

Abstract
BACKGROUND
Colorectal cancer is a common, deadly disease with different incidence rates in different parts of the world. The present study aims to investigate the clinical presentations, colonoscopic findings, and family history of colorectal cancer in the city of Khorramabad, Iran.
METHODS
This cross-sectional study, conducted in 2013, included 112 patients diagnosed with colorectal cancer by colonoscopy with pathological confirmation in addition to 112 individuals matched with patients for age and gender. Controls were chosen from the outpatients admitted to the Skin and Eye Clinics of ShohadaAshayer Hospital in Khorramabad who had no gastrointestinal diseases. A self-generated questionnaire was used to assess family history of smoking and gastrointestinal cancer history in immediate relatives of subjects from both groups. Fisher’s exact test and odds ratios (OR) were used to analyze the data.
RESULTS
Based on the findings of this study, the most common clinical presentation in the patients was abdominal pain (67.9%). The sigmoid colon (40%) was the most common anatomical site of the tumor in men; the rectum (34.6%) and sigmoid colon (34.6%) were the most common sites in women, which was not statistically significant (p=0.21). There were 11 (19.6%) patients and 2 (3.6%) individuals in the control group who reported a history of colorectal cancer in their immediate relatives, which was statistically significant (p=0.008).
CONCLUSION
In this study, left-sided colon cancer was more common. Subjects with colon cancer had more positive FHx. This indicated that genetic factors, in addition to environmental factors, could increase the incidence of colorectal cancer in a community. A better identification of these factors would result in better control and management of this disease.
Keywords: Colorectal cancer, Family history, Clinical presentations, Khorramabad
INTRODUCTION
Today, in countries that have adopted the Western lifestyle, approximately half of the deaths are due to cardiovascular diseases, and one-fourth due to cancers. Cancer, as a major problem in today’s world, has affected public health and governments.1 Colorectal cancer is one of the most important cancers and the fourth most common in the world, with an estimation of 783,000 new cases per year.1 This disease is the third leading cause of death from cancer in the world.2 The number of new cases of this disease (500,000 new cases per year) has increasingly risen since 1975.1
The epidemiological characteristics of colorectal cancer vary in different parts of the world.3 While the annual incidence of in Europe and North America is approximately 30 to 50 cases per 100,000 people, the rate in the Middle East is estimated to be between 3 to 7 cases per 100,000 people.4 According to the annual report of the Cancer Center related to the Disease Management Center in Iran, the incidence of this cancer has increased over the last 25 years in Iran.5
Since the epidemiological characteristics of the disease are different in various geographical areas and because performing different studies in this field can help in developing comprehensive screening programs and providing early diagnosis of the disease, therefore the present study aims to investigate the clinical presentations, colonoscopic findings, and family history of colorectal cancer in the city of Khorramabad, Western Iran.
MATERIALS AND METHODS
This cross-sectional study, conducted in 2013, included patients admitted to Shohada Ashayer Hospital and a subspecialty private clinic for gastrointestinal diseases in Khorramabad, Western Iran, who were diagnosed with colorectal cancer through colonoscopy and pathological confirmation. The study included only the patients who resided in the city and its suburban areas. The census sampling was applied to select the patients, which resulted in the inclusion of 112 patients diagnosed with colorectal cancer. The control group included 112 individuals matched for age and gender with the patients, who were selected from outpatients admitted to the Skin and Eye Clinics of the hospital who had no history of any chronic physical or mental diseases.
The data collection tool was a self-designed questionnaire that consisted of demographic information along with questions regarding family history of smoking and family history of gastrointestinal polyps and cancers among immediate relatives. Total endoscopy was performed for most patients, and only sigmoidoscopy was performed in some patients due to blockages in the colon. All the diagnostic analyses were performed by one subspecialist in gastrointestinal diseases. In the control group, we collected data regarding history of smoking and alcohol consumption along with family history of colorectal cancer. Written informed consents to participate in the study were obtained from all patients. The data were analyzed using SPSS version 19 software. Descriptive statistics, Fisher’s exact test and the chi-square test were used for data analysis. Odds ratio (OR) was applied to analyze the intensity of the relationship between family history of gastrointestinal diseases and individual history of colorectal polyps with the disease incidence, with a confidence interval (CI) of 95%.
