

Abstract
Diagnosis of periodontal disease mainly depends on clinical signs and symptoms. However, in the case of bone destruction, radiographs are valuable diagnostic tools as an adjunct to the clinical examination. Two dimensional periapical and panoramic radiographs are routinely used for diagnosing periodontal bone levels. In two dimensional imaging, evaluation of bone craters, lamina dura and periodontal bone level is limited by projection geometry and superpositions of adjacent anatomical structures. Those limitations of 2D radiographs can be eliminated by three-dimensional imaging techniques such as computed tomography. Cone beam computed tomography (CBCT) generates 3D volumetric images and is also commonly used in dentistry. All CBCT units provide axial, coronal and sagittal multi-planar reconstructed images without magnification. Also, panoramic images without distortion and magnification can be generated with curved planar reformation. CBCT displays 3D images that are necessary for the diagnosis of intra bony defects, furcation involvements and buccal/lingual bone destructions. CBCT applications provide obvious benefits in periodontics, however; it should be used only in correct indications considering the necessity and the potential hazards of the examination.
Keywords: Cone beam computed tomography, Periodontology, Radiology, Dentistry, Oral diagnosis
Core tip: Dentomaxillofacial cone beam computed tomography (CBCT) is now commonly used for a variety of diagnostic tasks in dentistry. Its applications in periodontal disease has not been very well reviewed and documented previously. This review paper will shed light into this innovative technology and its use in periodontology. Diagnosis of periodontal disease depends on clinical signs and symptoms. However, in the case of bone destruction, radiographs are valuable diagnostic tools as an adjunct to the clinical examination. Two dimensional periapical and panoramic radiographs are routinely used for diagnosing periodontal bone levels. In two dimensional imaging, evaluation of bone craters, lamina dura and periodontal bone level is limited by projection geometry and superposition of adjacent anatomical structures. Those limitations of 2D radiographs can be eliminated by three-dimensional imaging techniques such as computed tomography. CBCT generates 3D volumetric images and is also commonly used in dentistry. All CBCT units provide axial, coronal and sagittal multi-planar reconstructed images without magnification. Also, panoramic images without distortion and magnification can be generated with curved planar reformation. CBCT displays 3D images that are necessary for the diagnosis of intra bony defects, furcation involvements and buccal/lingual bone destructions. CBCT applications provide obvious benefits in periodontics, however; it should be used only in correct indications considering the necessity and the potential hazards of the examination.
INTRODUCTION
Periodontal diseases consist of a variety of conditions affecting the periodontal tissues such as: gingiva, periodontal ligament, root cementum and alveolar bone. Some of these tissues are soft (gingiva, periodontal ligament) whereas some are hard tissues (root cementum and alveolar bone)[1]. Inflammation of periodontal tissues is a common disease which results in attachment loss and destruction of alveolar bone. Diagnosis of periodontal diseases mainly depends on clinical signs and symptoms[2]. However, in the case of bone destruction, radiographs are valuable diagnostic tools as an adjunct to the clinical examination. Although periapical and panoramic radiographs are routinely used for diagnosing periodontal bone levels, the projection geometry of the X-ray beam may cause magnification and distortion which makes it impossible to obtain accurate diagnosis[3]. In panoramic and periapical radiographs, bone craters, lamina dura and periodontal bone level evaluation is limited by the superposition of adjacent anatomic structures and projection geometry. Conventional two-dimensional radiographs generate 2D images in which teeth roots are superimposed on the alveolar bone and as a result bone changes such as; furcation involvement, buccal and lingual alveolar bone defects are obscured[4-6]. Limitations of 2D radiographs can be eliminated by using three-dimensional imaging techniques such as computed tomography (CT)[7]. CT can be categorized into two groups according to the geometry of X-ray beam: 1-fan beam and 2-cone beam (Figure 1). Cone beam computed tomography (CBCT) generates 3D volumetric images and is commonly used in dentistry[8]. CBCT technology has developed rapidly since it was first used in 1982 at Mayo Clinic Biodynamic Research Laboratory for angiography, radiotherapy and mammography applications. In CBCT technique, a cone-shaped X-ray beam rotates around the patient’s head and collects base images used to construct 3D volumetric data from which multi-planar (axial, sagittal, coronal and cross-sectional) reconstructions can be generated[7,8] (Figure 2). Voxel sizes affect CBCT image quality and alveolar defects can be evaluated with highest accuracy when smaller voxel sizes are utilized[9]. Similarly, accuracy of alveolar bone height measurements are inversely proportional to voxel sizes of CBCT images evaluated[10].
Figure 1.
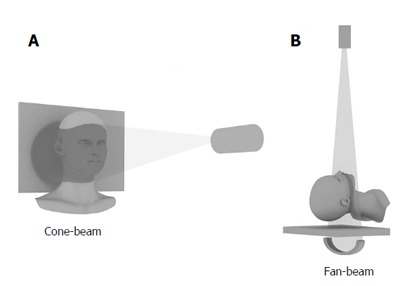
The diagram displays cone-beam and fan-beam shapes in cone beam computed tomography (A) and medical computed tomography (B).
