

Abstract
Hepatitis B virus (HBV) infection is a public health problem as a cause of liver diseases including hepatocellular carcinoma and cirrhosis. It is estimated that 350 million people live with chronic infection and about one million people die every year from complication of this chronic disease in the world. So far, ten HBV genotypes (A-J) has been identified which show a geographical distribution. Throughout the world, carrier variability rate for hepatitis B infection is estimated to be 0.1% to 20%, with regions classified as having low endemicity (<2%), intermediate endemicity (2-7%) and high endemicity (>8%). The prevalence of hepatitis B infection is estimated at 2 to 7 percent In Iran. After HBV vaccination program the prevalence of hepatitis B infection has been reported less than 2%, so Iran can be considered one of the countries with low HBV infection endemicity. In Iran several studies were shown that the only genotype of HBV(100%)was found genotype D as the prominent type in some provinces, but some studies reported genotype B(5%)as well as genotype D(95%).The distribution of HBV genotypes may guide us in determining disease burden, prognosis and antiviral responses. So, it is important to know the epidemiologically of HBV genotyping as well.
Keywords: HBV, hepatocellular carcinoma, cirrhosis
1. INTRODUCTION
Hepatitis B virus is one of the most important factors for infected diseases in the world. It was estimated that 350 million people infected with hepatitis B virus and almost 75% patients are living in Asia (1). Nearly one million people die annually from chronic liver diseases such as, chronic hepatitis B , cirrhosis and hepatocellular carcinoma (2).
The prevalence of hepatitis B is reported various in different parts of the world, so this virus existed as hyper endemic in most Asian countries. Throughout the world, carrier variability rate for hepatitis B infection is estimated to be 0.1% to 20% which is different in various areas and is classified into three regions: the first group with areas as having low (<2%), the second group with intermediate prevalence (2-7%) and with high prevalence (>8%) (3). The prevalence of hepatitis B infection is high in Africa, Southeast Asia, the middle East, southern and western pacific island, (they are of endemic regions) intermediate areas consist of south central and southwest Asia, Israel, Japan, Eastern, Southern Europe and Russia and prevalence of hepatitis B infection is low in Northern and Western Europe, North America, Australia, New Zealand, Mexico and southern America (4).
In Iran, a study showed that 35% of population were infected with hepatitis B and the percentage of chronic carriers is about 3%; although after implementing control programs and public vaccination, the prevalence of HBV infection has reduced to less than 2 % (5).
The HBV has ten genotypes (A-J) ,multiple subtypes and serotypes (adr, adw, ayr, ayw), showing genotypes vary in different geographic areas worldwide. There is a relation between serotype and genotype in the world (6). It seems that infected persons with different genotypes show various responses to therapy (7). Also different in genotypes have shown influences in sever course of disease, infection and vaccination (8). Some studies suggested that genotype D could increase the risk of cirrhosis than genotype C(9), on the other hand some evidences showed no difference between these types in infection risk to HCC(10). Moreover some researches found that genotype A is more associated with higher risk of HCC than genotype D(11). Recent study showed that genotype C was more strongly associated with HCC than infected patients with genotypes A, B and D (12). Pre-core stop codon and basal core promoter mutations are of another difference in risk of HCC in various HBV genotypes. Pre-core stop codon A1896 is less in genotype C than genotype B. Basal core promoter mutations in X gene upstream of pre-core area is more in genotypes C (13). This mutation increases the risk of HCC in patients with chronic hepatitis (14). HBV genotypes have different distinguished biological and are able to influence the expression of antigen and immune functional, so recognizing HBV genotypes is important in a country.
This article has investigated the HBV genotyping and was carried out Iran based on papers that identified HBV genotype in Iranian population published in English and Persian languages.
2. HBV MUTANTS
The HBV belongs to hepadenaviridae family. This genome of HBV includes circular DNA that some part of it is bi-string and contains reverse transaction enzyme and/or polymerase DNA Full string genome contains 3020-3320 nucleotides and short length strand is 1700-2800 nucleotides. There are four areas encoded by HBV genome C, X,P,S. Some mutants have found in hepatitis B. In many of this, mutation in pre-core genome is associated with inactivation of HBe Ag (YMDD, S mutant) (15). In patients, this mutant is associated with severity of disease and less response to therapy (16). YMDD region in virus polymerase is located in places influenced by most of reverse transcriptase inhibitor such as Lamivudine and lamivudine. The variables of these regions are derived from partial resistance to these drugs. Variation of YMDD occurred as a result using lamivudinethus, after one year therapy with lamivudine, nearly 24% of patients have showed YMDD mutations (17). The most common core promoter includes the relocation between 1762 and 1764 nucleotides(18). Many of pre-core mutations are related to G-A changing in the 1896 nucleotide, causing the stop codon and preventing the functional of HBe Ag genome.
