

Abstract
Background:
Traumatic brain injury (TBI) has an immense psychosocial impact on an individual as well as on the close relatives. Sexuality is one among the functions which are usually found compromised post injury. The aim of present study was to examine cognitive and sexual functions post TBI. The objective of the study was to explore these domains and their relationship with each other.
Tools:
The tools used were sociodemographics record sheet, Edinburg handedness inventory, brief sexual function inventory, depression anxiety stress scales-21 and NIMHANS head injury battery. The sample consisted of 30 patients with mild-to-moderate TBI. All the subjects were tested individually in their regional language.
Results:
On cognitive domain, patients performed inadequately on all the tests; however, the percentage was higher in mental speed (43.3%), sustained attention (26.7%), verbal working memory (30%), response inhibition (36.7%), verbal memory (immediate and delayed) (43%) and visual (immediate, 23.3% and delayed, 26.7%). On the domain of sexual functions, all the four domains (sexual drive, erection, ejaculation and problem assessment) were affected however overall satisfaction (93.3%) was adequate. Among the four domains higher percentage of involvement was noted on problem assessment (70%), ejaculation (56.7%), and erection (46.7%). Significant correlation was found between mental speed, verbal working memory, planning, and visual memory with sexual drive, erection, ejaculation and overall satisfaction domains of sexual functioning. Negative correlation was found between motor speed and sustained attention with sexual drive, erection and ejaculation.
Conclusion:
Both cognitive and sexual functioning were found effected post TBI. However less emphasis is given to sexual functioning by the professionals. Educational intervention is needed to sensitize professional about this area and to include this area for better management.
Keywords: Cognitive, sexuality, traumatic brain injury
Introduction
TBI is “an alteration in brain function manifest as confusion, altered level of consciousness, seizure, coma, or focal sensory or motor neurological deficit resulting from blunt or penetrating force to the head”.[1] Literature shows it not only affects the injured but also disturbs the whole family system and society at large which makes it a global health problem.[2] Damage to brain tissue affects an individual at different levels. At cognitive level attention,[3] information processing,[4] memory[4] and behavioral problems in the form of irritability, disinhibition, low frustration and poor motivation[5,6] are mostly reported. Gradual improvement in cognitive symptoms is reported over time.[3]
At sexual level, lack of sexual drive,[7,8] ejaculation and erection[7] are commonly reported. The impact upon sexuality has been reported by number of studies, between 50 and 60% of people reporting some level of sexual disruption post injury,[9] which further worsens the adjustment with the environment and overall well-being. The stresses and strains produced can be bad for relationships in many different ways. There is paucity of studies focusing on sexual functioning in TBI especially at national level. So exploring this area will help in better management.
Materials and Methods
Participants
A sample of 30 male patients, post three months of mild-to-moderate traumatic brain injury were taken from the outpatient services of the Department of Neurosurgery and Neuropsychology of the NIMHANS, Bangalore. The age range was between 20 and 55 years (Mean = 38.13 and SD = 8.82). Out of 30 patients, 60% were with mild and 40% were moderate TBI (Mean = 12.77; SD = 1.85) on Glasgow Coma Scale (GCS). The time duration following injury ranged from 3 to 53 months, with a mean of 12.43 months (SD = 12.95). Patients with other pre-existing neurological and psychiatric histories were excluded.
Tools
Sociodemographic data sheet was developed regarding information about patients. The patients were assessed on NIMHANS neuropsychological battery and self-report questionnaires, which were translated in regional languages. Participants were tested individually. Edinburg Handedness Inventory[10] was used to assess handedness. It consisted of ten items relating to the use of hands. Depression Anxiety Stress Scales-21[11] is a 14 items self-report scales designed to measure the negative emotional states of depression, anxiety and stress. It is a four-point rating scale with high internal consistency of subscales (Cronbach's alphas). Brief Sexual Function Inventory (BSFI)[12] is 11 items brief, self-administered measure of current sexual functioning. The items cover sexual drive, erection, ejaculation, whereas the other questions focus on subjective problem assessment about drive, erection and ejaculation and overall satisfaction. The scaling is from zero (big problem) to four (no problem). It has an internal consistency and retest coefficients of 0.62-0.95 and 0.79-0.90, respectively. NIMHANS head injury battery[13] was used to assess cognitive functions. The tests have been standardized on Indian population with an age range of 16-65 for both literate and illiterate males and females. The tests selected for the current study are the following: Tests of speed includes Finger tapping test and Digit symbol substitution test, Tests of attention includes Digit Vigilance, Tests of executive functions includes Category Fluency, N-Back test for verbal working memory, Tower of London, Wisconsin Card Sorting Test and Stroop Color Word Test, test of comprehension includes Token test, Test of learning and memory includes Rey's Auditory Verbal Learning Test (AVLT) and Rey's Complex Figure Test (CFT).