Figure 2.
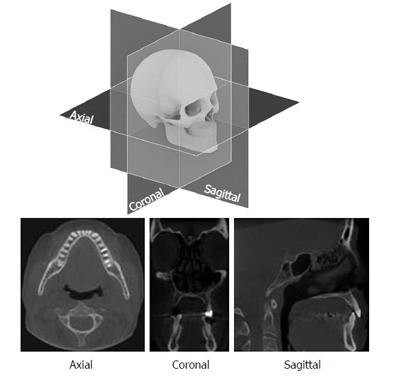
Multi-planar reconstructed images can be generated by cone beam computed tomography volumetric data.
ADVANTAGES OF CBCT
A single rotation is sufficient during irradiation of the patient for acquisition of base projection images and CBCT scanners use two-dimensional flat-panel detectors which provide a scan of the entire region of interest [11,12]. The collimation of the X-ray beam to the area of interest minimizes the radiation dose. Most CBCT units offer different field of view (FOV) options with various sizes (Figure 3). The use of small FOV lowers the effective radiation dose[8-13]. The voxels in CBCT units are isotropic that enables sub-millimeter geometric resolution, thereby; a high degree of measurement accuracy can be obtained (Figure 4). This feature contributes to the high diagnostic capacity of CBCT images obtained from high-density dento-maxillofacial structures such as teeth and bone[8]. Whereas medical CT requires multiple rotations entailing high effective radiation doses, with CBCT, a single rotation is sufficient for the acquisition of base images[8,14,15]. All CBCT units provide axial, coronal and sagittal multi-planar reconstructed images without magnification. Panoramic images can also be generated with curved planar reformation. Multiplanar image can be thickened by increasing the number of adjacent voxels and it is also possible to apply 3D volume rendering and modeling by use of appropriate software package[8,11]. In comparison to medical CT, CBCT offers lower radiation dose and cost along with smaller space requirement[14]. CBCT has better spatial resolution when compared with medical CT[16,17] (Table 1).
Figure 3.
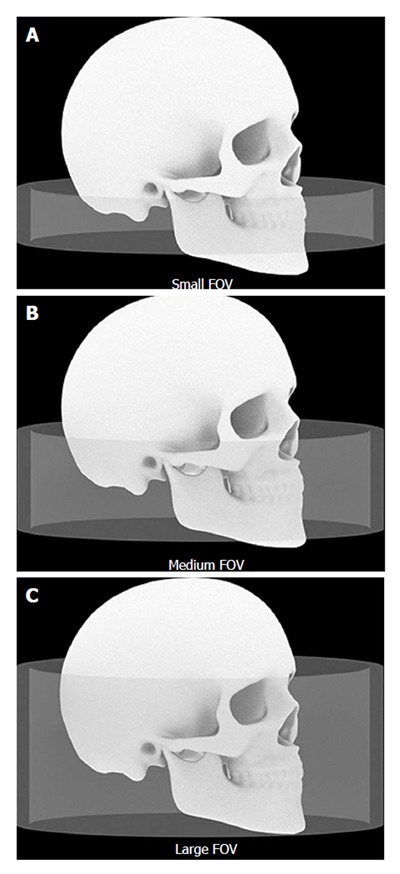
The dimensions of the irradiated regions with different field of view sizes are shown schematically. A: Small FOV; B: Medium FOV; C: Large FOV. FOV: Field of view.
Figure 4.
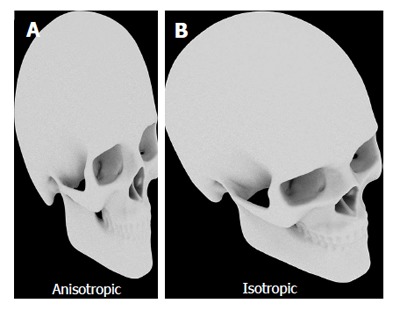
Anisotropic (A) and isotropic (B) 3D images.
Table 1.
Comparison of cone beam computed tomography and medical computed tomography are listed in the table
| CBCT | Medical CT |
| Single rotation | Multiple rotations |
| Lower radiation dose | Higher radiation dose |
| Isotropic voxels | Anisotropic voxels |
| Lower cost | Higher cost |
| Smaller space requirement | Larger devices |
| Better spatial resolution | Better contrast resolution |
| Deficiency to display soft tissues | Clear evaluation of soft tissues |
| Higher scatter radiation | Lower scatter radiation |
CT: computed tomography; CBCT: Cone beam computed tomography.