RESULTS
In this study, 112 patients with colorectal cancer and 112 controls were studied in a year (2013). The mean age of the patients was 52.2±15.3 years and the mean age of the individuals in the control group was 51.8±12.8 years, with no statistically significant difference between the two groups. Moreover, 53.6% of all the patients were male, which showed no statistically significant difference between the two groups in terms of gender. The youngest patient with colorectal cancer was 24 years old and the oldest was 88 years old. The mean age of female patients with colorectal cancer was 47.3±13.2 years and the mean age of the male patients with colorectal cancer was 56.5±16 years, which was statistically significant based on the independent t-test (p=0.022).
Most patients (83.9%) were married and most (48.2%) had an educational level of junior high school and lower (Table 1). Moreover, 35.7% of the patients were housewives, 17.9% were self-employed, 71.4% were urban residents, and 64.3% belonged to the Lur ethnic group (Table 1). No statistically significant differences were found between the two groups in terms of frequency distribution of the mentioned variables. A total of 38 (33.9%) patients had a history of regular smoking while this history was reported by 16 (14.3%) in the control group, which was statistically significant according to the chi-square test results (p=0.015). Also, an OR of 3.08 with a CI of 2.21-6.81 was found regarding the intensity of the relationship between regular smoking and the incidence of colorectal cancer.
Table 1. Frequency distribution of demographic characteristics of patients with colorectal cancer in Khorramabad, Iran.
| Variable | Absolute frequency(N) | Relative frequency(%) | |
| Age (years) | <40 | 30 | 26.8 |
| ≥40 | 82 | 73.2 | |
| Gender | Male | 60 | 53.6 |
| Female | 52 | 46.4 | |
| Marital status | Married | 97 | 83.9 |
| Unmarried | 8 | 7.2 | |
| Other | 10 | 8.9 | |
| Education | Illiterate | 22 | 19.6 |
| Junior high school or lower | 54 | 48.2 | |
| Senior high school | 18 | 16.1 | |
| University | 18 | 16.1 | |
| Occupation | Unemployed | 2 | 1.8 |
| Employees | 12 | 10.7 | |
| Workers | 10 | 8.9 | |
| Self-employed | 20 | 17.9 | |
| Housewives | 40 | 35.7 | |
| Farmers | 12 | 10.7 | |
| Other | 16 | 14.3 | |
| Place of residence | Urban | 80 | 71.4 |
| Rural | 32 | 28.6 | |
| Ethnicity | Lur | 78 | 69. 6 |
| Lak | 34 | 30.4 |
Regarding family history of colorectal cancer in immediate relatives, the results showed that 22 (19.6%) patients and 4 (3.6%) individuals in the control group reported a positive family history, which was a statistically significant difference (p=0.008). An OR of 6.6 (CI=3.39-9.33) was found for the intensity of the relationship between a positive family history of colorectal cancer in immediate relatives and the incidence of the cancer. In addition, 20 (17.9%) patients had a history of colorectal polyps in their immediate relatives.
Colonoscopic examinations revealed that most tumors (37.5%) were located in the sigmoid colon, followed by the rectum (32.1%), the cecum (12.5%), and the ascending and descending colons (8.9% each). Pathologically, most tumors (45.2%) were well-differentiated adenocarcinomas (Figure 1).
Fig. 1.
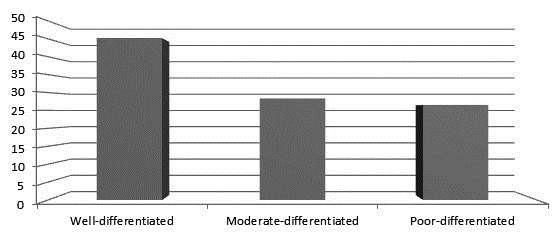
Frequency distribution of degree of differentiation of colorectal cancer in patients.
The most common clinical presentations of the disease among study patients were abdominal pain (67.9%), rectal bleeding (57.1%), weight loss (41.1%), and constipation (41.1%)(Table 2).
