

Abstract
This update develops the actual therapeutic options in the management of the joint involvement of calcium pyrophosphate deposition disease (CPPD), basic calcium phosphate (BCP) deposition disease, hemochromatosis (HH), ochronosis, oxalosis, and Wilson's disease. Conventional pharmaceutical treatment provides benefits for most diseases. Anti-interleukine-1 (IL-1) treatment could provide similar results in CPPD than in gout flares. There is only limited evidence about the efficacy of preventive long-term colchicine intake, methotrexate, and hydroxychloroquine in chronic CPPD. Needle aspiration and lavage have satisfactory short and midterm results in BCP. Extracorporeal shockwave therapy has also proved its efficacy for high-doses regimes. Phlebotomy does not seem to have shown real efficacy on joint involvement in HH so far. Iron chelators' effects have not been assessed on joint involvement either, while IL-1 blockade may prove useful. NSAIDs have limited efficacy on joint involvement of oxalosis, while colchicine and steroids have not been assessed either. The use of nitisinone for ochronotic arthropathy is still much debated, but it could provide beneficial effects on joint involvement. The effects of copper chelators have not been assessed either in the joint involvement of Wilson's disease. NSAIDs should be avoided because of the liver affection they may worsen.
1. Introduction
New interest in crystal-induced arthropathies has developed over the last few years mainly through the new discoveries on gout pathophysiology and especially with the understanding of the inflammasome [1] which paved the way for new therapeutic options [2]. These breakthroughs in the field of gout have given a new insight into other crystal-induced arthropathies [3] and recent international guidelines have been produced for both the treatment of gout [4, 5] and calcium pyrophosphate deposition (CPPD) [6]. However, other crystal-induced rheumatisms such as the basic calcium phosphate (BCP) deposition disease [7] do not seem to have benefited from these new developments although they are widespread in clinical practice.
Rare conditions such as hemochromatosic arthropathy [8], ochronotic arthropathy [9], Wilson's disease [10], and oxalate crystal deposition disease [11] can lead to difficult clinical situations. Other joint deposition-related entities such as cholesterol crystal arthropathy, cryoglobulin-crystal arthropathy, liquid lipid crystals arthropathy, corticosteroid crystals-induced arthritis, or Charcot-Leyden crystals deposition are exceptional and therefore not developed here. Crystal-induced arthropathies, and more generally deposition diseases, share similarities in their treatment but also have distinctive features. To our knowledge, no recent global overview of the treatment of deposition-induced rheumatisms has been published in international literature [12, 13]. The main objective of this literature review is to provide a general update of the actual available treatments for deposition-induced arthropathies.
2. Methods
MEDLINE (medical literature analysis and retrieval system onLine) was used to pick out relevant articles up to January 2014. The keywords “treatment,” “management,” “guidelines,” “recommendations,” “colchicine,” “nonsteroidal anti-inflammatory drugs,” “Anakinra,” and “corticosteroids” were successively associated with the terms “deposition,” “crystal-induced,” “micro-crystalline,” “deposition,” “arthropathies,” or “arthritis” and with the name of the different deposition disease (e.g., for “calcium pyrophosphate deposition,” the key words “chondrocalcinosis,” “calcium pyrophosphate dehydrate crystals,” and “pseudogout” were also used). Initial article selection was based upon titles and abstracts. Cross-references from the found articles were also explored. Articles written out in languages other than English were studied for information when relevant but their data were not included in the review.
3. Results and Discussion
CPPD shows the highest number of publications amongst other deposition diseases which are the subject of around thirty to forty articles per year. Incidentally over the same time period, an average of 258 publications per year dealt with the issue of the management of gout (Figure 1).
Figure 1.
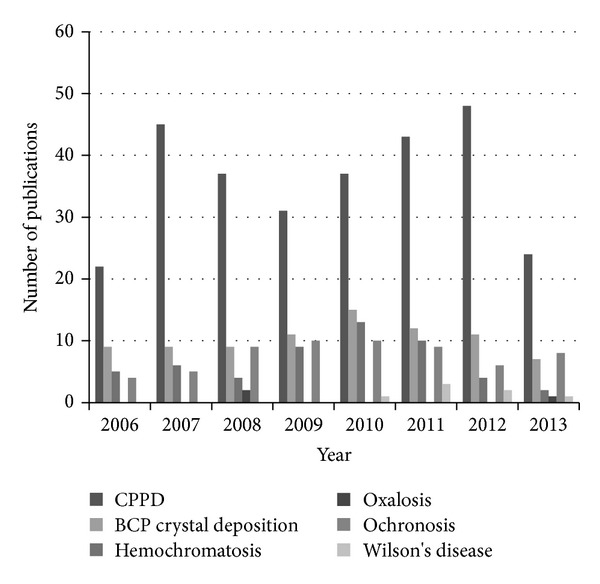
Number of publications per year related to management or treatment of each joint deposition disease from 2006 to 2013. CPPD: calcium pyrophosphate deposition; BCP: basic calcium phosphate.
3.1. Calcium Pyrophosphate Deposition (CPPD)
CPPD is widespread and its prevalence increases with age [14]. It is therefore fundamental to take cardiovascular and renal comorbidities into account, frequent amongst the elderly, when pharmacological treatment is considered. Relatively close to gout in terms of mechanisms and treatment habits, some new therapeutic options inspired by the discoveries in gout are emerging in the CPPD.
