

Abstract
Objective
Among older white and Mexican origin male primary care patients, we examined preferences for features of depression care programs that would encourage depressed older men to enter and remain in treatment.
Method
Sixty-three (45 white, 18 Mexican origin) older men were recruited in six primary care clinics. All had clinical depression in the past year and/or were receiving depression treatment. Participants completed a conjoint analysis preference survey regarding depression treatments, providers and treatment enhancements.
Results
The data suggest that white men preferred medication over counseling [odds ratio (OR): 1.64 95% confidence interval (CI): 1.12–2.41], while Mexican origin men preferred counseling (OR: medication over counseling: 0.28, 95% CI: 0.12–0.66). Both white and Mexican origin men preferred treatment that included family involvement (vs. none) (white: OR: 1.60, 95% CI 1.12–2.30; Mexican origin: OR: 3.31 95% CI 1.44–7.62) and treatment for insomnia (vs. treatment for alcohol use) (white: OR: 1.72, 95% CI 1.01–2.91; Mexican origin: OR: 3.93 95% CI 1.35–11.42). White men also preferred treatment by telephone (OR: 1.80, 95% CI 1.12–2.87).
Conclusions
Findings could inform development of patient-centered depression treatment programs for older men and suggest strategies, such as attention to sleep problems, which providers may employ to tailor treatment to preferences of older men.
Keywords: Older men, Depression, Treatment preferences, Conjoint analysis, Latino
1. Introduction
Depression is underrecognized and undertreated in older men [1–3]. In usual primary care, less than half of older adults with depression receive treatment [4]. Rates of depression treatment are especially low for ethnic minority groups, including Mexican Americans [5]. In one primary care sample, English-speaking Mexican American older men were four times less likely to receive depression treatment compared to whites; Spanish-speaking Mexican American older men were 10 times less likely than whites to receive such treatment [6]. These disparities may result in part from the fact that available treatments and strategies for encouraging patients to enter and remain in care are not tailored to the preferences of older men. Receipt of preferred treatment may be associated with higher satisfaction, improved therapeutic alliance and, in some studies, improved depression outcomes, especially among those with a strong preference for psychotherapy [7,8].
Available literature on patient preferences has focused almost entirely on patient preferences for antidepressant medication or counseling. Although the literature is mixed and lacks comparisons between whites and Latinos, available studies suggest that Latinos are more likely to prefer counseling [9,10] and that older white men are more likely to prefer medication [11,12]. However, studies of multifaceted interventions that improve outcomes for depression care in older adults, such as collaborative care [13], suggest that other features of depression treatment, such as organization of care and patient engagement and education, are key to improving rates and quality of care. No previous study has examined older men’s preferences for treatment setting, provider type and treatment enhancements to improve engagement and retention into depression care.
In response to calls to design interventions to improve quality of treatment for depressed older men, especially Mexican Americans [5], we conducted a study that used qualitative and quantitative methods to assess patient experiences with depression and depression care among older male white non-Hispanic (hereafter white) and Mexican origin primary care patients with current major depression or recent depression treatment [6,14]. In a subsample, we used conjoint analysis, a market research survey method [15], to assess depression treatment preferences. Based on prior literature [9,10,12,16], we expected that older white men would be more likely to prefer medication, while Mexican origin men would be more likely to prefer counseling. After reviewing existing evidence-based models for improving quality of depression care for older adults and consultation with experts in the field, we designed the survey to explore older men’s preferences for treatment setting (primary care, specialty mental health or home based), provider (specialty, gender, ethnicity) and treatment features such as telephone appointments, assistance with transportation, family involvement, screening for depression and addressing other problems such as pain and insomnia.
2. Methods
2.1. Study sites and participants
This study was conducted from 2008 to 2011 in California’s central valley in two outpatient clinics of a large county hospital and in four primary care clinics associated with an academic medical center (two clinics at a teaching hospital and two in the affiliated primary care network). The study protocol was approved by Institutional Review Boards at both study sites: the University of Washington and the Rand Corporation. A two-stage screening process was used to identify older men meeting the following criteria: (a) age 60 and above, (b) self-identified Mexican origin (Mexican or US-born Mexican American) or US born white non-Hispanic, (c) current clinical depression and/or depression treatment in the past year, (d) nonpsychotic, (e) nondemented and (f) noninstitutionalized.
