

Abstract
Parental role modeling of healthful eating behaviors has been shown to be positively correlated to children’s dietary intake and preference for fruits and vegetables. However, no study to date has utilized both parent and child report of parental role modeling and assessed role modeling at snacks and dinner. The purpose of this study is to 1) examine associations between parent and child report of parental role modeling of fruit and vegetable consumption at snacks and dinner and 2) determine whether parental role modeling is associated with children meeting daily fruit and vegetable recommendations. Parent-child dyads (N=160) participating in the Healthy Home Offerings via the Mealtime Environment (HOME) Plus study completed baseline surveys that included questions regarding parental role modeling of fruits and vegetables at dinner and snacks. Children also completed 24-hour dietary recalls. Spearman correlations and chi-square/Fisher’s exact test were used to examine relationships between parent and child report of parental role modeling of fruit and vegetable consumption at snacks and dinner and whether children met daily recommended servings of fruits and vegetables. On average, children consumed less than three servings of fruits and vegetables per day with only 23% of children consuming the recommended four daily servings. Similarities between parent and child reports of parental role modeling of fruits and vegetables at snacks and dinner varied by food type (e.g., fruit versus green salad) and whether the role modeling behavior was at snack or dinner. Statistically significant correlations were seen between parent and child report of parental role modeling consumption of fruit at dinner and green salad at dinner. Children who reported parental role modeling of vegetable consumption at snack and green salad at dinner were significantly more likely, than those who did not, to meet the daily fruit and vegetable consumption recommendations. Parents who reported role modeling consumption of fruit at snack were significantly more likely to have children who met daily fruit and vegetable consumption recommendations. Results indicate that children are aware of their parents’ eating behaviors and on occasion report this behavior similarly to their parents. Parents should be encouraged to utilize the opportunity to role model healthful dietary intake, especially at snacks, where consumption of fruits and vegetables may be very low.
Keywords: Role modeling, family meals, child nutrition, fruit and vegetable, snacks, parent
INTRODUCTION
The Dietary Guidelines for Americans recommends children consume a diet rich in fruits and vegetables (U.S. Department of Agriculture and U.S. Department of Health and Human Services, 2010). Diets rich in fruits and vegetables tend to be more nutrient-dense and are associated with many health benefits, including lower body mass index (BMI) and reduced risk for multiple chronic diseases. Currently, one out of four children aged 6–11 years meet daily recommendations for fruit and less than 20% meet recommendations for vegetable intake (Lorson, Melgar-Quinonez, & Taylor, 2009). Additionally, consumption of these foods decreases as children get older (Granner et al., 2004; Vereecken, Ojala, & Delgrande Jordan, 2004). Identifying strategies to reverse this decreasing trend is imperative.
There are several factors that influence children’s intake of fruits and vegetables, including personal, social and environmental factors (De Bourdeaudhuij et al., 2006; Wind et al., 2006). Parental role modeling of healthy eating behaviors is an important social factor and several studies have shown role modeling of healthful foods to be positively associated with child’s dietary intake and preference for fruits and vegetables (Bere & Klepp, 2004; Cullen et al., 2001; De Bourdeaudhuij et al., 2008; Granner et al., 2004; Reinaerts, de Nooijer, Candel, & de Vries, 2007; Wind et al., 2006; Young, Fors, & Hayes, 2004). However, not all studies have had similar findings. Some studies have found that parental role modeling of healthful foods is not significantly associated with children’s consumption of healthful foods (Matheson, Robinson, Varady, & Killen, 2006), that parental role modeling is significantly associated only for girls’ intake of fruits and vegetables (Kristjansdottir et al., 2006) or parental role modeling is significantly associated with intake of fruits and vegetables for normal weight, but not overweight boys (De Bourdeaudhuij et al., 2006).
Methods for measuring parental role modeling of fruit and vegetable consumption have differed significantly and may contribute to different findings observed across studies. Previous studies have either used parent report of modeling (Bauer, Neumark-Sztainer, Fulkerson, Hannan, & Story, 2011; Hendy, Williams, Camise, Eckman, & Hedemann, 2009; Matheson et al., 2006; Palfreyman, Haycraft, & Meyer, 2012; Reinaerts et al., 2007) or child report of parental role modeling (Bere & Klepp, 2004; Cullen et al., 2001; De Bourdeaudhuij et al., 2008; De Bourdeaudhuij et al., 2006; Granner et al., 2004; Kristjansdottir et al., 2006; Wind et al., 2006; Young et al., 2004) with no consistency of findings based on reporter. Studies that have utilized both parent and child report are limited and have focused on meal environments and behavior (Boutelle, Lytle, Murray, Birnbaum, & Story, 2001), diet behaviors (Keery, Eisenberg, Boutelle, Neumark-Sztainer, & Story, 2006), and child quality of life (Cremeens, Eiser, & Blades, 2006; Marques et al., 2013) with no studies assessing dietary intake. Correlations between parent and child report for these studies have also been mixed.