LIMITATIONS OF CBCT
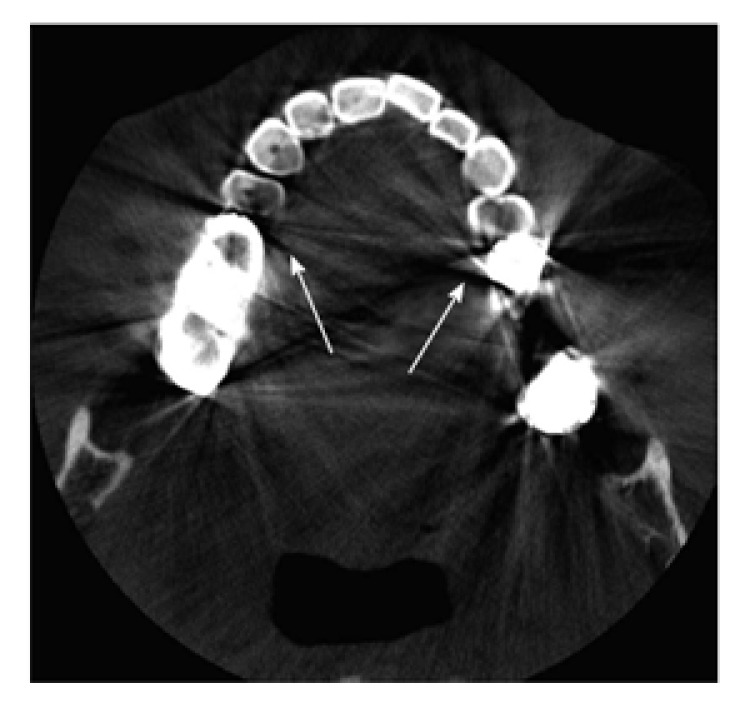
CBCT is not able to offer high contrast resolution and it can not utilized soft tissues, therefore; CBCT is mainly indicated for the evaluation of hard tissues in the dentomaxillofacial complex[11,12]. When compared to 2D imaging, CBCT has higher cost and effective radiation dose but it has lower resolution and lack of availability[13,16,17] (Table 2). Because of the shape of X-ray beam, the scatter radiation is higher in CBCT than with fan-beam tomography. Moreover, the beam-hardening artifacts that comprise radiolucent areas and radiopaque lines can occur more often in CBCT images (Figure 5). A significant limitation of CBCT imaging is the presence of metal artifacts, i.e., image flaws that are unrelated to the scanned object, which are caused by metal and amalgam restorations and, to a lesser extent, root-canal filling material and implants. Such artifacts include streaks around materials as well as dark zones that affect the overall quality of the image. Streak artifacts appear as linear hyperdensities that radiate from a metallic object and may extend to the width of the field, affecting visualization of areas even on the opposite side of an image (Figure 6). Beam-hardening artifacts, which appear as dark bands adjacent to high-density structures, may mimic disease[8,9,18].
Table 2.
The table shows the features of cone beam computed tomography and conventional radiographs
| CBCT | Conventional radiography |
| 3D imaging | 2D imaging |
| Cross-sectional and volumetric images | Superpositions |
| Elimination of image deformity | Distortion and magnification |
| Higher radiation dose | Lower radiation dose |
| Higher cost | Lower cost |
| Larger devices | Smaller space requirement |
CBCT: Cone beam computed tomography.
Figure 5.
Beam-hardening artifacts caused by metal restorations (arrows).
Figure 6.
Streak artifacts are observed as radiopacity in a radial manner (arrows).
RADIOLOGICAL EVALUATION OF PERIODONTAL TISSUES
Radiographs provide information about quantity, localization and pattern of bone resorption, changes in bone trabeculations, conditions of lamina dura and periodontal space, length and shape of teeth roots, ratio of clinical crown length to root length. Some etiological factors of periodontal disease, such as calculus, incompatible restorations may be also seen in radiographs. Inter-proximal areas of maxillary and mandibular teeth can be clearly evaluated in bitewing radiographs because the projection geometry which is applied in this technique does not cause distortion and superposition of the teeth on each other in the image[19,20].
Digital radiographs have not a proven superiority to conventional radiographs in diagnosis, although digital imaging has some distinct practical advantages including the elimination of processing procedure, less radiation dose, shorter exposure and image acquisition times, some benefits that software is allowed such as adjustment of image contrast, density and size[8,21].
CBCT displays two dimensional and three dimensional images that are necessary for the diagnosis and treatment planning of intra bony defects, furcation involvements and buccal/lingual bone destructions[4,7,22] but periapical radiographs have better image quality than CBCT including contrast resolution, clarity and detail[17,23]. Mol et al[19] observed that the CBCT images provided more accurate information on periodontal bone levels in three dimensions than the images of photostimulated phosphor plates. In a similar study, it was found that CBCT was better in morphological description of periodontal bone defects, while the images obtained by charged coupled device sensor provided more bone details[24]. Moreover, it was reported that CBCT and conventional periapical radiographs differed in instead of about measuring the height of the alveolar bone crest but there was not a significant difference between the two methods in detecting the depth and width of bone defects[20]. Mengel et al[25] demonstrated that CBCT images were better in detection of periodontal defects compared with periapical radiographs and medical CT. Likewise, Noujeim et al[26] concluded that CBCT technique has better diagnostic accuracy than periapical films in the detection of interradicular periodontal bone defects.
