

Abstract
Background
Acute traumatic tendon injuries of the hand and wrist are commonly encountered in the emergency department. Despite the frequency, few studies have examined the true incidence of acute traumatic tendon injuries in the hand and wrist or compared the incidences of both extensor and flexor tendon injuries.
Methods
We performed a retrospective population-based cohort study of all acute traumatic tendon injuries of the hand and wrist in a mixed urban and rural Midwest county in the United States between 2001-2010. A regional epidemiologic database and medical codes were used to identify index cases. Epidemiologic information including occupation, year of injury, mechanism of injury and the injured tendon and zone were recorded.
Results
During the 10-year study period there was an incidence rate of 33.2 injuries per 100,000 person-years. There was a decreasing rate of injury during the study period. Highest incidence of injury occurred at 20-29 years of age. There was significant association between injury rate and age, and males had a higher incidence than females. The majority of cases involved a single tendon, with extensor tendon injuries occurring more frequently than flexor tendons. Typically, extensor tendon injuries involved zone three of the index finger, while flexor tendons involved zone two of the index finger. Work-related injuries accounted for 24.9% of acute traumatic tendon injuries. The occupations of work-related injuries were assigned to major groups defined by the 2010 Standard Occupational Classification structure. After assigning these patients' occupations to respective major groups, the most common groups work-related injuries occurred in construction and extraction occupations (44.2%), food preparation and serving related occupations (14.4%), and transportation and material moving occupations (12.5%).
Conclusions
Epidemiology data enhances our knowledge of injury patterns and may play a role in the prevention and treatment of future injuries, with an end result of reducing lost work time and economic burden.
Keywords: Injury, Incidence, Hand, Tendon, Trauma, Wrist
Penetrating hand trauma is common. Injuries of the hand comprise approximately 10% of all Emergency Department visits and up to 20% of all injuries treated.1) Soft tissue injuries of the hand predominate these statistics and are responsible for up to 82% of all hand injuries evaluated in the Emergency Department, as was noted by Clark et al.1) in a study of 1,074 hand injuries. With penetrating trauma the tendons of the hand or wrist are frequently injured. In an evaluation of laceration injuries to the hand, Tuncali et al.2) found that 54.8% of patients with a small laceration experienced concomitant tendon injury, and 92.5% of patients with a deep injury through a small laceration experienced concomitant tendon injury. These studies and others suggest that traumatic tendon injuries play a major role in hand trauma.3,4,5,6,7)
Despite its reported frequency, there are very few studies examining the true incidence of acute traumatic tendon injuries in the hand or wrist. Furthermore no study has examined and compared the incidences of both acute traumatic extensor and flexor tendon injuries. It is important for surgeons and health care providers to understand the epidemiology and incidence of acute tendon injuries in the hand and wrist as even a relatively small injury may result in a significant clinical, social and economical impact on the patient and society.
The purpose of this study was to determine the incidence and associated injury patterns of tendon injuries that may result from acute trauma to the hand and wrist. A retrospective analysis identifying both flexor and extensor tendon injuries occurring within a mixed urban and rural Midwest population in the United States during the years 2001 through 2010.
METHODS
Study Design
We performed a retrospective population-based cohort study to describe the epidemiology and incidence of traumatic tendon injuries occurring in the hand and wrist within Olmsted County, MN, United States (population range, 127,626 to 138,420 citizens during the years of the study period) during a 10-year period from January 1, 2001 through December 31, 2010. Minimal risk study (09-003826) approved on 6/26/2009.
Study Population
Approval from our hospital and county Institutional Review Board was obtained prior to initiating the study and all patients gave consent for research. The study was performed using the Rochester Epidemiology Project (REP), a comprehensive database of all medical records of virtually all medical care providers to Olmsted County, Rochester, MN. The database has tracked residents since the early 1960's.8) Olmsted County contains one large urban community (Rochester, MN) which represents roughly 75% of the overall population, with a surrounding rural and mostly agricultural region. Roughly 85% of the county's population is Caucasian. The majority of workers in Olmsted County are in service industries, primarily healthcare and hospitality.
Incident cases were defined as patients with an open wound of the hand or wrist with tendon involvement, secondary to acute trauma. Only patients who gave authorization to be included for research and lived in Olmsted County at the time of the trauma were included. Exclusion criteria involved all chronic or non-traumatic injuries (e.g., secondary to inflammation, congenital malformations or flexion deformities). Also excluded were avulsion fractures, complete amputations and closed tendon injuries including spontaneous ruptures and closed mallet fingers. Hand and wrist injuries were examined, and forearm injuries proximal to extensor zone 8 and flexor zone 5 were excluded.
