

Abstract
Goal: We want to remove differences in frequency response between different commercial hearing aids so that we can compare the sound quality of signal processing features from different hearing-aid in a future paired-comparison set-up. More specifically, we want to control for the confounding effects of the linear hearing aid response when evaluating nonlinear processing. This article presents a control procedure and evaluates its effectiveness. Method: We increased the similarity of hearing-aid recordings in three steps and used both an objective quality metric and listening tests to investigate if the recordings from different hearing aids were perceptually similar. Results: Neither was it sufficient to manually adjust the hearing-aid insertion gain, nor was it sufficient to add an additional bandwidth limitation to the recordings. Only after the application of an inverse filter the perceptual differences between recordings were removed adequately. Conclusion: It was possible to level the ground between different hearing devices, so to speak. This will allow future research to evaluate the sound quality of nonlinear signal processing features.
Keywords: hearing aids, perceptual evaluation, sound quality, noise reduction
Introduction
Most hearing aids currently marketed have advanced signal processing schemes implemented, such as noise reduction. In our experience, many clinicians do not actively select such techniques or their fitting options to meet the requirements of an individual hearing-impaired listener. One reason for this is a lack of knowledge about the processing details and their perceptual effects for the user. For instance, most research into noise reduction in (commercial) hearing aids was done by comparing different settings within the same hearing aid (e.g., Bentler, 2005; Boymans & Dreschler, 2000; Mueller, Weber, & Hornsby, 2006). However, a clinician needs to be able to choose also between devices. Unfortunately, direct perceptual comparisons of the sound quality between different devices are uninformative because the perceptual effects are largely determined by other parameters not related to the signal processing under investigation. For instance, the frequency dependent hearing-aid gain can differ substantially across hearing aids, even for hearing aids fitted to the same hearing loss (e.g., Mueller, Bentler, & Wu, 2008, showed differences up to 15 dB). There can also be large differences in sound quality. Legarth, Simonsen, Bramsløw, Le Ray, and Zacharov (2010) fitted four hearing aids according to the same fitting rule and found that for normal hearing listeners these four aids differed markedly in subjective sound quality (ranging from between “poor” and “fair” to “good” on a mean opinion scale). These examples illustrate clearly that audible differences between hearing aids cannot be removed just by fitting them to the same hearing loss. Spectral characteristics can strongly influence a sound-quality percept (Davis & Davidson, 1996; Gabrielsson, Schenkman, & Hagerman, 1988). For instance, Gabrielsson and Sjögren (1979) did an experiment in which participants had to describe the sound of eight different headphones. They found that the headphone with a 10-dB peak in the frequency response at 3 kHz scored strongly on adjectives related to “sharp/hard/loud” and on adjectives related to “disturbance.” In general, smoother frequency responses lead to better sound-quality judgments (Arehart, Kates, & Anderson, 2010) and can improve the threshold of discomfort (Warner & Bentler, 2002).
In conclusion, there is need for a method that allows for perceptual comparison between features of hearing aids by removing the (usually large) differences in frequency response between devices. In this article, we will therefore answer the following research question:
-
Research Question: Is it possible to reduce the perceptual differences (without reducing sound quality) between a set of hearing-aid recordings so that the recordings are indistinguishable from each other, with the following three successive steps:
Careful manual adjustment of the insertion gain of the hearing aids;
Limitation of bandwidth of hearing aid recordings;
Application of an inverse filter on the bandwidth limited hearing-aid recordings?
To answer this, we recorded the output of a selection of hearing aids and these recordings were processed in three varying degrees (careful adjustment of the insertion gain, adjustment with bandwidth limitation, and inverse filtering with bandwidth limitation) to minimize differences between them. A sound-quality model was used to determine objective differences in quality between the hearing aids in each set. Additionally, we did two listening experiments with six normal-hearing participants. In the first experiment, the participants had to detect which sound sample differed from two other identical samples. The outcome was the percentage of times the participants could detect differences between the hearing aids, within each set of stimuli. Finally, we did a paired comparison test in which the participants had to indicate which sample they would prefer for long-time listening. This test was meant to measure the effect of our processing on the sound quality of the recordings.