Parental role modeling studies have employed different methods, with varying validity, to measure children’s dietary intake, including child-administered food frequency questionnaires, 24-hour dietary recalls and parent report of child dietary intake. Dietary recall interviews are a valid method for assessing dietary intake in children (Burrows et al., 2012; Field et al., 1998) whereas evidence suggests limitations with food frequency questionnaires (Collins, Watson, & Burrows, 2010) and parent report of child intake (Baranowski, Sprague, Baranowski, & Harrison, 1991). Research on meal-specific outcomes is also limited in previous research. Cullen et al (2001) validated a fruit, juice and vegetable consumption questionnaire, which asked meal- and snack-specific parental role modeling questions, but reported on the correlation between parental role modeling of healthful foods and child consumption rather than on meal-specific findings. Hendy et al (2009) reported that children who ate more snacks had mothers who role modeled eating snacks but did not report findings specific to fruit and vegetable consumption at snack. To our knowledge, no studies exist utilizing both parent and child report of parental role modeling of fruits and vegetables nor do they report meal-specific dietary intake.
The present study will add to the literature by comparing parent- and child-report of parental role modeling of fruits and vegetables at both dinner and snacks and by providing associations of parental role modeling and child’s dietary intake as measured by 24-hour dietary recalls.
METHODS
Study Design
For the present study, data were drawn from the baseline measurement of the Healthy Home Offerings via the Mealtime Environment (HOME) Plus study. HOME Plus is a randomized controlled trial designed to prevent childhood obesity via a family-focused, community-based program that encourages families to eat healthy meals and snacks together and limit their sedentary behavior. The main meal-preparing parent and one 8–12 year-old child per household were recruited to participate. Parent-child dyads (n=160) were recruited for HOME Plus through events and flyers at Minneapolis Park and Recreation centers, where the intervention program was held, as well as other community events. Families were ineligible to participate if parents or children did not speak English, children had conditions such as food allergies that prevented them from participating in the intervention, or children had an age- and gender-adjusted body mass index (BMI) below the 50th percentile. Baseline surveys were completed by 160 parent-child dyads in their homes during the summers of 2011 and 2012 (two cohorts). All adults and children provided written consent and assent, respectively. Families received a $75 gift card for participating in baseline data collection. The study was approved by the University of Minnesota’s Institutional Review Board.
Measures
At baseline, parents and children completed psychosocial surveys and anthropometric measurements, and children completed three 24-hour dietary recalls. The psychosocial surveys assessed a variety of topics, including parental role modeling of healthful foods at snacks and dinner and demographic characteristics. To eliminate bias of parents and children influencing one another’s responses, many steps of precaution were taken. First, trained research staff ensured participants completed their surveys independently as they completed the home visits and if children needed assistance completing their surveys, they were assisted by research staff and not their parent. Second, when possible, parents and children were in separate rooms. If this was not possible, researchers ensured that parents could not see the child’s survey, and vice versa, by placing participants on opposite sides of the table with a research staff seated between them. Third, the orders of the parent and child surveys were structured differently so when participants were completing their surveys simultaneously, they were answering questions on different topics. Finally, since parents and children completed data collection simultaneously, parents did not have the opportunity to read or influence their child’s survey responses since they were completing their own.
Child Report of Parent Role Modeling of Healthful Foods
Parental role modeling of fruits and vegetables was assessed on the child survey using a six-item parent role modeling scale (α=0.84) adapted from a validated scale previously used with children (Cullen et al., 2001). Cullen and colleagues used a 15-item scale that asked children if their parents ate fruit, vegetables, and low-fat foods while with them at snacks; if their parents ate fruit, vegetables, or salad while with them at lunch, supper, and restaurants; and if parents drank 100% juice, ate low fat dressing, and ate low fat mayonnaise while with them. Our six-item scale included two items that assessed parental role modeling at snacks (“When I am with my parent(s)… they eat fruit as a snack. …they eat vegetables as a snack.”) and four items that assessed role modeling at dinner (“When I am with my parent(s)… they eat fruit at dinner. …they eat vegetables at dinner. …they eat green salad at dinner. …they make ½ of the food on their plate at dinner fruits and vegetables.”). Response options were on a 4-point scale: “Usually/Always,” “Sometimes,” “Hardly ever,” and “Never.” For analyses comparing child report and parent report of parental role modeling, response options were not collapsed. For analyses comparing parental role modeling of healthful foods to children’s dietary intake, survey response options were collapsed to “Usually/Always,” and “Sometimes, Hardly ever, Never”.
Parent Report of Role Modeling of Healthful Foods
Parental role modeling of fruits and vegetables was assessed on the parent survey using a six-item parent role modeling scale (α=0.66) created to reflect the same questions that were asked on the child survey. Two validated measures of parental role modeling exist in the literature but do not ask questions about modeling in front of the child nor do they capture meal- and food-specific modeling behaviors (Hendy et al., 2009; Musher-Eizenman & Holub, 2007). Two items on our survey assessed role modeling at snacks (“When you eat a snack in front of your child, how often do you… eat fruit as a snack? …eat vegetables as a snack?”) and four items assessed role modeling at dinner (“When you are with your child, how often do you… eat fruit at dinner? …eat vegetables at dinner? …eat green salad at dinner? …fill ½ your plate with fruits and vegetables at dinner?”). Responses for role modeling of healthful foods at both snack and dinner were on a 4-point scale: “Usually/Always,” “Sometimes,” “Hardly ever,” and “Never.” As described above for the child responses, response options were not collapsed for analyses comparing parent report and child report of parental role modeling. For analyses comparing parental role modeling of healthful foods to children’s dietary intake, survey response options were collapsed to “Usually/Always,” and “Sometimes, Hardly ever, Never.”
