

Abstract
C-shaped configuration in the upper maillary first molar is an extremely rare appearance (0.12%). This case reports management of the tooth with such a configuration as well as depiction of its internal morpholgy and external morphology through spiral computed tomography and dentascan in the contralateral tooth with similar morphology. After careful clinical observation and confirmation through spiral computed tomography, it was concluded that the teeth had Melton category I configuration with fused roots.
Keywords: Dental Pulp Cavity, Molar, Spiral Computed Tomography
INTRODUCTION
Successful endodontic therapy depends on many factors and one of the most important steps in any root canal treatment is canal preparation. Canal preparation determines the degree of control over the complete elimination of root canal contents that is crucial to debridement infection [1]. Knowledge of the internal root morphology is a complex and extremely important point for planning and performing endodontic therapy. Several anatomic variations existing in the root canal system may contribute to the failure of root canal therapy [2].
Reports of C-shaped canals in the maxillary first molar are very rare and there have been reports by few authors previously. Newton and McDonald in 1984 [3], Dankner et al. in 1990 [4] and Kottor et al. in 2011 reported a C-shaped canal in the palatal root of the maxillary first molar [5]. In 2002, De Moor [6] concluded that the probability of observing C-shaped canals in maxillary first molars was as low as 0.091% while in 2006, Cleghorn et al. [7] reported C-shaped roots and canals were found only in 0.12% of the maxillary first molars. The literature has documentation mostly from studies (in vitro), clinical root canal system anatomy studies (in vivo) or clinical case reports with 2 dimensional radiographs used as tools for confirmation of the reports. Most of the cases reported have demonstrated fusion of distobuccal and mesiobuccal canals [6,8] and all the cases reported had two or more roots.
Owing to their inherent limitations, radio-graphs are of limited value in determining the complexity of C-shaped root canal patterns [9]. The use of spiral computed tomography for imaging and 3 dimensional reconstructions through dentascan gives a complete insight in to root canal configuration of the tooth.
This case report presents Melton category I root canal configuration in permanent maxillary first molars of the same patient. The diagnosis was done by clinical examination, spiral computed tomography and three-dimensional construction by dentascan.
CASE REPORT
A 24-year-old female complained of pain in the upper right posterior region of the jaw and heightened and prolonged sensitivity to cold since few days ago. On clinical examination, the patient had occlusal caries in the right maxillary first molar (tooth # 3) involving the pulp. The tooth was highly tender on percussion on vertical occlusal tapping and slightly tender on palpation in the slightly tender on percussion in vestibular region. Both thermal tests by hot and cold and electric pulp testing (Parkel Electronics Division, Farmingdale, NY) caused no response. On radiographic examination, involvement of pulp by caries was revealed in tooth #3. Based on clinical and radiographic examination, a diagnosis of symptomatic apical periodontitis was made, and nonsurgical endodontic treatment was recommended.
After anesthetizing the local region, root canal access cavity preparation was done using Endo Access bur and an Endo Z bur (Dentsply Tulsa, Tulsa, OK) under rubber dam. A C-shaped configuration extending from buccal end to palatal end of the pulp chamber was observed and its continuity could also be detected by DG 16 explorer (Figure 1). Biomechanical preparation of the tooth was started by insertion of ISO#10 to determine the paten-cy of the canal. Completion of bio-mechanical preparation was done by sequential use of nickel-titanium ProTaper S1, SX shaping rotary file till F2 finishing file (Dentsply Maillefer, Ballaigues, Switzerland). Brushing strokes were used in a circumferential manner to prepare all canal walls. Root canals were irrigated with 3% sodium hypochlorite and normal saline.
Fig 1.