Method
Experimental Setup
All recordings and experimental validations were done in a sound-treated double-walled booth (2.20 × 2.53 × 2.0 m). The recording system consisted of a B&K Head and Torso Simulator (HATS Type 4128C) fitted with a custom made tight-fitting ear mould without venting. Sound signals were generated and recorded monaurally at a 44100-Hz sample rate with a resolution of 24 bits. The digital signals were converted to the analogue domain with a RME Fireface 800 sound card, and were presented to the hearing aid via a Samsung Servo 120 amplifier connected to a Tannoy Reveal 6 near-field monitoring speaker that was placed at 62 cm in front of the recording microphone (on axis). All free-field hearing-aid input signals were corrected for the speaker response and all signals were presented within the direct sound field to minimize the influence of room reflections.
The hearing aids used in this study were five frequently used BTE hearing aids from different brands (Oticon Vigo Pro, Phonak Exélia M, ReSound Azure AZ80-DVI, Starkey Destiny 1200,Widex Mind 440), randomly coded as HA1 through HA5. All signal-processing features (directionality, feedback control, noise reduction, compression, frequency transposition, and so on) were turned off.
Stimuli
We recorded the hearing-aid output for speech (Versfeld, Daalder, Festen, & Houtgast, 2000) in speech babble (Luts et al., 2010). We used speech in noise because (a) this is the target signal for most signal-processing features in hearing aids, and (b) the evaluation has to take into account possible remaining differences in both the target speech and the background noise. The signal to noise ratio was chosen to be +10 dB because this is a relevant ratio for speech in noise experiments and it is high enough to allow perception of possible distortions and coloring to both speech and noise. Note that all hearing aids add noise to the signal. In our selection of hearing aids, the specified equivalent noise input level was between 20 to 30 dB SPL, and this resulted in a noise level about 45 dB lower than our average speech level. This was assumed not to influence the quality of the recordings of our speech in speech-shaped babble noise (at + 10 dB), as the low-level noises will be masked by the background noise.
Three sets of stimuli were made to answer the three parts of the research question. Set 1 consisted of the unprocessed hearing-aid recordings that were made after manual adjustment of the insertion gain (i.e., the difference between aided and unaided response). Set 2 was based on the same recordings, but the signals were limited in bandwidth, and in Set 3 these bandwidth limited recordings were also filtered with an inverse filter to remove differences in frequency response.
Stimulus Set 1: Adjustment of the insertion gain
During the hearing-aid fitting, the insertion gain was measured in-situ with pink noise. To simulate a realistic condition, we selected a conductive hearing loss of 30 dB at 500 Hz and 15 dB at 2 kHz, that resulted in a NAL-RP prescription (Dillon, 2001) of about 10 dB insertion gain in the low and mid frequencies. More precisely, the target insertion gain was 4 dB between 100 Hz and 125 Hz; 10 dB between 125 Hz and 2 kHz; decreasing to 0 dB at 2 kHz, and it was 0 dB from 4 to 6 kHz. This frequency range (100 Hz to 6 kHz) was within the specified operational frequency range for all hearing aids except for HA5 (its specified operational low-end frequency is 200 Hz, but the aid was verified to give reliable output to at least as low as 100 Hz). Although the fittings were carefully adjusted to obtain the same insertion gain for all hearing aids, several peaks and valleys remained in the responses, making them different from each other and from a flat frequency response. These remaining differences in gain between the devices can be seen from the top panel in Figure 1 and were smaller than 4.5 dB up to 2 kHz and smaller than 12 dB between 2 and 6 kHz.
Figure 1.