Table 2. Frequency distribution of anatomical sites of colorectal cancer in the patients in terms of age, sex, ethnicity, smoking history, and history of colorectal cancer in immediate relatives.
| Anatomical site of the tumor |
Rectum
N (%) |
Ascending colon
N (%) |
Descending colon
N (%) |
Sigmoid colon
N (%) |
Cecum
N (%) |
Total
N (%) |
p -value | |
| Gender | Male | 18 (30) | 4 (6.7) | 2 (3.3) | 24 (40) | 12 (20) | 60 (100) | 0.21 |
| Female | 18 (34.6) | 6 (11.5) | 8 (15.4) | 18 (34.6) | 2 (3.8) | 52 (100) | ||
| Age (years) | <40 | 12 (40) | 2 (6.7) | 2 (6.7) | 12 (40) | 2 (6.7) | 30 (100) | 0.65 |
| ≥40 | 12 (29.3) | 8 (9.8) | 8 (9.8) | 30 (36.6) | 12 (14.6) | 82 (100) | ||
| Ethnicity | Lur | 18 (23.1) | 8 (10.3) | 6 (7.7) | 40 (51.3) | 6 (7.7) | 78 (100) | 0.045 |
| Lak | 16 (47.1) | 2 (5.9) | 2 (5.9) | 6 (17.6) | 8 (23.5) | 34 (100) | ||
| Regular smoking | Yes | 10 (26.3) | 2 (5.3) | 4 (10.5) | 18 (47.4) | 4 (10.5) | 38 (100) | 0.84 |
| No | 24 (32.4) | 8 (10.8) | 4 (5.4) | 28 (37.8) | 10 (13.5) | 74 (100) | ||
| Family history of colorectal cancer in immediate relatives | Yes | 6 (27.3) | 0 (0) | 2 (9.1) | 12 (54.5) | 2 (9.1) | 22 (100) | 0.72 |
| No | 28 (31.1) | 10 (11.1) | 6 (6.7) | 34 (37.8) | 12 (13.3) | 90 (100) | ||
* Statistical test
** Level of significance: < 0.05
The most common anatomical sites of the tumor were the sigmoid colon in men (40%) and the rectum and sigmoid colon in women (34.6% each).
The most common anatomical sites of the tumor were the rectum and the sigmoid colon (40% each) in the age group of <40 years and the sigmoid colon (36.6%) in the age group of ≥40 years. The difference in the anatomical distribution of the tumor was not statistically significant in terms of age (p=0.65; Table 3).
Table 3. Comparison of frequency distributions of regular smoking, regular alcohol consumption, and family history of colorectal cancer in immediate relatives in the patients and the control group.
|
Patients
N (%) |
Controls
N (%) |
p -value | Odds ratio (OR) | Confidence interval (CI) | ||
| Regular smoking | Yes | 38 (33.9) | 16 (14.3) | 0.015 | 3.08 | 2.21-6.81 |
| No | 74 (66.1) | 96 (85.7) | ||||
| Total | 112 (100) | 112 (100) | ||||
| Regular alcohol consumption | Yes | 8 (7.1) | 2 (1.8) | 0.17 | 4.23 | 0.45-8.14 |
| No | 104 (92.9) | 110 (98.2) | ||||
| Total | 112 (100) | 112 (100) | ||||
| History of colorectal cancer in immediate relatives | Yes | 22 (19.6) | 4 (3.6) | 0.008 | 6.6 | 3.39-9.33 |
| No | 90 (80.4) | 108 (96.4) | ||||
| Total | 112 (100) | 112 (100) |
* Statistical test
** Level of significance: < 0.05
In terms of the relationship between the anatomical location of the tumor and ethnicity, the most common sites of involvement were the sigmoid colon (51.3%) in the Lur patients and the rectum (47.1%) in the Lak patients. This difference was statistically significant(p=0.045).
DISCUSSION
The present study has aimed to investigate the clinical presentations, colonoscopic findings, and family history of colorectal cancer in the city of Khorramabad in Lorestan Province, Iran. Since Shohada Ashayer Hospital is the only referral center for subspecialty health services in gastrointestinal diseases in the province, the information obtained by this study is of value.
The mean age of the patients in our study was higher than the mean ages in the studies conducted in Kenya (mean age of 49.7 years)6 and Egypt (mean age of 51 years),7 but lower than the mean ages in the studies carried out in China (mean age of 55.3 years),8 Jamaica (mean age of 65.5 years),9 and Hungary (mean age of 65.2±12.5 years).10 Studies conducted in Iran have reported different statistics so that that the mean age of the patients in our study was lower than the mean ages in studies conducted in Sari and Arak, but higher than the mean age in a study performed in Tehran.11-13
Most patients in our study were male, which was similar to the results of the studies conducted in China,8 Hungary,10 Tehran,11 Gorgan,14 Sari,14 Yazd,15 and Arak.1 However, 57.82% of the patients in a study in Jamaica were female.9 In our study, there was a statistically significant difference between the mean ages of women and men with colorectal cancer. According to the reference books, the mean ages for diagnosis of colorectal cancer have been reported as 63 (men) and 62 (women) years,16 which are higher than the mean ages in our study. This difference could be attributed to the younger community in Lorestan Province or to family history of colorectal cancer.
