

Description
Bony manifestations of hyperparathyroidism are characterised by diffuse osteopenia, brown tumours, subperisoteal bone resorption, pathological fractures, terminal acrosteolysis and salt-and-pepper appearance of the skull, and are secondary to increased resorption. Osteosclerotic changes have been described more often with secondary hyperparathyroidism, especially with renal osteodystrophy, however association with primary hyperparathyroidism (PHPT) has been rarely reported.1 We report one such case of focal osteosclerosis with PHPT.
A 23-year-old man presented with right lower limb swelling secondary to a pathological fracture of the distal end of the femur. On evaluation, he was found to have hypercalcaemia, hypophosphataemia, elevated alkaline phosphatase and hypovitaminosis D. Imaging showed nephrocalcinosis and ureteric calculi. Further evaluation revealed an elevated parathyroid hormone and a low bone mass on dual-energy X-ray absorptiometry (DXA) scan suggestive of PHPT. Localisation studies with an ultrasound of the neck showed lesion in the right superior parathyroid gland with a concordant sestamibi parathyroid scintigraphy (figure 1).
Figure 1.

Lateral view of the skull X-ray showing multiple round and oval-shaped osteosclerotic lesions.
His skeletal survey showed generalised osteopenia and pathological fracture of the right femur. His skull X-ray showed multiple round to oval focal sclerotic changes, which is an unusual radiological presentation in PHPT (figure 2).
Figure 2.
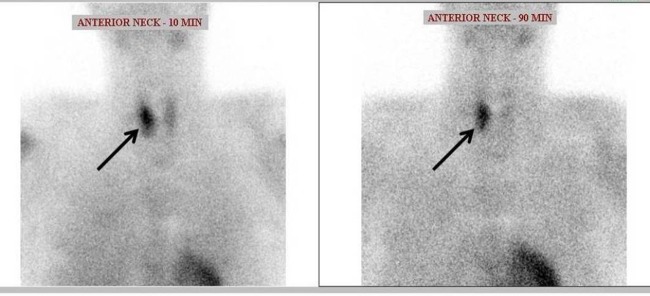
Parathyroid scintigraphy showing increased uptake in the right parathyroid gland.
The usual radiological features of the skull in PHPT are granular decalcification (salt-and-pepper appearance) and loss of lamina dura of the teeth. Osteosclerosis in hyperparathyroidism may be focal or diffuse. In PHPT, focal sclerotic lesions have been described at times to occur at sites such as the pelvis, spine, skull and the metaphyseal end of a bone with simultaneous lytic lesions. Disproportionate osteoblastic activity after prolonged osteoclastic activity, the anabolic effect of parathormone on bone metabolism and high bone turnover in young age could be the mechanisms responsible for osteosclerosis.2 3
Learning points.
Osteosclerosis, either focal or diffuse, is a rare radiological presentation in primary hyperparathyroidism.
The common sites of osteosclerotic involvement in hyperparathyroidism are pelvis, spine, skull and the metaphyseal end of long bones.
Footnotes
Contributors: SS and NK managed the patient. SS, NK and DN helped in the creation of the manuscript. TVP helped in supervising the management and proof reading the manuscript before submission.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Connor TB, Freijanes J, Stoner RE, et al. Generalized osteosclerosis in primary hyperparathyroidism. Trans Am Clin Climatol Assoc 1974;85:185–201 [PMC free article] [PubMed] [Google Scholar]
- 2.Fujino Y, Inaba M, Nakatsuka K, et al. Primary hyperparathyroidism with multiple osteosclerotic lesions of the calvarium. J Bone Miner Res 2003;18:410–12 [DOI] [PubMed] [Google Scholar]
- 3.Chopra S, Manchanda S, Kothari S, et al. Multiple osteosclerotic lesions of skull in two with co-existing hyperparathyroidism and vitamin D deficiency. JIACM 2012;13:349–51 [Google Scholar]