3.1.1. Treatment of CPPD Flares
The EULAR recently defined new guidelines for the management of CPPD [6]. Radiological findings of chondrocalcinosis do not motivate any particular management. Treatment should be limited to symptomatic CPPD. Local measures with ice bladders can provide some pain relief. Data is more limited regarding treatment of CPPD flares than of gout, but it is agreed that treatment of the crisis relies on the use of colchicine or NSAIDs. Considering the frequent side effects of colchicine and the renal impairment observed in this elderly population, no loading dose is recommended. Intra-articular injection of corticosteroids is an efficient and well tolerated therapeutic alternative. Oral or parenteral corticosteroids can be used in case of refractory flares. Retrospective data suggests satisfying efficacy of ACTH [15] with a rapid control of the symptoms after a 1 mg intramuscular injection of 13 out of 14 patients without any particular adverse effect. However, no information is given regarding the length of the follow-up. Evidence of the efficiency of anti-IL1 treatments (Anakinra) is growing but data is still limited and this option is not yet recommended, though it seems a good alternative in case of poor response or counterindications of NSAIDs, colchicine, and steroids, especially in case of polyarticular flare. The largest series included 16 cases among which two-thirds of the patients showed a satisfactory response [16]. Twelve patients were treated according to a protocol of daily subcutaneous administration of 100 mg Anakinra, the remaining four patients being treated from one week up to six months. Relapse occurred after treatment discontinuation in around one patient out of three, such results are similar to those observed in a case series of 40 gouty patients in which 13 cases experienced relapse [17]. Incidentally, 11 patients received simultaneous oral corticosteroids with various levels of prednisone and various prophylactic treatments were given to six patients after the flare, making it more difficult to assess the ability of Anakinra to cure the flare and prevent relapse.
3.1.2. Treatment for Chronic CPP Crystal Inflammatory Arthritis
Daily 1 mg intake of colchicine is sometimes used but there is too restricted data to prove its efficiency [18]. In fact, we can rely on single dated study including ten patients which showed a three-fold decrease of flares over a year of follow-up after they had received oral colchicine in comparison with the previous year without treatment [19]. Further evidence on a subset of patients affected with CPPD and knee osteoarthritis showed a symptomatic benefit after five months of a 1 mg colchicine daily intake added to initial treatment by piroxicam and intra-articular steroid injection compared to placebo [20]. However, only 74% of the patients included in the study had demonstrated CPPD crystals with synovial fluid examination. Although seldom used in clinical practice, the EULAR underlined the possible benefits of methotrexate [21] and hydroxychloroquine [22] in prophylaxis of CPPD flares. However, the study of 5 patients with an average follow-up of 6.2 years [21] upon which EULAR's recommendations for the use of methotrexate are based was contradicted by a report of three nonresponsive patients at 6 and 12 months [23]. A more recent observational study including ten patients suggested possible benefits of methotrexate; however, primary endpoints of the study were limited to a subjective assessment by the physician or the patient himself [24]. No further randomized controlled study has been performed so far. Guidelines regarding the use of hydroxychloroquine rely on a 6-month double-blind placebo-controlled study including 36 patients and showing some rapid benefits on the number of swollen and tender joints [22]. Magnesium intake in patients with hypomagnesaemia could reduce the number of flares and slow down radiographic progression of CPPD [25] as suggested in a dated placebo-controlled study including 38 patients [26]. Case reports suggest an inefficiency of Anakinra on chronic manifestations of CPPD [27] especially in the absence of systemic inflammation [28]. CPPD treatment is essentially medical but surgical treatment has been carried out successfully for the management of temporomandibular involvement [29, 30].
3.2. Basic Calcium Phosphate (BCP) Crystal Deposition Disease
Tendinitis and bursitis, especially of the shoulder, due to BCP crystal deposits are very frequent affections [7]. BCP deposits can also take place in intra-articular localizations associated with highly destructive arthritis, amongst which the most described form is the Milwaukee shoulder [31].
3.2.1. Treatment of Periarticular BCP Crystal Deposition Disease
In case of acute tendino-bursitis, symptomatic treatment with ice, joint rest, systemic NSAIDs, and periarticular corticosteroid injection is usually proposed [32]. Systemic corticosteroids at a dose of 30 mg per day of prednisone could be useful but this classical recommendation relies essentially on experts' clinical experience. In case of refractory tendinitis with large calcifications, ultrasound guided needle aspiration and lavage of the BCP deposit, followed by periarticular corticosteroid injection, show interesting results after one month, three months, and one year in both large nonrandomized controlled trials including 289 patients [33] and smaller randomized controlled studies [34]. This strong level of evidence suggests that needle aspiration and lavage should be proposed to patients with large calcifications refractory to conventional treatments. As expected, given the natural history of basic calcium deposits, no difference was found, however, on the long term (five and ten years), both groups of patients having benefited from a similar favorable outcome (Figure 2). The procedure can induce a painful flare due to the resorption of the calcification, which can justify a prophylaxis by colchicine or NSAIDs. Extracorporeal shockwave therapy could be used in case of failure of the preceding treatments as suggested by a randomized placebo-controlled trial conducted among 144 patients [35]. Reviews and meta-analyses suggest that proof of effectiveness of such treatment is limited to the shoulder and essentially with high-doses regime patients [36, 37]. Additional prospective studies using high-doses regime seem necessary to firmly recommend a more systematic use of shockwave therapy. Ultrasound therapy showed some possible benefits but too limited data is available apart from a prospective study of 63 patients which showed satisfactory results on the short term [38]. However, the sequence of administration of the ultrasound therapy was intense (daily administering) which is difficult to sustain in common practice. Yet, given the good tolerance profile of ultrasound therapy, although its efficacy when used only several times weekly, acceptable frequency in common practice, has not been thoroughly explored, this option seems interesting in a combined approach. Isolated data reports a possible benefit from IL-1 blockade. Indeed, an open-label study of five patients showed rapid control of the symptoms with relapse at the end of the treatment for a single patient [39]. Refractory calcifications to medical treatment responsible for recurrent flares can lead to surgical removal usually by arthroscopy [32, 40], but this option should be limited to situations where exhaustive medical treatment was ineffective.