2.2. Data collection
The depression screening process (Fig. 1) was conducted in English or Spanish by trained, bilingual bachelors-level research assistants. In the first stage, a systematic consecutive sample of men was identified from daily clinic schedules. We attempted to approach all potentially eligible men on the schedule in clinic waiting rooms and asked each to complete a short demographic questionnaire that included a modified Patient Health Questionnaire-2 (PHQ-2) and a question on depression care (“In the past 12 months, have you had any treatment such as medications or counseling for stress, depression, or problems with sleep, appetite, or energy?”). The PHQ-2 is based on the two core symptoms of depression (i.e., depressed mood and anhedonia) that have been used successfully with older men in improving mood promoting access to collaborative treatment for late life depression [13] and other studies [17–19]. To increase the sensitivity of the instrument for this study, the time frame for the PHQ-2 was changed from the past 2 weeks to the past year. Men who screened positive for depressive symptoms and/or depression care were then asked to participate in the second screening part of the interview. In an effort to capture a subset of men who might have been false negatives on the screening items, roughly 20% of the screened men (every fifth interview) were advanced to the second phase of the screening process regardless of their scores on the screening instruments.
Fig. 1.
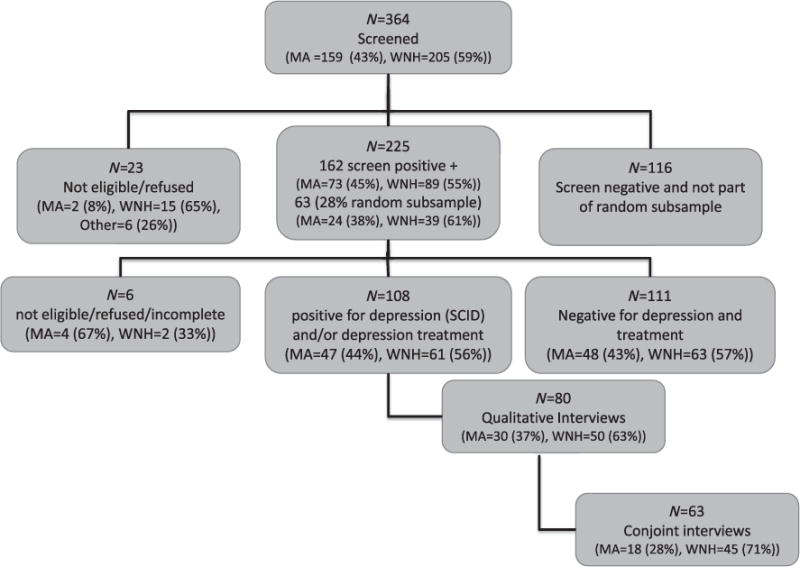
Flowchart for men’s health and aging study conjoint recruitment.
The second part of the screening included the (a) Structured Clinical Interview for DSM-IV (SCID) [20] major depression module (past month and past year) and additional questions for chronic depression, (b) a self-report of receipt of a depression diagnosis or depression treatment in the past year and (c) screening questions for psychosis and cognitive impairment (a score of 3 of greater on a six-item cognitive screener previously validated in a primary care population [21]) and (d) additional sociodemographic characteristics (e.g., health status). Chronic depression was assessed based on endorsement of three or more SCID items and at least one of two probes for chronic depressive symptoms (i.e. “In the past two years, have you been feeling sad or depressed most days even if you felt okay sometimes?” or “Have you felt down, depressed, or disinterested in things you normally enjoy on more than half of the days during the past two years?”).
2.2.1. Conjoint analysis survey
The conjoint survey was finalized after the qualitative portion of the study had already begun. Once available, we offered the conjoint survey to all 74 participants who subsequently completed qualitative interviews and attempted to contact the 6 who had previously completed qualitative interviews; 13 refused, and 4 could not be contacted.