Data Collection
Patients in the REP database were identified using International Classification of Diseases (ICD)-9 codes describing open wounds with tendon involvement of wrist, hand, finger or unspecified upper limb. The ICD-9 codes are very reliable as a result of the professional coders of the health care institutions in Olmsted County. The patients' age, gender, ethnicity, dominant hand, occupation, year of injury, mechanism of injury and the injured tendon and zone were identified and recorded from the patients' medical records. For analysis of incidence rates, age at diagnosis was categorized into eight groups: 0-9 years, 10-19 years, 20-29 years, 30-39 years, 40-49 years, 50-59 years, 60-69 years, and > 70 years. Additionally, the occupation of any patient who experienced a work-related injury was reviewed and assigned to one of 23 "Major Groups" as defined by the 2010 Standard Occupational Classification structure (SOC2010), which is used by Federal statistical agencies to classify workers into categories for statistical analysis.9)
Statistical Analysis
Incidence rates of tendon injuries were calculated for the years 2001 through 2010 assuming all Olmsted County residents were at risk. Rates were calculated as the number of tendon injuries divided by the number of population person-years and reported as per 1,000 person-years, with 95% confidence intervals assuming a Poisson distribution. The denominator age- and sex-specific population person-years were estimated from decennial census figures, with linear interpolation between census years. Age- and sex-adjusted estimates were calculated by direct adjustment to the 2000 US census population.10) Potential trends in the incidence of tendon injuries in the hand were examined by calculating age-, sex- and calendar-year-specific incidence rates, and evaluating these rates using Poisson regression. Descriptive statistics were used to describe patient characteristics. Statistical analyses were performed by the Division of Biostatistics using SAS ver. 9.2 (SAS Institute, Cary, NC, USA). All tests were two-sided and p < 0.05 was considered statistically significant.
RESULTS
Incidence of Acute Traumatic Tendon Injury
During the 10-year study period, 458 cases of acute traumatic tendon injuries of the hand and wrist were identified. This involved 692 tendons, of which 184 (26.6%) were reported to be only partially lacerated. None of the patients had more than one incident of acute traumatic tendon injury during the defined 10-year period. Three of the 458 patients suffered bilateral injuries.
The overall age- and sex-adjusted incidence rate was 33.2 per 100,000 person-years (95% confidence interval [CI], 30.1 to 36.2). Fig. 1 shows the incidence rates for males and females from 2001 to 2010. The rate of injuries was significantly associated with gender (p < 0.001), with an age-adjusted incidence rate of 56.3 per 100,000 person-years for males (95% CI, 50.6 to 62.0) and 10.7 per 100,000 person-years for females (95% CI, 8.3 to 13.2). Most tendon injuries occurred in 2002, with an incidence rate of 42.9 per 100,000 persons. The year 2010 had the lowest incidence rate with 24.1 per 100,000 persons. Overall, the rate of injuries was significantly associated with year (p = 0.040), with a decreasing trend over the 10-year period.
Fig. 1.
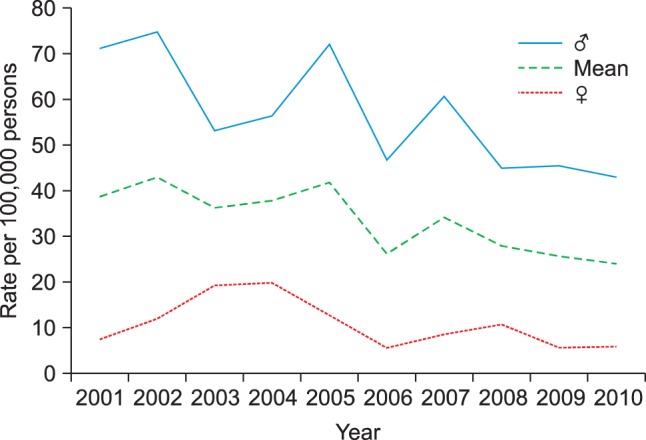
Overall incidence of acute traumatic tendon injury in the hand or wrist for males and females from 2001 to 2010.
The mean age at time of injury was 35.9 years (range, 1 to 91 years). Age was significantly associated with the rate of injuries (p < 0.001), with the highest crude incidence in patients aged 20-29 years. Additional patient population characteristics are presented in Table 1.
Table 1.