Figure 2.

Radiologically guided aspiration of a calcification of the supraspinatus.
3.2.2. Treatment of Intra-Articular BCP Crystal Deposition Disease
Symptomatic treatment by analgesics and NSAIDs is usually proposed with the injection of intra-articular steroids. In the long term, treatment is similar to any destructive arthritis with physical preservation of the joint and eventually joint replacement. Tidal lavage of joints has been studied on a small group of ten patients with better results on patients with recent onset of Milwaukee shoulders [41]. However, the natural evolution of the disease remains unclear and the efficacy of such intervention is argued. A recent case report suggests possible efficacy of oral corticosteroids [42] (Table 1).
Table 1.
Therapeutic options for CPPD and BCP deposition diseases compared to those available in gout.
| Gout | CPPD | BCP | |
|---|---|---|---|
| Guidelines | ACR (2012) EULAR (2006) BSR (2007) |
EULAR (2011) | None |
| Local treatment of the flare | Intra-articular corticosteroid injection | Intra-articular corticosteroid injection | Periarticular corticosteroid injection-calcification aspiration-shockwave therapy |
| Efficacy of colchicine in flares | Yes | Yes | Limited data |
| Loading dose of colchicine | Yes | No | — |
| Efficacy of NSAIDs in flares | Yes | Yes | Yes |
| Efficacy of systemic corticosteroids in flares | Yes | Yes | Limited data |
| First-line preventive treatments | Xanthine oxydase inhibitors | None | None |
| Second-line preventive treatment | Uricosurics | Little data on colchicine | — |
| Third-line preventive treatment | Recombinant uricase | Little data on methotrexate and hydroxychloroquine | — |
| Efficacy of anti-interleukine-1 treatments | Established | Possible | Possible |
CPPD: calcium pyrophosphate deposition; BCP: basic calcium phosphate; ACR: american college of rheumatology; EULAR: European league against rheumatic diseases; BSR: British society for rheumatology.
3.3. Hereditary Hemochromatosis (HH)
HH is a cause of secondary CPPD but is also responsible for osteoarticular manifestations by itself which can reveal the disease [43]. Joint involvement is the first cause of the degradation of the quality of life of patients suffering from HH [44] (Figure 3).
Figure 3.

Radiological manifestations of the hands of hereditary hemochromatosis.
Limited data regarding treatment of the joint involvement of HH exist. Treatment relies essentially on symptomatic measures with the use of analgesics and NSAIDs. Colchicine can be useful during flares most probably due to CPPD-associated involvement. Intra-articular injections of corticosteroids can be used but no relevant published data exist on the issue. Some data suggest the possible efficiency of phlebotomy but its effects, if any, this is still highly debated, are unpredictable [45]. Indeed, in an observational study of 199 patients of whom 132 underwent phlebotomy, 13.6% of the patients reported improvement of joint pain, 65.9% reported no change, and 20.5% experienced a worsening of their articular symptoms after phlebotomy. This is further supported by the fact that iron depletion has itself a paradoxical increasing effect on collagen II levels indicative of cartilage degradation [46]. Thus, given the actual contradictory available data, phlebotomy should not be proposed for articular purposes. Iron chelators, deferasirox in particular, have shown some efficiency when phlebotomy is contraindicated [47] but effects on joint involvement have not been assessed. Furthermore, some recently reported serious adverse effects question the overall safety of the drug [48]. Interleukin-1 receptor antagonist has been shown to be effective in some patients with refractory hemochromatosis-related arthritis of the hands [49] but these data remain very limited. Natural evolution can lead to joint replacement [50].
3.4. Oxalate Crystal Deposition Disease
Skeletal involvement of oxalosis is found almost exclusively in evolved primary hyperoxaluria [12] (genetic overproduction of oxalate) as opposed to secondary oxalosis (essentially due to chronic kidney disease or increased intestinal absorption). Oxalosis is responsible for bone pain and pathological fractures whereas joint involvement shows acute arthritis (especially of the hands) similar to other crystal-induced joint flares [11, 51, 52] but also tenosynovitis of the feet.
3.4.1. Treatment
NSAIDs seem to have very limited efficacy on oxalate arthritis in case reports [52, 53]. No evidence on the effect of colchicine or steroids (intra-articular or systemic) has been reported. General treatment of the disease can bring some benefits on the joint involvement. Diet modifications have no impact on the course of primary hyperoxaluria. Pyridoxine intake can partially correct the enzymatic defect, but eventually treatment leads to liver-kidney transplantation, which can sometimes be delayed by higher hydric intake, alkaline citrate, magnesium, and orthophosphates [54]. Recent data have suggested a possible efficacy of Anakinra on oxalate nephropathy [55] in mice models but have not yet been assessed in joint involvement. Liver cell transplantation, gene therapy, and use of chemical chaperones are leads towards new therapeutic options [54].
