

Abstract
Most giant pheochromocytomas do not present with classic symptoms, as documented by published case reports. Given this, clinicians have to consider a wide differential diagnosis for any retroperitoneal mass and perform screening tests to rule out a pheochromocytoma. We describe the largest pheochromocytoma reported in Canada, where the patient presented with a palpable abdominal mass and dyspnea. The 19 × 18 × 12-cm right retroperitoneal mass was biochemically active and was radiologically and pathologically consistent with a giant pheochromocytoma. We present this case and review the relevant current literature.
Introduction
Pheochromocytoma (PCC) is a catecholamine-secreting tumour from chromaffin cells of the embryonic neural crest. It has an estimated incidence of 0.1% in the general population.1,2 Sporadic disease usually strikes in the fourth and fifth decades of life, affecting both genders equally.3 PCCs are bilateral, malignant, pediatric, or asymptomatic in 10% of cases.4 Hereditary PCC is associated with von Hippel-Lindau (VHL) syndrome, multiple endocrine neoplasia type 2 (MEN-2A/2B), neurofibromatosis type 1 (NF1), and hereditary pheochromocytoma-paraganglioma (due to mitochondrial succinate dehydrogenase gene mutations).1,5 PCC classically presents with the quartet of episodic headaches, palpitations, diaphoresis, and hypertension.6
Case report
A 77-year-old female with an unremarkable medical history, apart from taking levothyroxine for hypothyroidism, presented to her family physician with dyspnea. She denied any palpitations, chest pain, abdominal pain or constitutional symptoms. Her family history was negative for genitourinary malignancies and syndromes. A cardiovascular etiology was suspected and she was referred to a cardiologist. Her cardiology workup was unremarkable, including no hypertension, but on physical examination the cardiologist palpated a large right upper quadrant abdominal mass. Imaging of the mass and a consultation to urology were arranged.
A computed tomography (CT) scan of the abdomen and pelvis demonstrated a large right retroperitoneal mass (Fig. 1a, Fig. 1b) measuring 19 × 18 × 12 cm. The mass was predominantly cystic with irregular wall thickness and multiple septations containing calcification. The normal configuration of the right adrenal gland was indistinguishable from the mass. The mass was separate from the right kidney but displaced it anteriorly across the midline and additionally compressed the right lower lobe of the liver. In addition, a 2.3-cm enhancing left adrenal mass was discovered. There was no evidence of distant metastases. The differential diagnosis included a primary adrenal mass (adrenocortical carcinoma, metastasis, or pheochromocytoma), sarcoma, lymphoma and a giant hemangioma. To rule out a functional adrenal mass, we ordered biochemical studies. In the end, we confirmed the pheochromocytoma (Table 1).
Fig. 1a.
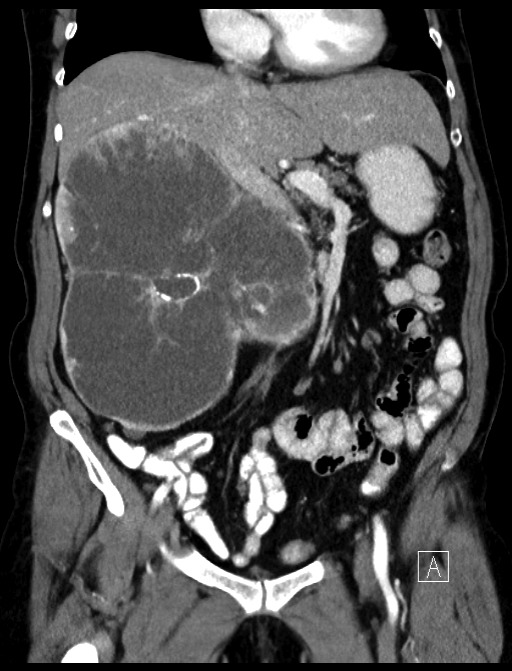
Large mass on computed tomography scan (coronal section).
Fig. 1b.
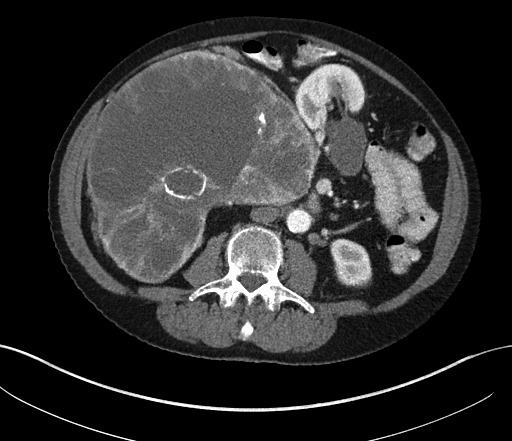
Large mass seen on computed tomography scan (axial section).