Dietary Assessment
Dietary recalls are considered valid for collecting food intake data with children (Lytle et al., 1993; McPherson, Hoelscher, Alexander, Scanlon, & Serdula, 2000) and were completed with all children at baseline. Servings of fruits and vegetables consumed for the total day, at snacks, and at dinner were averaged over three non-consecutive days (two weekdays and one weekend day). The first recall was completed in-person during the baseline data collection and the other two were completed over the phone with trained research staff within two weeks. Fried vegetables (e.g., French fries) were not included as a serving of fruit or vegetable while 100% fruit/vegetable juice was included. Dietary recalls were collected using Nutrition Data System for Research (NDSR) software (NDS-R 4.05, 2007, University of Minnesota, Minneapolis).
Fruit and Vegetable Recommendations
Recommended daily servings of fruits and vegetables for children vary based on age, gender, and physical activity level. The American Academy of Pediatrics recommends 3.5–4 daily servings of fruits and vegetables for sedentary children between the ages of 9–13 years (Gidding et al., 2006). Thus, for this study, children were classified as meeting daily fruit and vegetable recommendations if they consumed at least four daily servings of fruits and vegetables.
Demographics
Parents completed demographic items including information about their birth date (to assess age), race/ethnicity (Hispanic or Latino/Latina, American Indian/Alaskan Native, Asian, African American, White), gender and annual household income (less than $35,000, $35,000–$74,000, $75,000 or more), as well as their child’s birth date, race and ethnicity. Children reported on their own gender. Parent participants were primarily white (77%) and mothers (95%) with a mean age of 41.3 years (SD=7.70). Of the parent sample, 9% achieved high school level education or less, 32% completed some college, 35% had a bachelor’s degree, and 24% had an advanced degree. Child participants were split almost evenly between male and female with a mean age of 10.4 years (SD=1.40). Table 1 provides further information regarding participant demographics.
Table 1.
HOME Plus participant demographic characteristics
| Characteristics | Total | |
|---|---|---|
| % | n | |
| Parent Gender | ||
| - Male | 5% | 8 |
| - Female | 95% | 152 |
| Child Gender | ||
| - Male | 53% | 85 |
| - Female | 47% | 75 |
| Parent Race/Ethnicity | ||
| - Hispanic or Latino | 3% | 5 |
| - White | 77% | 123 |
| Child Race/Ethnicity | ||
| - Hispanic or Latino | 9% | 15 |
| - White | 68% | 109 |
| Income | ||
| - Less than $35,000 | 31% | 49 |
| - $35,000 to $74,000 | 23% | 36 |
| - $75,000 or more | 47% | 74 |
| Mean (SD) | ||
| Age of Adults | 41.38 (7.71) | |
| Age of Children | 10.37 (1.40) | |
Statistical Analysis
T-tests examined the relationship between the parental role modeling scales as reported by parents and children and whether children met four daily servings of fruits and vegetables. A p-value of 0.05 was set for statistical significance. In order to examine associations at different eating occasions (snacks and dinner, separately), additional analyses were performed. Spearman correlations were used to examine associations between parent and child report of parental role modeling of fruit and vegetable consumption at snacks and dinner, as these were rank-level variables. A more conservative p-value of 0.01 was set due to multiple comparisons. Parent and child report of parental role modeling of healthful foods (at snacks and dinner, separately) and whether children met daily recommended servings of fruits and vegetables were dichotomized into “Usually/Always,” and “Sometimes, Hardly ever, Never” and analyzed using Chi-square/Fisher’s exact test. A p-value of 0.05 was set for statistical significance. All analyses were performed using SAS software, version 9.2 (SAS Institute, Cary, NC, USA).
RESULTS
On average, children consumed less than three servings of fruits and vegetables per day while consuming less than half of one serving at snacks and slightly more than one serving at dinner (Table 2). Only 23% (n=36) of children consumed the recommended four daily servings of fruits and vegetables.
Table 2.
Child servings of fruits and vegetables for the total day, at snacks and at dinner
| Food Group | Total Day | Snacks | Dinner | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Fruit (including juice) | 1.60 | 1.34 | 0.28 | 0.53 | 0.32 | 0.55 |
| Vegetable (including juice) | 1.33 | 0.97 | 0.05 | 0.16 | 0.85 | 0.70 |
| Dark Green, Deep Yellow Vegetables | 0.34 | 0.46 | 0.02 | 0.11 | 0.19 | 0.35 |
| Total Fruit and Vegetable (including juice) | 2.93 | 1.80 | 0.33 | 0.54 | 1.17 | 0.85 |
Similarities between parent and child reports of parental role modeling fruits and vegetables at snacks and dinner varied by food type and whether the role modeling was at snack or dinner. Despite response options visually appearing correlated in the figures, correlations were low and not statistically significant between parent and child reports of parental role modeling of fruit and vegetable consumption at snack (Figure 1), vegetables at dinner (Figure 2) and ½ plate fruits/vegetables at dinner (Figure 3), indicating dyadic disagreement between parent and child reports. In contrast, statistically significant and positive correlations were seen between parent and child report of parental role modeling consumption of fruit at dinner (Figure 2) and green salad at dinner (Figure 3).