3.5. Ochronotic Arthropathy
Ochronosis is due to a congenital defect in homogentisic acid oxidase leading to homogentisic acid accumulation and its deposition, especially inside joints [9], leading to chondrocyte death and matrix degradation. Spondyloarthritis-like spinal involvement usually precedes peripheral ochronotic arthropathy [56] (Figure 4).
Figure 4.

Ochronotic spinal deposits.
3.5.1. Treatment
Pain control is essential and difficult. It relies on both pharmaceutical (conventional analgesics, NSAIDs, and anticonvulsants) and physical measures [9, 57, 58]. Intra-articular injections of corticosteroids and hyaluronic acid have been used in case reports with varying immediate results but no sustained efficacy [59]. Joint replacement is sometimes needed. Spinal surgery for complications especially spinal stenosis must be carried out according to case reports [60].
No treatment to compensate the enzymatic defect has been developed so far. Diets excluding tyrosine and phenylalanine have no effect on developed ochronotic arthropathy. However, restricted protein intake associated with ascorbic acid ingestion could show some benefits. Treatment by nitisinone has shown some results in biological outcomes [61]. Yet, it remains debated especially since the only available randomized controlled trial including 40 patients, though well-tolerated, could not show any efficacy on the primary and secondary clinical outcomes [62]. However, some patients experienced clear improvement in joint symptoms and some authors suggest the need for further trials on nitisinone [63]. The study also suggested the importance of physical medicine. A recent animal model of alkaptonuria brought further evidence in favor of nitisinone for the prevention of the development of ochronotic arthropathy [64]. Liver [65] and renal [66] transplantation for other causes have shown beneficial effect on alkaptonuria according to case reports but with few or no details on the evolution of the joint involvement. New development of animal models could provide an interesting gateway for innovative therapeutic agents [67]. Recent advances in the understanding of ochronosis pathophysiology opened new therapeutic perspectives and suggest possible benefits of antioxidants [68].
3.6. Wilson's Disease
Wilson's disease (hepatolenticular degeneration) is responsible for visceral copper deposition. Articular manifestations are usually mild and affect large joints (especially knees) [10]. Precocious onset of osteoarthritis is also described.
There is no specific treatment of the joint involvement of Wilson's disease, apart from the copper chelators (D-penicillamine, zinc, and trientine) used to treat the general disease. Reviews showed a better efficacy for D-penicillamine though rheumatologic symptoms were not assessed and tolerance was poor [69]. Furthermore, D-penicillamine can be responsible for rheumatologic disorders by itself especially with cases of induced lupus [70]. The choice of treatment differs according to the disease's clinical presentation, mostly according to which hepatic or neurological symptoms prevail [71]. Diets restricted in copper seem unnecessary to the exception of liver and shellfish. Physical therapy is both beneficial on joint involvement and mostly on the neurological manifestations [72]. NSAIDs should be avoided due to the underlying liver affection; no data was found for colchicine and corticosteroids. There is one case report suggesting improvement of joint pain after liver transplantation [73] (Table 2).
Table 2.
Treatment of rare deposits-induced arthropathies.
| Specific treatment of the joint involvement | Efficacy of colchicine | Efficacy of NSAIDs | Efficacy of systemic corticosteroids | Efficacy of intra-articular corticosteroid injection | Efficacy of interleukin-1 blocking agents | Other measures improving joint condition | |
|---|---|---|---|---|---|---|---|
| Hereditary hemochromatosis | No | No data | Yes (limited data) | No data | No data | Yes | Phlebotomy (debated) |
| Oxalosis | No | No data | Poor | No data | No data | Possible | Pyridoxine—liver-kidney transplantation (no clear efficacy on arthropathy) |
| Ochronosis | No | No data | Yes (limited data) | No data | No data | No data | Limited protein intake and ascorbic acid—nitisinone (debated) |
| Wilson's disease | No | No data | No data | No data | No data | No data | Copper chelators (no clear efficacy on joint involvement)—liver transplantation (one case report) |
4. Conclusion
The global interest in gout has provided advances in the management of the other joint deposition diseases, especially regarding Il-1 blocking treatments that seem efficient in CPPD, BCP, and HH. However, rather surprisingly, given the high prevalence of these diseases (especially CPPD and BCP), most of the data discussed in this study about their treatment rely on case reports and case series with isolated controlled trials. Further randomized controlled trials would bring considerable progress in the therapeutic management of joint deposition diseases.
Conflict of Interests
The authors declare that they have no conflict of interests regarding the publication of this paper.