Table 1.
24-hour urine values
| Test | Value | Normal |
|---|---|---|
| Creatinine | 10.34 mmoL/day | 5.3–13 mmoL/day |
| Metanephrines | 180 mmoL/day | 0.8–5.4 mmoL/day |
| Normetanephrines | >90 mmoL/day | 0.8–4.4 mmoL/day |
| Vanillylmandelate (VMA) | 510 mmoL/day | 9–34 mmoL/day |
| Homovanillate (HVA) | 66 μmoL/day | 0–82 μmoL/day |
| Epinephrine | 1467 nmoL/day | <125 nmoL/day |
| Norepinephrine | 343 nmoL/day | <505 nmoL/day |
| Catecholamines | 1810 nmoL/day | <630 nmoL/day |
A 123-I Meta-Iodobenzylguanidine (MIBG) scan was arranged demonstrating avid uptake of radiotracer to the right retroperitoneal mass only (Fig. 2). After a preoperative medical consult and adequate preoperative catecholamine blockade, the patient underwent bilateral open adrenal-ectomies with a chevron incision. Intraoperatively, there were no surgical complications; however, given the size of the mass, it was difficult to isolate the adrenal vein early and subsequent manipulation of the mass resulted in blood pressure fluctuations, despite preoperative blockade. She was discharged on steroid replacement and a follow-up was scheduled 6 months later. Histology confirmed a giant PCC with capsular invasion (1 point), vascular invasion (1 point), and a diffuse growth pattern (2 points), giving her a Pheochromocytoma of the Adrenal Gland Scaled (PASS) score of 4. The left adrenal gland pathology demonstrated a benign adrenal adenoma.
Fig. 2.
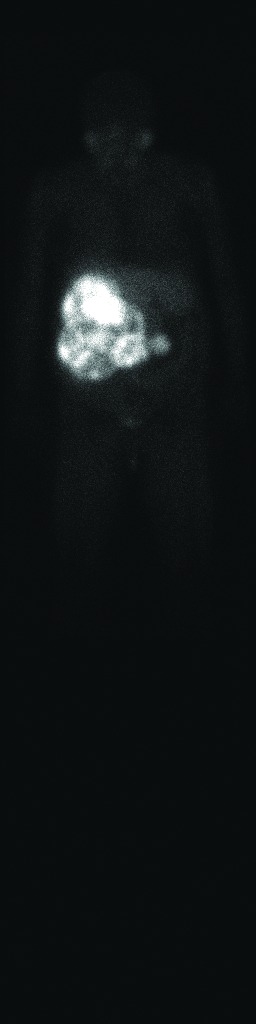
123I radiotracer distribution (anterior view).
Discussion
Although PCC usually presents with classic symptoms, there is no single clinical sign or symptom specific for pheochromocytoma.4,7,8 Seventy-five percent of affected patients suffer from sudden and unexpected weekly attacks, while others just once every few months.3 Hypertension is the most common sign, reported in 48% to 70% of cases, while dyspnea is only reported in 11% of cases.9
PCC is diagnosed by measurements of catecholamines and metanephrines in the serum and in a 24-hour urine collection, with a 98% sensitivity and specificity.1 A CT or magnetic resonance imaging of the abdomen are the imaging modalities of choice to localize a PCC, with a sensitivity of 90% to 100% and a specificity of 70% to 80%, respectively.6
En bloc surgical resection is the standard treatment of PCC; it has 5-year survival rates of 95% for benign and 50% for malignant PCC. Essential intra-operative surgical steps include early isolation of the tumour’s venous drainage with minimal manipulation of the mass followed by complete resection of the tumour.4 Preoperative management is essential to prevent hemodynamic instability and hypertensive crisis before or during surgery, which usually includes α-adrenergic blockade with phenoxybenzamine first and then β-blockade, with sufficient hydration with intravenous fluids the night before surgery.1,5,9 Postoperatively, patients typically experience BP fluctuations, heart rate fluctuations and hypoglycemia, warranting intensive care monitoring for at least 24 hours after the operation.6
This case is the fifth largest PCC reported in the English literature and the largest reported in Canada. Nineteen giant PCCs larger than 10 cm have been documented (Table 2).10–25 In this group of studies, the mean age was 48 years (range: 12–81), with 58% being male. Eight cases presented asymptomatically at the time of diagnosis, 4 had hypertension, and 1 other in addition to this case presented with dyspnea accompanied with chest pain, paraesthesia, and palpitations. Five of the 18 patients had metastases at the time of diagnosis. Metastases can appear up to 20 years after the initial presentation and can affect lymph nodes, bone, liver, and lungs.1 Benign and malignant tumours cannot be distinguished by histopathological methods, but only with the presence or development of distant metastases.2 Postoperatively, patients should be followed yearly for at least 10 years, as 16% of patients develop recurrence within 10 years.5,10
Table 2.