Figure 1.
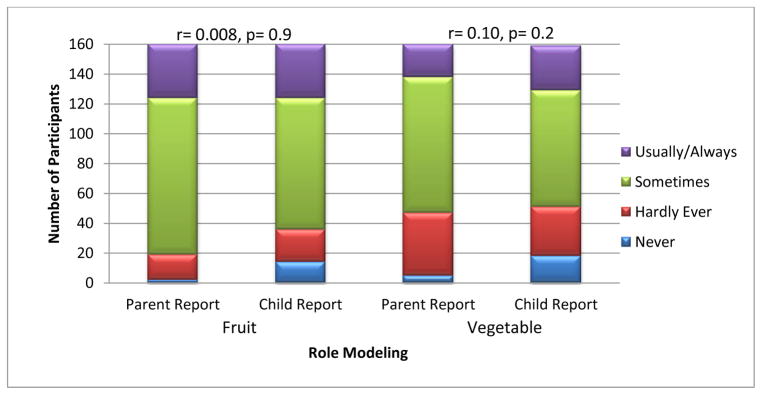
Comparisons of parent and child reports of parental role modeling of fruit and vegetable consumption at snacks
* Statistical significance at p<0.01
Figure 2.
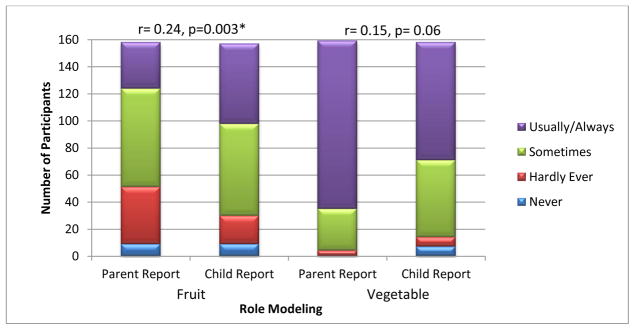
Comparisons of parent and child reports of parental role modeling of fruit and vegetable consumption at dinner
* Statistical significance at p<0.01
Figure 3.
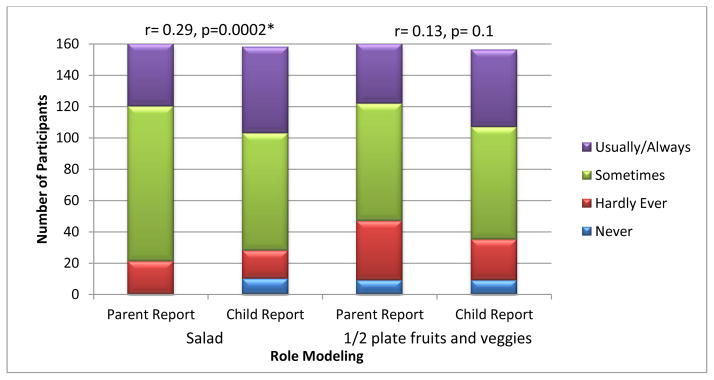
Comparisons of parent and child reports of parental role modeling of salad consumption and filling ½ of plate with fruits and vegetables at dinner
* Statistical significance at p<0.01
Almost all (97%) parents reported role modeling the consumption of vegetables “Sometimes” or “Usually/Always” at dinner compared to 71% role modeling vegetables at snacks. Similarly, 91% of children reported parental role modeling of vegetables “Sometimes” or “Usually/Always” at dinner compared to 68% at snacks. Other than role modeling fruit consumption at dinner and ½ plate fruits/vegetables at dinner, parents were more likely than their children to report frequent healthful parental role modeling (Figures 1, 2 and 3).