References
- 1.Martinon F, Pétrilli V, Mayor A, Tardivel A, Tschopp J. Gout-associated uric acid crystals activate the NALP3 inflammasome. Nature. 2006;440(7081):237–241. doi: 10.1038/nature04516. [DOI] [PubMed] [Google Scholar]
- 2.Burns CM, Wortmann RL. Gout therapeutics: new drugs for an old disease. The Lancet. 2011;377(9760):165–177. doi: 10.1016/S0140-6736(10)60665-4. [DOI] [PubMed] [Google Scholar]
- 3.Ottaviani S, Brunier L, Sibilia J, Maurier F, Ardizzone M, Wendling D, et al. Efficacy of anakinra in calcium pyrophosphate crystal-induced arthritis: a report of 16 cases and review of the literature. Joint Bone Spine. 2013;80(2):178–182. doi: 10.1016/j.jbspin.2012.07.018. [DOI] [PubMed] [Google Scholar]
- 4.Khanna D, Fitzgerald JD, Khanna PP, Bae S, Singh MK, Neogi T, et al. 2012 American College of Rheumatology guidelines for management of gout—part 1: systematic nonpharmacologic and pharmacologic therapeutic approaches to hyperuricemia. Arthritis Care & Research. 2012;64(10):1431–1446. doi: 10.1002/acr.21772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Khanna D, Khanna PP, Fitzgerald JD, Singh MK, Bae S, Neogi T, et al. 2012 American College of Rheumatology guidelines for management of gout—part 2: therapy and antiinflammatory prophylaxis of acute gouty arthritis. Arthritis Care & Research. 2012;64(10):1447–1461. doi: 10.1002/acr.21773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Zhang W, Doherty M, Pascual E, et al. EULAR recommendations for calcium pyrophosphate deposition—part II: management. Annals of the Rheumatic Diseases. 2011;70(4):571–575. doi: 10.1136/ard.2010.139360. [DOI] [PubMed] [Google Scholar]
- 7.Bosworth B. Calcium deposits in the shoulder and subacromial bursitis: a survey of 12, 122 shoulders. The Journal of the American Medical Association. 1941;116(22):2477–2482. [Google Scholar]
- 8.Carroll GJ, Breidahl WH, Olynyk JK. Characteristics of the arthropathy described in hereditary hemochromatosis. Arthritis Care & Research. 2012;64(1):9–14. doi: 10.1002/acr.20501. [DOI] [PubMed] [Google Scholar]
- 9.Phornphutkul C, Introne WJ, Perry MB, et al. Natural history of alkaptonuria. The New England Journal of Medicine. 2002;347(26):2111–2121. doi: 10.1056/NEJMoa021736. [DOI] [PubMed] [Google Scholar]
- 10.Quemeneur A-S, Trocello J-M, Ea H-K, Woimant F, Lioté F. Miscellaneous non-inflammatory musculoskeletal conditions. Musculoskeletal conditions associated with Wilson’s disease. Best Practice & Research Clinical Rheumatology. 2011;25(5):627–636. doi: 10.1016/j.berh.2011.10.021. [DOI] [PubMed] [Google Scholar]
- 11.Maldonado I, Prasad V, Reginato AJ. Oxalate crystal deposition disease. Current Rheumatology Reports. 2002;4(3):257–264. doi: 10.1007/s11926-002-0074-1. [DOI] [PubMed] [Google Scholar]
- 12.Rodnan GP. Treatment of the gout and other forms of crystal-induced arthritis. Bulletin on the Rheumatic Diseases. 1982;32(5):43–53. [PubMed] [Google Scholar]
- 13.Doherty M. Calcium pyrophosphate deposition disease and other crystal deposition diseases. Current Opinion in Rheumatology. 1990;2(5):789–796. doi: 10.1097/00002281-199002050-00017. [DOI] [PubMed] [Google Scholar]
- 14.Richette P, Bardin T, Doherty M. An update on the epidemiology of calcium pyrophosphate dihydrate crystal deposition disease. Rheumatology. 2009;48(7):711–715. doi: 10.1093/rheumatology/kep081. [DOI] [PubMed] [Google Scholar]
- 15.Daoussis D, Antonopoulos I, Yiannopoulos G, Andonopoulos AP. ACTH as first line treatment for acute calcium pyrophosphate crystal arthritis in 14 hospitalized patients. Joint Bone Spine. 2014;81(1):98–100. doi: 10.1016/j.jbspin.2013.05.006. [DOI] [PubMed] [Google Scholar]
- 16.Ottaviani S, Brunier L, Sibilia J, Maurier F, Ardizzone M, Wendling D, et al. Efficacy of anakinra in calcium pyrophosphate crystal-induced arthritis: a report of 16 cases and review of the literature. Joint Bone Spine. 2013;80(2):178–182. doi: 10.1016/j.jbspin.2012.07.018. [DOI] [PubMed] [Google Scholar]
- 17.Ottaviani S, Moltó A, Ea H-K, Neveu S, Gill G, Brunier L, et al. Efficacy of anakinra in gouty arthritis: a retrospective study of 40 cases. Arthritis Research & Therapy. 2013;15(5, article R123) doi: 10.1186/ar4303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Announ N, Guerne P-A. Treating difficult crystal pyrophosphate dihydrate deposition disease. Current Rheumatology Reports. 2008;10(3):228–234. doi: 10.1007/s11926-008-0037-2. [DOI] [PubMed] [Google Scholar]
- 19.Alvarellos A, Spilberg I. Colchicine prophylaxis in pseudogout. Journal of Rheumatology. 1986;13(4):804–805. [PubMed] [Google Scholar]