A summary of reported pheochromocytomas larger than 10 cm in the literature (descending order)
| Author/year | Sex/age | Country | Size/weight | Presentation |
|---|---|---|---|---|
| Grissom et al. 197911 | F/54 | USA | 45 × 25 cm/2100g | Asymptomatic |
| Costa et al. 200812 | M/46 | Brazil | 30 cm | Abdominal pain |
| Suga et al. 200013 | M/48 | Japan | 21 × 13 × 21 cm/3900 g | Asymptomatic |
| Melegh et al. 200214 | M/55 | Hungary | 20 cm | Asymptomatic |
| Current case | F/77 | Canada | 19 × 18 × 12 cm/2460 g | Dyspnea |
| Sharma et al. 20082 | M/46 | USA | 18 × 14 × 13 cm/1450 g | Episodic hypertension and headache |
| Sharma et al. 200615 | M/55 | India | 17 × 12 cm/850 g | Asymptomatic |
| Daughtry et al. 197716 | M/53 | USA | 17 cm/1150 g | Mild hypertension |
| Costa et al. 200812 | F/43 | Brazil | 16 cm | Abdominal pain¥ |
| Jain et al. 200217 | F/26 | India | 16 × 11 cm | Asymptomatic |
| Wu et al. 20007 | F/49 | USA | 15 × 12 × 12 cm | Asymptomatic |
| Santarone et al. 200818 | F/81 | Italy | 13 cm | Hypertension, palpitation, diaphoresis |
| Teng et al. 201219 | M/56 | China | 11.1 × 10.4 × 12.7 cm | Progressive weight loss & nausea |
| Dimitros et al. 200420 | M/70 | Greece | 12 × 8 × 10 cm | Asymptomatic |
| Schnakenburg et al. 197621 | M/12 | Former USSR/Ukraine | 12 × 10 × 9 cm/1100 g | Hemihypertrophy¥ |
| Chan et al. 200022 | M/63 | China | 11 × 6.6 × 11 cm | Asymptomatic |
| Awada et al. 200323 | F/26 | USA | 11 × 10 × 9 cm | Dyspnea, paresthesia, chest pain, palpitation |
| Uum et al. 201124 | F/27 | Canada | 10.5 × 10.6 cm | Headaches, episodic palpitations, pallor |
| Antedomenico et al. 20054 | F/39 | USA | 10.5 cm/782 g | Abdominal pain |
| Radfar et al. 201025 | M/53 | Iran | 3150 g | Abdominal pain |
These cases presented in metastasis at the time of diagnosis of giant pheochromocytoma.
Conclusion
We present a case of a 77-year-old female diagnosed with a giant PCC, the fifth largest in the literature and the largest reported in Canada. She presented with dyspnea and a palpable abdominal mass – both rare presentations for PCC. Giant PCCs typically lack the classic PCC symptoms, reiterating the need to have a high index of suspicion and a low threshold to order the appropriate serum and urine PCC screening tests.
Fig. 3.

Intraoperative open resection.
Footnotes
Competing interests: Dr. Ambati and Dr. Jana declare no competing financial or personal interests. Dr. Domes has received speaker fees from Lilly and Abbott.
This paper has been peer-reviewed.
References
- 1.Adler JT, Meyer-Rochow GY, Chen H, et al. Pheochromocytoma: Current approaches and future directions. Oncologist. 2008;13:779–93. doi: 10.1634/theoncologist.2008-0043. [DOI] [PubMed] [Google Scholar]
- 2.Pan Z, Repertinger S, Deng C, et al. A giant cystic pheochromocytoma of the adrenal gland. Endocr Pathol. 2008;19:133–8. doi: 10.1007/s12022-008-9016-4. [DOI] [PubMed] [Google Scholar]
- 3.Reisch N, Peczkowska M, Januszewicz A, et al. Pheochromocytoma: Presentation, diagnosis and treatment. J Hypertens. 2006;24:2331–9. doi: 10.1097/01.hjh.0000251887.01885.54. [DOI] [PubMed] [Google Scholar]
- 4.Antedomenico E, Wascher RA. A case of mistaken identity: Giant cystic pheochromocytoma. Curr Surg. 2005;62:193–8. doi: 10.1016/j.cursur.2004.08.015. [DOI] [PubMed] [Google Scholar]
- 5.Low G, Sahi K. Clinical and imaging overview of functional adrenal neoplasms. Int J Urol. 2012;19:697–708. doi: 10.1111/j.1442-2042.2012.03014.x. [DOI] [PubMed] [Google Scholar]
