

Abstract
Spontaneous carotid artery dissection in pregnancy has not been reported before. We present a case of a 31-year-old Caucasian woman who was 11 weeks pregnant and presented with neck pain, headache, vomiting and left side Horner's syndrome. Subsequent investigations with MR angiography confirmed spontaneous left internal carotid artery dissection.
Background
Spontaneous dissections of the internal carotid artery have been known about for over 30 years and their incidence is now specified, with several hundred cases having been published.1
However, there are very few case reports of young patients. There are no case reports of young pregnant patients with spontaneous carotid artery dissection. Some case reports of pregnancy on background of systemic lupus erythematosis and postpartum cases of spontaneous carotid artery dissection have been described.2 3
Case presentation
Spontaneous cervical artery dissection is increasingly recognised as a common cause of ischaemic stroke in the young aged and middle aged. Non-invasive imaging techniques such as MRI and magnetic resonance angiography have widely replaced conventional angiography as the initial diagnostic study of extra cranial dissections, allowing greater numbers of patients to be screened and thus leading to increased frequency of the diagnosis.4
Marked gadolinium enhancement of the right extra cranial internal carotid artery on MRI can lead to an initial diagnosis of vasculitis as a cause of dissection.5 Also, carotid artery dissection can result from trauma; very simple trauma like hyperextension of the neck during athletic activities can also result in dissection of carotid arteries.6 Infection and minor trauma result in transient vasculopathy causing damage to endothelium and also intrinsic factors controlling vessel wall integrity can be affected by strenuous activity and major trauma thus explaining other possible mechanisms of dissection.2 3
Another important condition which can result in carotid artery dissection in female patients is fibromuscular dysplasia (FMD) as described in a recent study as follows.7 It is a nonatherosclerotic and noninflammatory type of vascular disease affecting mostly middle-aged women. HTN was found in 72% of the FMD registry of 447 patients. 19.7% of patients had dissection and 75% of total dissections were in carotid arteries. Most of the patients were middle-aged women as opposed to our case of a young woman.
In this FMD registry 56% of patients had carotid artery involvement and 65% of patients had renal artery involvement proving that FMD is an important predisposing factor also causing carotid artery dissection in young-aged to middle-aged women.7
A 31-year-old 11-week pregnant woman presented in the accident and emergency department with neck pain, headache, vomiting and left side Horner's syndrome comprising ptosis, miosis and anhydrosis on clinical and neurological examination. The only history was of hypothyroidism. There were no risk factors for vascular disease.
The most frequently encountered symptoms in carotid artery dissection are head or neck pain (80%), cerebral ischaemia (TIA or infarct) (56%) and Horner's syndrome (25%).8
The majority of cervical artery dissection patients in the community have excellent outcome, and contrary to many tertiary referral series, re-dissection is rare. Complete and excellent recovery can occur in 70–85% of patients, major disabling deficits in 10–25% of patients and death in 5–10% of cases.
Routine blood tests were normal and also special blood tests to exclude vasculitis (vasculitis screen including antinuclear antibody, ESR, antineutrophil cytoplasmic antibodies) were back to normal.
Resting ECG and echocardiogram were normal.
Emergency brain MRI scan and carotid MRI angiography were performed revealing left internal carotid dissection (figures 1 and 2).
Figure 1.
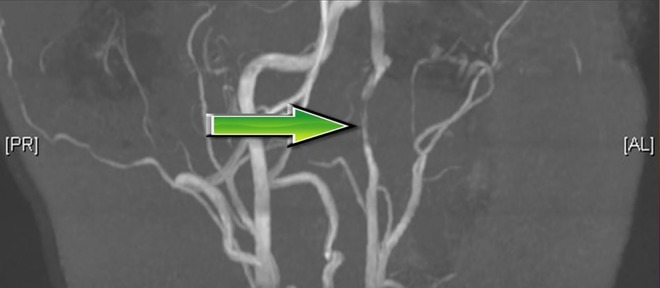
MR angiography (coronal image) showing left internal carotid artery dissection.
Figure 2.

MRI (axial image) showing left internal carotid artery dissection.