- 20.Das SK, Mishra K, Ramakrishnan S, et al. A randomized controlled trial to evaluate the slow-acting symptom modifying effects of a regimen containing colchicine in a subset of patients with osteoarthritis of the knee. Osteoarthritis and Cartilage. 2002;10(4):247–252. doi: 10.1053/joca.2002.0516. [DOI] [PubMed] [Google Scholar]
- 21.Chollet-Janin A, Finckh A, Dudler J, Guerne P-A. Methotrexate as an alternative therapy for chronic calcium pyrophosphate deposition disease: an exploratory analysis. Arthritis & Rheumatism. 2007;56(2):688–692. doi: 10.1002/art.22389. [DOI] [PubMed] [Google Scholar]
- 22.Rothschild B, Yakubov LE. Prospective 6-month, double-blind trial of hydroxychloroquine treatment of CPDD. Comprehensive Therapy. 1997;23(5):327–331. [PubMed] [Google Scholar]
- 23.Doan THT, Chevalier X, Leparc JM, Richette P, Bardin T, Forestier R. Premature enthusiasm for the use of methotrexate for refractory chondrocalcinosis: comment on the article by Chollet-Janin et al. Arthritis & Rheumatism. 2008;58(7):2210–2211. doi: 10.1002/art.23552. [DOI] [PubMed] [Google Scholar]
- 24.Andres M, Sivera F, Pascual E. Methotrexate is an option for patients with refractory calcium pyrophosphate crystal arthritis. Journal of Clinical Rheumatology. 2012;18(5):234–236. doi: 10.1097/RHU.0b013e3182611471. [DOI] [PubMed] [Google Scholar]
- 25.Wright GD, Doherty M. Calcium pyrophosphate crystal deposition is not always “wear and tear” or aging. Annals of the Rheumatic Diseases. 1997;56(10):586–588. doi: 10.1136/ard.56.10.586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Doherty M, Dieppe PA. Double blind, placebo controlled trial of magnesium carbonate in chronic pyrophosphate arthropathy. Annals of the Rheumatic Diseases. 1983;42:106–107. [Google Scholar]
- 27.Verhoeven F, Prati C, Godfrin-Valnet M, Guillot X, Wendling D. IL1 blockade in crystal-induced arthritis: impact of disease duration and the inflammatory syndrome. Comments on the article by Couderc M. et al. ‘Efficacy of anakinra in articular chondrocalcinosis’. Joint Bone Spine. 2013;80(1):115–116. doi: 10.1016/j.jbspin.2012.09.002. [DOI] [PubMed] [Google Scholar]
- 28.Couderc M, Mathieu S, Glace B, Soubrier M. Efficacy of anakinra in articular chondrocalcinosis: report of three cases. Joint Bone Spine. 2012;79(3):330–331. doi: 10.1016/j.jbspin.2011.12.017. [DOI] [PubMed] [Google Scholar]
- 29.Srinivasan V, Wensel A, Dutcher P, Newlands S, Johnson M, Vates GE. Calcium pyrophosphate deposition disease of the temporomandibular joint. Journal of Neurological Surgery Reports. 2012;73(1):6–8. doi: 10.1055/s-0032-1329190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wener MH. Destructive temporomandibular joint disease: also consider tophaceous voracious (hydroxy)apatite. The Journal of Rheumatology. 2009;36(2):453–454. doi: 10.3899/jrheum.080520. [DOI] [PubMed] [Google Scholar]
- 31.McCarty DJ, Halverson PB, Carrera GF. ‘Milwaukee shoulder’—association of microspheroids containing hydroxyapatite crystals, active collagenase, and neutral protease with rotator cuff defects. I. Clinical aspects. Arthritis & Rheumatism. 1981;24(3):464–473. doi: 10.1002/art.1780240303. [DOI] [PubMed] [Google Scholar]
- 32.Carcia CR, Scibek JS. Causation and management of calcific tendonitis and periarthritis. Current Opinion in Rheumatology. 2013;25(2):204–209. doi: 10.1097/BOR.0b013e32835d4e85. [DOI] [PubMed] [Google Scholar]
- 33.Serafini G, Sconfienza LM, Lacelli F, Silvestri E, Aliprandi A, Sardanelli F. Rotator cuff calcific tendonitis: short-term and 10-year outcomes after two-needle US-guided percutaneous treatment—nonrandomized controlled trial1. Radiology. 2009;252(1):157–164. doi: 10.1148/radiol.2521081816. [DOI] [PubMed] [Google Scholar]
- 34.de Witte PB, Selten JW, Navas A, et al. Calcific tendinitis of the rotator cuff: a randomized controlled trial of ultrasound-guided needling and lavage versus subacromial corticosteroids. The American Journal of Sports Medicine. 2013;41:1665–1673. doi: 10.1177/0363546513487066. [DOI] [PubMed] [Google Scholar]
- 35.Gerdesmeyer L, Wagenpfeil S, Haake M, et al. Extracorporeal shock wave therapy for the treatment of chronic calcifying tendonitis of the rotator cuff: a randomized controlled trial. Journal of the American Medical Association. 2003;290(19):2573–2580. doi: 10.1001/jama.290.19.2573. [DOI] [PubMed] [Google Scholar]
- 36.Speed C. A systematic review of shockwave therapies in soft tissue conditions: focusing on the evidence. British Journal of Sports Medicine. 2013 doi: 10.1136/bjsports-2012-091961. [DOI] [PubMed] [Google Scholar]