Conjoint analysis assumes that consumers make choices among products based on product characteristics (attributes) [15]. For example, consumers shopping for an automobile might simultaneously consider size, color, price, engine power, and fuel efficiency and trade-off among these attributes to make a choice. In a conjoint analysis survey, participants choose among hypothetical products with varying combinations of attributes. To design this conjoint analysis survey, attributes of depression interventions and strategies to reduce treatment barriers were identified from the literature [22–24] and clinical guidelines [25]. A team including experts in the field of collaborative care (J.U., M.D.J.), masculinity in older adults (L.H.), culturally appropriate interventions for older Mexican origin men (C.A.V., Sergio Aguillar-Gaxiola) and preference assessment for depression (M.D.J., J.H.) came to consensus about which attributes to include in the conjoint survey. For each attribute, the team determined “levels” (or options). For depression treatment interventions, levels were determined for attributes as follows: treatment type (counseling or antidepressants), visit frequency (weekly, every 2 weeks, every month), treatment location (home, primary care or mental health clinic) and cost (no cost, $10 or $20 per month). For provider characteristics, levels were assigned for specialty (social worker, primary care provider or psychiatrist), provider gender (male or female) and cultural background (same as or different from patient). We chose to assess provider cultural background instead of language spoken so that choice sets would be relevant for both Mexican origin and white non-Hispanic men, given that, in the study clinics, provider cultural background varied, but all providers spoke English. For barrier-reduction strategies, levels were assigned for reducing transportation barriers (bus passes, treatment sessions by telephone, no assistance), family involvement (yes or no), depression screening (by written questionnaire, nurse or physician), treatment for other concerns (alcohol, insomnia, pain or loneliness) and cost (no cost, $10 or $20 per month). Attribute levels were combined to create hypothetical treatments or barrier-reduction strategies (e.g., weekly counseling at the primary care clinic for $20 per month or monthly medication visits at a mental health clinic at no cost).
The survey was administered in English or Spanish with visual depictions of combinations (Fig. 2). The survey was translated into Spanish and then reviewed by native Spanish-speaking team members, one of whom was from Mexico, who came to consensus about the appropriateness of the final translation for the study population. Each survey included six pairwise comparisons each of treatment, provider and barrier-reduction scenarios determined using a fractional factorial design. For each pair of scenarios, patients selected the one they preferred. Brief standardized descriptions of all treatment, provider and barrier-reduction attributes were read to patients before the survey was administered (script available upon request). For example, counseling was described as weekly meetings with a trained therapist to learn new ways to understand one’s problems and develop techniques to work through them; new coping skills must be practiced between sessions, and improvement may occur over weeks to months. Medication treatment was described as a treatment provided by a primary care provider or psychiatrist; medication is not addictive, should be taken daily, may have side effects that can be managed and may result in improvement after approximately 1 month.
Fig. 2.

Sample conjoint survey cards.
2.2.2. Analysis
We used univariate and bivariate analyses to describe the sample. A random utility model was used to create binary logit estimates of treatment, provider and barrier-reduction preference parameters [15]. For each regression model, the dependent variable was a binary indicator of patient’s willingness to accept or not accept treatment, and independent variables were the attribute levels. The estimated β coefficients indicate the relative utility of each attribute level, with positive values indicating stronger preference. The exp(β) represents the odds that a particular attribute level will increase overall treatment acceptance, presented as odds ratios (ORs). To examine patient characteristics associated with treatment preferences, the following baseline covariates were included in the logistic regression models based on previous literature [16,26–28]: age, site, ethnicity, education, marital status, language of interview, general health status, depression treatment and clinical depression. Conjoint data were analyzed by using the SPSS 11.5 multinomial logit regression procedure.
3. Results
Fig. 1 summarizes patient recruitment. A total of 364 men agreed to screening. Of these, 162 (45%) screened positive for probable depression or recent depression treatment. An additional 63 men were randomly selected to complete the second-stage screening. Of the 219 men completing the second-stage screening, 108 (49%) met SCID criteria for past-year clinical depression (major depression and/or chronic depressive symptoms) and/or reported depression treatment in the past year. Of these, 80 (74%) completed the qualitative interviews, and 63 (58%) completed the conjoint surveys. Compared with the 17 who completed the qualitative interview but not the survey, men who completed both were significantly more likely to be white (χ2 = 10.08, P = .001), be US born (χ2 = 8.99, P = .003), be English speaking (χ2 = 12.96, P <.0001), have greater than a high school education (χ2 =4.76, P = .029) and rate their health as good or better (versus fair or poor) (χ2 = 5.12, P = .024) than those who did not.
Characteristics of the sample are described in Table 1. Compared with white non-Hispanic men, Mexican origin men were more likely to be Spanish speaking and to have had clinical depression in the last year, but were less likely to have had depression treatment or to have completed high school. Results are presented in Table 2 for each of the three conjoint surveys (treatment type, provider type and convenience). For each attribute within each of the surveys, the OR represents the odds that a particular attribute level will increase overall treatment acceptance. Offering antidepressant medication (instead of counseling) significantly increased the odds that a white man in the sample would accept a given treatment program, whereas Mexican origin men in the sample were less likely to choose a treatment option that included medication. Frequency of treatment sessions did not significantly impact odds of treatment program acceptance. Regarding treatment setting, Mexican origin men were more likely to prefer home-based services compared to specialty mental health care, but otherwise, treatment setting did not significantly influence treatment choice.