Patient Population Characteristics
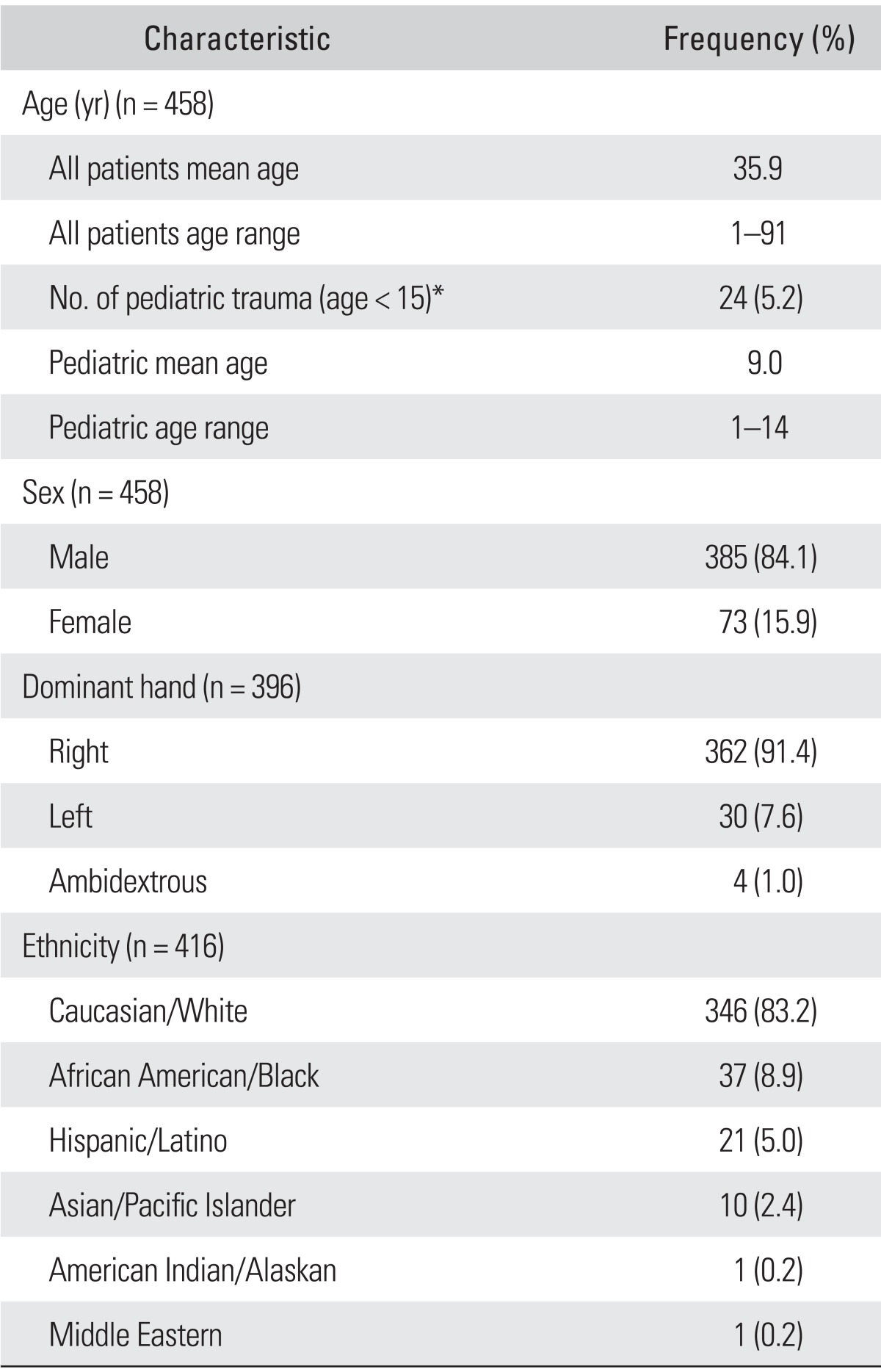
*Pediatric trauma defined as < 15 years of age per institutional-specific guidelines.
Injury Characteristics and Patterns
Of all patients, 377 patients (82%) had at least one laceration directly located on a digit (finger and/or thumb). The remaining patients suffered injuries to the palmar or dorsal hand or wrist. Patients with direct digit involvement injured between one to four digits, with the majority of injuries occurring on a single digit (75%). When the total number of tendon injuries in each digit was compared, injury to the index finger was the most common (Table 2).
Table 2.
Tendon Injury by Digit
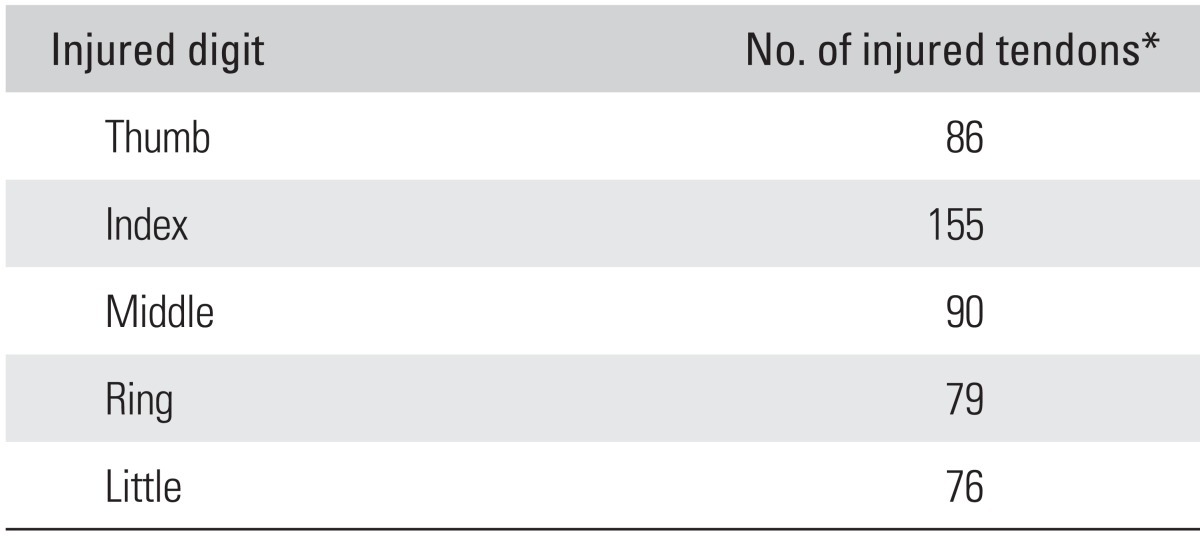
*Some patients injured more than one tendon on more than one digit.