Angiographic features of the internal carotid arteries involved can show various features ranging from a smooth tapered luminal narrowing or occlusion in a few patients, irregular narrowing in some, a pearl and string sign, and sometimes retention of the contrast media mimicking a filling defect due to a thrombosed pseudo lumen.4
There are numerous case reports in the literature describing patients presenting with spontaneous carotid artery dissection4 6 but this case report is the first one of a pregnant woman.
Also, the patient had no major neurological deficit apart from left side Horner's syndrome and she is due to have repeat MRI angiography in a few months’ time. In some studies spontaneous carotid artery dissection is responsible for 0.6% of ischaemic strokes.4
Investigations
These days MRI angiography is gold standard investigation to diagnose carotid artery dissection. Other useful modalities are CT angiography (contraindicated in pregnancy), Doppler ultrasound and also conventional catheter-based angiography.
Differential diagnosis
Any space-occupying lesion compressing the carotids and sympathetic chain can present with Horner’s syndrome. Also vasculitis of carotid vessels is a good differential diagnosis. Infectious causes have to be ruled out especially in septic, unwell patients. Fibromuscular dysplasia in young-aged to middle-aged women has to be considered and ruled out as a cause of carotid dissection.
Treatment
Treatment can range from supportive measures, anticoagulation therapy for patients who merit, hyperbaric therapy and treating underlying causes. Our patient was treated with simple analgesics, antiemetics and detailed counselling.
Outcome and follow-up
Good outcome is normally seen in many patients with no recurrence of dissection observed during a long period of follow-up. Complete recanalisation of the artery can happen in 50% cases.
Follow-up can depend on the residual neurological and vascular state and can range from 3 months to 3 years or more. Our patient delivered a healthy baby and is due for further MRI angiography in 6 months’ time to study the extent of spontaneous repair.
Discussion
Many case reports and case series have been published studying spontaneous carotid artery dissection and also traumatic carotid artery dissection but there are no case reports describing spontaneous carotid artery dissection in pregnant patients.
Learning points.
Spontaneous carotid artery dissection can happen in pregnancy.
Every patient with Horner's syndrome has to be examined and investigated appropriately.
MRI angiography is gold standard investigation to diagnose carotid artery dissection in pregnant patients.
4.70–85% of patients have spontaneous resolution of symptoms and dissection.
Footnotes
Contributors: IM was involved in design and case write up; MA images collection; NK revision; ICM diagnosis, work up, supervision and support.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review : Not commissioned; externally peer reviewed.
References
- 1.Goulley Y, Bastide G. Spontaneous dissection of the internal carotid artery. J Mal Vasc 1991;16:378–80 [PubMed] [Google Scholar]
- 2.Morton A. Internal carotid artery dissection following chiropractic treatment in a pregnant woman with systemic lupus erythematosus. Chiropr Man Therap 2012;20:38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Baffour FI, Kirchoff-Torres KF, Einstein FH, et al. Bilateral internal carotid artery dissection in the postpartum period. Obstet Gynecol 2012;119(2 Pt 2):489–92 [DOI] [PubMed] [Google Scholar]
- 4.Nagumo K, Nakamori A, Kojima S. Spontaneous intracranial internal carotid artery dissection: 6 case reports and a review of 39 cases in the literature. Rinsho Shinkeigaku 2003;43:313–21 [PubMed] [Google Scholar]
- 5.Collamer AN, Battafarano D. A pain in the neck: carotid artery dissection presenting as vasculitis. Mil Med 2013;178:e851–4 [DOI] [PubMed] [Google Scholar]
- 6.Cusmano F, Piazza P, De Donatis M, et al. Dissection of the internal carotid artery. Personal case reports and a review of the literature . Radiol Med 1988;76:262–73 [PubMed] [Google Scholar]
- 7.Olin JW, Froehlich J, Gu X, et al. The United States Registry for fibromuscular dysplasia: results in the first 447 patients. Circulation 2012;125:3182–90 [DOI] [PubMed] [Google Scholar]
- 8.Lee VH, Brown RD, Jr, Mandrekar JN, et al. Incidence and outcome of cervical artery dissection: a population-based study. Neurology 2006;67:1809–12 [DOI] [PubMed] [Google Scholar]