number of stairwells monitored with infrared beam counters. Analyses examining change over time in self-reported stair use (participant-reported flights of stairs per week at 1-year data collection minus participant-reported flights of stairs at baseline) also controlled for number of floors and number of stairwells monitored, as well as self-reported baseline stair use and also individual-level demographic characteristics (i.e., age, sex, race/ethnicity, BMI, marital status, and education). In addition, we tested a separate GEE model of self-reported stair use that included an interaction variable (intervention status × baseline stair use) to investigate whether the intervention was differentially effective among participants with higher versus lower amounts of stair use at baseline. Baseline stair use was centered prior to the computation of the multiplicative interaction term, and the analysis included main effects in addition to the interaction term.
Results
Results of the GEE analyses, presented in Table 2, indicated that the intervention had a positive effect on change from baseline to 2 years. The intervention sites showed greater increases in stair use over time than the control sites for both objectively-measured and self-reported stair use. Examination of predicted values from the GEE analyses indicated an objective stair use decrease of 124.06 stair counts per day over time at the control sites; at the intervention sites, stair use increased over time by 346.77 stair counts per day. For self-reported stair use, the control group change was an increase of 0.73 stair-use trips per week and the intervention group manifested an increase of 2.28 trips per week.
Table 2.
Change in stair use from baseline to 2-year follow-up using GEE models
| Predictor | Objectively-measured stair use
|
Self-reported stair use
|
||
|---|---|---|---|---|
| b (se) | p | b (se) | p | |
| Intervention versus controla | 470.83 (96.14) | <0.001 | 1.56 (0.63) | 0.01 |
| Baseline stair useb | 0.07 (0.03) | 0.03 | −0.34 (0.03) | <0.001 |
| Floors (# at worksite) | −74.24 (19.10) | <0.001 | 0.01 (0.13) | 0.93 |
| Proportion of stairwells with associated elevator | 1,160.65 (166.73) | <0.001 | −2.28 (1.22) | 0.06 |
| Age | 0.01 (0.02) | 0.83 | ||
| BMI | −0.16 (0.03) | <0.001 | ||
| Sexc | −0.59 (0.35) | 0.09 | ||
| Raced | 1.46 (0.54) | 0.01 | ||
| Education | −0.15 (0.19) | 0.43 | ||
| Marital statuse | −0.49 (0.34) | 0.15 | ||
| Interaction (baseline stair use × intervention)f | −0.08 (0.04) | 0.05 | ||
Note. Analyses accounted for clustering within worksite
Intervention coded as 1; control coded as 0
Baseline stair use assessed objectively (for objective stair use outcome) and via self-report (for self-reported stair use outcome)
Female = 2; male = 1
White = 1; else = 0
Married = 1; else = 0
Interaction tested in a separate model calculated using centered baseline stair use
In addition, the interaction tested (intervention status × baseline stair use) was a significant predictor of change in self-reported stair use, indicating that the intervention had a differential impact on change in stair use behavior over time based upon participants’ initial levels of stair use at baseline. To examine the nature of this interaction, we created a dichotomous variable that split participants into daily versus less-than-daily stair use at baseline (i.e., those who self-reported taking at least one flight of stairs per day at baseline versus those who reported less than one flight of stairs per day). Re-running the GEE models for only those participants reporting daily stair use revealed that intervention status was not a significant predictor of change in self-reported stair use over time (b = 0.71, SE = 0.48, p = 0.14). However, for participants reporting less-than-daily stair use at baseline, a GEE model of change in stair use over time indicated that the intervention significantly increased stair use (b = 1.51, SE = 0.46, p = 0.001). Examination of predicted values from the GEE analysis indicated that for these low stair users at baseline, the control group change in self-reported stair use was an increase of 1.55 stair-use trips per week and the intervention group change was twice as large (i.e., an increase of 3.06 trips per week). Thus, the intervention was most effective at increasing stair use among those participants who engaged in the lowest levels of stair use at baseline.