- 37.Ioppolo F, Tattoli M, di Sante L, et al. Clinical improvement and resorption of calcifications in calcific tendinitis of the shoulder after shock wave therapy at 6 months’ follow-up: a systematic review and meta-analysis. Archives of Physical Medicine and Rehabilitation. 2013;94(9):1699–1706. doi: 10.1016/j.apmr.2013.01.030. [DOI] [PubMed] [Google Scholar]
- 38.Ebenbichler GR, Erdogmus CB, Resch KL, et al. Ultrasound therapy for calcific tendinitis of the shoulder. The New England Journal of Medicine. 1999;340(20):1533–1538. doi: 10.1056/NEJM199905203402002. [DOI] [PubMed] [Google Scholar]
- 39.Zufferey P, So A. A pilot study of IL-1 inhibition in acute calcific periarthritis of the shoulder. Annals of the Rheumatic Diseases. 2013;72(3):465–467. doi: 10.1136/annrheumdis-2012-202380. [DOI] [PubMed] [Google Scholar]
- 40.Balke M, Bielefeld R, Schmidt C, Dedy N, Liem D. Calcifying tendinitis of the shoulder: midterm results after arthroscopic treatment. The American Journal of Sports Medicine. 2012;40(3):657–661. doi: 10.1177/0363546511430202. [DOI] [PubMed] [Google Scholar]
- 41.Epis O, Caporali R, Scirè CA, Bruschi E, Bonacci E, Montecucco C. Efficacy of tidal irrigation in Milwaukee shoulder syndrome. The Journal of Rheumatology. 2007;34(7):1545–1550. [PubMed] [Google Scholar]
- 42.Ornetti P, Vernier N, Fortunet C. Milwaukee shoulder syndrome affecting the elbow. Arthritis & Rheumatism. 2013;65(2):p. 538. doi: 10.1002/art.37774. [DOI] [PubMed] [Google Scholar]
- 43.Allen KJ, Gurrin LC, Constantine CC, et al. Iron-overload-related disease in HFE hereditary hemochromatosis. The New England Journal of Medicine. 2008;358(3):221–230. doi: 10.1056/NEJMoa073286. [DOI] [PubMed] [Google Scholar]
- 44.Richette P, Ottaviani S, Vicaut E, Bardin T. Musculoskeletal complications of hereditary hemochromatosis: a case-control study. The Journal of Rheumatology. 2010;37(10):2145–2150. doi: 10.3899/jrheum.100234. [DOI] [PubMed] [Google Scholar]
- 45.Sahinbegovic E, Dallos T, Aigner E, et al. Musculoskeletal disease burden of hereditary hemochromatosis. Arthritis & Rheumatism. 2010;62(12):3792–3798. doi: 10.1002/art.27712. [DOI] [PubMed] [Google Scholar]
- 46.Richette P, Eymard C, Deberg M, et al. Increase in type II collagen turnover after iron depletion in patients with hereditary haemochromatosis. Rheumatology. 2010;49(4):760–766. doi: 10.1093/rheumatology/kep429. [DOI] [PubMed] [Google Scholar]
- 47.Phatak P, Brissot P, Wurster M, et al. A phase 1/2, dose-escalation trial of deferasirox for the treatment of iron overload in HFE-related hereditary hemochromatosis. Hepatology. 2010;52(5):1671–1779. doi: 10.1002/hep.23879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Kontoghiorghes GJ. A record number of fatalities in many categories of patients treated with deferasirox: loopholes in regulatory and marketing procedures undermine patient safety and misguide public funds? Expert Opinion on Drug Safety. 2013;12(5):605–609. doi: 10.1517/14740338.2013.799664. [DOI] [PubMed] [Google Scholar]
- 49.Latourte A, Frazier A, Brière C, Ea H-K, Richette P. Interleukin-1 receptor antagonist in refractory haemochromatosis-related arthritis of the hands. Annals of the Rheumatic Diseases. 2013;72(5):783–784. doi: 10.1136/annrheumdis-2012-202738. [DOI] [PubMed] [Google Scholar]
- 50.Elmberg M, Hultcrantz R, Simard JF, Carlsson A, Askling J. Increased risk of arthropathies and joint replacement surgery in patients with genetic hemochromatosis. Arthritis Care & Research. 2013;65(5):678–685. doi: 10.1002/acr.21883. [DOI] [PubMed] [Google Scholar]
- 51.El Hage S, Ghanem I, Baradhi A, et al. Skeletal features of primary hyperoxaluria type 1, revisited. Journal of Children’s Orthopaedics. 2008;2(3):205–210. doi: 10.1007/s11832-008-0082-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Reginato AJ, Ferreiro Seoane JL, Alvarez CB. Arthropathy and cutaneous calcinosis in hemodialysis oxalosis. Arthritis & Rheumatism. 1986;29(11):1387–1396. doi: 10.1002/art.1780291112. [DOI] [PubMed] [Google Scholar]
- 53.Lorenz EC, Michet CJ, Milliner DS, Lieske JC. Update on oxalate crystal disease. Current Rheumatology Reports. 2013;15(article 340) doi: 10.1007/s11926-013-0340-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Hoppe B. An update on primary hyperoxaluria. Nature Reviews Nephrology. 2012;8:467–475. doi: 10.1038/nrneph.2012.113. [DOI] [PubMed] [Google Scholar]