Table 1.
Sample characteristics
| Characteristics | Overall
|
White non-Hispanic
|
Mexican origin
|
P value | |||
|---|---|---|---|---|---|---|---|
| N (63) | % | N (45) | % | N (18) | % | ||
| Age 60–64 | 31 | 49% | 21 | 47% | 10 | 56% | .524 |
| High school or above education | 45 | 71% | 37 | 82% | 7 | 39% | .001 |
| English is preferred language | 55 | 84% | 45 | 100% | 10 | 56% | .001 |
| Married | 36 | 57% | 23 | 51% | 13 | 72% | .126 |
| General health fair/poor | 37 | 59% | 26 | 58% | 11 | 61% | .808 |
| Clinical depression in past year | 48 | 76% | 31 | 69% | 17 | 94% | .031 |
| Depression treatment in past year | 40 | 63% | 34 | 54% | 6 | 33% | .002 |
| Recruitment sites | |||||||
| Large public hospital clinic | 31 | 49% | 20 | 44% | 11 | 61% | .232 |
| University based primary care clinic | 32 | 51% | 25 | 46% | 7 | 39% | .232 |
Table 2.
Logistic regression of conjoint analysis of preferences for depression treatment, provider and enhancements
| Total N=63
|
White non-Hispanic N=45
|
Mexican origin N=18
|
||||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Treatment type characteristic | ||||||
| Medication (reference is counseling) | 1.61 | 1.09–2.37 | 1.64 | 1.12–2.41 | .28 | .12–.66 |
| Frequency (reference is monthly) | ||||||
| Biweekly | .99 | .68–1.43 | .97 | .65–1.47 | .80 | .29–2.20 |
| Weekly | 1.34 | .92–1.96 | 1.40 | .90–2.17 | .85 | .37–1.95 |
| Location (reference is mental health clinic) | ||||||
| Primary care clinic | 1.08 | .72–1.61 | .89 | .56–1.41 | 2.30 | .92–5.79 |
| Home | .77 | .50–1.18 | .73 | .47–1.12 | 3.61 | 1.43–9.10 |
| Cost | .95 | .93–.97 | .96 | .94–.99 | .89 | .84–.94 |
| Provider type characteristic | ||||||
| Provider specialty (reference is social worker) | ||||||
| Psychiatrist | 2.03 | 1.27–3.25 | 1.66 | .98–2.83 | 4.04 | 1.32–12.35 |
| Primary care | 1.55 | .98–2.45 | 1.38 | .83–2.32 | 2.38 | .81–6.99 |
| Male provider (reference is female) | .97 | .69–1.36 | 1.01 | .69–1.48 | .82 | .37–1.80 |
| Provider culture same as patient (reference is different culture) | 1.40 | .94–2.09 | 1.23 | .77–1.95 | 2.00 | .80–4.99 |
| Cost | .93 | .91–.95 | .94 | .91–.96 | 0.91 | .86–.95 |
| Treatment enhancements | ||||||
| Family involvement (reference is none) | 1.75 | 1.27–2.41 | 1.60 | 1.12–2.30 | 3.31 | 1.44–7.62 |
| Convenience (reference is none) | ||||||
| Telephone appointments | 1.77 | 1.18–2.65 | 1.80 | 1.12–2.87 | 2.67 | .98–7.28 |
| Bus tokens | 1.72 | 1.07–2.77 | 1.51 | .87–2.62 | 4.74 | 1.40–16.02 |
| Screening for depression (reference is questionnaire) | ||||||
| Nurse screening | .75 | .48–1.17 | .75 | .43–1.30 | .73 | .30–1.77 |
| PCP screening | 1.82 | 1.25–2.66 | 1.90 | 1.21–2.97 | 1.79 | .79–4.03 |
| Help with other problems (reference is alcohol) | ||||||
| Loneliness | 1.50 | .95–2.39 | 1.55 | .90–2.69 | 1.27 | .50–3.22 |
| Pain | 1.27 | .82–1.97 | 1.15 | .67–1.96 | 1.32 | .56–3.09 |
| Insomnia | 2.02 | 1.28–3.18 | 1.72 | 1.02–2.91 | 3.93 | 1.35–11.42 |
CI, confidence interval; PCP, primary care provider.
Regarding provider characteristics, Mexican origin men were more likely to accept treatment from a psychiatrist compared to a social worker; however, neither white nor Mexican origin men demonstrated a significant preference regarding provider gender or cultural background.