In the present study, 33.9% of patients and 14.3% of individuals in the control group reported a regular smoking history, which showed a statistically significant difference. This finding was consistent with the results of a study conducted on colorectal cancer in Spain from 1951 to 2006. The results indicated a positive association between smoking and the incidence and mortality of colorectal cancer.17 On the other hand, the results of a case-control study in the US showed no positive association between smoking and colorectal cancer.18 Of note, the latest reference books of internal medicine have mentioned a positive relationship between smoking and colorectal cancer.
With respect to family history of colorectal cancer in immediate relatives, the results showed that 19.6% of patients and 3.6% of individuals in the control group reported a family history of the disease in their immediate relatives, which was statistically significant. This has indicated that genetic factors, in addition to environmental factors, can increase the incidence of colorectal cancer in a community. In other words, family history can be a key to diagnosis and the best way to identify people at risk. Many studies have confirmed the association between genetic factors and colorectal cancer risk; some of these studies have reported a 10%-15% family history of colorectal cancer in patients with colorectal cancer and 4%-10% in non-patients.19,20
In the present study, we have reported the most common anatomical sites of the tumor to be the sigmoid colon, the rectum, and the cecum, respectively. According to the reference books, the distribution and pattern of the tumor in the colon and rectum vary so that the right-side cancers are more prevalent in low-risk populations and the left-side cancers are more prevalent in high-risk populations.16
In our study, as with other studies in Jamaica,11 Arak,13 Gorgan,14 Yazd,15 and Tehran,21 adenocarcinoma was found to be the most common pathology.
The most common clinical presentations in the patients of this study were abdominal pain, rectal bleeding, weight loss, and constipation. Findings from the studies conducted in Jamaica,7 Gorgan,14 and Tehran21 also reported these clinical symptoms as the most common with slight differences in the percentage of each symptom. However, rectorrhagia was reported as the most common symptom of colorectal cancer in a study conducted in Arak by Fateh and Amini.13 The symptoms of colorectal and rectal cancers are non-specific, and usually occur when the cancer is locally advanced. The first classic symptoms of colorectal cancer include a change in bowel habits and rectal bleeding. Obstruction is usually caused by large tumors, and is suggestive of the disease progression. However, patients may be asymptomatic, or present with anemia, weight loss, and unjustifiable anorexia.22
Finally, given the increasing incidence of colorectal cancer in Iran, particularly in Lorestan Province, it is recommended that further complementary studies should be conducted to identify the underlying and predisposing factors of colorectal cancer. A better identification of these factors can result in better con trol and management of the disease.
ACKNOWLEGMENTS
We hereby appreciate the sincere help of the hard-working staff of the Colonoscopy and Endoscopy Wards of Shohada Ashayer Hospital in Khorramabad for helping us in conducting the present study.
CONFLICT OF INTEREST
The authors declare no conflict of interest related to this work.
Please cite this paper as:
Ghanadi K, Anbari K, Obeidavi Z, Pournia Y. Characteristics of Colorectal Cancer in Khorramabad, Iran during 2013. Middle East J Dig Dis 2014;6:81-6.