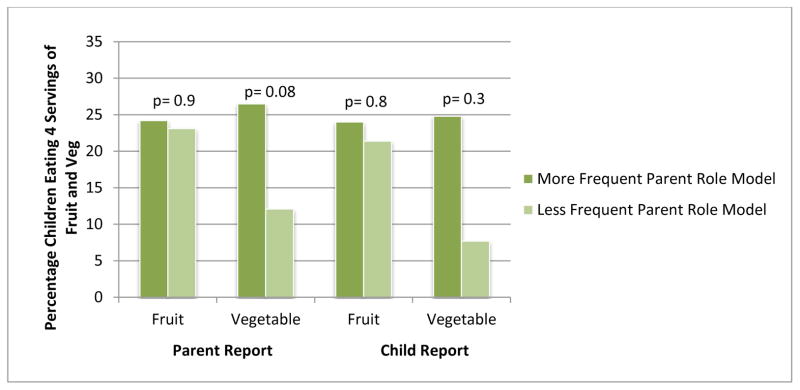
Mean parent role modeling scores were significantly higher among children who met daily fruit and vegetable recommendations (mean=19.3 ± 2.5) compared with children who did not meet recommendations (mean=18.2 ± 2.5, p=0.03). Child mean role modeling scores were similar with significantly higher scores among children who met daily recommendations (mean=19.5 ± 4.1) compared with children who did not (mean=17.7 ± 3.9, p=0.02). Similarly, parent and child report of parental role modeling fruits and vegetables were significantly and positively correlated with child fruit, vegetable and juice intake (r=0.21, p=0.008; r=0.20, p=0.01, respectively). Meeting recommended guidelines for daily fruit and vegetable consumption among children varied slightly by reporter and by whether the role modeling was at snack or dinner. As shown in Figure 4, parents who reported role modeling consumption of fruit at snack were significantly more likely to have children who met daily fruit and vegetable consumption recommendations; child report of this association was not statistically significant but in the same direction. Children who reported parental role modeling of vegetable consumption at snack were significantly more likely to meet daily fruit and vegetable consumption recommendations than those who did not (Figure 4); parental report of this association was not statistically significant but in the same direction. The percentage of children eating the recommended amount of fruits and vegetables did not differ by parental role modeling of fruits and vegetables at dinner regardless of reporter (Figure 5). As shown in Figure 6, children who reported parental role modeling of salad consumption at dinner were significantly more likely to meet recommendations for consumption of fruits and vegetables; parent report of this association was not statistically significant but in the same direction. The percentage of children eating the recommended amount of fruits and vegetables did not differ by parental role modeling of filling ½ their plate with fruits/vegetables at dinner, regardless of reporter (Figure 6).
Figure 4.

Percentage of children meeting recommendations for fruit and vegetable consumption by parental role modeling of fruit and vegetable consumption at snacks
Response options were dichotomized into “Usually/Always,” and “Sometimes, Hardly Ever, Never”
* Statistical significance at p<0.05
Figure 5.
Percentage of children meeting recommendations for fruit and vegetable consumption by parental role modeling of fruit and vegetable consumption at dinner
Response options were dichotomized into “Usually/Always,” and “Sometimes, Hardly Ever, Never”
* Statistical significance at p<0.05
Figure 6.

Percentage of children meeting recommendations for fruit and vegetable consumption by parental role modeling of salad consumption and filling ½ of plate with fruits and vegetables at dinner
Response options were dichotomized into “Usually/Always,” and “Sometimes, Hardly Ever, Never”
* Statistical significance at p<0.05
DISCUSSION
The present study aimed to examine the associations between parent and child reports of parental role modeling of fruit and vegetable consumption at snack and dinner and whether parental role modeling was associated with children meeting four daily servings of fruits and vegetables. This is the first study to utilize both parent and child reports of parental role modeling in this regard and we found that, in general, parents and children appeared similar in their reports of parental role modeling of healthful eating, although associations were statistically significant only for fruit and green salad at dinner. Parental role modeling may also increase the likelihood that children will meet dietary recommendations. Our findings suggest that children are aware of some of their parents’ eating behaviors and parents should capitalize on this opportunity to role model healthful dietary intake for their children, especially during snacks, where consumption of fruits and vegetables was shown to be very low.
Our findings of the importance of parental role modeling for snacks is particularly relevant given that the prevalence of children’s snacking has significantly increased over the last several decades (Piernas & Popkin, 2010). The largest snack consumption increases have been of salty snacks and candy with sugar-sweetened beverages and desserts contributing the most calories (Piernas & Popkin, 2010). Over the years, eating whole fruit at snacks has been replaced with fruit drinks, fruit juice and sports drinks (Piernas & Popkin, 2010). One previous study reported a significant association between parental role modeling at snacks and an increase in child snacking habits and child BMI. The association between parental role modeling at snacks and children’s fruit and vegetable consumption was non-significant (Hendy et al., 2009). However, snacking is an opportune time for kids to reduce consumption of low-nutrient, energy-dense foods and increase their servings of fruits and vegetables.
In addition to snacking, the family meal may also provide parents with an ideal opportunity to role model healthy eating behaviors which may facilitate better dietary intake among youth. Family meals have been shown to promote healthful eating (Hammons & Fiese, 2011) and be protective of overweight (Gable, Chang, & Krull, 2007), disordered eating (Neumark-sztainer, Eisenberg, & Fulkerson, 2008) and depressive symptoms (Fulkerson, Kubik, Story, Lytle, & Arcan, 2009; Hammons & Fiese, 2011). Although many parents report having family meals (Fulkerson, Neumark-Sztainer, & Story, 2006), it is unclear what proportion of parents actually sit and eat (i.e., role model healthful eating) with their children. Since role modeling appears to be related to children’s daily fruit and vegetable consumption, we recommend that parents use family meals as an opportunity to role model healthful food intake.