Discussion
Simple and inexpensive environmental modifications made in and around worksite stairwells were associated with long-term increases in objectively-measured and self-reported stair use. Although these increases were relatively small overall among intervention participants, it should be noted that the control participants’ stair use actually declined during this same span; further, the increase of approximately one stair-use trip per week among intervention participants constituted an average across those participants who already used the stairs frequently at baseline as well as infrequent stair users. This is noteworthy because, although those individuals who were already using the stairs frequently showed small changes in stair use over time, the environmental modifications implemented in the present intervention resulted in long-term increases in self-reported stair use of more than three trips per week among those individuals who, at baseline, were using the stairs the least (less than once per day).
These results support the enhancement of worksite stairwells as a low-cost strategy to promote employee physical activity, and therefore physical fitness and health. Recently many employers have begun offering incentives to employees to lose weight, increase their physical activity, or otherwise improve their health (Linnan et al., 2008). Such strategies can improve a workplace in a variety of ways, including saving money otherwise lost to illness or injury sustained by less healthy employees (Goetzel & Ozminkowski, 2008). Our results suggest that low-cost stairwell modifications can produce increased worksite physical activity, especially among those who currently use stairs the least. Thus, stairwell enhancement could work alongside other health promotion efforts being utilized in workplaces (e.g., fitness breaks, incentives/infrastructure for walking or cycling to work) to contribute to a more physically active workforce.
The present study objectively and subjectively measured stair use among individuals participating in a worksite weight-loss trial. Objective and subjective measures of stair use can be effectively used together to identify overall trends and to better understand patterns of change over time. The self-report and objective data from the present study each provide evidence that the intervention effectively increased worksite stair use, and each data source provided its own strengths and weaknesses. Self-report measures of physical activity are subject to exaggeration, recall bias, and other well-documented problems (Sallis & Saelens, 2000). With the objective measurement of stair use, it was not possible to identify whether the individuals using the stairs were study participants or other individuals in the building (e.g., employees not enrolled in the study, visitors). In addition, the number of employees per site was counted only once, at baseline. Although no large changes in the worksite populations under investigation were reported during this time period, it is possible that the numbers of employees fluctuated during the study time frame. Such fluctuations could constitute a limitation of the objective, but not the self-report, data collected.
For both objective and subjective measures of stair use, we could not discern whether the stair use was occurring as ascending or descending of the stairs. Use of a combined stair ascent and descent measure is a limitation of both measures, because more than twice as much energy is expended in climbing stairs as descending them (Teh & Aziz, 2002), and it was possible in the study worksites for individuals to use elevators to ascend to higher floors and stairs to descend. Although we cannot determine the frequency of this combination of elevator and stair use, previous researchers have found descending stairs to be more common than ascending (Eves, Webb, & Mutrie, 2006), and have also found interventions to successfully increase descent, but not ascent (Kerr, Eves, & Carroll, 2001d). It is, however, worth noting that stair descending burns significantly more calories than standing in an elevator. Additionally, the present self-report stair use data are consistent with previous work assessing stair ascending, in that the pattern of demographic characteristics of those reporting the most stair use in the present study are consistent with previous work (e.g., non-white, overweight individuals and females climb stairs less than their comparison groups; Webb & Eves, 2007; Webb, Eves, & Kerr, 2011; Eves et al., 2006).
We also noted that not all intervention sites were equally compliant with study guidelines regarding implementation of signage and music in stairwells. Specifically, one of the three intervention worksites (notably, the one that showed the smallest increase in stair use over time among the intervention sites) did not institute the intervention components of playing music or placing decorative posters in the stairwells. This inconsistency in applying the intervention could have weakened the efficacy of the intervention and resulted in smaller increases in stair use at the worksite that did not fully comply with requested stairwell modifications. Indeed, a similar intervention designed to increase stair use (Kerr et al., 2004) produced a short-term increase in stair use, but stairwell use decreased after the first 3 months of the intervention for both artwork and signs, the two techniques used across all three intervention sites. It is possible that if the non-compliant intervention site had integrated all three recommended stairwell modifications the difference in stair-use change over time we noted would have been even greater. Future studies of worksite stair use could test various combinations of these three stairwell modifications (signage, art, and music) and other changes, such as enhanced lighting, altering the type of stair covering, and color of stairwell paint, to determine what combinations of factors work most effectively in concert to promote stair use at worksites.