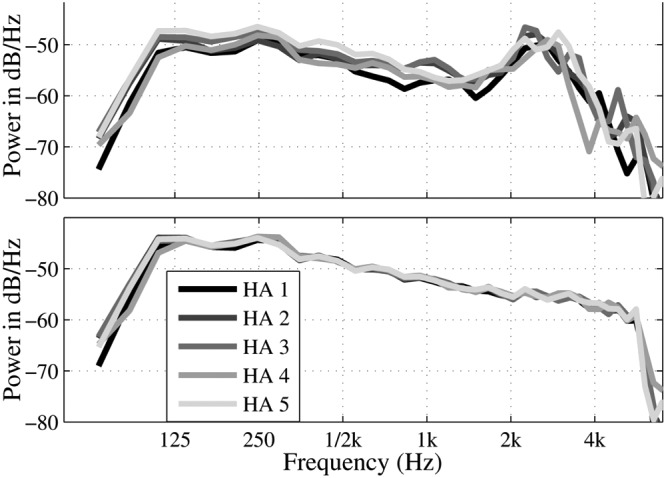
Narrowband analyses of the hearing-aid output for an input of pink noise at 70 dB SPL. The top panel shows the spectra of the raw recordings for the five hearing aids, the bottom panel shows the spectra for the recordings that were filtered with the inverse filter and bandwidth limited.
Stimulus Set 2: Bandwidth limited recordings
During the fitting, we selected a linear setting (no dynamic range compression) with the devices’ fitting software for input sound levels between 50 and 95 dB SPL and we verified the linearity of the gain by electro-acoustical measurements. For input levels below 55 dB SPL, the response of HA3 turned out to be compressed above 6 kHz. To remove this nonlinearity, we limited the frequency range of all devices to 5.8 kHz. Additionally, we used a high pass filter to remove frequencies lower than 100 Hz to limit the frequency response to those frequencies that are clinically relevant (100 Hz through 5.8 kHz). The band limitation filters were designed with Matlab (function “ellip”) and were elliptical low-pass and high-pass filters of the seventh order with a pass-band ripple of 0.1 dB, a stop band attenuation of >50 dB, and low and high frequency knee points at 100 Hz and 5800 Hz, respectively.
Stimulus Set 3: Fully filtered recordings
Inverse filters were designed to remove the remaining irregularities (after careful manual adjustment and bandwidth limiting) in the frequency response. For each hearing aid, one filter was calculated. The goal of the filter was to remove perceptually disturbing effects such as sound coloration, and not to compensate for hearing-aid processing delay and the phase response. Therefore, the required transfer function was determined with linear system identification (Bendat & Piersol, 2010). As our recordings are intended to be used for speech-in-noise measurements, it sufficed to estimate the transfer function by simply dividing the output spectrum by the input spectrum. The frequency response was measured with pink noise, because this resembles the speech spectrum as a first-order approximation. The required filter response of the inverse filter was obtained by comparing the hearing-aid output to that of a measurement microphone (B&K 2260) at the location of the hearing-aid microphone. The coefficients of the inverse filter were calculated with the Matlab function “fir2.” The constructed filter had 500 taps and was designed for noncausal application (Smith, 1997) to correct for group delay and phase distortion introduced by the filter. The maximally required correction (difference between highest unwanted peak and lowest unwanted valley) was 22 dB and the maximum slope was 50 dB/octave and occurred around 4 kHz. These requirements were met by the digital filter. The resulting time-domain impulse response was windowed with a Hamming window. Other windows (e.g., a Bartlett window) might be more suitable if an accurate low-frequency response is important, but this was not necessary now since our signals were limited to frequencies above 100 Hz. Figure 1 shows the response to pink noise for each hearing aid prior and post filtering (excluding the band limitation). As expected, the inverse filter reduced the differences in frequency responses between hearing aids. To remove differences in bandwidth, all stimuli were bandwidth limited with the same filters as used on the previous set of stimuli.