A study has reported that 58% of infections are the type of pre-core infection in Iran(19). Negative HBe Ag carriers have been heterogeneous; most of them have had less DNA level and normal alanintransferase; so they could not be able to completely respond to therapy. Some evidences showed that 15-20 of HBe Ag carriers have a high level of ALT and HBV DNA in Mediterranean, Eastern Asia and Southern Europe (20).
3. GEOGRAPHICAL PREVALENCE HBV GENOTYPES IN THE WORLD
Genotype A is divided into two sub-genotypes Aa (A1), Ae(A2). Sub-genotype Aa (A1) was found in Africa/Asia and Philippine. Sub genotype Ae(A2) was more common in Europe/united state. Genotype B is also divided into two sub genotype Ba/B2 (Asia) and Bj/B2 (j-Japan) and the prevalence of them has been reported in different areas. Ba has classified to four classB2-B4, these sub genotypes have more virulence than Bj (21).
Genotype C contains five sub genotype (C1-C6). Variation of nucleotide between C1, C2 is 5/2%. Cs (C1) is more common in south east of Asia and Ce (C2) was observed in Japan, China, Korea, east of Asia (22).C3 was reported in Polynesia ,Caledonia areas and C4 was detected in Australia, and C5 and C6 were found in Philippine (23). Genotype C, is associated with hepatocellular carcinoma in Japanese patients and it was not found in Taiwanese patients less than 50 years of age (24). The prevalence of C-1858 strains was found in Southeast Asia (25). In addition, several phylogenetic locations for genotype C isolations were observed. Genotype D is divided into seven sub-genotype (D1-D2) which are prevalent in Pakistan, India, Afghanistan, Mediterranean areas (26). Studies show that sub genotypes D1and D2 were found in Turkey (27) but sub genotype D3 was observed more in Asia (East India), south of Africa and Europe and sub genotype D4 was identified in Australia (28). Recently sub genotype D5 has been reported in east of India and Japan (29). A study suggested that genotype D and serotype ayw2 with 94/4% are predominant in HBV positive in Iran (30).
Genotype E is limited to sub-Saharan Africa. Genotype F has been divided into four sub genotype (F1-F4), also sub genotype F1 was classified to two sub genotype 1a, 1b. Sub- genotypes F2, F1 were observed in Venezuela and sub genotype F3 was found in east and west of America. F3 is the only predominant sub genotype in south of America. Some evidences showed that sub genotype 1a from F1 is derived from center of America, sub genotype F3 is found in north of America and sub genotype F4 had been identified from South of America, but sub genotypes of 1b from F2 is prevalent in most of united states instead of north of southern America and north of America (31).
Genotype F is predominant in Brazil and genotype G is reported in France and united state; also 4-8 % difference in subtypes of genotype E and F has been reported (32).Genotype H is limited to center of America , Mexico and California(33).
Figure 1 illustrates the prevalence of HBV genotypes in the world (32). It has been reported that genotype I was found in north east of India and genotype J was detected in Japanese patients (33).
Figure 1.

Epidemiology of HBV genotypes in the world (34)
There are some significant differences in clinical characteristics and virology of infected patients with various genotypes. It seems that different genotypes may have different responses to therapy(8).
4. EPIDEMIOLOGY OF SEROTYPES AND GENOTYPES OF HBV IN IRAN
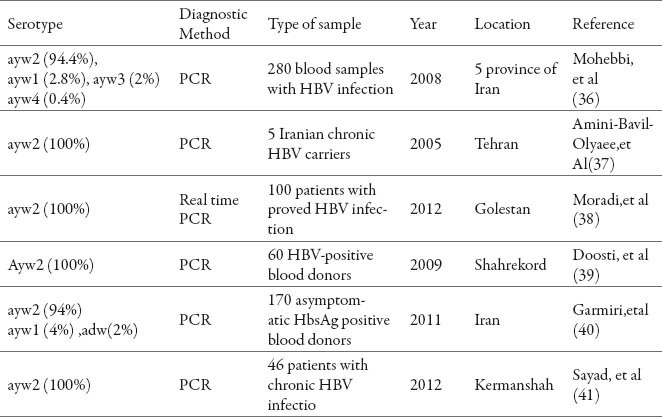
In this study we found 22 studies that were discussed about serotypes and genotypes of HBV in Iran. In six studies, serotype ayw2 was reported as the predominant serotype with relatively abundance more than 94% (Table 1).