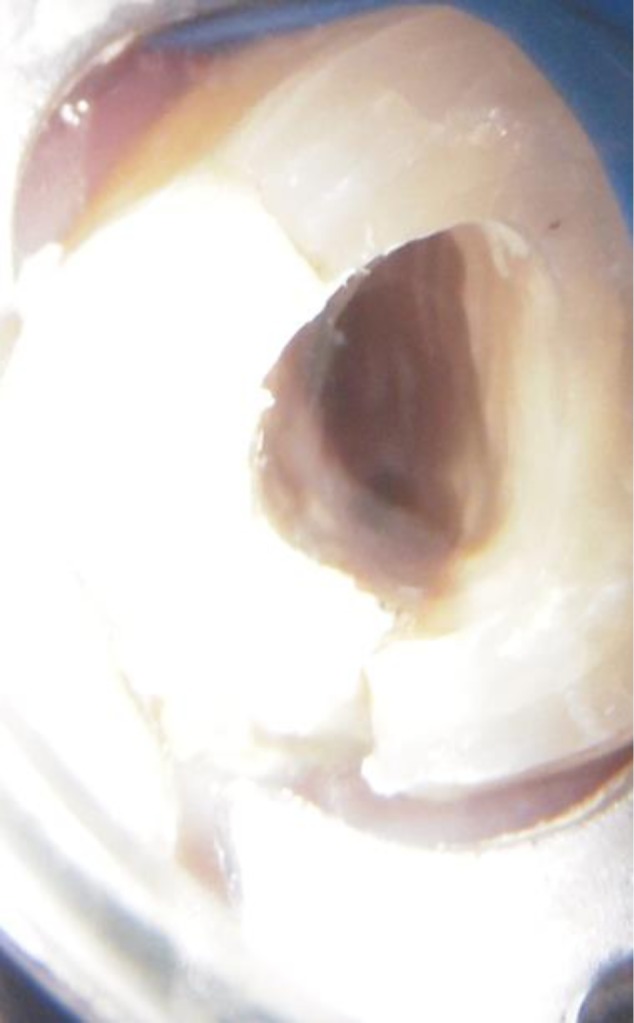
Shows C–shaped canal after access opening
A calcium hydroxide intracanal medicament was placed in canals and the patient was recalled after one week. In the next appointment, obturation was done. Coronal restoration was done in the access cavity to prevent microleakage and fracture of the tooth. A spiral computed tomography scan and three-dimensional reconstruction of data was than performed to confirm the observations and note similar finding in any other tooth in the oral cavity. The spiral computed tomography (CT) clearly depicted a C-shaped canal in tooth number #14 (Figure 2a–e) that was contralateral to tooth number #3. The scan also revealed single canals in both teeth. Three-dimensional recontstruction through dentascan also revealed fused roots that formed a single root (Figure 3a, 3b, 4).
Fig 2a.

Shows typical C-shaped configuration at the coronal level
2b. C-shaped configuration at the middle third
2c. Canal continuing as single canal at the apical third
2d. & 2e. Canal terminating at the single foramen at the apical end
Fig 3a & 3b.

3 dimensional reconstruction shows fused roots in both teeth #3 and #14
Fig 4.

3 dimensional imaging shows single root apex of teeth #3 and #14
DISCUSSION
It has been speculated that the failure of the Hertwig’s epithelial root sheath to fuse on the lingual or buccal root surface was the main cause of a C-shaped root that always contains a C-shaped canal. The C-shaped root may also be formed by coalescence because of deposition of cementum with time [10].
A number of reports have described different trends in the shape and number of roots and root canals among different human races. The variation appears to be genetically determined and may be used in tracing the ethnic origin of the subjects [11]. This particular case reports the presence of C-shaped canal in tooth #3 and tooth # 14 with a single fused root and a single canal continuing till the apex. The complete picture of the internal anatomy as well as bony and root topography was clearly depicted by spiral computed tomography and three-dimensional imaging. Dentascan is a unique new computer software program that provides computed tomographic (CT) imaging of the mandible and maxilla in three planes of reference: axial, panoramic, and oblique sagittal (or cross-sectional).
The clarity and identical scale between the various views permits uniformity of measurements and cross-referencing of anatomic structures through all three planes [12].
C-shaped canals with a single swath of canal are the exception rather than the rule [13]. In such teeth, the floor of the pulp chamber is usually situated deeply and may assume an unusual anatomic appearance.