Extensor tendon injuries accounted for more injuries than flexor tendon injuries (p < 0.001). In total, 395 extensor tendons and 297 flexor tendons were injured. Patients injured between one to nine tendons in the hand or wrist, the majority having injured one tendon (72%). Of all extensor tendon injuries, the extensor mechanism in the index finger was injured significantly more often than any other tendon (15.6%), which remained significant after a Bonferroni correction (Bonferroni p < 0.003). The most commonly injured zone of all extensor tendons was zone three (12.6%). Extensor tendon zone three was injured more often than zones two and five, although this was not significant (Bonferroni p < 0.004).
The flexor digitorum profundus to the index finger was the most injured flexor tendon (9.1%). However, after Bonferroni adjustment, it was not injured significantly more often than the flexor digitorum profundus tendons to the long, ring and little finger, the flexor digitorum superficialis to the little finger or the flexor pollicis longus (Bonferroni p < 0.004). Of all flexor tendon zones, zone two was injured in 19.1%, which was significantly more often than every other flexor zone (Bonferroni p < 0.006). Tables 3 and 4 summarize the frequency and percentages of individual tendons injured and the percentage of tendon injuries by zone, respectively.
Table 3.
Frequency of Specific Extensor and Flexor Tendon Injury
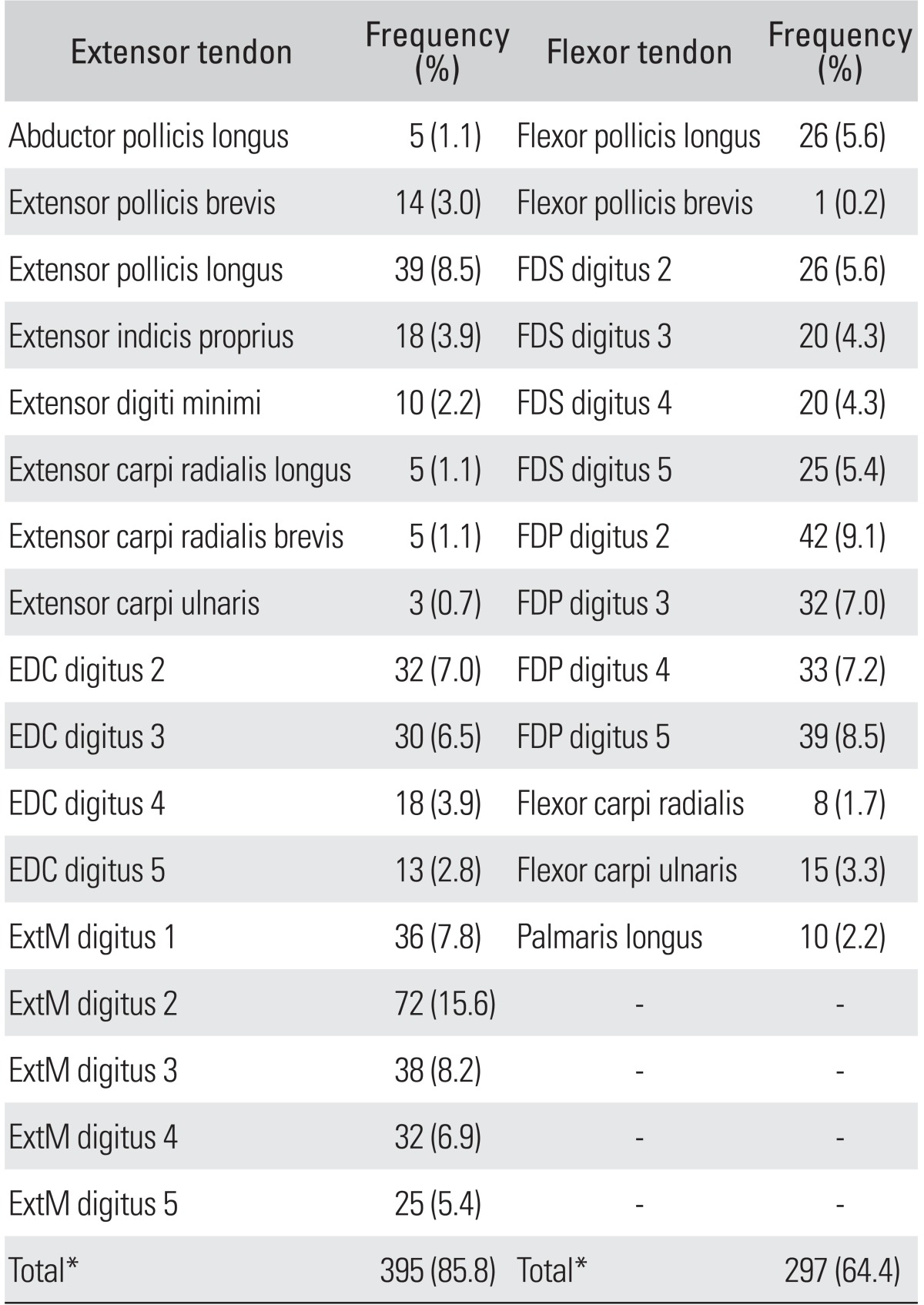
EDC: extensor digiti communis, ExtM: extensor mechanism of the finger within extensor zone 1-4 and T1-T2, FDS: flexor digitorum superficialis, FDP: flexor digitorum profundus.