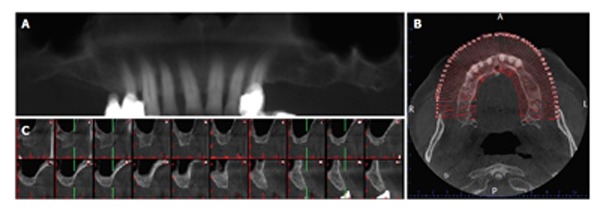
Furcation involvement
An accurate diagnosis of inter radicular bone loss is an important issue prior to the decision of appropriate treatment options including apically repositioned flaps with or without tunnel preparation, root amputation, hemi-/trisection or root separation. Conventional two dimensional radiographs can be deceptive in evaluating periodontal tissue support and inter radicular bone due to superposition of anatomical structures. However, 3D images provide detailed information about areas of multi rooted teeth (Figure 7). CBCT images of maxillary molars provided detailed information of furcation involvement and a reliable basis for treatment decision[23] (Figure 8). Intra-surgical furcation involvement measurements were compared by using CBCT images and it was reported that CBCT images demonstrated a high accuracy in assessing the loss of periodontal tissue and classifying the degree of furcation involvement in maxillary molars[27]. Authors evaluated CBCT images of artificially created furcation involvement of the second molars in pig mandibles and accuracy for furcation lesion detection ranged between 78% and 88%[5]. A study compared dental radiographs and high resolution CT (HR-CT) in detecting and grading of artificial furcation involvements in jaw specimens from cadavers. The diagnostic rate of dental radiographs was 21% whereas HR-CT was 100%[28].
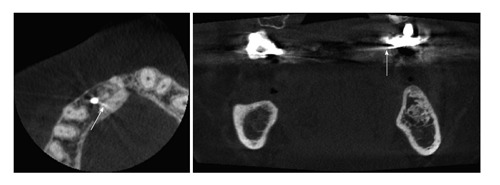
Figure 7.
Furcation involvement can not be observed in the panoramic-like section (A) whereas it can be evaluated in the axial (B) and cross-sectional (C) cone beam computed tomography image (arrows).
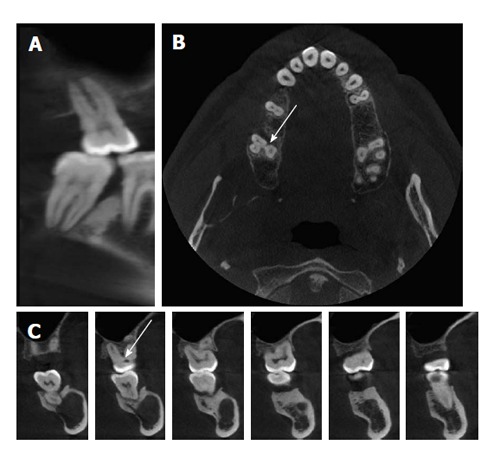
Figure 8.
The amount and shape of bone resorption in the furcation area of maxillary molar tooth can not be assessed in the panoramic-like section (A), however, this involvement is seen in the axial section (B) (arrow).
Soft tissue assessment
CBCT is a more appropriate tool for evaluating mineralized tissues than soft tissues[12]. However, a practical method named soft tissue CBCT (ST-CBCT), was reported[29], and it was utilized to determine the dimensions and relationships of the structures of the dentogingival unit. The tongues were retracted toward the floor of patients’ mouths and a plastic lip retractor was used to retract the soft tissues away from the teeth and gingiva during CBCT scans and the images that were obtained provided clear information for the analysis of various dentogingival unit measurements[29]. Mentioned method was used in another study in which the average thickness of the palatal mucosa according to ages and specific localizations were determined on thirty one patients[30]. The thickness of palatal mucosa has a major importance for the treatment planning of soft tissue grafts. However, this technique provides only quantitative assessment, thus the differences between the epithelial, fat and connective tissues can not be distinguished on ST-CBCT images[29,30].
Periodontal ligament space
The earliest sign of periodontitis that can be detected on radiographs is a wedge-shaped radiolucent area in the inter-proximal region. At this stage, the continuity of lamina dura is lost and some changes in periodontal ligament space can be observed[6,7,16]. Authors compared CBCT with conventional radiography in terms of their ability to produce images of periodontal ligament space on a phantom model with artificially created periodontal ligament of various thicknesses. Periapical radiographs were found to be superior to CBCT for the measurement of periodontal ligament space[6]. However, authors of another study[16] concluded that CBCT images had higher accuracy than intraoral radiographs in the determination of periodontal space in a similar research[16]. Conflicting findings may be attributed to the differences between radiographic systems and settings used in various studies. Visibility of periodontal ligament space using different radiographic techniques should be assessed in further studies.