The main anatomic feature of C-shaped canals is the presence of a fin or web connecting the individual root canals. Roots containing a C-shaped canal often have a conical or square configuration [14]. In all cases reported in the literature, the C-shaped canal has been reported in the tooth with two roots [3,4,6,15]. but in the present case, the teeth have single canal configuration that is confirmed by spiral computed tomography (CT) scan and dentascan (Figure 5). Radiographic identification of this phenomenon is difficult, and occassionally it is identified only during access-cavity preparation [16]. In our case, we could not use spiral computed tomography (CT) scan for confirmation before root canal treatment in tooth number #3, but it neverthless revealed ideal C-shaped configuration in the contralateral tooth #14. There are some hints that can be taken into account to recognise C-shaped configuration even when advanced diagnostic tools are not around. Clinical recognition of C-shaped canals is based on definite observable criteria such as the anatomy of the floor of the pulp chamber and the persistence of hemorrhage or pain when separate canal orifices were found [17].
Fig 5.

Orthopentogram view shows single root canal configuration from the coronal portion till the apex
The pulp chamber in teeth with C-shaped canals may be large in the occlusoapical dimension with a low bifurcation. Alternatively, the canal can be calcified, disguising its C-shape. At the outset, several orifices may be probed that link up on further instrumentation [18]. In a true C-shaped canal, it is possible to pass an instrument from the mesial to the distal aspect without obstruction. In other configurations, discontinuous dentine bridges impede such passage. If a file could not be passed through the isthmus of the pulpal floor during clinical inspection, the practitioner might consider the root canal as being separated, but in the laboratory analysis, these canals might merge just below the isthmus area [19]. The extravagant use of small files and 5.25% sodium hypochlorite solution and deeper penetration with small instruments using sonics or ultrasonics may allow for better cleaning in fan-shaped areas and furcation canals of the C-shaped canal system. Possibly, a noninstrumentation technique, light-activated disinfection, and ultrasonic irrigation may improve the debridement or elimination of microbial infections in these irregular canal areas [20]. The diagnosis, cleaning and shaping of the canal and obturation of the canal may be a challenge, but can be dealt with throrough knowledge of root canal anatomy and application of proper clinical skills.
CONCLUSION
In this case we have reported management of C-shaped configuration in the upper maxillary first molar. The images from spiral CT scan show the typical Melton category I C-shaped pattern. The three-dimensional reconstruction of bony topography showed fusion of all three roots with a single apical root end demonstrating a relationship between external and internal root morphology.
REFERENCES
- 1.Tang L, Sun TQ, Gao XJ, Zhou XD, Huang DM. Tooth anatomy risk factors influencing root canal working length accessibility. Int J Oral Sci. 2011 Jul;3(3):135–40. doi: 10.4248/IJOS11050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Nimigean V, Nimigean VR, Sălăvăstru DI. A rare variant of internal anatomy of a third mandibular molar: a case report. Rom J Morphol Embryol. 2011;52(2):691–3. [PubMed] [Google Scholar]
- 3.Newton CW, McDonald S. A C-shaped canal configuration in a maxillary first molar. J Endod. 1984 Aug;10(8):397–9. doi: 10.1016/S0099-2399(84)80162-4. [DOI] [PubMed] [Google Scholar]