References
- 1.Boyle P, Langman J S. ABC of colorectal cancer: Epidemiology. BMJ. 2000;321:805–8. doi: 10.1136/bmj.321.7264.805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Parkin DM. Global cancer statistics in the year 2000. Lancet Oncol. 2001;2:533–43. doi: 10.1016/S1470-2045(01)00486-7. [DOI] [PubMed] [Google Scholar]
- 3.Ansari R, Mahdavinia M, Sadjadi A. Incidence and age distribution of colorectal cancer in Iran: Results of a population-based cancer registry. Cancer Letters. 2006;240:143–7. doi: 10.1016/j.canlet.2005.09.004. [DOI] [PubMed] [Google Scholar]
- 4.Stewart BW, Kleihues P. World Cancer Report, International Agency for Research on Cancer. Lyon. 2003 doi: 10.1016/s0140-6736(03)12634-7. [DOI] [PubMed] [Google Scholar]
- 5.Mosavi-Jarrahi A, Zali MR, Mohagheghi MA. Changes in GI Cancer Incidence Iran: last 25 years. Institute cancer central. 2005 [Google Scholar]
- 6.Saidi H, Nyaim EO, Githaiga JW, Karuri D. CRC surgery trends in Kenya, 1993- 2005. World J Surg. 2008;32:217–23. doi: 10.1007/s00268-007-9301-2. [DOI] [PubMed] [Google Scholar]
- 7.El-Bolkainy TN, Sakr MA, Nouh AA, El-Din NH. A comparative study of rectal and colonic carcinoma: demographic, pathologic and TNM staging analysis. J Egypt Natl Canc Inst. 2006;18:258–63. [PubMed] [Google Scholar]
- 8.Xu AG, Jiang B, Zhong XH, Liu JH. Clinical epidemiological characteristics of 3870 cases of colorectal cancers in Guangdong region. Zhonghua Nei Ke Za Zhi. 2006;45:9–12. [PubMed] [Google Scholar]
- 9.McFarlane ME, Rhoden A, Fletcher PR, Carpenter R. Cancer of the colon and rectum in a Jamaican population: diagnostic implications of the changing frequency and subsite distribution. West Indian Med J. 2004;53:170–3. [PubMed] [Google Scholar]
- 10.Fuszek P, Horváth HC, Speer G, Papp J, Haller P, Halász J. et al. Change in location of colorectal cancer in Hungarian patients between 1993- 2004. Orv Hetil. 2006;147:741–6. [PubMed] [Google Scholar]
- 11.Jalali SM, Kordjazi ID, Jalali SA. Epidemiological characteristic of colorectal cancer in patients referred to Imam Khomeini hospital during (1981-2001) J Iran Univ Med Sci. 2005;11:723–30. [Google Scholar]
- 12.TirgarFakhari H, Janbabaei GH, Bari Z, Eshghi F. The epidemiologic and clinical pathologic characteristic of colorectal cancer from 1999 to 2007 in Sari, Iran. J Mazandaran Univ Med Sci. 2009;18:58–66. [Google Scholar]
- 13.Fateh SH, Amini M. An epidemiologic study of colorectal cancer in Arak During 1994-2004. Iran J Surgery. 2008;16:11–7. [Google Scholar]
- 14.Semnani SH, Kazeminezhad V, Abdelahi N. The Epidemiological aspect of colorectal cancer in Gorgan. J Gorgan Univ Med Sci 2003- 2004;5:13–8. [In Persian]. [Google Scholar]
- 15.Salari AA, Dehghan HR. Evaluation and treatment of colorectal cancer in ShahidRahnemoon and Afshar hospitals, Yazd-Iran. J Shahid Sadoughi Univ Med Sci. 2007;15:20–5. [Google Scholar]
- 16. Corman ML. Colon and Rectal surgery. 4thed. New York: Lippincott Company 1999;625-762.
- 17.Béjar L, Gili M, Díaz V, Ramírez G, López J, Cabanillas JL. et al. Incidence and mortality by colorectal cancer in Spain during 1951-2006 and its relationship with behavioral factors. Eur J Cancer Prev. 2009;18:436–44. doi: 10.1097/CEJ.0b013e328330eb2f. [DOI] [PubMed] [Google Scholar]
- 18.Peppone LJ, Hyland A, Moysich KB, Reid ME, Piazza KM, Purnell JQ. et al. Examining the association between cigarette smoking and colorectal cancer using historical case-control data. Cancer Epidemiol. 2009;33:182–8. doi: 10.1016/j.canep.2009.07.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mitchell RJ, Brewster D, Campbell H, Porteous ME, Wyllie AH, Bird CC. et al. Accuracy of reporting of family history of colorectal cancer. Gut. 2004;53:291–5. doi: 10.1136/gut.2003.027896. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Butterworth AS, Higgins JP, Pharoah P. Relative and absolute risk of colorectal cancer for individuals with a family history: a meta-analysis. Eur J Cancer. 2006;42:216–27. doi: 10.1016/j.ejca.2005.09.023. [DOI] [PubMed] [Google Scholar]
- 21.Abdollahi A, Feyzollah M. The prevalence of colorectal tumors in two medical centers in Tehran 2004 and 2007. Med Sci J Islamic Azad Univ. 2009;19:65–8. [Google Scholar]
- 22. Schwartz SI. Principles of surgery. 9thed. New York: MC Graw Hill 2010;1328-52.