*Sum of total percentages is > 100% because some patients injured more than one tendon on more than one digit.
Table 4.
Percentage of Specific Extensor and Flexor Tendon Zone Injury
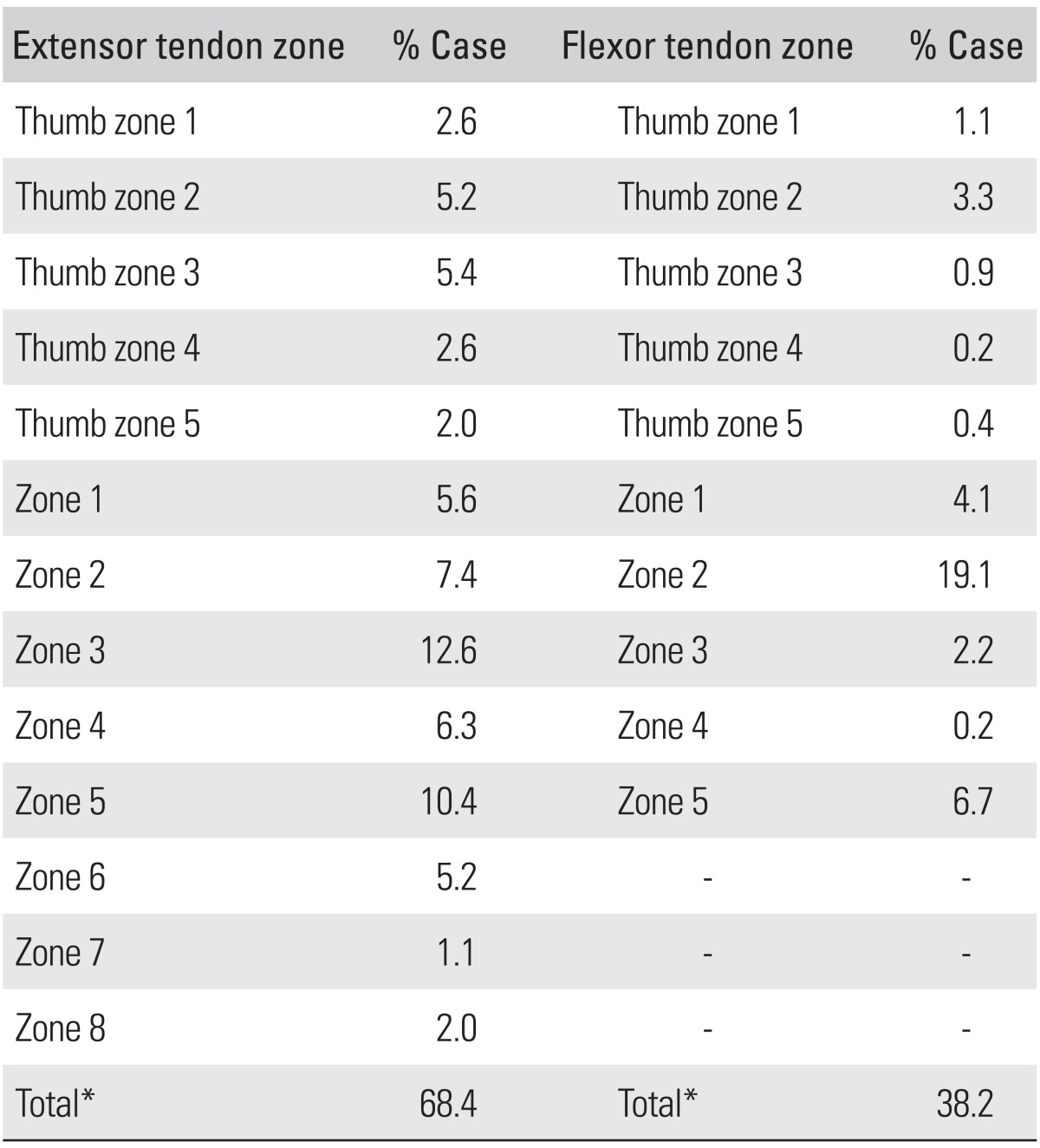
*Sum of total percentages is > 100% because some patients had injury in more than one zone.