- 4.Dankner E, Friedman S, Stabholz A. Bilateral C shaped configuration in maxillary first molars. J Endod. 1990 Dec;16(12):601–3. doi: 10.1016/S0099-2399(07)80204-4. [DOI] [PubMed] [Google Scholar]
- 5.Kottoor J, Velmurugan N, Ballal S, Roy A. Four-rooted maxillary first molar having C-shaped palatal root canal morphology evaluated using cone-beam computerized tomography: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011 May;111(5):e41–5. doi: 10.1016/j.tripleo.2010.12.009. [DOI] [PubMed] [Google Scholar]
- 6.De Moor RJ. C-shaped root canal configuration in maxillary first molars. Int Endod J. 2002 Feb;35(2):200–8. doi: 10.1046/j.1365-2591.2002.00461.x. [DOI] [PubMed] [Google Scholar]
- 7.Cleghorn BM, Christie WH, Dong CC. Root and root canal morphology of the human permanent maxillary first molar: a literature review. J Endod. 2006 Sep;32(9):813–21. doi: 10.1016/j.joen.2006.04.014. [DOI] [PubMed] [Google Scholar]
- 8.Al Shalabi RM, Omer OE, Glennon J, Jennings M, Claffey NM. Root canal anatomy of maxillary first and second permanent molars. Int Endod J. 2000 Sep;33(5):405–14. doi: 10.1046/j.1365-2591.2000.00221.x. [DOI] [PubMed] [Google Scholar]
- 9.Gao Y, Fan B, Cheung GS, Gutmann JL, Fan M. C-shaped canal system in mandibular second molars part IV: 3-D morphological analysis and transverse measurement. J Endod. 2006 Nov;32(11):1062–5. doi: 10.1016/j.joen.2006.05.014. [DOI] [PubMed] [Google Scholar]
- 10.Manning SA. Root canal anatomy of mandibular second molars. Part II. C-shaped canals. Int Endod J. 1990 Jan;23(1):40–5. doi: 10.1111/j.1365-2591.1990.tb00801.x. [DOI] [PubMed] [Google Scholar]
- 11.Fan B, Cheung GS, Fan M, Gutmann JL, Bian Z. C-shaped canal system in mandibular second molars: Part I-Anatomical features. J Endod. 2004 Dec;30(12):899–903. doi: 10.1097/01.don.0000136207.12204.e4. [DOI] [PubMed] [Google Scholar]
- 12.Yanagisawa K, Friedman CD, Vining EM, Abrahams JJ. DentaScan imaging of the mandible and maxilla. Head Neck. 1993 Jan-Feb;15(1):1–7. doi: 10.1002/hed.2880150102. [DOI] [PubMed] [Google Scholar]
- 13.Cohen S, Burns RC. Pathways of the pulp. 8th ed. St. Louis: Mosby; 2002. pp. 196–229. [Google Scholar]
- 14.Jafarzadeb H, Wu Y. The C-shaped root canal configuration: a review. J Endod. 2007 May;33(5):517–23. doi: 10.1016/j.joen.2007.01.005. [DOI] [PubMed] [Google Scholar]
- 15.Yilmaz Z, Tuncel B, Serper A, Calt S. C-shaped root canal in a maxillary first molar: a case report. Int Endod J. 2006 Feb;39(2):162–6. doi: 10.1111/j.1365-2591.2006.01069.x. [DOI] [PubMed] [Google Scholar]
- 16.Keinan D, Nuni E, Slutzky-Goldberg I. Is a C-shaped configuration possible in teeth other than mandibular molars? Quintessence Int. 2009 Jul-Aug;40(7):541–3. [PubMed] [Google Scholar]
- 17.Lambrianidis T, Lyroudia K, Pandelidou O, Nicolaou A. Evaluation of periapical radiographs in the recognition of Cshaped mandibular second molars. Int Endod J. 2001 Sep;34(6):458–62. doi: 10.1046/j.1365-2591.2001.00417.x. [DOI] [PubMed] [Google Scholar]
- 18.Cooke HG, 3rd, Cox FL. C-shaped canal configurations in mandibular molars. J Am Dent Assoc. 1979 Nov;99(5):836–9. doi: 10.14219/jada.archive.1979.0402. [DOI] [PubMed] [Google Scholar]
- 19.Lyroudia K, Samakovitis G, Pitas I, Lambrianidis T, Molyvdas I, Mikrogeorgis G. 3D reconstruction of two C-shape mandibular molars. J Endod. 1997 Feb;23(2):101–4. doi: 10.1016/S0099-2399(97)80254-3. [DOI] [PubMed] [Google Scholar]
- 20.Fan B, Min Y, Lu G, Yang J, Cheung GS, Gutmann JL. Negotiation of C-shaped canal systems in mandibular second molars. J Endod. 2009 Jul;35(7):1003–8. doi: 10.1016/j.joen.2009.04.011. [DOI] [PubMed] [Google Scholar]