In addition, we note that although intervention and control worksites were randomized in pairs to approximately match worksites on size and employee characteristics, no two worksite buildings were identical. Some of the between-building differences were structural elements that were relevant for the assessment of stair-usage. For example, one of the three control worksites contained an escalator whereas its comparison intervention site did not have an escalator. Escalator use was not explicitly assessed in this study, as employees could use the escalator either actively (by walking on the moving stairs) or passively (by standing). Another between-site difference was that one control site had a staircase that was open, in an atrium, which could not be equipped with an infrared counter, so use of these stairs was not measured objectively at either baseline or follow-up. Although we would have preferred to objectively measure stair use on all stairs available at all worksites, it seems likely that measuring stair use on all stairwells at five of the six worksites and five of the six stairwells at the remaining site, and having measured the same stairwells at both baseline and follow-up, that the present analyses fairly reflect the overall rate of change across all the sites. Additional support comes from the consistent findings in the self-report data, which reflected use of all staircases at the worksites.
Although any individual employee’s increase in physical activity at a worksite which has made enhancements to one or more stairwells is likely to be rather modest, modifying a workplace stairwell as was done in this intervention is a relatively easy and low-cost undertaking. The equipment (posters, signs, materials for hanging posters and signs, and music player/music) can be obtained relatively inexpensively (approximately $200–300 for an office stairwell, depending on the number of posters and signs as well as the type of music player purchased) and quickly installed in stairwells. Recently, the cost-effectiveness of obesity prevention interventions has become a critical measure of intervention success and utility (Goetzel & Ozminkowski, 2008). Future research promoting worksite physical activity could objectively monitor individual change over time using pedometers, accelerometers, or other measuring devices to more precisely determine change in individual energy expenditure from pre- to post-stairwell enhancement. In addition, future studies could incorporate sophisticated analyses of cost-effectiveness of stair-use promotion interventions. The present analyses have indicated that an inexpensive intervention can successfully increase worksite stair use over 2 years, with greatest increases evident among those individuals who were using the stairs the least at baseline.
Supplementary Material
Acknowledgments
This study was funded by National Institutes of Health Grant 1 R01 DK067362 (R. W. Jeffery, PI); ClinicalTrials.gov identifier: NCT00708461, “Environmental Intervention for Weight Gain Prevention (HealthWorks).”
Footnotes
Conflict of interest The authors have no conflict of interest to disclose.
Electronic supplementary material The online version of this article (doi:10.1007/s10935-013-0323-2) contains supplementary material, which is available to authorized users.
Contributor Information
Dan J. Graham, Email: djgraham@umn.edu, dan.graham@colostate.edu, Division of Epidemiology and Community Health, School of Public Health, University of Minnesota, Minneapolis, MN, USA.
Jennifer A. Linde, Division of Epidemiology and Community Health, School of Public Health, University of Minnesota, Minneapolis, MN, USA
Julie M. Cousins, School of Kinesiology, College of Education and Human Development, University of Minnesota, Minneapolis, MN, USA
Robert W. Jeffery, Division of Epidemiology and Community Health, School of Public Health, University of Minnesota, Minneapolis, MN, USA
References
- Andersen RE, Franckowiak SC, Snyder J, Bartlett SJ, Fontaine KR. Can inexpensive signs encourage the use of stairs? Results from a community intervention. Annals of Internal Medicine. 1998;129(5):363–369. doi: 10.7326/0003-4819-129-5-199809010-00003. [DOI] [PubMed] [Google Scholar]