Evaluation Methods
To assess the homogenization of the recordings in the three stimulus sets, an objective quality metric was used and two listening tests were done.
Objective Evaluation
We calculated the objective Hearing-Aid Speech Quality Index (HASQI, Kates & Arehart, 2010) for all stimuli. This index estimates the quality of a target signal by comparing it to a reference signal. HASQI provides two outcome indices, one for linear effects and one for non-linear effects. The calculation for linear effects considers the change in the long-term spectral shape caused by the processing, while ignoring any changes to the signal envelope modulation. The calculation of nonlinear effects, by contrast, considers the change in signal envelope modulations caused by the processing, whereas ignoring any long-term spectral changes. This nonlinear measure is sensitive to the effects of noise, distortion, and nonlinear signal processing, and is expected to be rather insensitive to our noncausal inverse filtering. The reference signal was the original unfiltered digital input signal (i.e., the original speech-in-noise wave file that was not processed by the hearing aids). The reason for using speech in noise as reference is that we want to detect any differences caused by the filter, irrespective of whether the differences occur in the speech or in the noise. An additional calculation using the clean speech signal as reference gave the same linear HASQI scores and lower non-linear HASQI scores (with an average of 0.19) due to the fact that now the noise is not part of the reference but considered a distortion. An important observation for the validity of our approach with speech in noise was that the ranking of the hearing aids was the same for clean and noisy speech as reference signal. The target signals consisted of the three sets of stimuli. The calculation was done on the same three sentences that were used in the subjective measurements (see next section). Calculation with 50 sentences gave near identical results and will therefore not be shown.
Listening Test: Detection
To investigate whether listeners can distinguish between the hearing-aid recordings, we conducted a listening experiment with six normal-hearing (ANSI, 2004) participants. Although different from the target group, we chose normal-hearing listeners because they are assumingly better at detecting differences between stimuli than hearing-impaired listeners. Listeners with a sensorineural hearing deficit may be expected to have not only poorer hearing sensitivity, but also poorer suprathreshold processing like frequency resolution (Moore, 1996), and modulation detection (Grant, Summers, & Leek, 1998). If differences cannot be detected by normal-hearing participants, we can be quite confident that these differences will also be unnoticeable for hearing-impaired listeners. Participants were presented with three stimuli of which two were from the same hearing aid (standard) and one was from another aid (target). The participants’ task was to select the hearing aid recording that differed from the other two (i.e., an odd-ball paradigm). To limit the duration of the experiment, only Set 2 (bandwidth limited) and Set3 (fully filtered) were included and Set 1 (the raw recordings, based on a manually optimized insertion gain) was omitted. The stimulus duration was on average 2.7 s (i.e., one sentence of 1.7 s with a 0.5 s lead-in and a 0.5 sec lead-out). The stimuli were presented diotically with Sennheiser HDA200 headphones at 70 dB SPL. All combinations of hearing aids and filter conditions were presented at random in one session. Standard and target were always from the same stimulus set (i.e., bandwidth limited or fully filtered). Recordings from each hearing aid were used as target with standards of the recordings of all other hearing aids and vice versa. In total 20 distinct stimulus pairs were included (5 × 4, including AAB and BBA) and each stimulus pair was tested three times, leading to 60 trials per filter condition and thus 120 trials per participant. Directly after the participants had given their response, they received feedback on whether they had chosen the correct stimulus and if not, which one they should have chosen.
Listening Test: Preference Judgment
To determine if the inverse filtering influenced the sound quality of the signals, we also did a paired-comparison test in which the same participants were asked to choose the sound sample they preferred. The participant’s task was to make a choice based on the question: “Imagine that you will have to listen to these signals all day. Which sound would you prefer for prolonged listening?” The choice was between the fully filtered stimulus (Set 3) and its counterpart from the same hearing aid that was only bandwidth limited (Set 2). The stimuli were identical to those from the previous experiment (three comparisons per hearing aid and 5 × 3 = 15 comparisons per participant).