Results
Table 1 shows the mean, standard deviation and percentage of adequate and inadequate performance on different neuropsychological tests. Patients performed inadequately on most of the tests. Here we have mentioned the results of tests on which percentage was higher. It is evident from the table that patients have performed inadequately on basic as well as higher cognitive functions; however the percentage is higher on basic functioning.
Table 1.
Performance on neuropsychological tests
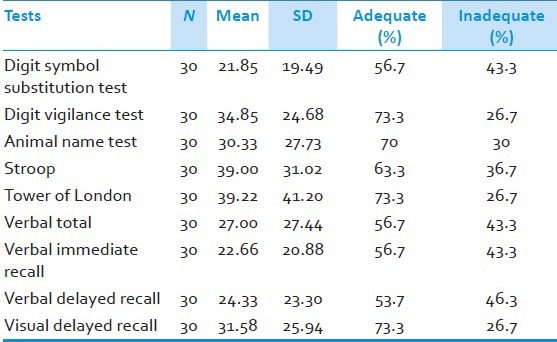
Table 2 shows mean, standard deviation and percentage of adequate and inadequate performance in different domains of sexual functions. Patients have reported higher dysfunctions in all the domains; however, patients seem satisfied with their overall sexual life.
Table 2.
Brief sexual function inventory

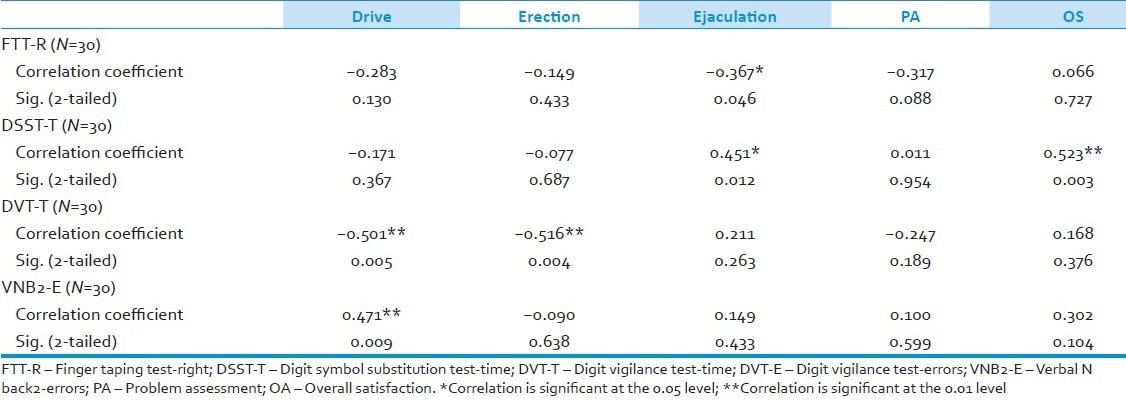
Table 3 shows correlation between neuropsychological tests and different domains of sexual functions. As evident from the table, significant negative correlation was found between motor function and ejaculation at 0.05 level of significance. Significant negative correlation was also found between sustained attention, drive and erection at 0.01 level of significance. Significant positive correlation was found mental speed, working speed, ejaculation and problem assessment at 0.01 level of significance.
Table 3.
Correlation between cognitive and sexual functioning
Discussion
This study tried to explore cognitive and sexual functioning post injury. Among both the domains, cognitive domain is a well-researched and documented area in the field of neuropsychology especially in patients with mild-to-moderate TBI. Cognitive functions include basic to highly complex functions. In the current study patients performed inadequately on most of the neuropsychological tests. However the percentage was found higher on some of the domains which are discussed below.
