

Abstract
Excessive gingival display is a frequent finding that can occur because of various intraoral or extraoral etiologies. This report describes the use of surgical lip repositioning technique for the management of a gummy smile associated with vertical maxillary excess and hypermobility of the upper lip. The procedure restricts the muscle pull of the elevator lip muscles by shortening the vestibule, thus reducing the gingival display when smiling. Healing was uneventful and follow-up examinations of 10 months revealed reduced gingival display. For patients desiring a less invasive alternative to orthognathic surgery, lip repositioning is a viable alternative.
Keywords: Excessive gingival display, gummy smile, lip repositioning
INTRODUCTION
A smile is an expression denoting pleasure, joy, happiness, or amusement. Smiling is something that is understood by everyone irrespective of one's culture, race, or religion. Smiling is a means of communicating emotions throughout the world.
A smile is an important gestural method of communication and is an interaction between the teeth, the lip framework, and the gingival scaffold.[1] One of the most important or distinct features of dental and facial esthetics is the vertical anterior tooth display.[2] Esthetic judgment is made by viewing the patient from the front in dynamic states like conversation, facial expressions, and smiling.[3]
The harmony of the smile is determined by the shape, the position, and the color of teeth and also by the gingival tissues. The gingival margin should be healthy and harmonious and today both patients and dentists are more aware of the impact of the gingiva on the beauty of the smile[4] and particularly the periodontist can influence the appearance of the patient's smile.[1]
The amount of visibility of the periodontium depends on the position of the smile line, which is defined as the relationship between the upper lip and the visibility of gingival tissues and teeth. The smile line is an imaginary line following the lower margin of the upper lip and usually has a convex appearance.[4] Few publications exist regarding the relationship between teeth and periodontium visibility during the smile.[5,6] Most dental professionals believe that during smiling the upper lip should position itself at the gingival margin of the maxillary central incisors.[7,8] However, it is known that displaying a certain amount of gingiva is esthetically acceptable and in many cases imparts a youthful appearance.[2,9] Common cause of patient dissatisfaction is excessive gingival display. Patients may complain of a “gummy smile” and “short” maxillary anterior teeth.
At least 50% of patients exhibit some form of gingival display in a normal smile.[5] However, exaggerated or forced smile patterns in up to 76% of all patients may exhibit gingiva. In absolute numbers, a normal gingival display between the inferior border of the upper lip and the gingival margin of the anterior central incisors during a “normal” smile is 1-2 mm.[10] In contrast, an excessive gingiva-to-lip distance of 4 mm or more is classified as “unattractive” by lay people and general dentists.[11]
Four possible etiologies of excessive gingival display and the various treatment modalities are as follows:[12]
Delayed eruption as a result the gingiva fails to complete the apical migration over the maxillary teeth to a position that is 1 mm coronal to the cemento-enamel junctions.[13,14] In these patients, restoring the normal dentogingival relationships can be achieved with an esthetic crown lengthening, which is a well-documented treatment modality that is highly effective in treating patients with delayed eruption.[15,16] The procedure involves moving the gingival margins apically through soft and possibly hard tissue resection
Compensatory eruption of the maxillary teeth with concomitant coronal migration of the attachment apparatus, which includes the gingival margins. Orthodontic leveling of the gingival margins of the maxillary teeth may be considered in this situation.[17] Resective surgery is also possible but may expose the narrow root surface and necessitate a restoration
Vertical maxillary excess in which there is an enlarged vertical dimension of the midface and “incompetent” lips. Treatment involves orthognathic surgery to restore normal inter-jaw relationships and to reduce the gingival display,[18] this involves hospitalization and significant side effects for patients
When the patient smiles, if the upper lip moves in an apical direction and exposes the dentition and excessive gingiva, then surgical lip repositioning may be utilized to reduce the labial retraction of the elevator smile muscle and minimize the gingival display. This procedure was first described in the plastic surgery literature in 1973[19] and was recently published in the dental literature.[20]
So it is very important to establish the etiology responsible for the excessive gingival display. Lip repositioning is suggested as an additional treatment modality for patients with lip hypermobility exposing undesired gingiva in a smile.[12] This article gives a short review on lip repositioning and a case report of the surgical technique that was used to reduce gingival display.