Table 1.
Prevalence of HBV serotype in Iran.
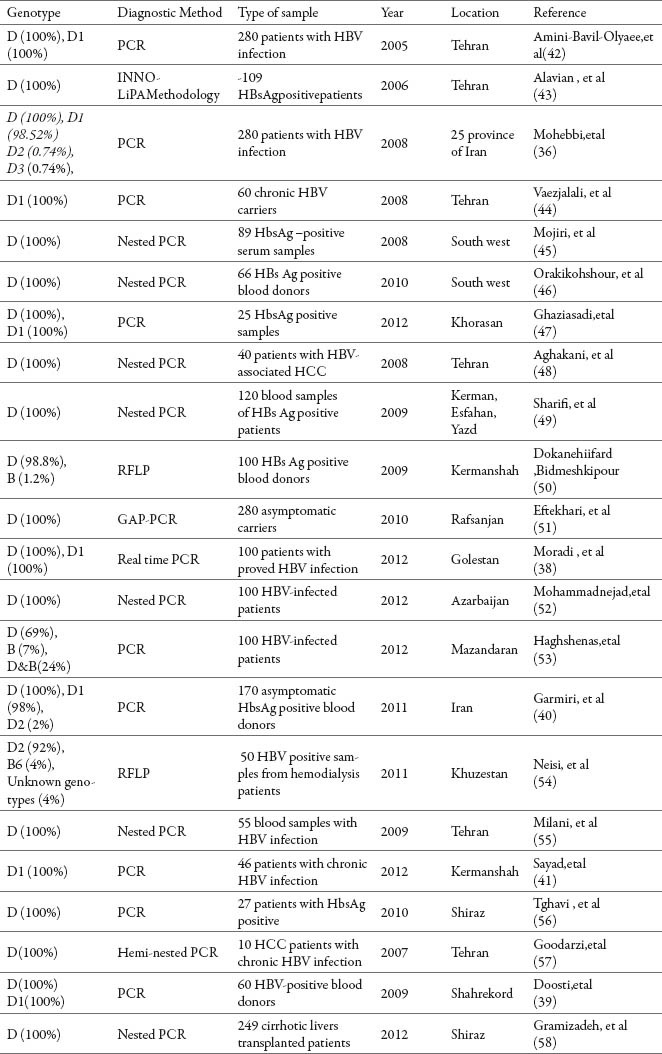
The first study about genotypes of HBV was done in 2005 in Iran and genotype D is defined as predominant genotype in Iran (Table 2).
Table 2.
Prevalence of HBV genotype in Iran
5. DISCUSSION
In this article, 22 studies were discussed about serotypes and genotypes of HBV in Iran. The results of these studies indicate that the predominant genotype and serotype in Iran is D and ayw2, respectively.
In other studies, there is genotype D in South Asia and East Asia, such as Iran, Afghanistan and India (57). This genotype was found the oldest type widely spread in the world. Also, addition to ancient civilization, evolving a special genotype for HBV shows its evolution. In addition, the importance of geographical distribution by presenting genotype D has been reported 46 % in the areas surrounding Iran such as Pakistan, north India (58). Several studies show that the genotype HBV has a special distribution. In the south of Japan (Okinawa) it was indicated that Genotype B is the predominant genotype (59) while in Mainland genotype C is predominant (60). This difference might be the reason of heterogeneity among various areas in Japan. This relations show that factors for the area of human and racial populations are more important than the geographical factors. In Asian countries such as India genotype D and sub-genotype D3 are originated from the counties of Europe (61). Genetically research DNA mitochondria chromosome Y in Indians showed the integration of migrators' genotypes from Europe countries that defines in the northern area more than India (62). Other studies have showed that abundance of genotype HBV can be the reflection of geographical Close relation among this transformation. Genotype D is the oldest type that has spread widely in the world (Nicobar and Andaman Islands). Also, there are genotypes A and D in the north of India and much more probably it is due to migration from Europe which resulted in high prevalence of genotype D in most parts of India. In Iran, it can be deduced that Aryans was first habitants of Caspian sea, then migrated to the other areas of India and Europe. It is possible that some persons infected with genotype D were infected before migration and caused to spread it. Therefore, in Iran, India and most of Europian countries, genotype D is seemingly prevalent (63).