Results
Objective Evaluation
The results of the calculations with the HASQI model are shown in Figure 2. The mean linear index of the unfiltered signal (Set 1) of the five hearing aids was 0.865 (with a range of 0.853 to 0.872). For the bandwidth limited signals (Set 2), it was 0.863 (with a range of 0.849 to 0.871), and for the fully filtered signals (Set 3), it was 0.945 (with a range of 0.941 to 0.947). Bandwidth limiting did not reduce the maximum difference between two hearing-aids signals (0.02, for both Sets 1 and 2), but applying the full filter reduced the maximum difference to 0.006. For the nonlinear index, the average indices were 0.752 (with a range of 0.697 to 0.798) for the unprocessed, 0.759 (with a range of 0.685 to 0.793) for the bandwidth limited signals, and 0.790 (with a range of 0.731 to 0.814) for the fully filtered signals. Thus, bandwidth limitation increased the maximum difference in the nonlinear index between two hearing-aid stimuli from 0.10 (Set 1) to 0.11 (Set 2) and additional application of the inverse filter reduced the maximum difference to 0.08 (Set 3).
Figure 2.
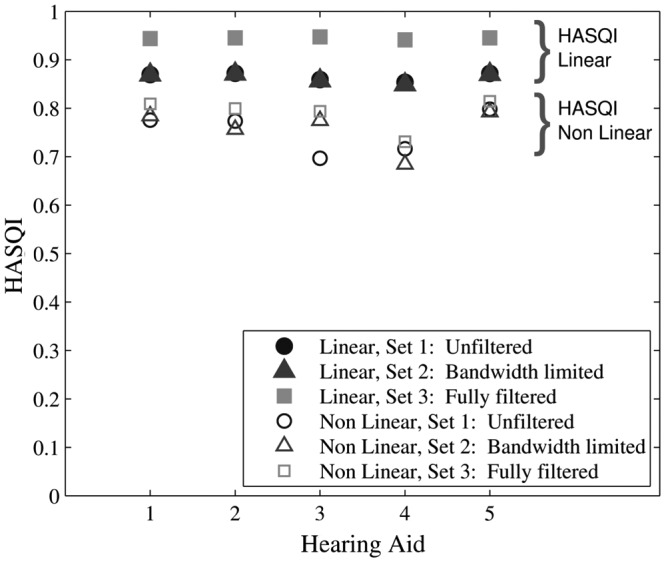
Results of the HASQI objective-quality model for the three stimulus sets.
Listening Tests
Detection Task
Figure 3 shows the percentages of correct detection averaged over all participants. The average detection score for the bandwidth limited signals was 87% and for the fully filtered signals it was 39%. A two-way analysis of variance with participant (6 levels) as random effect and hearing aid (5 levels) and stimulus set (2 levels) as fixed effects indicated that the main effect of stimulus set (fully filtered vs. bandwidth limited) was highly significant, F(1,20) = 90, p < .0005. The interaction between participant and filter type was significant as well, F(5,20) = 6, p < .005. The other main and interaction effects were statistically insignificant (p > .1). To determine if the detection rate of any of the hearing-aid signals was higher than chance (33%), one-sided t-tests were used with Bonferroni correction. For the bandwidth limited set, all results were significant (p ≤ .001). For the fully filtered stimuli, none of the results were significant (p > .13). A one-sided t-test on the pooled data of this set showed that the detection of the group of hearing aids was slightly higher than chance: 39% with p < .002 (for this no Bonferroni correction was required).
Figure 3.