Alveolar bone defects
Radiographs are frequently utilized to diagnose the amount and shape of alveolar bone destruction that affects treatment planning in periodontal therapy[25]. 2D radiographs can be insufficient for the detection of intra-bony alveolar defects due to obstruction of spongious bone changes by cortical plate. Thus, three-dimensional imaging is required for mapping of alveolar defects[22] (Figure 9). Periodontal defects in pigs and human mandibles were displayed using intraoral radiography, panoramic radiography, CT and CBCT which were compared with histological specimens. The results of the mentioned study showed that 3D imaging had high accuracy in the detection of alveolar defects. Whereas, intraoral and panoramic radiographs could not determine the dehiscence unequivocally, tomographic images displayed all dehiscences and provided accurate measurements of the defects. Authors also reported that CBCT displayed the best imaging quality[25]. Authors evaluated periodontal defects in human dry cadaver skulls using CBCT and traditional methods. Consequently, they found that there was no difference between intraoral radiography and CBCT in linear measurements for all defects[22]. In another study[31], authors evaluated accuracy and reliability of CBCT for measuring alveolar bone height and detecting bony dehiscence and fenestration. CBCT measurements were found to be equivalent to direct measurements and dehiscences were diagnosed with higher accuracy than fenestrations[31]. CBCT and multi-slice CT (MSCT) images were used for alveolar bone width measurements[18]. There was no significance difference between the measurements obtained by CBCT and MSCT or direct measurements and radiographic methods[18].
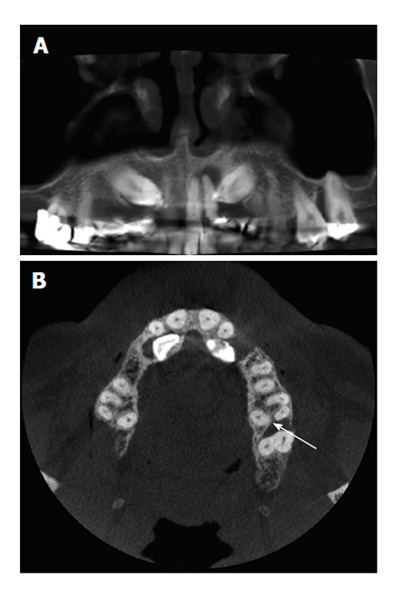
Figure 9.
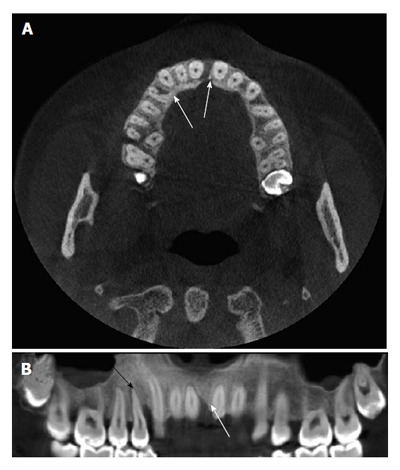
The vertical alveolar bone defects are viewed in cone beam computed tomography images (A, B) (white arrows) and the expansion of periodontal ligament space is also seen in the right maxillary first premolar tooth (B) (black arrow).
Regenerative periodontal therapy and bone grafts
Bone grafting is commonly used for maxillary sinus lifting and treatment of intra bony defects but evaluation of osseous defect regeneration with conventional radiography can be insufficient due to superimpositions[25,32]. Furthermore, histological evaluation of a sample of the graft is not a preferred method due to its quite invasive procedure. CBCT was found to be significantly more accurate than digital intraoral radiographs when direct surgical measurements served as the gold standard for the evaluation of intra-bony defects’ regenerative treatment outcomes. CBCT can replace surgical re-entry by providing 3D images and measurements that are almost equivalent to direct surgical measurements[32].
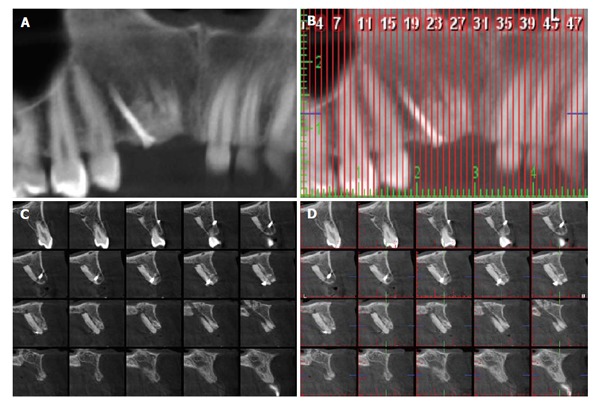
Dimensions of alveolar process should be examined in detail prior to dental implant placement to avoid various complications and evaluation of CBCT images has a major importance in preoperative planning and postoperative localization of dental implants[8,33] (Figure 10). Moreover, the evaluation of CBCT images are preferred method to observe bone graft healing prior to dental implant placement[17] (Figure 11). In a previous study[33], which was based on measurement accuracy and reliability of CBCT and MSCT with the specific implant planning software package and the stereolithographic drill guide, authors applied implant surgeries in a one-stage flapless procedure. The deviations were acceptable and no complications were observed[33]. In contrary, authors of another study concluded that CBCT may be deceptive compared to direct caliper measurements and they found that ridge mapping method gave more accurate results than CBCT[34]. However, ridge mapping technique is an invasive technique whereas CBCT is not.