Besides the old civilization; a specific genotype is showing the evaluation of HBV. HBV genotypes show different geographic distribution in the world. Genotype B is predominant in southern Japan (Okinawa) (64); while genotype C has been reported as the dominant type in mainland Japan (65). In various areas of Japan, this difference is related to the heterogeneity between ethnic relations (66). These relations suggests that human factors and racial is more important than geographical factors. HBV genotypes may derive from Europe in Asian countries like the case of India.
Genetic studies of mitochondrial DNA and Y chromosome in Indian population indicates the integration of immigrants gene from European countries and in northern parts is more than of South India(67). Another study showing the prevalence of HBV genotype and changing geographical; so that genotype D is more prevalent in west India. That Genotypes A and D are in the North of India, is likely related to the migration of people from Europe to India and led to genotype D is replaced by genotype A in main areas. In Iran, we can know that the Aryans have been in the north Caspian Sea, and then they moved to other parts of Iran, India and Europe. It seems that genotype D patients have been infected with virus before migration, and then they led to increasing this genotype so genotype D is prevalent in Iran, India and most of Europe (68).
Further studies are needed to achieve complete sequencing of HBV genotypes in Iran. It is related to molecular and cellular mechanism to find other genotypes.
6. CONCLUSION
Because HBV genotypes show distinct geographical distribution, genotype D is predominant in Iran. Despite the different geographical areas in different parts of Iran, genotype D is considered as the predominant genotype. With regard to surveillance, hepatitis in Iranian health system, defining sequences among different isolates of HBV by appropriate intervals or disease outbreaks can be effective in explaining differences in clinical treatment and response to treatment. Also, knowing infection to HBV genotypes can help in the standardization of treatment interference and selection of proper regimens for this disease.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.Yahyaeftekhari Mohammad Kazemiardabili, Hamidhakimi, Ebrahimrezazadeh Zarandi. Common HBV genotype in southeastern Iranian patients. Archiran med. 2010;13(2):147–149. [PubMed] [Google Scholar]
- 2.Who report. 2002. downloaded from www.who.int/emc .
- 3.Alter MJ. Epidemiology of hepatitis B in Europe and worldwide. J Hepatol. 2003;39(Suppl 1):S64–S69. doi: 10.1016/s0168-8278(03)00141-7. [DOI] [PubMed] [Google Scholar]
- 4.Centers for disease control and prevention US Department of health and human services, public health service: Health information for international travel. 2008 [Google Scholar]
- 5.Farzadegan H, Shamszadeh M, Noori-AryaK Epidemiology of viral hepatitis among Iranian population; a viral marker study. AnnAcead Med Singapore. 1980;9(2):144–148. [PubMed] [Google Scholar]
- 6.Chan HL, Hussain M, Lok AS. Different hepatitis B virus genotypes are associated with different mutations in the core promoter and precore regions during hepatitis B e antigen seroconversion. Hepatology. 1999;29:976–984. doi: 10.1002/hep.510290352. [DOI] [PubMed] [Google Scholar]
- 7.Lin CL, Kao JH. The clinical implication of hepatitis B virus genotype: recent advances. J GastroenterolHepatol. 2011;26:123–130. doi: 10.1111/j.1440-1746.2010.06541.x. [DOI] [PubMed] [Google Scholar]
- 8.Zuckerman AJ. Baron’s Medical Microbiology. 4th edition. 1996. Hepatitis Viruses. [PubMed] [Google Scholar]