The objective of lip repositioning is to minimize the gingival display by limiting the retraction of the elevator smile muscles (e.g., zygomaticus minor, levator anguli oris, orbicularis oris and levator labii superioris) which is achieved by removing a strip of mucosa from the maxillary buccal vestibule and creating a partial-thickness flap between the mucogingival junction and the upper lip musculature. The lip mucosa is then sutured to the mucogingival line, resulting in a narrower vestibule and restricted muscle pull, thereby reducing gingival display during smiling.[20]
This technique was originally described as cosmetic surgery by Rubinstein and Kostianovsky[19] for correction of a gummy smile caused by a hypermobile lip. This surgical procedure was designed to be shorter, less aggressive, and was thought to have fewer postoperative complications compared to orthognathic surgery. The procedure was advocated again by Litton and Fournier[21] for the correction of excessive gingival display in the presence of a short upper lip. This was accomplished by detaching the muscles from the bony structures to coronally position the upper lip and no complications were reported. After a period of 25 years, two case reports again described this procedure.[12,20] The authors described good results. This technique is also termed as mucosal coronally positioned flap in a recently published case report[22] wherein this technique demonstrates short-term successful use of this technique for the management of excessive gingival display in the presence of slight vertical maxillary excess and hypermobility of the upper lip. First case of lip repositioning done by an Indian dentist was by Gupta et al.[23]
Contraindications of lip repositioning include the presence of a minimal zone of attached gingiva, which can create difficulties in flap design, stabilization and suturing, and severe vertical maxillary excess.[12,20]
Previous reports have shown increased chances of relapse in cases with thin biotypes.[12,20] From a surgical design standpoint, the amount of epithelium to be excised varies considerably. In the first report,[19] although an elliptical-shaped incision was used, the amount of epithelium to be excised was not specified. To achieve optimal results, in one study,[22] the mucosal coronally positioned flap was advanced a distance of two times the gingival display arbitrarily excising 10 to 12 mm,[12,20] and in some instances up to 20 mm[24] of epithelium as described in previous reports.
Postoperative symptoms usually include some mild discomfort for several days and a feeling of “tension” when the patient smiles.[12] The procedure is safe and has minimal side effects like postoperative bruising, discomfort, and swelling of the upper lip.[22]
Variations in surgical lip repositioning have been reported in the medical literature. Several articles[21,24] advocate severing the smile muscle attachment to prevent relapse of the smile muscle into its original position, this may also minimize the flap tension during suturing. Another method to prevent reattachment of the smile muscles is to use an alloplastic or autogenous separator.[25] This spacer is placed with nasal approach between the elevator muscles of the lip and the anterior nasal spine, thus preventing the superior displacement of the repositioned lip. Lip repositioning has also been performed in conjunction with rhinoplasty.[26] There are case reports of lip repositioning combined with depigmentation and crown lengthening,[27] frenectomy and crown lengthening[28] in single visit. Laser has also been used for lip repositioning procedure combined with crown lengthening.[29]
CASE REPORT
A 25-year-old female patient reported to the Department of Periodontology, H.K.E's S. Nijalingappa Institute of Dental Sciences and Research, Gulbarga (India) with a chief complaint of a excessive display of gums. There was no significant medical or family history and the patient was medically sound and fit for the surgical procedure. On clinical examination extraorally, the face was bilaterally symmetrical with incompetent lips. A severe gingival display was seen during smiling which extended from the maxillary right second premolar to the maxillary left second premolar [Figure 1]. A diagnosis of moderate vertical maxillary excess with hypermobility of upper lip was made. As the patient preferred a less invasive procedure to address her chief complaint, an informed consent was obtained after discussing the alternate treatment modalities, benefits, and possible complications for a lip repositioning procedure.
Figure 1.
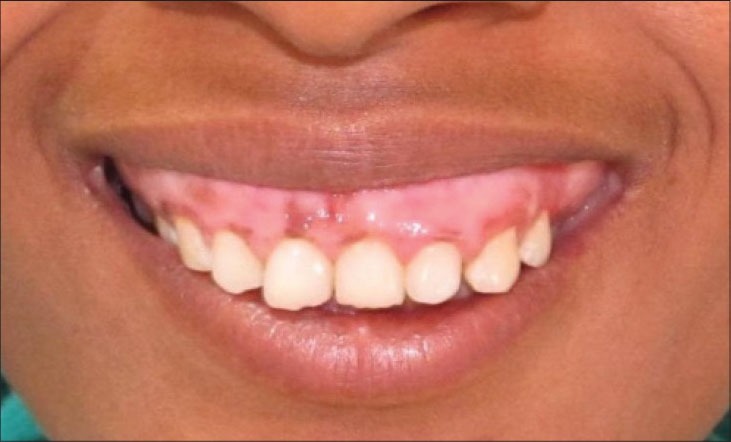
Preoperative
Procedure
Complete extraoral and intraoral mouth disinfection was carried out, and the surgical site was anesthetized between the first maxillary molars. The local infiltration was administered in the buccal vestibule, with additional infiltration for hemostasis purposes. The surgical area was demarcated with sterile pencil on dried tissue [Figure 2]. The partial thickness incision was started at the mucogingival junction extending from right first molar to left first molar. A second parallel incision was made at the facial mucosa at approximately 13-15 mm distance from the first incision. The two incisions were connected to create an elliptical outline [Figure 3]. After these incisions were made, the epithelium was excised [Figure 4] leaving the underlying connective tissue exposed [Figure 5].
Figure 2.