Figure 10.
The images acquired for preoperative implant planning are displayed the distances between the alveolar process of maxillary molar areas and the bases of the maxillary sinuses (A), a curve is projected on the axial section (B) and the cross-sectional images are obtained (C).
Figure 11.
The block graft and mini screw providing graft stabilization are placed in the maxillary anterior region (A and B), the amount of bone augmentation can be evaluated in the cross-sectional images (C and D).
CBCT evaluation can be used for determining the width, height and distance to the anatomical structures of alveolar process in pre-surgical dental implant planning. Likewise, the surgical guide stents were used while dental implant surgery was produced by aid of CBCT images and software packages[17]. Immediate implant placement enables one-stage surgery and eliminates bone recovery time. In this technique, dimensions of alveolar process which is selected for dental implant placement and relationships with adjacent anatomical structures of this region should be carefully assessed[8,35]. Jin et al[35] studied bone thickness evaluation on the buccal and palatal aspects of the maxillary canine and premolars using CBCT and it was concluded that CBCT images might be advantageous in preoperative planning of dental implants[35].
As a summary, in cases, where two-dimensional imaging is an inadequate method for accurate diagnosis of periodontal defect configuration and guiding for appropriate treatment planning, three-dimensional radiographic examinations may be required. Periodontal intra-bony defects and furcation involvements keep a challenge for the examiner. Misdiagnosed or misclassification of these pathologies can lead to progress of bone destruction and teeth loss as a result of improper treatment[5,16]. CBCT evaluation can be used for determining the width, height and distance to the anatomical structures of alveolar process in pre-surgical dental implant planning. Likewise, the surgical guide stents used during dental implant surgery is produced by aid of CBCT images and software packages[17]. There are numerous studies that 3D imaging had high accuracy in the detection of alveolar defects and furcation involvements[18,25,27,28,31]. CBCT is well complied for imaging the highly mineralized structures such as bone or teeth but it cannot provide clear images of soft tissues. However, a novel, CBCT-based method to display and measure the dimensions of the palatal mucosa was reported in a recent study[29,30]. There are contradictory results on whether CBCT or conventional radiographs are more efficient in evaluation of periodontal ligament space[6,16].
Assessment of regenerative periodontal therapy and bone grafts’ outcomes can be performed accurately and reliably with CBCT imaging[17,32]. In conclusion, CBCT applications provide obvious benefits in periodontology, although it should be used when two-dimensional radiographs are insufficient considering the necessity and the potential radiation hazards of the examination[36].
Footnotes
P- Reviewers: Ma YL, Oliveira L, Santos FA S- Editor: Ji FF L- Editor: A E- Editor: Liu SQ
References
- 1.Lindhe J, Lang NP, Karring T. Clinical periodontology and implant dentistry. In: Lindhe J, Karring T, Araújo M, editors. The anatomy of periodontal tissues. Singapore: Blackwell Publishing Ltd; 2008. pp. 3–8. [Google Scholar]
- 2.Highfield J. Diagnosis and classification of periodontal disease. Aust Dent J. 2009;54 Suppl 1:S11–S26. doi: 10.1111/j.1834-7819.2009.01140.x. [DOI] [PubMed] [Google Scholar]
- 3.Newman M, Takei HH, Carranza FA. Clinical Periodontology. In: Carranza FA, Takei HH, editors. Radiographic Aids in the Diagnosis of Periodontal Disease. Philadelphia: W.B. Saunders Company; 2002. pp. 454–468. [Google Scholar]
- 4.du Bois AH, Kardachi B, Bartold PM. Is there a role for the use of volumetric cone beam computerized tomography in periodontics? Aust Dent J. 2012;57 Suppl 1:103–108. doi: 10.1111/j.1834-7819.2011.01659.x. [DOI] [PubMed] [Google Scholar]
- 5.Umetsubo OS, Gaia BF, Costa FF, Cavalcanti MG. Detection of simulated incipient furcation involvement by CBCT: an in vitro study using pig mandibles. Braz Oral Res. 2012;26:341–347. doi: 10.1590/s1806-83242012000400010. [DOI] [PubMed] [Google Scholar]