Associations between parent report of role modeling and children’s dietary intake of fruits and vegetables, as well as children’s increased likelihood of meeting dietary recommendations are similar to previous studies that used food frequency questionnaires (Cullen et al., 2001; De Bourdeaudhuij et al., 2008; Palfreyman et al., 2012; Reinaerts et al., 2007; Wind et al., 2006). Our findings extend this work by showing that children have similar perceptions as their parents regarding their parents’ role modeling behavior of fruit and green salads at dinner, indicating that children may be good reporters in this regard. Furthermore, our findings demonstrate that encouragement of parental role modeling of fruits and vegetables at snacks and salad at dinner are warranted and may increase healthful dietary habits among children. We speculate that children observe their parents eating behaviors at dinner more frequently than at snack and therefore, they have more similar perceptions of parental role modeling for dinner. The association between meeting recommended daily servings of fruits and vegetables and parental role modeling at snack may be influenced by what the parent has pre-planned for household snacks (e.g., fruits and vegetables are prepared and ready-to-eat in the refrigerator or are readily available whole). This hypotheses, however, is a speculation as it was not tested.
Although our study only found significant correlations between two of the six comparisons between parent and child report, this pattern is similar to previous studies that have reported mixed findings on the correlations between parent and child reports. Boutelle and colleagues (2001) examined the perceptions of parents and adolescents on the mealtime environment and adolescents’ eating and mealtime behaviors. Of eight parent and child reported constructs measured, only one was significantly correlated (frequency of arguments at dinner time). A study by Keery et al (2006) reported mixed findings on child and parent report of maternal weight control behaviors. Reports of maternal dieting based on mother report and daughter report resulted in non-significant correlations, whereas mother report and son report were significantly correlated. Additionally, parent and child report on child’s quality of life (QOL) found low correlations between parents and children with parents reporting higher QOL for their child than child self-report (Cremeens et al., 2006). However, significant correlations have been reported in previous research examining the relationship between parent and child report on child obsessive compulsive behaviors (Storch et al., 2006) and QOL for children with attention deficit hyperactivity disorder (Marques et al., 2013). Thus, our findings and those presented in previous research regarding correspondence between parent and child report indicate that correspondence varies by topic.
This study has limitations and strengths. Although our sample size was not particularly large, it was adequate for the association assessments in our planned data analyses. Also, social desirability may have influenced parent and child responses to reflect what they might perceive as normative parental role modeling of fruits and vegetables. However, we expected that children would report in a less socially desirable manner and they did, indicating that social desirability may not have influenced child reporting as much as their parent’s reporting. Another limitation includes the lack of a validated tool via parental report that captures parental role modeling of specific foods and at specific eating events (meals versus snacks). We adapted validated questions from Cullen et al. (2001) for parent self-report of role modeling for these specific foods and eating behaviors. It remains unclear as to whether parents or children are better reporters of behaviors, however, both parents and children provide information that is invaluable and should be taken into account (Eiser & Varni, 2013). Further research should be conducted to validate questionnaires on parent self-report of role modeling.
Despite limitations, our study is unique as it looked specifically at role modeling at snacks, as well as the evening meal using both survey items and psychometrically-sound scales. Health practitioners should encourage parents to role model healthful eating behaviors, especially fruits and vegetables, at both meals and snacks. Although not always statistically significant, children who had parents that role modeled eating fruits and vegetables were consistently more likely to meet daily recommended servings for these foods. Healthy parental role modeling is one strategy to attempt to increase children’s intakes of these foods.
HIGHLIGHTS.
Parents and children are similar in their reports of parental role modeling of food
Role modeling is related to children meeting fruit and vegetable recommendations
Parental role modeling of fruit at snack was more common than vegetables at snack
Parental role modeling of vegetables at dinner was more common than fruit at dinner
Acknowledgments
