

Abstract
Complete rupture of the Achilles tendon is relatively rare, but it is an injury of considerable clinical relevance. A common cause of non-traumatic tendon rupture is local corticosteroid infiltration. Corticosteroid injections may start a degenerative process resulting in partial rupture and subsequent complete rupture of the tendon due to a direct toxic effect, because corticosteroids inhibit production of extracellular matrix collagen and also because of poor local vascularization. This paper describes the case of a patient who presented with complete rupture of the Achilles tendon shortly after administration of local corticosteroid injections in the treatment of deep retrocalcaneal bursitis. This confirms that corticosteroid treatment which is not correctly and accurately administered may be a factor contributing to major injury. It demonstrates that the physician must take all necessary precautions when administering corticosteroid infiltration. It is particularly important that corticosteroid injection is performed under ultrasound guidance which permits visualization of the needle tip and therefore exact identification of the injection site.
Keywords: Achilles tendon, Ultrasound, Corticosteroid injections
Riassunto
Le rotture complete del tendine d’Achille sono piuttosto rare, ma hanno una notevole rilevanza clinica. Tra le cause atraumatiche di rottura sono abbastanza frequenti quelle che riconoscono come concausa i trattamenti infiltrativi locali di corticosteroidi. Questi, sia con un’azione tossica diretta, sia con l’inibizione sulla produzione della matrice extracellulare del collagene, sia con una riduzione della vascolarizzazione locale, determinano un processo degenerativo che progredendo determina dapprima una lesione parziale e poi una rottura completa del tendine. Il caso riportato si riferisce ad una paziente che, per il trattamento di una borsite retrocalcaneale profonda, veniva trattata con terapia infiltrativa locale con cortisone e, a breve distanza di tempo, presentava una rottura completa del tendine d’Achille; è esplicativo come un trattamento terapeutico con corticosteroidi, eseguito in maniera non del tutto corretta, possa essere concausa di lesioni importanti. E’ indicativo del fatto che sia necessario rispettare tutte le precauzioni quando si procede a terapia infiltrativa locale di corticosteroidi, in particolare come sia importante iniettare sotto guida ecografica perché ciò consente di valutare in tempo reale la posizione della punta dell’ago e quindi di conoscere esattamente la sede di iniezione.
Introduction
Ultrasound (US)-guided local infiltration has often proved to be a valid therapy in the treatment of muscoloskeletal pain due to characteristics such as economicity, effectiveness and long-term pain relief [1, 2]. Various drugs including corticosteroids are used in interventional musculoskeletal procedures. They have been used since 1953 in degenerative joint diseases of the shoulder, knee and hip and in inflammatory conditions such as bursitis. While the effectiveness of short-term treatment is undisputed, prolonged use of these drugs is highly controversial [2].
The corticosteroids which are commonly used today are analogs of human hormones synthesized in the laboratory. In humans, corticosteroid hormones are produced by the adrenal glands and released in the body in response to stress; they control the protein, fat and carbohydrate metabolism and furthermore exert an important anti-inflammatory activity by preventing phospholipid release, decreasing the effect of eosinophils and proinflammatory cytokines and through a number of other mechanisms, e.g. reducing the vascularization.
The rationale behind the use of corticosteroids in pain control is related to their anti-inflammatory effect, which provides pain relief without affecting the mechanism that caused the pain, and they furthermore reduce adhesions between the various structures. However, corticosteroids also cause adverse effects including osteoporosis, and they have a local immunosuppressive effect which increases the risk of infections as well as the risk of partial and complete tendon rupture [2, 3].
Complete Achilles tendon rupture is relatively rare, but it is an injury of considerable clinical relevance [4–6]. We report this case as it confirms that corticosteroid treatment may be a factor contributing to major injury.
Description of the case
A 54-year-old overweight patient presented with retrocalcaneal swelling and pain. US imaging showed moderate degeneration of the Achilles tendon with a significant fluid collection in the deep retrocalcaneal bursa. Two procedures were carried out (1 week interval between the two) to drain the inflamed bursa and subsequently administer injection of corticosteroids without US guidance. This therapy significantly improved the symptoms.
However, 2 weeks after the last treatment the patient experienced acute pain in the ipsilateral Achilles tendon and consequent functional impotence for no apparent reason. Physical examination suggested rupture of the Achilles tendon. US examination including dynamic maneuvers was therefore performed revealing complete rupture of the distal portion with interposed hematoma and moderate retraction of the stumps (Fig. 1), particularly the proximal stump. Subsequent surgery confirmed complete rupture of the Achilles tendon.
Fig. 1.
