

Abstract
Renal cell carcinoma is an aggressive urological malignancy. Metastases from the lesion are encountered late in the course of the disease and most often involve the lung and the liver. It is rare that metastatic lesions are the primary presentation of an otherwise clinically silent renal cell carcinoma. We report a case who presented with calvarial and cutaneous lesions which were later found to be metastases from an asymptomatic renal cell carcinoma.
Background
Metastases from renal cell carcinoma are common and occur in the late stages of the disease. The sites usually involved are the lung, liver, bone, etc.1 Cutaneous and skull metastases are rare and they present very late in the clinical course of the disease when the patient has already received treatment for the primary renal lesion. It is highly unusual for metastatic lesions to be the primary presentation in a clinically silent renal cell carcinoma.2 We report a case who presented with calvarial and skin nodules which proved to be metastatic lesions from a renal cell carcinoma.
Case presentation
A 35-year-old woman presented with lesions on her skull which she had first noticed 3 months ago. The lesions gradually increased in size (figure 1). She then noticed a small lesion below the umbilicus which was painless (figure 2). This lesion did not progress over time. There was a history of significant weight loss (5 kg over 3 months). There was no history of pain in the abdomen, cough, haematemesis, malena or haematuria. Her history and family history were unremarkable. She was a non-smoker. On examination, there were two discreet non-tender lesions, possibly osseous, involving the bilateral frontal area and another lesion in the left maxilla. The skin over the lesions was mobile. There was a cutaneous nodule of approximately 2 cm×2 cm in size in the infraumbilical area. It was non-tender and was not fixed to the underlying muscles. The systemic examination was normal.
Figure 1.

Clinical image of the patient showing the calvarial metastasis (arrows).
Figure 2.