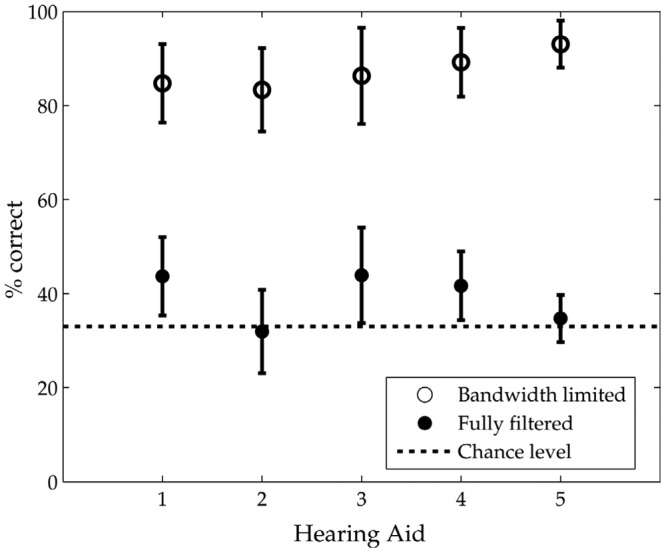
Percentage of times the participants selected the correct stimulus as deviant from the other two. Signals were only compared to others of the group they belonged to, that is, bandwidth filtered only (open circles), or fully filtered (bandwidth limited and inversely filtered, filled circles). Chance level was 33% and error bars denote 95% confidence intervals.
Preference Judgment
Five of the six participants preferred the fully filtered signals over the bandwidth limited signals in all (100%) of the sound samples, the sixth participant preferred the fully filtered signals in 73% of the sound samples.
Discussion
The results indicate that to reduce the perceptual differences between hearing-aid recordings,
it was not sufficient to carefully adjust the insertion gain of the hearing aids;
it was not sufficient to limit the bandwidth of the recordings to that of the smallest device;
it was sufficient to apply a hearing-aid specific inverse filter on the bandwidth limited recordings.
Objective Evaluation
For both Sets 1 and 2, the difference in score between the hearing aids was larger than for Set 3 (0.02 compared to 0.006). This indicates that both manual adjustment of insertion gain (Set 1) and bandwidth limitation (Set 2) were not sufficient to make the hearing-aid recordings undistinguishable from each other, and additional application of the inverse filter (Set 3) was required. Moreover, the linear HASQI score was improved by the inverse filtering, which suggests that the filter actually improved sound quality.
The range of scores for the nonlinear HASQI metric was similar for all three sets. As expected, the bandwidth limitation and the inverse filters did not greatly influence the nonlinear HASQI score. Therefore, these results indicate that the inverse filters did not add nonlinear distortions (at least for those aspects for which HASQI nonlinear is sensitive). HA3 and HA4 had lower scores than the other aids, but this does not necessarily mean that the sound quality of these hearing aids is lower. The lower scores for HA3 and HA4 indicate that these aids were perhaps not operating completely linear, although all nonlinear processing was switched off. Indeed, HA3 was shown to be compressive above 6 kHz (see Method section) and the nonlinear index increased after band-pass limiting. The reason for this is that the bandwidth limiting removed those frequencies that fell outside the linear range of the hearing aid: HA3 was the aid that limited the bandwidth in the high frequencies. The reason for the lower score for HA4 is unknown and falls beyond the scope of this article.
Listening Tests
The fact that the detection of the “oddball” was much poorer for the fully filtered signals than for the signals that were bandwidth limited only, indicates that the inverse filtering clearly increased the similarity between the hearing-aid signals. The detection for the inverse filter for each of the five hearing aids did not deviate significantly from chance.
The result for the pooled data set was slightly, but significantly, above chance (detection was 39%). The larger number of comparisons, coupled with the fact that a Bonferroni correction was not necessary here, gave larger statistical power. However, the influence of this detection rate on perceptual comparisons is expected to be only small since one will be primarily interested in differences between single pairs and thus have access to only a smaller number of comparisons than was used for the pooled data set. The higher than chance detection rate was probably caused by small residual differences in frequency response between hearing aids. These small differences are unlikely to lead to differences in quality judgments.