- 6.Ozmeric N, Kostioutchenko I, Hägler G, Frentzen M, Jervøe-Storm PM. Cone-beam computerized tomography in assessment of periodontal ligament space: in vitro study on artificial tooth model. Clin Oral Investig. 2008;12:233–239. doi: 10.1007/s00784-008-0186-8. [DOI] [PubMed] [Google Scholar]
- 7.Mohan R, Singh A, Gundappa M. Three-dimensional imaging in periodontal diagnosis - Utilization of cone beam computerized tomography. J Indian Soc Periodontol. 2011;15:11–17. doi: 10.4103/0972-124X.82256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Scarfe WC, Farman AG, Sukovic P. Clinical applications of cone-beam computerized tomography in dental practice. J Can Dent Assoc. 2006;72:75–80. [PubMed] [Google Scholar]
- 9.de-Azevedo-Vaz SL, Vasconcelos Kde F, Neves FS, Melo SL, Campos PS, Haiter-Neto F. Detection of periimplant fenestration and dehiscence with the use of two scan modes and the smallest voxel sizes of a cone-beam computerized tomography device. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;115:121–127. doi: 10.1016/j.oooo.2012.10.003. [DOI] [PubMed] [Google Scholar]
- 10.Sun Z, Smith T, Kortam S, Kim DG, Tee BC, Fields H. Effect of bone thickness on alveolar bone-height measurements from cone-beam computerized tomography images. Am J Orthod Dentofacial Orthop. 2011;139:e117–e127. doi: 10.1016/j.ajodo.2010.08.016. [DOI] [PubMed] [Google Scholar]
- 11.Shah MA, Shah SS, Dave DH. CBCT-A Positive Amelioration In Periodontics. NJIRM. 2013;4:144–148. [Google Scholar]
- 12.Agrawal P, Sanikop S, Patil S. New developments in tools for periodontal diagnosis. Int Dent J. 2012;62:57–64. doi: 10.1111/j.1875-595X.2011.00099.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tyndall DA, Rathore S. Cone-beam CT diagnostic applications: caries, periodontal bone assessment, and endodontic applications. Dent Clin North Am. 2008;52:825–41, vii. doi: 10.1016/j.cden.2008.05.002. [DOI] [PubMed] [Google Scholar]
- 14.Mischkowski RA, Pulsfort R, Ritter L, Neugebauer J, Brochhagen HG, Keeve E, Zöller JE. Geometric accuracy of a newly developed cone-beam device for maxillofacial imaging. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:551–559. doi: 10.1016/j.tripleo.2007.02.021. [DOI] [PubMed] [Google Scholar]
- 15.Veyre-Goulet S, Fortin T, Thierry A. Accuracy of linear measurement provided by cone beam computerized tomography to assess bone quantity in the posterior maxilla: a human cadaver study. Clin Implant Dent Relat Res. 2008;10:226–230. doi: 10.1111/j.1708-8208.2008.00083.x. [DOI] [PubMed] [Google Scholar]
- 16.Jervøe-Storm PM, Hagner M, Neugebauer J, Ritter L, Zöller JE, Jepsen S, Frentzen M. Comparison of cone-beam computerized tomography and intraoral radiographs for determination of the periodontal ligament in a variable phantom. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109:e95–e101. doi: 10.1016/j.tripleo.2009.10.023. [DOI] [PubMed] [Google Scholar]
- 17.Eshraghi T, McAllister N, McAllister B. Clinical applications of digital 2-D and 3-D radiography for the periodontist. J Evid Based Dent Pract. 2012;12:36–45. doi: 10.1016/S1532-3382(12)70010-6. [DOI] [PubMed] [Google Scholar]
- 18.Loubele M, Van Assche N, Carpentier K, Maes F, Jacobs R, van Steenberghe D, Suetens P. Comparative localized linear accuracy of small-field cone-beam CT and multislice CT for alveolar bone measurements. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105:512–518. doi: 10.1016/j.tripleo.2007.05.004. [DOI] [PubMed] [Google Scholar]
- 19.Mol A, Balasundaram A. In vitro cone beam computerized tomography imaging of periodontal bone. Dentomaxillofac Radiol. 2008;37:319–324. doi: 10.1259/dmfr/26475758. [DOI] [PubMed] [Google Scholar]
- 20.de Faria Vasconcelos K, Evangelista KM, Rodrigues CD, Estrela C, de Sousa TO, Silva MA. Detection of periodontal bone loss using cone beam CT and intraoral radiography. Dentomaxillofac Radiol. 2012;41:64–69. doi: 10.1259/dmfr/13676777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Gomes-Filho IS, Sarmento VA, de Castro MS, da Costa NP, da Cruz SS, Trindade SC, de Freitas CO, de Santana Passos J. Radiographic features of periodontal bone defects: evaluation of digitized images. Dentomaxillofac Radiol. 2007;36:256–262. doi: 10.1259/dmfr/25386411. [DOI] [PubMed] [Google Scholar]