- Ballinger GA. Using generalized estimating equations for longitudinal data analysis. Organizational Research Methods. 2004;72(2):127–150. doi: 10.1177/1094428104263672. [DOI] [Google Scholar]
- Blamey A, Mutrie N, Aitchison T. Health promotion by encouraged use of stairs. British Medical Journal. 1995;311(7000):289–290. doi: 10.1136/bmj.311.7000.289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boutelle KN, Jeffery RW, Murray DM, Schmitz MK. Using signs, artwork, and music to promote stair use in a public building. American Journal of Public Health. 2001;91(12):2004–2006. doi: 10.2105/ajph.91.12.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brownell KD, Stunkard AJ, Albaum JM. Evaluation and modification of exercise patterns in the natural environment. American Journal of Psychiatry. 1980;137(12):1540–1545. doi: 10.1176/ajp.137.12.1540. [DOI] [PubMed] [Google Scholar]
- Brownson RC, Baker EA, Housemann RA, Brennan LK, Bacak SJ. Environmental and policy determinants of physical activity in the United States. American Journal of Public Health. 2001;91(12):1995–2003. doi: 10.2105/ajph.91.12.1995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bungum T, Meacham M, Truax N. The effects of signage and the physical environment on stair usage. Journal of Physical Activity and Health. 2007;4(3):237–244. doi: 10.1123/jpah.4.3.237. [DOI] [PubMed] [Google Scholar]
- Coleman KJ, Gonzalez EC. Promoting stair use in a US-Mexico border community. American Journal of Public Health. 2001;91(12):2007–2009. doi: 10.2105/ajph.91.12.2007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crespo NC, Sallis JF, Conway TL, Saelens BE, Frank LD. Worksite physical activity policies and environments in relation to employee physical activity. American Journal of Health Promotion. 2011;25(4):264–271. doi: 10.4278/ajhp.081112-QUAN-280. [DOI] [PubMed] [Google Scholar]
- Dunn AL, Andersen RE, Jakicic JM. Lifestyle physical activity interventions. History, short- and long-term effects, and recommendations. American Journal of Preventive Medicine. 1998;15(4):398–412. doi: 10.1016/s0749-3797(98)00084-1. [DOI] [PubMed] [Google Scholar]
- Engbers LH, van Poppel MN, van Mechelen W. Modest effects of a controlled worksite environmental intervention on cardiovascular risk in office workers. Preventive Medicine. 2007;44(4):356–362. doi: 10.1016/j.ypmed.2006.11.005. [DOI] [PubMed] [Google Scholar]
- Eves FF, Masters RS, McManus A, Leung M, Wong P, White MJ. Contextual barriers to lifestyle physical activity interventions in Hong Kong. Medicine and Science in Sports and Exercise. 2008;40(5):965–971. doi: 10.1249/MSS.0b013e3181659c68. [DOI] [PubMed] [Google Scholar]
- Eves FF, Webb OJ, Mutrie N. A workplace intervention to promote stair climbing: Greater effects in the overweight. Obesity. 2006;14(12):2210–2216. doi: 10.1038/oby.2006.259. [DOI] [PubMed] [Google Scholar]
- Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999–2008. The Journal of the American Medical Association. 2010;303(3):235–241. doi: 10.1001/jama.2009.2014. [DOI] [PubMed] [Google Scholar]
- Ford MA, Torok D. Motivational signage increases physical activity on a college campus. Journal of American College Health. 2008;57(2):242–244. doi: 10.3200/JACH.57.2.242-244. [DOI] [PubMed] [Google Scholar]
- Goetzel RZ, Ozminkowski RJ. The health and cost benefits of work site health-promotion programs. Annual Review of Public Health. 2008;29:303–323. doi: 10.1146/annurev.publhealth.29.020907.090930. [DOI] [PubMed] [Google Scholar]
- Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, et al. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Medicine and Science in Sports and Exercise. 2007;39(8):1423–1434. doi: 10.1249/mss.0b013e3180616b27. [DOI] [PubMed] [Google Scholar]
- Horton NJ, Lipsitz SR. Review of software to fit generalized estimating equation regression models. The American Statistician. 1999;53:160–169. doi: 10.1002/(SICI)1097-0258(19990130)18:2<213:AID-SIM999>3.0.CO;2-E. [DOI] [Google Scholar]
- Kerr J, Eves F, Carroll D. Posters can prompt less active people to use the stairs. Journal of Epidemiology and Community Health. 2000;54(12):942. doi: 10.1136/jech.54.12.942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kerr J, Eves F, Carroll D. Encouraging stair use: Stair-riser banners are better than posters. American Journal of Public Health. 2001a;91(8):1192–1193. doi: 10.2105/ajph.91.8.1192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kerr J, Eves F, Carroll D. Six-month observational study of prompted stair climbing. Preventive Medicine. 2001b;33(5):422–427. doi: 10.1006/pmed.2001.0908. [DOI] [PubMed] [Google Scholar]