Incision outline made with a marking pencil
Figure 3.

Incisions made
Figure 4.

The epithelial layer is removed
Figure 5.

Underlying connective tissue exposed
The tissue tags were removed. The mucosal flap was advanced and sutured at the mucogingival junction. First, interrupted suture was placed at the midline to ensure proper alignment of the lip midline with the midline of the teeth [Figure 6], then continuous interlocking sutures were used to approximate both flaps [Figure 7]. Due to short anatomical crown length, crown lengthening was not advisable. Pressure pack was applied for hemostasis [Figure 8]. Postoperative instructions included placing ice packs over the upper lip for several hours, limited facial movements for 1 -week, no brushing around the surgical site for 14 days. The patient was advised to rinse gently with 0.12% chlorhexidine gluconate twice daily for 2 weeks. Postoperative pain was managed with analgesics.
Figure 6.

Interrupted suture placed at the midline
Figure 7.

Continuous interlocking suturing
Figure 8.

Pressure pack applied for hemostasis
At 1-week post operative, uneventful healing pattern was seen [Figure 9]. After 2 months of healing, a scar formation was observed [Figure 10]. Follow-up examinations revealed reduced gingival display [Figures 11 and 12]. Our results indicate good stability at the 1-year follow up.
Figure 9.

1-week postoperative retracted view
Figure 10.

2-months postoperative retracted view showing scar formation
Figure 11.