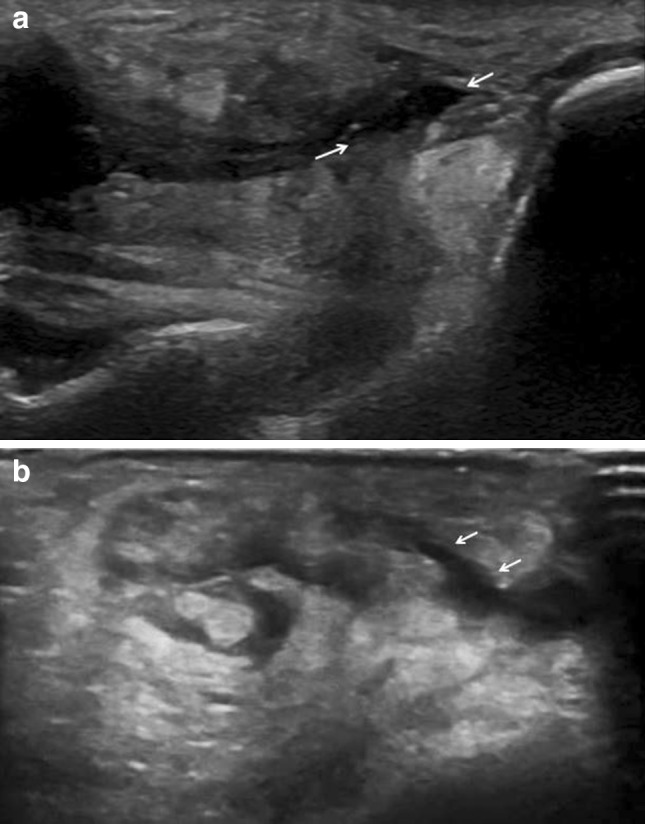
US imaging performed along the long axis (a) and along the second short-axis (b) of the Achilles tendon revealed complete rupture of the tendon fibers in the portion before insertion (arrows), with moderate retraction of the stumps and interposed hematoma
Discussion and conclusions
Complete rupture of the Achilles tendon, traumatic or non-traumatic, is relatively rare [6]. Non-traumatic ruptures are most often related to degenerative phenomena, which reduce the strength and elasticity of the tendon tissue over time, to predisposing factors which increase stress on the tendon and to local or systemic medication, such as fluoroquinolones and corticosteroids [4, 5].
The mechanism underlying these phenomena is linked to hypoxia, and non-traumatic lesions are typically localized in the critical area (about 3 cm proximal to the calcaneal insertion) which receives less blood flow. When progressing, the degenerative process may initially result in partial rupture and subsequently in complete rupture of the tendon [6]. Subcutaneous rupture of the Achilles tendon generally affects the medium-proximal portion. However, in cases where the degenerative disease affects the distal third, it is frequently associated with deep retrocalcaneal bursitis.
There are not many papers in the literature dealing with this issue, but it has been demonstrated that tendon ruptures are more frequent after local infiltration of corticosteroids [3]. This occurs due to a direct toxic effect of the drug, because corticosteroids inhibit production of extracellular matrix collagen and also because of poor local vascularization. Local infiltration of corticosteroid about the Achilles tendon is therefore rarely performed nowadays. However, local infiltration in case of bursitis is still considered a valid treatment and it is widely performed [1, 2].
In the present case, rupture did not occur in the typical location, but more distally in the portion located right above the deep retrocalcaneal bursa, where local infiltration of corticosteroids had been performed without US guidance. Re-evaluation of US images, taken 3 weeks before the rupture, showed only moderate degeneration of the tendon in addition to bursitis. This fact as well as the atypical location of the lesion led to the suspicion that iatrogenic injury may have contributed to the rupture.
We consider this case worthy of being reported to emphasize that adequate precaution must be taken in connection with local corticosteroid infiltration. It is particularly important that injection is performed under US guidance as this procedure permits visualization of the needle tip and therefore exact identification of the injection site.
Conflict of interest
Gianfranco Vallone and Vittorio Tarallo declare that they have no conflict of interest related to this paper.
Informed consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. The patient provided written informed consent to the publication of this paper and to the inclusion in this article of information that could potentially lead to her identification.
References
- 1.Robotti Guido, Canepa Maria Grazia, Bortolotto Chandra, Draghi Ferdinando. Interventional musculoskeletal US: an update on materials and methods. Journal of Ultrasound. 2013;16(2):45–55. doi: 10.1007/s40477-013-0018-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Draghi F, Robotti G, Jacob D, Bianchi S. Interventional musculoskeletal ultrasonography: precautions and contraindications. J Ultrasound Sept. 2010;13(3):126–133. doi: 10.1016/j.jus.2010.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Nichols AW. Complications associated with the use of corticosteroids in the treatment of athletic injuries. Clin J Sport Med. 2005;15(5):370–375. doi: 10.1097/01.jsm.0000179233.17885.18. [DOI] [PubMed] [Google Scholar]
- 4.Bianchi S, Martinoli C. Ultrasound of the musculoskeletal system, vol 16. Springer, Berlin, pp 817–823 (2007)
- 5.Hartgerink P, Fessell DP, Jacobson JA, Van Holsbeeck MT. Full-versus partial-thickness Achilles tendon tears: sonographic accuracy and characterization in 26 cases with surgical correlation. Radiology. 2001;220:406–412. doi: 10.1148/radiology.220.2.r01au41406. [DOI] [PubMed] [Google Scholar]
- 6.Gervasio Andrea, Bollani Paola, Biasio Aurelio. US in mid-portion Achilles tendon injury. Journal of Ultrasound. 2013;17(2):135–139. doi: 10.1007/s40477-013-0023-z. [DOI] [PMC free article] [PubMed] [Google Scholar]