Performance on neuropsychological tests
Attention is a basic element of cognition which makes it important for other cognitive functions as well. In order to perform any activity one need to attend and process it mentally and then make appropriate movements to perform any work. In the current study 43.3% and 26.6% of patients were having deficits in attention and mental processing, respectively. Once the information is attended and processed we need to encode, retrieve and store it in order to perform a task when needed in future. 43.3%, 43.3%, 46.3% and 26.7% of patients were having deficits on learning, immediate verbal memory, delayed verbal memory and delayed visual memory, respectively, in the current study. In order to execute a function one need to activate, organize, integrate and manage other functions which are referred as executive functions. It enables individuals to plan ahead keeping consequences in mind and to evaluate their actions. In the current study, results showed 30%, 36.7% and 26.7% patient were having deficits on working memory, response inhibition and planning. These test findings are suggestive of involvement of prefrontal cortex and bilateral temporal lobe. These findings are supported by previous studies on TBI.[14,15,3]
Sexual functioning
The results showed that overall satisfaction with sexual life was not affected. However different domains of sexual functioning like sexual drive, erection, ejaculation were affected.[7,16] Higher percentage of patients reported having problem in sexual functioning on problem assessment domain. However on overall satisfaction domain, most patients reported satisfied with their overall sexual life (93.3%).[16] In this domain the patient's subjective feeling of how much one is satisfied with his sexual relationship was measured.
Recent research in the field of sexuality is suggesting important role of personal factors in sexual intimacy but these factors must be seen within the family, interpersonal, society and cultural context.[17] India being a conservative society does not allow free expression of sexual issues at individual and family level. It also receives less importance and priority in comparison to other areas, which may have led to higher level of satisfaction in spite of dysfunction in all the four areas.
Correlation between cognitive and sexual functioning
The second objective of the study was to examine the relationship between cognitive and sexual functions. Studies have shown that sexual behavior is monitored by different parts of the brain especially the frontal lobe and temporal lobe.[18,19,20] Results from the current study showed significant correlation between different cognitive functions and different domains of sexual functioning. These cognitive functions are controlled by different parts of the brain. However it is difficult to point out to specific regions of the brain considering the complexity of sexual response and other factors which affect human sexual response.[17,21,22] If we analyze above results it is clear that frontal especially prefrontal lobe plays a role in sexual functioning as we have seen cognitive functions controlled by these areas are significantly correlated with sexual functioning.[20,21,22]
Limitations
The study could not include female subjects because of cultural taboos and comfort level observed during the pilot phase of the study. Also frequency of TBI is observed higher in males than females. In the current study more than 135 married male patients were screened, out of which only 39 met the inclusion and exclusion criteria. Out of 39 patients, only 30 gave the consent for participation. Considering the small size purposive sampling it may be difficult to generalize these findings. However this study highlights the need for emphasis on sexual functioning, which plays important role in overall adjustment of an individual within a society.[16] Lack of comparison or control group because of time constraint would have helped to understand if these problems are really specific to the given population and culture.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Bruns J, Hauser W. The epidemiology of traumatic brain injury: A review. Epilepsia. 2003;44:2–10. doi: 10.1046/j.1528-1157.44.s10.3.x. [DOI] [PubMed] [Google Scholar]