There was a significant interaction between participant and filter type: the difference in detection rate between the fully filtered and the bandwidth limited signals depended on the participant. The reason for this is that some participants performed worse at the detection of the bandwidth limited signals, whereas the detection of the fully filtered signals was around chance for all participants. The interaction thus reflects that participants differ in the discrimination of the bandwidth limited signals and not in the discrimination of the fully filtered signals. This interaction will therefore not be relevant for use of the inverse filter.
The second listening experiment showed that all participants preferred the fully filtered signals over the bandwidth limited signals. This supports the results from the objective quality model and indicates that the filtering did not degrade the sound quality and in fact improved it for all hearing aids. This leads to two conclusions. First, the fact that the filter did not lower the quality shows that the filter did not add distortions while reducing the differences between hearing aids. Second, it shows that the quality of the recordings could be easily improved by flattening the frequency response. This agrees with results from previous research that a smoother frequency response leads to better sound quality judgments (Arehart et al., 2010). It supports the implication of this study that quality judgment tests across hearing aids should not be based on raw recordings because this can mask the effect of the processing under investigation, but that additional filtering is required.
Application of the Inverse Filter
An inverse filter has been shown to be able to compensate for the response of the hearing aids included in this study. This compensation also works after an additional signal processing feature is turned on. The filter does this signal processing (such as noise reduction) itself because the filtering acts at the output of the hearing aid and only corrects for the characteristics that remain equal with or without the noise reduction. However, filters cannot transparently correct for compression. In case a noise reduction is implemented such that it depends on a compression stage, one would need to investigate compression and noise reduction in interaction. An inverse filter is then still required to remove differences in frequency response between hearing aids. The intended use of this research is to facilitate research into hearing aids. Application of the inverse filter in a clinical setting, (e.g., to allow clients to directly compare the effect of noise reduction between different devices) is cumbersome as the technique requires a specific filter for each device.
The normal-hearing participants preferred the recordings with a flattened frequency response. Perhaps, this result carries over to listeners with hearing loss, especially for participants with mild conductive loss. If this is true, one might contemplate to add a simplified version of the inverse filter to a hearing aid.
Instead of focusing on group results, recently the individualization of noise reduction in hearing aids has gained attention. The few available studies (Houben, Dijkstra, & Dreschler, 2011; Zakis, Hau, & Blamey, 2009) are inconclusive. The current approach might stimulate research that focuses on individuals rather than on the group they belong to.
Conclusion
We conclude that the perceptual differences between recordings of different linearly fitted hearing-aids can be removed by application of an inverse filter in combination with a band-pass filter. Application of such a filter might even improve the sound quality of the recordings. However, the main objective is to remove large differences in frequency response between hearing aids, thereby facilitating the comparison of more subtle differences between hearing aids due to nonlinear processing. Once an inverse filter is designed for a specific hearing aid, it can also be applied on recordings with (nonlinear) processing, such as noise reduction, turned on.
Acknowledgments
Approval by the Medical Ethical Committee of AMC was obtained on 24 April 2008.
Footnotes
Authors’ Note: Parts of this work were presented at the Workshop on Speech in Noise: Intelligibility and Quality, Lyon, France, 2011 and at the 130th AES Convention, London, UK, May 2011.
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from STW (Dutch Foundation for Science and Technology) for the HearClip project.