Image showing the cutaneous lesion below the umbilicus (arrow).
Investigations
Her blood workup revealed low haemoglobin. An X-ray of the head revealed lytic lesions in the aforementioned areas. Fine-needle aspiration cytology from the skull, maxillary and cutaneous lesions was suggestive of metastatic adenocarcinoma. Chest X-ray was normal.
Differential diagnosis
Considering the histopathology, a primary internal organ malignancy was suspected. A contrast-enchanced CT of the abdomen was performed that revealed an enhancing lesion involving the left kidney suggestive of renal cell carcinoma (figure 3).
Figure 3.
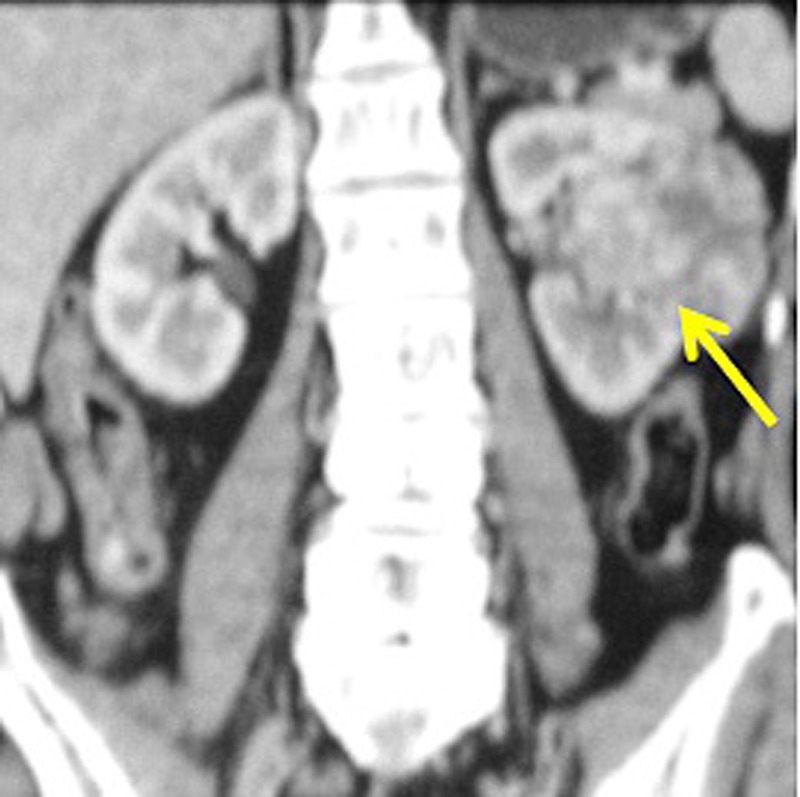
Contrast-enhanced CT scan image (coronal reformat) of the patient showing the heterogeneous, enhancing lesion in the left kidney suggestive of renal cell carcinoma (arrow).
Treatment
The patient was planned for targeted therapy for renal cell carcinoma and was offered a cytoreductive resection but she did not give her consent for it.
Outcome and follow-up
After 3 weeks, she had a sudden bout of massive haematuria at her house and could not be resuscitated.
Discussion
Renal cell carcinoma is an aggressive urological malignancy and has a propensity to develop metastasis. Skull and cutaneous metastases are rare and present in the advanced stages or after radical nephrectomy, when the patient is on follow-up. It is extremely unusual that these metastatic lesions are the primary presentation in an otherwise asymptomatic patient.3 4 In a recent review it was shown that isolated skull metastases, as the first presentation, were seen in only five cases.2 Isolated skin lesions, as the primary presentation of the underlying renal cell carcinoma, have been reported in less than 20 cases till date in the English literature.1 5 6 The presence of a combination of calvarial, maxillary and cutaneous metastases as the presenting lesions in an otherwise asymptomatic patient of renal cell carcinoma makes our report unique in the literature.
It has been proposed that once the tumour cells disseminate into the systemic circulation, the presence of systemic shunts and tumour-associated growth factors favours their deposition in the head and neck area. The normal pathway of dissemination to the head and neck area is through the lung which is the reason why patients with metastasis of the head and neck usually have associated pulmonary metastasis. The alternate pathway of dissemination of tumour cells via the vertebral venous plexus explains the absence of lung metastasis in patients who have isolated metastasis in the head and neck.2 7 The most often involved sites in the head and neck are paranasal sinuses, larynx, mandible and skull bones. The presentations can vary from slowly progressive asymptomatic swellings to painful, pulsatile masses. Patients may also present with nasal obstruction, nasal bleed, facial pain, diplopia, etc.2 8
Clinical appearance of the skin metastasis is variable ranging from plaques to nodules which can also be pulsatile at times. Skin lesions usually occur in the head and neck area and can be solitary or multiple. The cutaneous and head and neck metastases usually indicate a grave prognosis with a reported survival of less than 6 months.2 7 9
The treatment of such advanced tumours is debatable. Palliative nephrectomy can be offered in symptomatic patients. Nephrectomy along with aggressive surgical resection of the metastatic lesions also has a role in the management of such patients. Radiotherapy alone or along with surgery, cytoreductive surgery, systemic or intralesional interferon therapy, targeted therapy, stereotactic radiotherapy, etc have also been proposed.1 2 10 11
Patients with a solitary metastasis fare better than those with multiple metastases. The 5 year survival of patients with multiple metastases has been reported to range from 0 to 7%.1 2 3 10
Learning points.
Renal cell carcinoma can present with atypical metastasis.
Metastatic lesions can be the first presentation of a clinically silent renal cell carcinoma.
High index of clinical suspicion and prompt treatment is mandatory.
Footnotes
Contributors: RKS and TJ were involved in data collection, data interpretation, writing, editing and review of the manuscript. SM was involved in data collection and editing. DK was involved in editing and review of the manuscript.
Competing interests: None.
Patient consent: None.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Porter AN, Anderson LH, Al-Dujaily S. Renal cell carcinoma presenting as a solitary cutaneous facial metastasis: case report and review of the literature. Int Semin Surg Oncol 2006;3:27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sountoulides P, Metaxa L, Cindolo L. Atypical presentations and rare metastatic sites of renal cell carcinoma: a review of case reports. J Med Case Rep 2011;5:429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kouroupakis D, Patsea E, Sofras F, et al. Renal cell carcinoma metastases to the skin: a not so rare case? Br J Urol 1995;75:583–5 [DOI] [PubMed] [Google Scholar]
- 4.Rajasekharan P, Kavishwar VS, Butle P. Cutaneous metastasis from silent renal cell carcinoma. J Postgrad Med 2004;50:287–8 [PubMed] [Google Scholar]
- 5.de Paula TA, da Silva PS, Berriel LG. Renal cell carcinoma with cutaneous metastasis: case report. Bras Nefrol 2010;32:213–5 [PubMed] [Google Scholar]
- 6.Carlesimo M, Abruzzese C, Narcisi A, et al. Renal cell carcinoma diagnosed by cutaneous metastasis: a case report. Cutis 2012;90:196–9 [PubMed] [Google Scholar]
- 7.Mahmoudi HR, Kamyab K, Daneshpazhooh M. Cutaneous metastasis of renal cell carcinoma: a case report. Dermatol Online J 2012;18:12. [PubMed] [Google Scholar]
- 8.Sepúlveda I, Platin E, Klaassen R, et al. Skull base clear cell carcinoma, metastasis of renal primary tumor: a case report and literature review. Case Rep Oncol 2013;6:416–23 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chauhan A, Ganguly M, Nath P, et al. Cutaneous metastasis to face and neck as a sole manifestation of an unsuspected renal cell carcinoma. Int J Dermatol 2011;50:81–4 [DOI] [PubMed] [Google Scholar]
- 10.Powles T, Albers P. Management of favorable-risk patients with metastatic renal cell carcinoma: when to start and when to stop targeted therapy. Clin Genitourin Cancer 2012;10:213–18 [DOI] [PubMed] [Google Scholar]
- 11.Dutcher JP, Mourad WF, Ennis RD. Integrating innovative therapeutic strategies into the management of renal cell carcinoma. Oncology (Williston Park) 2012;26:526–30 [PubMed] [Google Scholar]