- 9.Chan HL, Tse CH, Mo F, et al. High viral load and hepatitis B virus subgenotypece are associated with increased risk of hepatocellular carcinoma. J Clin Oncol. 2008;26:177–182. doi: 10.1200/JCO.2007.13.2043. [DOI] [PubMed] [Google Scholar]
- 10.Sumi H, Yokosuka O, Seki N, et al. Influence of hepatitis B virus genotypes on the progression of chronic type B liver disease. Hepatology. 2003;37:19–26. doi: 10.1053/jhep.2003.50036. [DOI] [PubMed] [Google Scholar]
- 11.Livingston SE, Simonetti JP, McMahon BJ, et al. Hepatitis B virus genotypes in Alaska Native people with hepatocellular carcinoma: preponderance of genotype F. J Infect Dis. 2007;195:5–11. doi: 10.1086/509894. [DOI] [PubMed] [Google Scholar]
- 12.Wong GL, Wong VW, Tan GM, et al. Surveillance programme for hepatocellular carcinoma improves the survival of patients with chronic viral hepatitis. Liver Int. 2008;28:79–87. doi: 10.1111/j.1478-3231.2007.01576.x. [DOI] [PubMed] [Google Scholar]
- 13.Yang HI, Yeh SH, Chen PJ, et al. Associations between hepatitis B virus genotype and mutants and the risk of hepatocellular carcinoma. J Natl Cancer Inst. 2008;100:1134–1143. doi: 10.1093/jnci/djn243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Liu S, Zhang H, Gu C, et al. Associations between hepatitis B virus mutations and the risk of hepatocellular carcinoma: a meta-analysis. J Natl Cancer Inst. 2009;101:1066–1082. doi: 10.1093/jnci/djp180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Locarnini SJ, McMillan A. Bartholomeusz. The hepatitis B virus and common mutants. Semin Liver Dis. 2003;23:5–20. doi: 10.1055/s-2003-37587. [DOI] [PubMed] [Google Scholar]
- 16.Bruneto MR, Giarin M, Saracco G, et al. Hepatitis B virus unable to secrete e-antigen and response to interferon in chronic hepatitis B. Gastroenterology. 1993;105:845–850. doi: 10.1016/0016-5085(93)90903-p. [DOI] [PubMed] [Google Scholar]
- 17.Tu H, XiongSD, Trepo C, Wen YM. Frequency of hepatitis B virus e-minus varies in patients from different areas of China. J Med Virol. 1997;51:85–89. doi: 10.1002/(sici)1096-9071(199702)51:2<85::aid-jmv1>3.0.co;2-n. [DOI] [PubMed] [Google Scholar]
- 18.Bortolotti F, Cadrobbi P, Crivellaro C, et al. Long-term outcome of chronic type B hepatitis in patients who acquire hepatitis B virus infectionin childhood. Gastroenterology. 1990;99:805–810. doi: 10.1016/0016-5085(90)90972-4. [DOI] [PubMed] [Google Scholar]
- 19.Yosefirad M, Malekzadeh R, Khatibian M, et al. Prospective controlled trial of interferon alpha-2b in Iranian patients with chronic hepatitis B. Gastroenterology. 1997:112–142. [Google Scholar]
- 20.Funk ML, Rosenberg DM, Lok ASF. World-wide epidemiology of HBeAg-negative chronic hepatitis B and associated precore and core promoter variants. J Viral Hepat. 2002;9:52–61. doi: 10.1046/j.1365-2893.2002.00304.x. [DOI] [PubMed] [Google Scholar]
- 21.Huy TT, Ushijima H, Quang VX, Win KM, Luengrojanakul P, Kikuchi K, Sata T, Abe K. Genotype C of hepatitis B virus can be classified into at least two subgroups. J Gen Virol. 2004;85:283–292. doi: 10.1099/vir.0.19633-0. [DOI] [PubMed] [Google Scholar]
- 22.Bruss V. Hepatitis B virus morphogenesis. World J Gastroenterol. 2007;13(1):65–73. doi: 10.3748/wjg.v13.i1.65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kao JH, Chen PJ, Lai MY, Chen DS. Hepatitis B genotypes correlate with clinical outcomes in patients with chronic hepatitis B. Gastroenterology. 2000;118:554–559. doi: 10.1016/s0016-5085(00)70261-7. [DOI] [PubMed] [Google Scholar]
- 24.Lindh M, Andersson AS, Gusdal A. Genotypes, nt 1858 variants, and geographic origin of hepatitis B virus-large-scale analysis using a new genotyping method. J Infect Dis. 1997;175:1285–1293. doi: 10.1086/516458. [DOI] [PubMed] [Google Scholar]