References
- ANSI Standard S3.6-2004. (2004). Specification for audiometers. New York [Google Scholar]
- Arehart K. H., Kates J. M., Anderson M. C. (2010). Effects of noise, nonlinear processing, and linear filtering on perceived speech quality. Ear and Hearing, 31, 420-436 [DOI] [PubMed] [Google Scholar]
- Bendat J. S., Piersol A. G. (2010). Random data: Analysis and measurement procedures. Hoboken, NJ: John Wiley [Google Scholar]
- Bentler R. A. (2005). Effectiveness of directional microphones and noise reduction schemes in hearing aids: A systematic review of the evidence. Journal of the American Academy of Audiology, 16, 473-484 [DOI] [PubMed] [Google Scholar]
- Boymans M., Dreschler W. A. (2000). Field trials using a digital hearing aid with active noise reduction and dual-microphone directionality. International Journal of Audiology, 39, 260-268 [DOI] [PubMed] [Google Scholar]
- Davis L. A., Davidson S. A. (1996). Preference for and performance with damped and undamped hearing aids by listeners with sensorineural hearing loss. Journal of Speech and Hearing Research, 39, 483-493 [DOI] [PubMed] [Google Scholar]
- Gabrielsson A., Schenkman B. N, Hagerman B. (1988). The effects of different frequency responses on sound quality judgments and speech intelligibility. Journal of Speech and Hearing Research, 31, 166-177 [DOI] [PubMed] [Google Scholar]
- Gabrielsson A., Sjögren H. (1979). Perceived sound quality of sound-reproducing systems. Journal of the Acoustical Society of America, 65, 1019-1033 [DOI] [PubMed] [Google Scholar]
- Grant K. W., Summers V., Leek M. R. (1998). Modulation rate detection and discrimination by normal-hearing and hearing-impaired listeners. Journal of the Acoustical Society of America, 104, 1051-1060 [DOI] [PubMed] [Google Scholar]
- Houben R., Dijkstra T. M. H., Dreschler W. A. (2011). Differences in preference for noise reduction strength between individual listeners (pp. 1-9). Proceedings of the 130th Convention of the Audio Engineering Society, London [Google Scholar]
- Kates J. M., Arehart K. H. (2010). The Hearing-Aid Speech Quality Index (HASQI). Journal of the Audio Engineering Society, 58, 363-381 [Google Scholar]
- Legarth S. V., Simonsen C. S., Bramsløw L., Le Ray G., Zacharov N. (2010). Evaluation of hearing aid performance based on normal-hearing listeners (pp. 149-154). Proceedings of the 3rd International Workshop on Perceptual Quality of Systems, Dresden, Germany [Google Scholar]
- Luts H., Eneman K., Wouters J., Schulte M., Vormann M., Buechler M., . . . Spriet A. (2010). Multicenter evaluation of signal enhancement algorithms for hearing aids. Journal of the Acoustical Society of America, 127, 1491-1505 [DOI] [PubMed] [Google Scholar]
- Moore B. C. (1996). Perceptual consequences of cochlear hearing loss and their implications for the design of hearing aids. Ear and Hearing, 17, 133-161 [DOI] [PubMed] [Google Scholar]
- Mueller H. G., Weber J., Hornsby B. W. (2006). The effects of digital noise reduction on the acceptance of background noise. Trends in Amplification, 10, 83-93 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mueller H. G., Bentler R. A., Wu Y. H. (2008). Prescribing maximum hearing aid output: Differences among manufacturers found. Hearing Journal, 61, 30-36 [Google Scholar]
- Smith S. (1997). The scientist and engineer’s guide to digital signal processing. San Diego, CA: California Technical [Google Scholar]
- Versfeld N. J., Daalder L., Festen J. M., Houtgast T. (2000). Method for the selection of sentence materials for efficient measurement of the speech reception threshold. Journal of the Acoustical Society of America, 107, 1671-1684 [DOI] [PubMed] [Google Scholar]
- Warner R. L., Bentler R. A. (2002). Thresholds of discomfort for complex stimuli: Acoustic and sound-quality predictors. Journal of Speech, Language, and Hearing Research, 45, 1016-1026 [DOI] [PubMed] [Google Scholar]
- Zakis J., Hau J., Blamey P. (2009). Environmental noise reduction configuration: Effects on preferences, satisfaction, and speech understanding. International Journal of Audiology, 48, 853-867 [DOI] [PubMed] [Google Scholar]