This study and publication was supported by Grant R01 DK08400 by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) at the National Institutes of Health (NIH). Its contents are solely the responsibility of the authors and do not necessarily represent the views of the NIH. Software support was also provided by the University of Minnesota’s Clinical and Translational Science Institute (Grant Number 1UL1RR033183 from the National Center for Research Resources (NCRR) of the National Institutes of Health (NIH)). The HOME Plus trial is registered with ClinicalTrials.gov Identifier: NCT01538615. We would also like to thank Olga Gurvich for her input and assistance with statistical analyses.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Baranowski T, Sprague D, Baranowski JH, Harrison JA. Accuracy of maternal dietary recall for preschool children. Journal of the American Dietetic Association. 1991;91(6):669–674. [PubMed] [Google Scholar]
- Bauer KW, Neumark-Sztainer D, Fulkerson JA, Hannan PJ, Story M. Familial correlates of adolescent girls’ physical activity, television use, dietary intake, weight, and body composition. The International Journal of Behavioral Nutrition and Physical Activity. 2011;8(1):25. doi: 10.1186/1479-5868-8-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bere E, Klepp K. Correlates of fruit and vegetable intake among Norwegian schoolchildren: Parental and self-reports. Public Health Nutrition. 2004;7(8):991–998. doi: 10.1079/PHN2004619. [DOI] [PubMed] [Google Scholar]
- Boutelle KN, Lytle LA, Murray DM, Birnbaum AS, Story M. Perceptions of the family mealtime environment and adolescent mealtime behavior: Do adults and adolescents agree? Journal of Nutrition Education. 2001;33(3):128–33. doi: 10.1016/s1499-4046(06)60181-4. [DOI] [PubMed] [Google Scholar]
- Burrows T, Golley RK, Khambalia A, McNaughton SA, Magarey A, Rosenkranz RR, Collins C. The quality of dietary intake methodology and reporting in child and adolescent obesity intervention trials: A systematic review. Obesity Reviews: An Official Journal of the International Association for the Study of Obesity. 2012;13(12):1125–1138. doi: 10.1111/j.1467-789X.2012.01022.x. [DOI] [PubMed] [Google Scholar]
- Collins CE, Watson J, Burrows T. Measuring dietary intake in children and adolescents in the context of overweight and obesity. International Journal of Obesity. 2010;34(7):1103–1115. doi: 10.1038/ijo.2009.241. [DOI] [PubMed] [Google Scholar]
- Cremeens J, Eiser C, Blades M. Factors influencing agreement between child self-report and parent proxy-reports on the pediatric quality of life inventory 4.0 (PedsQL) generic core scales. Health and Quality of Life Outcomes. 2006;4:58–58. doi: 10.1186/1477-7525-4-58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cullen KW, Baranowski T, Rittenberry L, Cosart C, Hebert D, de Moor C. Child-reported family and peer influences on fruit, juice and vegetable consumption: Reliability and validity of measures. Health Education Research. 2001;16(2):187–200. doi: 10.1093/her/16.2.187. [DOI] [PubMed] [Google Scholar]
- De Bourdeaudhuij I, te Velde S, Brug J, Due P, Wind M, Sandvik C, Klepp K. Personal, social and environmental predictors of daily fruit and vegetable intake in 11-year-old children in nine European countries. European Journal of Clinical Nutrition. 2008;62(7):834–841. doi: 10.1038/sj.ejcn.1602794. [DOI] [PubMed] [Google Scholar]
- De Bourdeaudhuij I, Yngve A, Velde SJ, Klepp K, Rasmussen M, Thorsdottir I, Brug J. Personal, social and environmental correlates of vegetable intake in normal weight and overweight 9 to 13-year old boys. International Journal of Behavioral Nutrition and Physical Activity. 2006;9:1–9. doi: 10.1186/1479-Received. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eiser C, Varni JW. Health-related quality of life and symptom reporting: Similarities and differences between children and their parents. European Journal of Pediatrics. 2013;172(10):1299–304. doi: 10.1007/s00431-013-2049-9. [DOI] [PubMed] [Google Scholar]
- Field AE, Colditz GA, Fox MK, Byers T, Serdula M, Bosch RJ, Peterson KE. Comparison of 4 questionnaires for assessment of fruit and vegetable intake. American Journal of Public Health. 1998;88(8):1216–1218. doi: 10.2105/ajph.88.8.1216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fulkerson JA, Kubik MY, Story M, Lytle L, Arcan C. Are there nutritional and other benefits associated with family meals among at-risk youth? The Journal of Adolescent Health: Official Publication of the Society for Adolescent Medicine. 2009;45(4):389–395. doi: 10.1016/j.jadohealth.2009.02.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fulkerson JA, Neumark-Sztainer D, Story M. Adolescent and parent views of family meals. Journal of the American Dietetic Association. 2006;106(4):526–532. doi: 10.1016/j.jada.2006.01.006. [DOI] [PubMed] [Google Scholar]
- Gable S, Chang Y, Krull JL. Television watching and frequency of family meals are predictive of overweight onset and persistence in a national sample of school-aged children. Journal of the American Dietetic Association. 2007;107(1):53–61. doi: 10.1016/j.jada.2006.10.010. [DOI] [PubMed] [Google Scholar]
- Gidding SS, Dennison BA, Birch LL, Daniels SR, Gillman MW, Gilman MW, Van Horn L. Dietary recommendations for children and adolescents: A guide for practitioners. Pediatrics. 2006;117(2):544–559. doi: 10.1542/peds.2005-2374. [DOI] [PubMed] [Google Scholar]