- 2.Ghajar J. Traumatic brain injury. Lancet. 2000;356:923–9. doi: 10.1016/S0140-6736(00)02689-1. [DOI] [PubMed] [Google Scholar]
- 3.Kwok FY, Lee TM, Leung CH, Poon WS. Changes of cognitive functioning following mild traumatic brain injury over a 3-month period. Brain Injury. 2008;22:740–51. doi: 10.1080/02699050802336989. [DOI] [PubMed] [Google Scholar]
- 4.Rajkumari K, Jamuna N, Devi BI. Bangalore: National Institute of Mental Health and Neurosciences; 2011. Neurofeedback training in patients with traumatic brain injury. [Google Scholar]
- 5.Baguley IJ, Cooper J, Felmingham K. Aggressive behavior following traumatic brain injury: How common is common? J Head Trauma Rehabil. 2006;21:45–56. doi: 10.1097/00001199-200601000-00005. [DOI] [PubMed] [Google Scholar]
- 6.Deb S, Lyons I, Koutzoukis C. Neuropsychiatric sequelae one year after a minor head injury. J Neurol Neurosurg Psychiatry. 1998;65:899–902. doi: 10.1136/jnnp.65.6.899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ponsford J. Sexual changes associated with traumatic brain injury. Neuropsychol Rehabil. 2003;13:275–89. doi: 10.1080/09602010244000363. [DOI] [PubMed] [Google Scholar]
- 8.Hibbard MR, Gordon W, Flanagan S, Haddad L, Labonsky E. Sexual dysfunction after traumatic brain injury. Neuro Rehabil. 2000;15:107–20. [PubMed] [Google Scholar]
- 9.Kreuter M, Dahllof A, Gudjonsson F, Sullivan M, Siosteen A. Sexual adjustment and its predictors after traumatic brain injury. Brain Injury. 1998;12:209–17. [Google Scholar]
- 10.Oldfield RC. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia. 1971;9:97–113. doi: 10.1016/0028-3932(71)90067-4. [DOI] [PubMed] [Google Scholar]
- 11.Lovibond SH, Lovibond PF. 2nd ed. Sydney: Psychology Foundation; 1995. Manual for the Depression Anxiety Stress Scales. [Google Scholar]
- 12.O’Leary MP, Fowler FJ, Lenderking WR, Barber B, Sagnier PP, Guess HA, et al. A brief male sexual function inventory for urology. Urology. 1995;46:697–706. doi: 10.1016/S0090-4295(99)80304-5. [DOI] [PubMed] [Google Scholar]
- 13.Rao SL, Subbakrishna DK, Gopukumar K. Bangalore: NIMHANS Publications; 2004. NIMHANS Neuropsychology Battery. [Google Scholar]
- 14.Atchison TB, Sander AM, Struchen MA, High WM, Jr, Roebuck TM, Contant CF. Relationship between neuropsychological test performance and productivity at 1-year following traumatic brain injury. Clin Neuropsychol. 2004;18:249–65. doi: 10.1080/13854040490501475. [DOI] [PubMed] [Google Scholar]
- 15.Zec RF, Zellers D, Belman J, Miller J, Matthews J, Femeau-Belman D. Long-term consequences of severe closed head injury on episodic memory. J Clin Exp Neuropsychol. 2001;23:671–91. doi: 10.1076/jcen.23.5.671.1247. [DOI] [PubMed] [Google Scholar]
- 16.Sander AM, Maestas KL, Pappadis MR, Sherer M, Hammond FM, Hanks R. Sexual functioning one year after traumatic brain injury: Findings from a prospective traumatic brain injury model systems collaborative study. Arch Physical Med Rehabil. 2012;93:1331–7. doi: 10.1016/j.apmr.2012.03.037. [DOI] [PubMed] [Google Scholar]
- 17.Basson R. The female sexual response: A different model. J Sex Marital Therapy. 2000;26:51–65. doi: 10.1080/009262300278641. [DOI] [PubMed] [Google Scholar]
- 18.Sabhesan S, Natarajan M. Sexual behaviour after head injury in Indian men and women. Arch Sexual Behav. 1989;18:671–91. doi: 10.1007/BF01541953. [DOI] [PubMed] [Google Scholar]
- 19.Park K, Seo JJ, Kang HK, Ryu SB, Kim HJ, Jeon GW. A new potential of blood oxygenation level dependent (BOLD) functional MRI for evaluating cerebral centers of penile erection. Int J Impot Res. 2001;13:73–81. doi: 10.1038/sj.ijir.3900649. [DOI] [PubMed] [Google Scholar]
- 20.Redoute J, Stoleru S, Gregoire MC, Costes N, Cinotti L, Lavenne F, et al. Brain processing of visual sexual stimuli in human males. Hum Brain Mapping. 2000;11:162–77. doi: 10.1002/1097-0193(200011)11:3<162::AID-HBM30>3.0.CO;2-A. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Katz S, Aloni R. Sexual dysfunction of persons after traumatic brain injury: perceptions of professionals. Int J Rehabil Res. 1999;22:45–53. doi: 10.1097/00004356-199903000-00006. [DOI] [PubMed] [Google Scholar]
- 22.Baird AD, Wilson SJ, Bladin PF, Saling MM, Reutens DC. Neurological control of human sexual behaviour: Insight from lesion studies. J Neurol Neurosurg Psychiatry. 2007;78:1042–9. doi: 10.1136/jnnp.2006.107193. [DOI] [PMC free article] [PubMed] [Google Scholar]