A variety of mechanisms accounted for acute traumatic tendon injuries and included: knife (n = 129), glass or mirror (n = 71), any kind of saw (n = 68), crush injury (n = 27), degloving injury (n = 5), and bite injury (n = 3). Mechanism was not recorded in 40 cases, tendon injury was caused by sharp objects too diverse to specify in 105 cases. These cases were mainly due to sharp metal (e.g., sheet metal, blades of lawn mower, snow blower), work instruments (e.g., scissor, chisel) or ceramic splinters. Thirty-four patients (7.4%) were reported to be moderately to severely intoxicated with alcohol, of which one case involved bilateral injury. Tendon injuries related to violence or physical altercations were seen in 27 cases (6.4%). Of these 27, alcohol was involved in 16 cases (59.3%), and the most common mechanism involved a knife (n = 10, 37.0%). Nineteen patients (4.5%) had self-inflicted or purposely imposed wounds that were obtained in a variety of circumstances. Six patients (1.4%) had self-inflicted wounds secondary to attempted suicide, of which one case involved bilateral injury. Ten cases which were self-inflicted were the result of punching/hitting something (most commonly glass), all while intoxicated with alcohol, and not related to violence or physical altercation.
Pediatric cases (defined at our institution as < 15 years of age) of acute traumatic tendon injury occurred in 24 patients (5.2%) with a mean age of 9.0 years of age (range, 1 to 14 years) (Table 1). Of these patients, 6 patients specifically suffered acute tendon injury at school during a workshop class.
Work-related injuries accounted for 24.9% (n = 104) of acute traumatic tendon injuries. After assigning these patients' occupations to respective SOC2010 major groupings, the groups with the highest work-related injuries occurred in construction and extraction occupations (n = 46, 44.2%), food preparation and serving related occupations (n = 15, 14.4%), and transportation and material moving occupations (n = 13, 12.5%) (Table 5).
Table 5.
Standard Occupational Classification of Work-related Injuries*
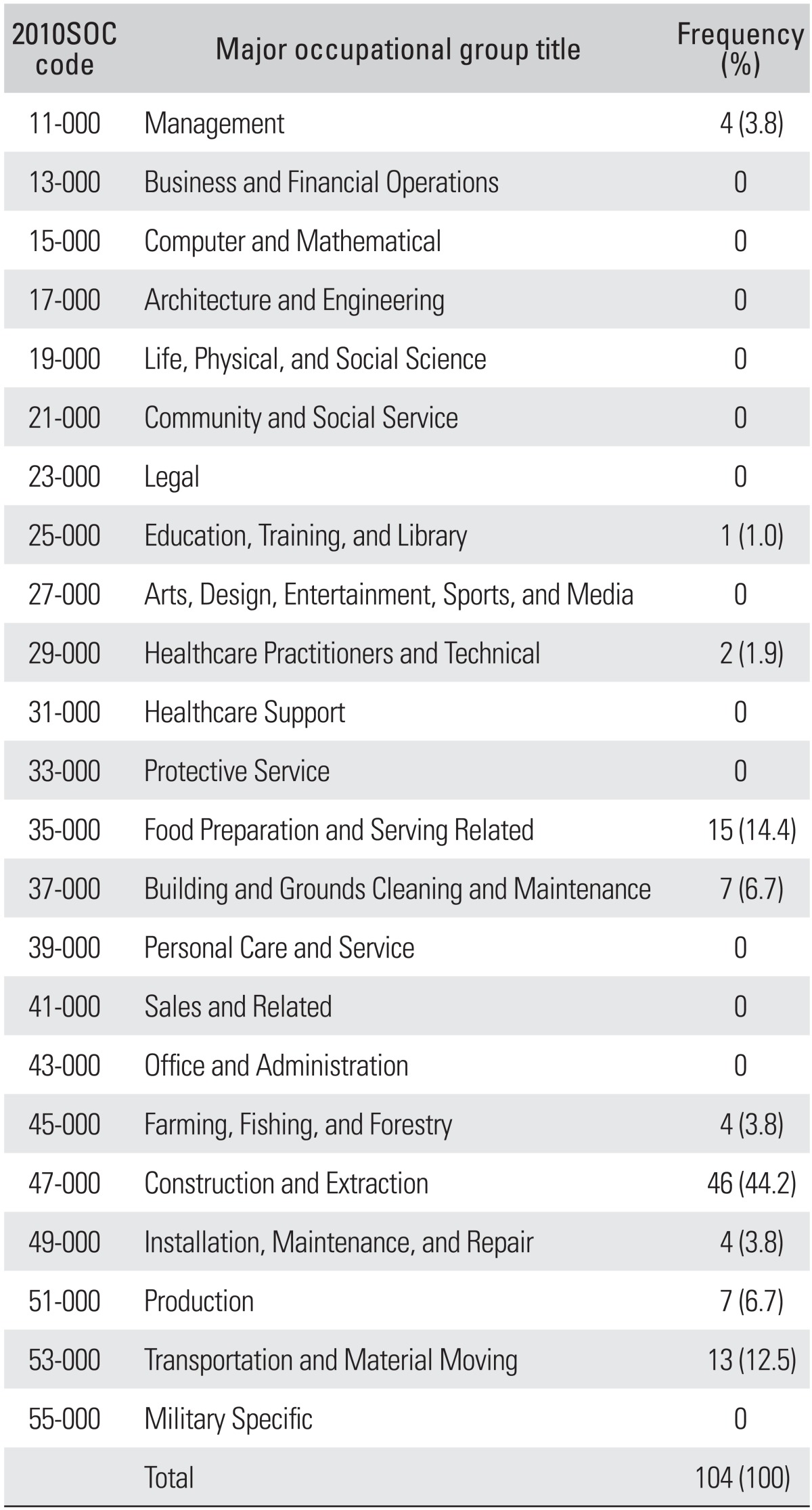
*Based on US Department of Labor 2010 Standard Occupational Classification (2010SOC) major grouping.