- 22.Misch KA, Yi ES, Sarment DP. Accuracy of cone beam computerized tomography for periodontal defect measurements. J Periodontol. 2006;77:1261–1266. doi: 10.1902/jop.2006.050367. [DOI] [PubMed] [Google Scholar]
- 23.Walter C, Kaner D, Berndt DC, Weiger R, Zitzmann NU. Three-dimensional imaging as a pre-operative tool in decision making for furcation surgery. J Clin Periodontol. 2009;36:250–257. doi: 10.1111/j.1600-051X.2008.01367.x. [DOI] [PubMed] [Google Scholar]
- 24.Vandenberghe B, Jacobs R, Yang J. Diagnostic validity (or acuity) of 2D CCD versus 3D CBCT-images for assessing periodontal breakdown. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:395–401. doi: 10.1016/j.tripleo.2007.03.012. [DOI] [PubMed] [Google Scholar]
- 25.Mengel R, Candir M, Shiratori K, Flores-de-Jacoby L. Digital volume tomography in the diagnosis of periodontal defects: an in vitro study on native pig and human mandibles. J Periodontol. 2005;76:665–673. doi: 10.1902/jop.2005.76.5.665. [DOI] [PubMed] [Google Scholar]
- 26.Noujeim M, Prihoda T, Langlais R, Nummikoski P. Evaluation of high-resolution cone beam computerized tomography in the detection of simulated interradicular bone lesions. Dentomaxillofac Radiol. 2009;38:156–162. doi: 10.1259/dmfr/61676894. [DOI] [PubMed] [Google Scholar]
- 27.Walter C, Weiger R, Zitzmann NU. Accuracy of three-dimensional imaging in assessing maxillary molar furcation involvement. J Clin Periodontol. 2010;37:436–441. doi: 10.1111/j.1600-051X.2010.01556.x. [DOI] [PubMed] [Google Scholar]
- 28.Fuhrmann RA, Bücker A, Diedrich PR. Furcation involvement: comparison of dental radiographs and HR-CT-slices in human specimens. J Periodontal Res. 1997;32:409–418. doi: 10.1111/j.1600-0765.1997.tb00553.x. [DOI] [PubMed] [Google Scholar]
- 29.Januário AL, Barriviera M, Duarte WR. Soft tissue cone-beam computerized tomography: a novel method for the measurement of gingival tissue and the dimensions of the dentogingival unit. J Esthet Restor Dent. 2008;20:366–373; discussion 374. doi: 10.1111/j.1708-8240.2008.00210.x. [DOI] [PubMed] [Google Scholar]
- 30.Barriviera M, Duarte WR, Januário AL, Faber J, Bezerra AC. A new method to assess and measure palatal masticatory mucosa by cone-beam computerized tomography. J Clin Periodontol. 2009;36:564–568. doi: 10.1111/j.1600-051X.2009.01422.x. [DOI] [PubMed] [Google Scholar]
- 31.Leung CC, Palomo L, Griffith R, Hans MG. Accuracy and reliability of cone-beam computerized tomography for measuring alveolar bone height and detecting bony dehiscences and fenestrations. Am J Orthod Dentofacial Orthop. 2010;137:S109–S119. doi: 10.1016/j.ajodo.2009.07.013. [DOI] [PubMed] [Google Scholar]
- 32.Grimard BA, Hoidal MJ, Mills MP, Mellonig JT, Nummikoski PV, Mealey BL. Comparison of clinical, periapical radiograph, and cone-beam volume tomography measurement techniques for assessing bone level changes following regenerative periodontal therapy. J Periodontol. 2009;80:48–55. doi: 10.1902/jop.2009.080289. [DOI] [PubMed] [Google Scholar]
- 33.Van Assche N, van Steenberghe D, Quirynen M, Jacobs R. Accuracy assessment of computer-assisted flapless implant placement in partial edentulism. J Clin Periodontol. 2010;37:398–403. doi: 10.1111/j.1600-051X.2010.01535.x. [DOI] [PubMed] [Google Scholar]
- 34.Chen LC, Lundgren T, Hallström H, Cherel F. Comparison of different methods of assessing alveolar ridge dimensions prior to dental implant placement. J Periodontol. 2008;79:401–405. doi: 10.1902/jop.2008.070021. [DOI] [PubMed] [Google Scholar]
- 35.Jin SH, Park JB, Kim N, Park S, Kim KJ, Kim Y, Kook YA, Ko Y. The thickness of alveolar bone at the maxillary canine and premolar teeth in normal occlusion. J Periodontal Implant Sci. 2012;42:173–178. doi: 10.5051/jpis.2012.42.5.173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kamburoğlu K, Acar B, Yakar EN, Paksoy CS. Dento-maxillofacial Cone Beam computerized Tomography Part 1: Basic Principles (Dentomaksillofasiyal Konik Işın Demetli Bilgisayarlı Tomografi Bölüm 1: Temel Prensipler) J Clin Sc. 2012;6:1125–1136. [Google Scholar]