- 55.Mulay SR, Kulkarni OP, Rupanagudi KV, Migliorini A, Darisipudi MN, Vilaysane A, et al. Calcium oxalate crystals induce renal inflammation by NLRP3-mediated IL-1β secretion. The Journal of Clinical Investigation. 2013;123(1):236–246. doi: 10.1172/JCI63679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Mannoni A, Selvi E, Lorenzini S, et al. Alkaptonuria, ochronosis, and ochronotic arthropathy. Seminars in Arthritis and Rheumatism. 2004;33(4):239–248. doi: 10.1053/s0049-0172(03)00080-5. [DOI] [PubMed] [Google Scholar]
- 57.Ranganath LR, Jarvis JC, Gallagher JA. Recent advances in management of alkaptonuria (invited review, best practice article) Journal of Clinical Pathology. 2013;66(5):367–373. doi: 10.1136/jclinpath-2012-200877. [DOI] [PubMed] [Google Scholar]
- 58.Perry MB, Suwannarat P, Furst GP, Gahl WA, Gerber LH. Musculoskeletal findings and disability in alkaptonuria. The Journal of Rheumatology. 2006;33(11):2280–2285. [PubMed] [Google Scholar]
- 59.Toussirot É, Aquaron R. Short-term efficacy of hyaluronic acid joint injections in a case of ochronotic arthropathy. Journal of Clinical Rheumatology. 2013;19(3):152–153. doi: 10.1097/RHU.0b013e318289e7fa. [DOI] [PubMed] [Google Scholar]
- 60.Manoj Kumar RV, Rajasekaran S. Spontaneous tendon ruptures in alkaptonuria. Journal of Bone and Joint Surgery B. 2003;85(6):883–886. [PubMed] [Google Scholar]
- 61.Suwannarat P, O’Brien K, Perry MB, et al. Use of nitisinone in patients with alkaptonuria. Metabolism: Clinical and Experimental. 2005;54(6):719–728. doi: 10.1016/j.metabol.2004.12.017. [DOI] [PubMed] [Google Scholar]
- 62.Introne WJ, Perry MB, Troendle J, et al. A 3-year randomized therapeutic trial of nitisinone in alkaptonuria. Molecular Genetics and Metabolism. 2011;103(4):307–314. doi: 10.1016/j.ymgme.2011.04.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Cox TM. JIMD Reports—Case and Research Reports, 2012/2. Vol. 5. Berlin, Germany: Springer; 2012. Alkaptonuria: leading to the treasure in exceptions; pp. 49–57. (JIMD Reports). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Preston AJ, Keenan CM, Sutherland H, Wilson PJ, Wlodarski B, Taylor AM, et al. Ochronotic osteoarthropathy in a mouse model of alkaptonuria, and its inhibition by nitisinone. Annals of the Rheumatic Diseases. 2014;73(1):284–289. doi: 10.1136/annrheumdis-2012-202878. [DOI] [PubMed] [Google Scholar]
- 65.Kobak AC, Oder G, Kobak Ş, Argin M, Inal V. Ochronotic arthropathy: disappearance of alkaptonuria after liver transplantation for hepatitis B-related cirrhosis. The Journal of Clinical Rheumatology. 2005;11(6):323–325. doi: 10.1097/01.rhu.0000191157.25894.55. [DOI] [PubMed] [Google Scholar]
- 66.Introne WJ, Phornphutkul C, Bernardini I, McLaughlin K, Fitzpatrick D, Gahl WA. Exacerbation of the ochronosis of alkaptonuria due to renal insufficiency and improvement after renal transplantation. Molecular Genetics and Metabolism. 2002;77(1-2):136–142. doi: 10.1016/s1096-7192(02)00121-x. [DOI] [PubMed] [Google Scholar]
- 67.Taylor AM, Preston AJ, Paulk NK, Sutherland H, Keenan CM, Wilson PJM, et al. Ochronosis in a murine model of alkaptonuria is synonymous to that in the human condition. Osteoarthritis and Cartilage. 2012;20(8):880–886. doi: 10.1016/j.joca.2012.04.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Spreafico A, Millucci L, Ghezzi L, Geminiani M, Braconi D, Amato L, et al. Antioxidants inhibit SAA formation and pro-inflammatory cytokine release in a human cell model of alkaptonuria. Rheumatology. 2013;52(9):1667–1673. doi: 10.1093/rheumatology/ket185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Wiggelinkhuizen M, Tilanus MEC, Bollen CW, Houwen RHJ. Systematic review: clinical efficacy of chelator agents and zinc in the initial treatment of Wilson disease. Alimentary Pharmacology and Therapeutics. 2009;29(9):947–958. doi: 10.1111/j.1365-2036.2009.03959.x. [DOI] [PubMed] [Google Scholar]
- 70.Uetrecht J. Current trends in drug-induced autoimmunity. Autoimmunity Reviews. 2005;4(5):309–314. doi: 10.1016/j.autrev.2005.01.002. [DOI] [PubMed] [Google Scholar]
- 71.Kodama H, Fujisawa C, Bhadhprasit W. Inherited copper transport disorders: biochemical mechanisms, diagnosis, and treatment. Current Drug Metabolism. 2012;13(3):237–250. doi: 10.2174/138920012799320455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Brewer GJ, Askari FK. Wilson’s disease: clinical management and therapy. Journal of Hepatology. 2005;42(1):S13–S21. doi: 10.1016/j.jhep.2004.11.013. [DOI] [PubMed] [Google Scholar]
- 73.Nagral A, Sathe K. Reversal of severe Wilson arthropathy by liver transplantation. Indian Pediatrics. 2011;48(5):406–407. [PubMed] [Google Scholar]