DISCUSSION
Hand injuries account for up to 20% of all treated injuries in an Emergency Department.1) Furthermore, acute hand injuries are the most common occupational injury evaluated in emergency departments within the United State.11) The spectrum of traumatic hand injuries includes minor soft tissue injuries and fractures to complex injuries requiring nerve, tendon, or artery repair. Within this spectrum, tendon injuries are quite common and were reported in 54.8% of patients with a small laceration and 92.5% of patients with a deep injury through a small laceration.2) Thus, it is important for the treating physician to recognize that even a small laceration to the hand may involve the flexor or extensor mechanism; however, the incidence of such injuries has not been extensively studied in the literature. Without adequate epidemiologic data, it is difficult for one to predict the economic burden of these injuries on society, which is of particular relevance in the current setting of growing healthcare costs and limited available economic resources.3,4,5,6,7)
Our data from a mixed urban and rural population show tendon injury in the hand or wrist to occur at a rate of 33.2 injuries per 100,000 person-years. Males have a significantly higher incidence of traumatic tendon injuries to the hand or wrist compared to females; a finding in accordance with previous studies.12) This may be partly due to the nature of gender-related professional work and recreational activities. Previous reports have suggested that most hand injuries appear to occur while performing manual labor either on-the-job or at home.13) It was also noted that traumatic tendon injuries in the hand occur most frequently in the 20-29 year old age group. This corresponds with the age of the workforce most likely to have more physical labor intensive occupations which may place them at increased risk for injury. In our study, the most common occupations experiencing work-related injury occurred in construction and extraction occupations (e.g., carpentry, construction, electrical, textile), food preparation and serving related occupations (e.g., cooking/chefs, restaurant personnel), and transportation and material moving occupations (e.g., machinist, manufacturing-related jobs, equipment operators). While unable to be calculated in our study, the combination of these work-related injuries surely accounts for an incredible amount of lost work time and overall economic burden to our population.
This study shows that extensor tendon injuries occurred more frequently than flexor tendon injuries, with the index finger representing the most commonly injured finger. Previous reports have noted the predominance of flexor tendon research, but a paucity of outcome studies exists examining the outcomes following extensor tendon repair and its long-term morbidity on young laborers.14,15,16,17,18) As such, future research may wish to focus on the treatment and rehabilitation of extensor tendon injuries.
With regard to flexor tendon injuries, injury was most commonly located in zone two, suggesting that most flexor tendon injuries occur distal to Camper's chiasm. Rosberg et al.7) previously reported that isolated injury of the profundus tendon to the small finger was the most common flexor tendon injury during their examination of 135 flexor tendon injuries in a Swedish population.
Weaknesses of the present study include the retrospective nature of the study and the specific geography of our cohort population. The incidence of traumatic tendon injuries reported here may not be applicable to large metropolitan areas, but rather be of relevance to smaller urban and mixed communities with agricultural areas within the Midwest United States. We did not examine the socioeconomic factors or the working environment of injured patients, which may have influenced injury patterns. In addition, no effort was made to examine treatment modalities, outcomes, or health care cost related to the management of these injuries which will be the subject of future analysis. Missed cases in the present database include all neglected injuries and cases of tendon injury not seen within our health care centers. The chance of missed cases, however, is most likely low, as it is unlikely for patients with an injury in the county studied to seek care outside the large region that this hospital provides.
To put the frequency of tendon injuries into perspective, it is interesting to note that the incidence of scaphoid fractures is 1.47 fractures per 100,000 person-years.19) This rate is 23 times smaller than the incidence rate of tendon injuries showed by our study. Although our data demonstrates a significant decrease in incidence over the 10-year period, we believe the present incidence is still of such importance that it should encourage the ongoing study of tendon healing and rehabilitation as a means of decreasing morbidity following these injuries. The reason for this decrease is a question for further investigation, but could be related to changing occupations and increasing awareness of possible risks.11,13)
In conclusion, an improved and updated understanding of the epidemiology of acute tendon injuries will hopefully stimulate additional investigation into the prevention and treatment of these injuries.
ACKNOWLEDGEMENTS
This study was made possible through use of the Rochester Epidemiology Project (R01 AG034676-45). We would like to thank Dr. Marianne Huebner and William Harmsen in the Department of Health Sciences Research for their help with statistical analysis.
Footnotes
Presented at Federation of European Societies for Surgery of the Hand (FESSH), Antwerp, Belgium, June 20-23, 2012.
Mayo Clinic receives Consultancy and Royalties from Integra for Dr. Steven Moran. All remaining authors have declared no conflicts of interest.