- 25.Fung SK, Lok ASF. Hepatitis B virus genotypes: do they play a role in the outcome of HBV infection? Hepatology. 2004;40:790–792. doi: 10.1002/hep.1840400407. [DOI] [PubMed] [Google Scholar]
- 26.Sobia A, Rehmansu Khan S, Alii Ali S, Khan A. Prevalence of hepatitis B virus genotypes in HBs Ag positive individuals of Afghanistan. Virology journal. 2011;8:281. doi: 10.1186/1743-422X-8-281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bozdayi G, Turkyilmaz AR, Idilman R, et al. Complete genome sequence and phylogenetic analysis of hepatitis B virus isolated from Turkish patients with chronic HBV infection. J Med Virol. 2005;76:476–481. doi: 10.1002/jmv.20386. [DOI] [PubMed] [Google Scholar]
- 28.Kumar S, Tamura K, Nei M. MEGA3: integrated software for molecular evolutionary genetics analysis and sequence alignment. Brief Bioinform. 2004;5:150–163. doi: 10.1093/bib/5.2.150. [DOI] [PubMed] [Google Scholar]
- 29.Banerjee A, Kurbanov F, Datta S, et al. Phylogenetic relatedness and genetic diversity of hepatitis B virus isolates in Eastern India. J Med Virol. 2006;78:1164–1174. doi: 10.1002/jmv.20677. [DOI] [PubMed] [Google Scholar]
- 30.Alavian SM, Keyvani H, Rezai M, Ashayeri N, Sadeghi HM. Preliminary report of hepatitis B virus genotype prevalence in Iran. World J Gastroenterol. 2006;12:5211–5213. doi: 10.3748/wjg.v12.i32.5211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Arauz-Ruiz, Norder PH, Robertson BH, Magnius LO. Genotype H: A new Amerindian genotype of hepatitis B virus revealed in Central America. J Gen Virol. 2002;83:2059–2073. doi: 10.1099/0022-1317-83-8-2059. [DOI] [PubMed] [Google Scholar]
- 32.Zhang Q, Cao G. Genotypes, mutations, and viral load of hepatitis B virus and the risk of hepatocellular carcinoma. Hepatitis Monthly. 2001;11(2):86–91. [PMC free article] [PubMed] [Google Scholar]
- 33.Arauz-ruiz P, Norder H, Robertson BH, Magnius LO. Genotype H: a new Amerindian genotype of hepatitis B virus revealed in central America. J Gen virol. 2002;83(pt8):2059–2073. doi: 10.1099/0022-1317-83-8-2059. [DOI] [PubMed] [Google Scholar]
- 34.Mohebi SR, Amini Bavil-Olyaee S, Zali N, Noorinayer B, Derakhshan F, Chiani M. Molecular epidemiology of hepatitis B virus in Iran. Clin Microbiol Infect. 2008;14(9):858–866. doi: 10.1111/j.1469-0691.2008.02053.x. [DOI] [PubMed] [Google Scholar]
- 35.Amini-Bavil-Olyaee, Sarrami-Forooshani, Abedi A, Sabahi F, Abachi M, Azizi M, et al. Complete genomic sequence and phylogenetic relatedness of hepatitis B virus isolated from Iran. Journal of Medical Virology. 2005;76:318–326. doi: 10.1002/jmv.20362. [DOI] [PubMed] [Google Scholar]
- 36.Moradi A, Zhand S, Ghaemi A, Javid N, Tabarraei A. Mutations in the S gene region of hepatitis B virus genotype D in Golestan province –Iran. Virus Genes. 2012;44:382–387. doi: 10.1007/s11262-012-0715-z. [DOI] [PubMed] [Google Scholar]
- 37.Doosti A, Amini-Bavil-Olyaee S, Tajbakhsh E, Adeli A, Mahboudi F. Prevalence of viral hepatitis and molecular analysis of HBV among voluntary blood donors in west Iran. 2009;32:193–198. [PubMed] [Google Scholar]
- 38.Garmiri P, Rezvan H, Abolghasemi H, Allian JP. Full genome characterization of hepatitis B virus strans from blood donors in Iran. J Med Virol. 2011;83(6):948–952. doi: 10.1002/jmv.21772. [DOI] [PubMed] [Google Scholar]
- 39.Sayad B, Anvari FA, Alavian SM, Norouzi M, Hamzelooie M, Shirvani M, et al. Correlatin of hepatitis B surface antigene mutations with clinical status of the chronically infected patients from kermanshah, west of Iran. Minerva Gastroenterologica e Dietologica. 2012;58(1):9–18. [PubMed] [Google Scholar]