- 6.Därr R, Lenders JW, Hofbauer LC, et al. Pheochromocytoma: Update on disease management. Ther Adv Endocrinol Metab. 2012;3:11–26. doi: 10.1177/2042018812437356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wu JS, Ahya SN, Reploeg MD, et al. Pheochromocytoma presenting as a giant cystic tumor of the liver. Surgery. 2000;128:482–4. doi: 10.1067/msy.2000.104113. [DOI] [PubMed] [Google Scholar]
- 8.Bravo EL. Pheochromocytoma: Current perspectives in the pathogenesis, diagnosis, and management. Arq Bras Endocrinol Metabol. 2004;48:746–50. doi: 10.1590/S0004-27302004000500021. [DOI] [PubMed] [Google Scholar]
- 9.Kavoussi LR, Novick AC, Partin AW, et al. Campbell-Walsh Urology. 10th ed. Philadelphia: PA: Saunders; 2012. [Google Scholar]
- 10.Khorram-Manesh A, Ahlman H, Nilsson O, et al. Mortality associated with pheochromocytoma in a large Swedish cohort. Eur J Surg Oncol. 2004;30:556–9. doi: 10.1016/j.ejso.2004.03.006. [DOI] [PubMed] [Google Scholar]
- 11.Grissom JR, Yamase HT, Prosser PR. Giant pheochromocytoma with sarcoidosis. South Med J. 1979;72:1605–7. doi: 10.1097/00007611-197912000-00035. [DOI] [PubMed] [Google Scholar]
- 12.Costa SRP, Cabral NM, Abhrão AT, et al. Giant cystic malignant pheochromocytoma invading right hepatic lobe: Report on two cases. Sao Paulo Med J. 2008;126:229–31. doi: 10.1590/S1516-31802008000400008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Suga K, Motoyama K, Hara A, et al. Tc-99m MIBG imaging in a huge clinically silent pheochromocytoma with cystic degeneration and massive hemorrhage. Clin Nucl Med. 2000;25:796–800. doi: 10.1097/00003072-200010000-00009. [DOI] [PubMed] [Google Scholar]
- 14.Melegh Z, Rényi-Vámos F, Tanyay Z, et al. Giant cystic pheochromocytoma located in the renal hilus. Pathol Res Pract. 2002;198:103–6. doi: 10.1078/0344-0338-00194. discussion 107-8. [DOI] [PubMed] [Google Scholar]
- 15.Pradeep PS. Pheochromocytoma: A composite resection. Ind J Surg. 2006;68:163–4. [Google Scholar]
- 16.Daughtry JD, Susan LP, Straffon RA, et al. A case of a giant pheochromocytoma. J Urol. 1977;118:840. doi: 10.1016/s0022-5347(17)58215-4. [DOI] [PubMed] [Google Scholar]
- 17.Jain SK, Agarwal N. Asymptomatic giant pheochromocytoma. J Assoc Physicians India. 2002;50:842–4. [PubMed] [Google Scholar]
- 18.Santarone M, Borghi C, Miglierina E, et al. Giant cystic pheochromocytoma. J Cardiovasc Med (Hagerstown) 2008;9:971–2. doi: 10.2459/JCM.0b013e328303698b. [DOI] [PubMed] [Google Scholar]
- 19.Li C, Chen Y, Wang W, et al. A case of clinically silent giant right pheochromocytoma and review of literature. Can Urol Assoc J. 2012;6:E267–9. doi: 10.5489/cuaj.11195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Filippou DC, Rizos S, Nissiotis A, et al. A rare case of clinically silent giant pheochromocytoma. Internet J Oncol. 2004;2 [Google Scholar]
- 21.Schnakenburg KV, Müller M, Dörner K, et al. Congenital hemihypertrophy and malignant giant pheochromocytoma - a previously undescribed coincidence. Eur J Pediatr. 1976;122:263–73. doi: 10.1007/BF00481506. [DOI] [PubMed] [Google Scholar]
- 22.Chan FK, Choi KL, Tiu SC, et al. A case of giant malignant phaeochromocytoma. Hong Kong Med J. 2000;6:325–8. [PubMed] [Google Scholar]
- 23.Awada SH, Grisham A, Woods SE. Large dopamine-secreting pheochromocytoma: Case report. South Med J. 2003;96:914–7. doi: 10.1097/01.SMJ.0000077069.95831.62. [DOI] [PubMed] [Google Scholar]
- 24.Goldberg A, Pautler SE, Harle C, et al. Giant cystic pheochromocytoma containing high concentrations of catecholamines and metanephrines. J Clin Endocrinol Metab. 2011;96:2308–9. doi: 10.1210/jc.2011-0465. [DOI] [PubMed] [Google Scholar]
- 25.Basiri A, Radfar MH. Giant cystic pheochromocyt oma. Urol J. 2010;7:16. [PubMed] [Google Scholar]