References
- 1.Clark DP, Scott RN, Anderson IW. Hand problems in an accident and emergency department. J Hand Surg Br. 1985;10(3):297–299. doi: 10.1016/s0266-7681(85)80047-4. [DOI] [PubMed] [Google Scholar]
- 2.Tuncali D, Yavuz N, Terzioglu A, Aslan G. The rate of upper-extremity deep-structure injuries through small penetrating lacerations. Ann Plast Surg. 2005;55(2):146–148. doi: 10.1097/01.sap.0000168884.88016.e1. [DOI] [PubMed] [Google Scholar]
- 3.Broback LG, Ekdahl PH, Aschan GW, Grenabo JK. Clinical and socio-economical aspects of hand injuries. Acta Chir Scand. 1978;144(7-8):455–461. [PubMed] [Google Scholar]
- 4.Hoxie SC, Capo JA, Dennison DG, Shin AY. The economic impact of electric saw injuries to the hand. J Hand Surg Am. 2009;34(5):886–889. doi: 10.1016/j.jhsa.2009.02.002. [DOI] [PubMed] [Google Scholar]
- 5.Mathur N, Sharma KK. Medico-economic implications of industrial hand injuries in India. J Hand Surg Br. 1988;13(3):325–327. doi: 10.1016/0266-7681_88_90101-5. [DOI] [PubMed] [Google Scholar]
- 6.O'Sullivan ME, Colville J. The economic impact of hand injuries. J Hand Surg Br. 1993;18(3):395–398. doi: 10.1016/0266-7681(93)90072-n. [DOI] [PubMed] [Google Scholar]
- 7.Rosberg HE, Carlsson KS, Hojgard S, Lindgren B, Lundborg G, Dahlin LB. What determines the costs of repair and rehabilitation of flexor tendon injuries in zone II? A multiple regression analysis of data from southern Sweden. J Hand Surg Br. 2003;28(2):106–112. doi: 10.1016/s0266-7681(02)00352-2. [DOI] [PubMed] [Google Scholar]
- 8.Melton LJ., 3rd History of the Rochester Epidemiology Project. Mayo Clin Proc. 1996;71(3):266–274. doi: 10.4065/71.3.266. [DOI] [PubMed] [Google Scholar]
- 9.US Department of Labor. Standard occupational classification [Internet] Washington, DC: US Department of Labor; [cited 2013 Mar 30]. Available from: http://www.bls.gov/soc/ [Google Scholar]
- 10.Bergstralh EJ, Offord KP, Chu CP, Beard CM, O'Fallon WM, Melton LJ. Calculating incidence, prevalence and mortality rates for Olmsted County, Minnesota: an update. Rochester: Mayo Clinic; 1992. Report No.: Technical Report No 49. [Google Scholar]
- 11.Sorock GS, Lombardi DA, Courtney TK, Cotnam JP, Mittleman MA. Epidemiology of occupational acute traumatic hand injuries: a literature review. Saf Sci. 2001;38(3):241–256. [Google Scholar]
- 12.Hill C, Riaz M, Mozzam A, Brennen MD. A regional audit of hand and wrist injuries: a study of 4873 injuries. J Hand Surg Br. 1998;23(2):196–200. doi: 10.1016/s0266-7681(98)80174-5. [DOI] [PubMed] [Google Scholar]
- 13.Campbell AS. Hand injuries at leisure. J Hand Surg Br. 1985;10(3):300–302. doi: 10.1016/s0266-7681(85)80048-6. [DOI] [PubMed] [Google Scholar]
- 14.Koul AR, Patil RK, Philip V. Complex extensor tendon injuries: early active motion following single-stage reconstruction. J Hand Surg Eur Vol. 2008;33(6):753–759. doi: 10.1177/1753193408092786. [DOI] [PubMed] [Google Scholar]
- 15.Lee SK, Dubey A, Kim BH, Zingman A, Landa J, Paksima N. A biomechanical study of extensor tendon repair methods: introduction to the running-interlocking horizontal mattress extensor tendon repair technique. J Hand Surg Am. 2010;35(1):19–23. doi: 10.1016/j.jhsa.2009.09.011. [DOI] [PubMed] [Google Scholar]
- 16.Manske PR. History of flexor tendon repair. Hand Clin. 2005;21(2):123–127. doi: 10.1016/j.hcl.2004.03.004. [DOI] [PubMed] [Google Scholar]
- 17.Newmeyer WL., 3rd History of the journal of hand surgery: 1976-1999. J Hand Surg Am. 2000;25(1):5–13. doi: 10.1053/jhsu.2000.0005. [DOI] [PubMed] [Google Scholar]
- 18.Soni P, Stern CA, Foreman KB, Rockwell WB. Advances in extensor tendon diagnosis and therapy. Plast Reconstr Surg. 2009;123(2):727–728. doi: 10.1097/PRS.0b013e318197b692. [DOI] [PubMed] [Google Scholar]
- 19.Van Tassel DC, Owens BD, Wolf JM. Incidence estimates and demographics of scaphoid fracture in the U.S. population. J Hand Surg Am. 2010;35(8):1242–1245. doi: 10.1016/j.jhsa.2010.05.017. [DOI] [PubMed] [Google Scholar]