- 40.Amini-Bavil-Olyaee S, Sarrami-Forooshani R, Mahboudi F, Sabahi F, Adeli A, Noorinayer B, et al. Genotype Characterization and Phylogenetic Analysis of Hepatitis B Virus Isolates From Iranian Patients. Journal of Medical Virology. 2005;75:227–234. doi: 10.1002/jmv.20261. [DOI] [PubMed] [Google Scholar]
- 41.Alavian SM, Keyvani H, Rezai M, Asayeri N, Sadeghi HM. Preliminary report of hepatitis B virus genotype prevalence in Iran. World J Gastroenterol. 2006;12(32)(5211) doi: 10.3748/wjg.v12.i32.5211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Vaezjalali M, Alavian SM, Jazayeri AM, Nategh R, Mahmoodi M, Hajibeigi B, et al. Genotype of hepatitis B virus Isolated from Iranian Chronic arriers of the virus. Hepatitis Monthly. 2008;8(2):97–100. [Google Scholar]
- 43.Mojiri A, Behzad-behbahani A, Saberifirozi M, Ardabili M, Beheshti M, Rahsaz M, et al. Hepatitis B virus in southwest Iran: molecular serological and clinical outcomes. World J Gastroenterol. 2008;14(10):1510–1513. doi: 10.3748/wjg.14.1510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Oraki Kohshur M, Galehdari H, Foroughmand AM, Andashti B, Jalalifar MA, Bidmeshlipour A. HBV Genotyping in HBs Ag- positive blood donors from southwestern Iran. Hepat Mon. 2010;10(2):147–148. [PMC free article] [PubMed] [Google Scholar]
- 45.Ghaziasadi A, Ziaee M, Norouzi M, Malekzadeh R, Alavian SM, Saberfar E, et al. The prevalence of hepatitis B virus surface antigen (HbsAg) variations and correlation with the clinical and serologic pictures in chronic carriers from khorasan province, North-East of Iran. Acta Medica Iranica. 2012;50(4):265–272. [PubMed] [Google Scholar]
- 46.Aghakani A, Hamkar R, Zamani N, Eslamifar A, Banifazl M, Saadat A, et al. Heoatitis B virus genotype in Iranian patients with hepatocellular carcinoma. Int J infect Dis. 2009;13(6):685–689. doi: 10.1016/j.ijid.2008.10.009. [DOI] [PubMed] [Google Scholar]
- 47.Sharifi Z, Gharehbaghian A, Noroozi M. Prevalence of hepatitis B virus genotypes to be determined by sequencing in blood donors in Kerman, Esfahan and Yazd. Scientific Journal of Iranian Blood Transfusion Organizatin. 2009;6(4):248–256. [Google Scholar]
- 48.Dokanehifard S, Bidmeshkipour A. A study of hepatitis B virus(HBV) genotypes in Kermanshah province, west of Iran. Journal of biological sciences. 2009;1:113–120. [Google Scholar]
- 49.Eftekari Y, Kazemi Arababadi M, Hakimi H, Rezazadehzarandi E. Common HBV genotype in Southeastern Iranian patients. Arch Iran Med. 2010;13(2):147–149. [PubMed] [Google Scholar]
- 50.Mohammadnejad l, Farajnia S, Parivar K, Naghili B, Yousefzadehkheimagsh R. Hepatitis B virus genotype in Eastern Azarbaijan, Northwest Iran. Arch Iran Med. 2012;15(7):446–448. [PubMed] [Google Scholar]
- 51.Haghshenas M, Mosavi T, Rafiee R, Hosseini V, Hosseinikha Z. Prevalence of hepatitis B virus genotypes with HBs Ag positive patients in the northern of Iran (Mazandaran) during 2010-2011. Healthmed. 2012;6(5):1568. [Google Scholar]
- 52.Neisi N, Makvandi M, Samarbaf-zadeh AR. A study on genotypes of hepatitis B virus among hemodialysis patients in Kuzestan province. Jundishapur J Microbiol. 2011;4(2):65–70. [Google Scholar]
- 53.Milani S, Sharifi Z, M Hosseini I, Mahmoodian Shooshtari M. Determination of HBV Genotypes among Hbs Ag Positive Blood Donors in Tehran, Iran Using PCR-RFLP. Iranian Journal of Public Health. 2009;38(1):41–47. [Google Scholar]
- 54.Taghavi SA, Tabibi M, Eshraghian A, Keyvani H, Eshraghian H. Prevalence and clinical significance of hepatitis B basal core promoter and precore gene mutations in Southern Iranian patients. Hepatitis Monthly. 2010;10(4):294–297. [PMC free article] [PubMed] [Google Scholar]