- Granner ML, Sargent RG, Calderon KS, Hussey JR, Evans AE, Watkins KW. Factors of fruit and vegetable intake by race, gender, and age among young adolescents. Journal of Nutrition Education and Behavior. 2004;36(4):173–180. doi: 10.1016/s1499-4046(06)60231-5. [DOI] [PubMed] [Google Scholar]
- Hammons AJ, Fiese BH. Is frequency of shared family meals related to the nutritional health of children and adolescents? Pediatrics. 2011;127(6):e1565–74. doi: 10.1542/peds.2010-1440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hendy HM, Williams KE, Camise TS, Eckman N, Hedemann A. The parent mealtime action scale (PMAS). Development and association with children’s diet and weight. Appetite. 2009;52(2):328–339. doi: 10.1016/j.appet.2008.11.003. [DOI] [PubMed] [Google Scholar]
- Keery H, Eisenberg ME, Boutelle K, Neumark-Sztainer D, Story M. Relationships between maternal and adolescent weight-related behaviors and concerns: The role of perception. Journal of Psychosomatic Research. 2006;61(1):105–11. doi: 10.1016/j.jpsychores.2006.01.011. [DOI] [PubMed] [Google Scholar]
- Kristjansdottir AG, Thorsdottir I, Bourdeaudhuij ID, Due P, Wind M, Klepp K. Determinants of fruit and vegetable intake among 11-year-old schoolchildren in a country of traditionally low fruit and vegetable consumption. International Journal of Behavioral Nutrition and Physical Activity. 2006;3(41) doi: 10.1186/1479-Received. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lorson BA, Melgar-Quinonez HR, Taylor CA. Correlates of fruit and vegetable intakes in US children. Journal of the American Dietetic Association. 2009;109(3):474–478. doi: 10.1016/j.jada.2008.11.022. [DOI] [PubMed] [Google Scholar]
- Lytle L, Nichaman M, Obarzanek E, Glovsky E, Montgomery D, Nicklas T, Feldman H. Validation of 24-hour recalls assisted by food records in third-grade children. Journal of the American Dietetic Association. 1993;93(12):1431–36. doi: 10.1016/0002-8223(93)92247-u. [DOI] [PubMed] [Google Scholar]
- Marques JC, Oliveira JA, Goulardins JB, Nascimento RO, Lima AM, Casella EB. Comparison of child self-reports and parent proxy-reports on quality of life of children with attention deficit hyperactivity disorder. Health and Quality of Life Outcomes. 2013;11(1):186–186. doi: 10.1186/1477-7525-11-186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Matheson DM, Robinson TN, Varady A, Killen JD. Do Mexican-American mothers’ food-related parenting practices influence their children’s weight and dietary intake? Journal of the American Dietetic Association. 2006;106(11):1861–1865. doi: 10.1016/j.jada.2006.08.004. [DOI] [PubMed] [Google Scholar]
- McPherson RS, Hoelscher DM, Alexander M, Scanlon KS, Serdula MK. Dietary assessment methods among school-aged children: Validity and reliability. Preventive Medicine. 2000;31(2):S11–S33. doi: 10.1006/pmed.2000.0631. [DOI] [Google Scholar]
- Musher-Eizenman D, Holub S. Comprehensive feeding practices questionnaire: Validation of a new measure of parental feeding practices. Journal of Pediatric Psychology. 2007;32(8) doi: 10.1093/jpepsy/jsm037. [DOI] [PubMed] [Google Scholar]
- Neumark-sztainer D, Eisenberg ME, Fulkerson JA. Family meals and disordered eating in adolescents. Arch Pediatr Adolesc Med. 2008;162(1):17–22. doi: 10.1001/archpediatrics.2007.9. [DOI] [PubMed] [Google Scholar]
- Palfreyman Z, Haycraft E, Meyer C. Development of the parental modelling of eating behaviours scale (PARM): Links with food intake among children and their mothers. Maternal & Child Nutrition. 2012:1–13. doi: 10.1111/j.1740-8709.2012.00438.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piernas C, Popkin BM. Trends in snacking among U.S. children. Health Affairs (Project Hope) 2010;29(3):398–404. doi: 10.1377/hlthaff.2009.0666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reinaerts E, de Nooijer J, Candel M, de Vries N. Explaining school children’s fruit and vegetable consumption: The contributions of availability, accessibility, exposure, parental consumption and habit in addition to psychosocial factors. Appetite. 2007;48(2):248–258. doi: 10.1016/j.appet.2006.09.007. [DOI] [PubMed] [Google Scholar]
- Storch EA, Murphy TK, Adkins JW, Lewin AB, Geffken GR, Johns NB, Goodman WK. The children’s Yale-Brown obsessive-compulsive scale: Psychometric properties of child- and parent-report formats. Journal of Anxiety Disorders. 2006;20(8):1055–70. doi: 10.1016/j.janxdis.2006.01.006. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans. 7. Washington DC: US Government Printing Office; 2010. [Google Scholar]
- Vereecken C, Ojala K, Delgrande Jordan M. Eating habits. In: Currie C, et al., editors. Young people’s health in context. HBSC study: International report from the 2001/02 survey. WHO policy series: Health policy for children and adolescents. 4. Copenhagen: World Health Organization; 2004. [Google Scholar]
- Wind M, de Bourdeaudhuij I, te Velde SJ, Sandvik C, Due P, Klepp K, Brug J. Correlates of fruit and vegetable consumption among 11-year-old Belgian-Flemish and Dutch schoolchildren. Journal of Nutrition Education and Behavior. 2006;38(4):211–221. doi: 10.1016/j.jneb.2006.02.011. [DOI] [PubMed] [Google Scholar]
- Young EM, Fors SW, Hayes DM. Associations between perceived parent behaviors and middle school student fruit and vegetable consumption. Journal of Nutrition Education and Behavior. 2004;36(1):2–8. doi: 10.1016/s1499-4046(06)60122-x. [DOI] [PubMed] [Google Scholar]