2-months postoperative
Figure 12.
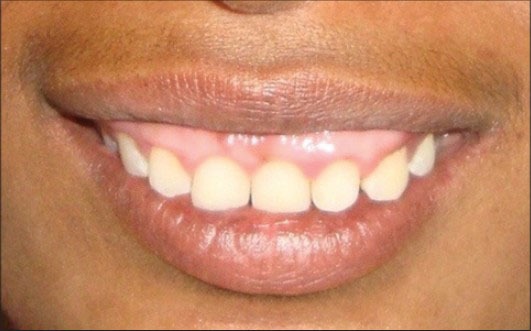
10-months postoperative
CONCLUSION
Surgical lip repositioning is an effective procedure to reduce gingival display by positioning the upper lip in a more coronal location. The long-term stability of the results remains to be seen, but it is a promising alternative treatment modality in esthetic rehabilitation.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Garber DA, Salama MA. The aesthetic smile: Diagnosis and treatment. Periodontol2000. 1996;11:18–28. doi: 10.1111/j.1600-0757.1996.tb00179.x. [DOI] [PubMed] [Google Scholar]
- 2.Zachrisson BU. Esthetic factors involved in anterior tooth display and the smile: Vertical dimension. J Clin Orthod. 1998;35:432–45. [Google Scholar]
- 3.Geron S, Atalia W. Influence of sex on the perception of oral and smile esthetics with different gingival display and incisal plane inclination. Angle Orthod. 2005;75:778–84. doi: 10.1043/0003-3219(2005)75[778:IOSOTP]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 4.Towsend CL. Resective surgery: An esthetic application. Quintessence Int. 1993;24:535–42. [PubMed] [Google Scholar]
- 5.Crispin BJ, Watson JF. Margin placement of esthetic veneer crowns. Part II: Posterior tooth visibility. J Prosthet Dent. 1981;45:389–91. doi: 10.1016/0022-3913(81)90097-4. [DOI] [PubMed] [Google Scholar]
- 6.Tjan AH, Miller GD, The JG. Some esthetic factors in a smile. J Prosthet Dent. 1984;51:24–8. doi: 10.1016/s0022-3913(84)80097-9. [DOI] [PubMed] [Google Scholar]
- 7.Levine RA, McGuire M. The diagnosis and treatment of the gummy smile. Compend Contin Educ Dent. 1997;18:757–62. [PubMed] [Google Scholar]
- 8.Marckley RJ. An evaluation of smiles before and after orthodontic treatment. Angle Orthod. 1993;63:183–9. doi: 10.1043/0003-3219(1993)063<0183:AEOSBA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 9.Arnett GW, Bergman RT. Facial keys to orthodontic diagnosis and treatment planning. Part I. Am J Orthod Dentofacial Orthop. 1993;103:299–312. doi: 10.1016/0889-5406(93)70010-L. [DOI] [PubMed] [Google Scholar]
- 10.Vig RG, Brundo GC. The kinetics of anterior tooth display. J Prosthet Dent. 1978;39:502–4. doi: 10.1016/s0022-3913(78)80179-6. [DOI] [PubMed] [Google Scholar]
- 11.Kokich VO, Jr, Kiyak HA, Shapiro PA. Comparing the perception of dentists and lay people to altered dental esthetics. J Esthet Dent. 1999;11:311–24. doi: 10.1111/j.1708-8240.1999.tb00414.x. [DOI] [PubMed] [Google Scholar]
- 12.Simon Z, Rosenblatt A, Dorfman W. Eliminating a gummy smile with surgical lip repositioning. Cosmet Dent. 2007;23:100–8. [Google Scholar]
- 13.Garguilo A, Wenz F, Orban B. Dimensions and relations at the dentogingival junction in humans. J Periodontol. 1961;132:261–7. [Google Scholar]
- 14.Maynard JG, Jr, Wilson RD. Physiologic dimensions of the periodontium significant to the restorative dentist. J Periodontol. 1979;50:170–4. doi: 10.1902/jop.1979.50.4.170. [DOI] [PubMed] [Google Scholar]
- 15.Lee EA. Aesthetic crown lengthening: Classification, biologic rationale and treatment planning considerations. Pract Proced Aesthet Dent. 2004;16:769–78. [PubMed] [Google Scholar]
- 16.Chu SJ, Karabin S, Mistry S. Short tooth syndrome: Diagnosis, etiology and treatment management. J Calif Dent Assoc. 2004;32:143–52. [PubMed] [Google Scholar]
- 17.Kokich VG. Esthetics: The orthodontic-periodontic restorative connection. Semin Orthod. 1996;2:21–30. doi: 10.1016/s1073-8746(96)80036-3. [DOI] [PubMed] [Google Scholar]
- 18.Ezquerra F, Berrazueta MJ, Ruiz-Capillas A, Arregui JS. New approach to the gummy smile. Plast Reconstr Surg. 1999;104:1143–50. [PubMed] [Google Scholar]
- 19.Rubinstein AM, Kostianovsky AS. Cosmetic surgery for the malformation of the laugh: Original technique in Spanish. Prensa Med Argent. 1973;60:952. [Google Scholar]
- 20.Rosenblatt A, Simon Z. Lip repositioning for reduction of excessive gingival display: A clinical report. Int J Periodontics Restorative Dent. 2006;26:433–7. [PubMed] [Google Scholar]
- 21.Litton C, Fournier P. Simple surgical correction of the gummy smile. Plast Reconstr Surg. 1984;63:372–3. doi: 10.1097/00006534-197903000-00014. [DOI] [PubMed] [Google Scholar]
- 22.Humayun N, Kolhatkar S, Souiyas J, Bhola M. Mucosal coronally positioned flap for the management of excessive gingival display in the presence of hypermobility of the upper lip and vertical maxillary excess: A case report. J Periodontol. 2010;81:1858–63. doi: 10.1902/jop.2010.100292. [DOI] [PubMed] [Google Scholar]
- 23.Gupta KK, Srivastava A, Singhal R, Srivastava S. An innovative cosmetic technique called lip repositioning. J Indian Soc Periodontol. 2010;14:266–9. doi: 10.4103/0972-124X.76936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Miskinyar SA. A new method for correcting a gummy smile. Plast Reconstr Surg. 1983;72:397–400. doi: 10.1097/00006534-198309000-00027. [DOI] [PubMed] [Google Scholar]
- 25.Ellenbogen R, Swara N. The improvement of the gummy smile using the implant spacer technique. Ann Plast Surg. 1984;12:16–24. doi: 10.1097/00000637-198401000-00004. [DOI] [PubMed] [Google Scholar]
- 26.Cachay-Velasquez H. Rhinoplasty and facial evpression. Ann Plast Surg. 1992;28:427–33. doi: 10.1097/00000637-199205000-00006. [DOI] [PubMed] [Google Scholar]
- 27.Gupta KK, Srivastava A, Chandra C, Tripathi V. Lip repositioning with crown Lengthening and gingival Depigmentation: A Case Report. J Periodontol Implant Dent. 2011;3:38–42. [Google Scholar]
- 28.Silva CO, Ribeiro-Júnior NV, Campos TV, Rodrigues JG, Tatakis DN. Excessive gingival display: Treatment by a modified lip repositioning technique. J Clin Periodontol. 2013;40:260–5. doi: 10.1111/jcpe.12046. [DOI] [PubMed] [Google Scholar]
- 29.Haseeb H, Al-Dary Surgical lip repositioning using LASER for the reduction of excessive gummy smiles: A case Report. Smile Dent J. 2012;7:26–30. [Google Scholar]