- 55.Goodarzi Z, Malekzadeh R, Montazeri G, Alavian SM, Qurbanalizadgan M, Daram M, et al. Phylogenetic analysis of HBV based on Pre S region in iranian hepatocellular carcinoma patients. Hepatitis monthly. 2007;7(4):201–205. [Google Scholar]
- 56.Gramizadeh B, Nikeghbalian S, Kazemi K, Shamsaifar A, Bahador A, Salahi H, et al. Hepatocellular carcinoma in explanted livers of pstients with genotype D HBV cirrhosis: report of the first experience from Iran. Archives of Iranian Medicine. 2013;16:6. [PubMed] [Google Scholar]
- 57.Baig S, Siddiqui A, Chakravaty R, Moatter T. Hepatitis B virus subgenotypes D1 and D3 are prevalent in Pakistan. BMC Research Note. 2009;2(1) doi: 10.1186/1756-0500-2-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Bozdayi AM, Aslan N, Bozdayi G, Takyilmaz AR, Sengezer T, Wend U, et al. Molecular epidemiology of hepatitis B, C and D viruses in Turkish patients. Arch Virol. 2004 Nov;149(11):2115–2129. doi: 10.1007/s00705-004-0363-2. [DOI] [PubMed] [Google Scholar]
- 59.Abdo AA, AL-Jarallah BM, Sanai FM, Hersi AS, AL-Swat K, Azzam NA, et al. Hepatitis B genotypes: Relation to clinical outcome in patients with chronic hepatitis B in Saudi Arabia. World J Gastroenterol. 2006 Nov;1(43):7019–7024. doi: 10.3748/wjg.v12.i43.7019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Sobia A, Saif R, Sanaullah K, Ljaz A, Sajid A, Shahid N. Prevalence of hepatitis B virus genotypes in HBs Ag positive individuals of Afghanistan. Virology journal. 2011;8:281. doi: 10.1186/1743-422X-8-281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Banerjee A, Datta S, Chandara PK, Roychowdhury S, Panda CK, Chakravarty R. Distribution of hepatitis B virus genotypes: phylogenetic analysis and virological characteristics of genotype C circulation among HBV carriers in Kolkata, Eastern India. World J Gastroenterol. 2006 Oct;12(37):5964–5971. doi: 10.3748/wjg.v12.i37.5964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Kato H, Ruzibakiev R, Yuldasheva N, Hegay T, Kurbanov F, Achundjanov B, et al. Hepaitis B virus genotypes in Uzbekistan and validity of two different systems for genotyping. J Med Virol. 2002 Aug;67(4):477–483. doi: 10.1002/jmv.10126. [DOI] [PubMed] [Google Scholar]
- 63.Morozov V, Pisareva M, Groudinin M. Homologous recombination between different genotypes of hepatitis B virus. Gene. 2000;260(1-2):55–65. doi: 10.1016/s0378-1119(00)00424-8. [DOI] [PubMed] [Google Scholar]
- 64.Orito E, Mizokami M. Hepatitis B virus genotypes and hepatocellular carcinoma in Japan. Intervirology. 2003;46(6):408–412. doi: 10.1159/000075000. [DOI] [PubMed] [Google Scholar]
- 65.Orito E, Ichida T, Sakugawa H, Sata M, Horiike N, Hino K, Okita K, Okanoue T, Iino S, Tanaka E, Suzuki K, Watanabe H, Hige S, Mizokami M. Geographic distribution of hepatitis B virus (HBV) genotype in patients with chronic HBV in Japan. Hepatology. 2001;34:590–594. doi: 10.1053/jhep.2001.27221. [DOI] [PubMed] [Google Scholar]
- 66.Horai S, Murayama K, Hayasaka K, Matsubayashi S, Hattori Y, Fucharoen G, Harihara S, Park KS, Omoto K. Pan IH: mtDNA polymorphism in East Asian populations, with special reference to the people of Japan. Am J Hum Genet. 1996;59:579–590. [PMC free article] [PubMed] [Google Scholar]
- 67.Bamshad M, Kivisild T, Watkins WS, Dixon ME, Ricker CE, Rao BB, et al. Genetic evidence on the origins of Indian caste populations. Genome Res. 2001;11:994–1004. doi: 10.1101/gr.173301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Jazayeri SM. Carmanwf: Evalution of HBV genotype D in the middle East and South Asia. Hepatitis Monthly. 2009;9(1):9–11. [Google Scholar]