- Kerr J, Eves FF, Carroll D. The influence of poster prompts on stair use: The effects of setting, poster size and content. British Journal of Health Psychology. 2001c;6(Part 4):397–405. doi: 10.1348/135910701169296. [DOI] [PubMed] [Google Scholar]
- Kerr J, Eves FF, Carroll D. Can posters prompt stair use in a worksite environment? Journal of Occupational Health. 2001d;43:205–207. [Google Scholar]
- Kerr NA, Yore MM, Ham SA, Dietz WH. Increasing stair use in a worksite through environmental changes. American Journal of Health Promotion. 2004;18(4):312–315. doi: 10.4278/0890-1171-18.4.312. [DOI] [PubMed] [Google Scholar]
- Lee IM, Djousse L, Sesso HD, Wang L, Buring JE. Physical activity and weight gain prevention. The Journal of the American Medical Association. 2010;303(12):1173–1179. doi: 10.1001/jama.2010.312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Linde JA, Nygaard KE, MacLehose RF, Mitchell NR, Harnack LJ, Cousins JM, et al. HealthWorks: Results of a multi-component group-randomized worksite environmental intervention trial for weight gain prevention. International Journal of Behavioral Nutrition and Physical Activity. 2012;9:14. doi: 10.1186/1479-5868-9-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Linnan L, Bowling M, Childress J, Lindsay G, Blakey C, Pronk S, et al. Results of the 2004 National Worksite Health Promotion Survey. American Journal of Public Health. 2008;98(8):1503–1509. doi: 10.2105/AJPH.2006.100313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshall AL, Bauman AE, Patch C, Wilson J, Chen J. Can motivational signs prompt increases in incidental physical activity in an Australian health-care facility? Health Education Research. 2002;17(6):743–749. doi: 10.1093/her/17.6.743. [DOI] [PubMed] [Google Scholar]
- Matson-Koffman DM, Brownstein JN, Neiner JA, Greaney ML. A site-specific literature review of policy and environmental interventions that promote physical activity and nutrition for cardiovascular health: What works? American Journal of Health Promotion. 2005;19(3):167–193. doi: 10.4278/0890-1171-19.3.167. [DOI] [PubMed] [Google Scholar]
- Norton EC, Garfinkel SA, McQuay LJ, Heck DA, Wright JG, Dittus R, et al. The effect of hospital volume on the in-hospital complication rate in knee replacement patients. Health Services Research. 1998;33(5 Pt 1):1191–1210. [PMC free article] [PubMed] [Google Scholar]
- Porter E. Women in workplace—Trend reversing/study: They may be unable to fit more in. New York Times 2006 Mar 2; [Google Scholar]
- Sallis JF, Saelens BE. Assessment of physical activity by self-report: Status, limitations, and future directions. Research Quarterly for Exercise and Sport. 2000;71(2 Suppl):S1–S14. [PubMed] [Google Scholar]
- Teh KC, Aziz AR. Heart rate, oxygen uptake, and energy cost of ascending and descending the stairs. Medicine and Science in Sports and Exercise. 2002;34(4):695–699. doi: 10.1097/00005768-200204000-00021. [DOI] [PubMed] [Google Scholar]
- Troiano RP, Berrigan D, Dodd KW, Masse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Medicine and Science in Sports and Exercise. 2008;40(1):181–188. doi: 10.1249/mss.0b013e31815a51b3. [DOI] [PubMed] [Google Scholar]
- Webb OJ, Eves FF. Promoting stair climbing: Intervention effects generalize to a subsequent stair ascent. American Journal of Health Promotion. 2007;22(2):114–119. doi: 10.4278/0890-1171-22.2.114. [DOI] [PubMed] [Google Scholar]
- Webb OJ, Eves FF, Kerr J. A statistical summary of mall-based stair-climbing interventions. Journal of Physical Activity & Health. 2011;8(4):558–565. doi: 10.1123/jpah.8.4.558. [DOI] [PubMed] [Google Scholar]
- Zeger SL, Liang KY. Longitudinal data analysis for discrete and continuous outcomes. Biometrics. 1986;42(1):121–130. [PubMed] [Google Scholar]
- Zeger SL, Liang KY, Albert PS. Models for longitudinal data: A generalized estimating equation approach. Biometrics. 1988;44(4):1049–1060. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.