Regarding additional features of depression treatment, both Mexican origin and white men were more likely to accept treatment that includes family involvement (compared to none) and that addressed insomnia (compared to treatment for alcohol problems). Mexican origin men were also more accepting of treatment that offered assistance with public transportation (over no such help). For white men, telephone counseling and having their primary doctor screen for depression (compared to nurse screening or written questionnaires) enhanced treatment acceptance. For all three conjoint surveys (treatment type, provider type, treatment enhancements), lower cost enhanced treatment acceptance among both white and Mexican origin men.
Our logistic regression models examined whether patient characteristics, in addition to ethnicity, were associated with preferences. Among Mexican origin men, education was the only patient characteristic that was significantly associated with preference for treatment type. Among white men, no patient characteristics were associated with preference for treatment type. Regarding provider type, age was significantly associated with preferences among Mexican origin men, while recruitment site was significantly associated with preferences among white men. Finally, in models predicting preference for treatment enhancements, among Mexican origin men, language and depressive symptom severity were significantly associated with preferences; among white men, no patient characteristics were associated with preferences for treatment enhancements.
4. Conclusions
This is the first study to employ conjoint analysis to assess treatment preferences of older men with depression and/or a recent history of depression treatment. Consistent with previous studies among depressed older adults, we found that older white men preferred medication as first-line treatment for depression [11]. In contrast, older Mexican origin men preferred counseling, more consistent with previous studies of younger, mostly female samples of Latino primary care patients [9,10]. In addition to ethnicity, the only demographic characteristic that predicted preference for treatment type was education (among Mexican origin men).
This is the first study to assess older men’s preferences for other features of depression treatment that might enhance acceptance and retention in care. While white men did not have a strong preference for treatment site or provider type, Mexican origin men found home-based treatment appealing and preferred a psychiatrist as a provider rather than a primary care provider or social worker. Although we do not know the reason behind this preference, one hypothesis is that they may have regarded psychiatrists as experts in delivering psychotherapy, the treatment they most commonly preferred. Neither Mexican origin nor white men had a significant preference for provider gender or cultural background. We lacked a sufficiently large and diverse sample of Mexican origin men to determine if preference for provider cultural background varied depending on patient acculturation.
Both white and Mexican origin men found that telephone appointments and involvement of family enhanced the appeal of a treatment program. Both white and Mexican origin men were more likely to accept treatment that addressed insomnia compared to alcohol. Neither Mexican origin nor white men were interested in treatment for alcohol problems, despite the fact that alcohol was a common theme that emerged in the qualitative interviews (unpublished data), that depression increases risk of alcohol use disorders among older adults [29] and that alcohol use increases the risk of suicide [30]. In one previous study, less than 20% of older adults who met criteria for lifetime alcohol dependence perceived a need for treatment for emotional or substance abuse issues [31]. Perceived stigma related to alcohol use disorders is more common among men than women and among Hispanics than non-Hispanic whites and has been shown to be associated with lower rates of treatment for alcohol use disorders [32].
Our results suggest that primary care and mental health providers should offer patients the choice of medication or psychotherapy given that treatment preferences vary significantly between patients. Several studies suggest the feasibility and effectiveness of training nurses and social workers to deliver brief, evidence-based psychotherapy in primary care [10,13,33], including telephone therapy; however, sustainability of such models is often challenging due to financial constraints in safety net primary care. Providers may be able to make depression care more accessible to older men by encouraging family involvement and paying more specific attention to sleep problems. Providing telephone and home-based services responds to patient preferences, and such strategies have been demonstrated to improve quality and outcomes of depression care [34–36].
Limitations of this study should be considered when interpreting these results. Conjoint analysis can reliably assess preferences in small samples [15]. However, the generalizability of our findings may still be limited, especially among the small sample of Mexican origin respondents, all of whom were enrolled in primary care and most of whom shared similar sociodemographic characteristics. Although conjoint analysis has been used in low-income and Latino immigrant populations [37–39], in this sample, Mexican origin men (especially those who are Spanish speaking and/or born outside the United States) were less likely to participate in the survey. Conjoint analysis is considered more accurate than standard survey methods and has been shown to predict consumer behavior [40,41]; however, the ability to accurately assess treatment preferences among those with limited treatment experience and knowledge may be limited. While education about attributes is standard practice in conjoint analysis surveys, content of the script may bias participants’ responses or not provide in-depth understanding of the treatment choices. Even though the white sample was larger and included a broader range of sociodemographic backgrounds, men with more education and better self-rated health were more likely to participate. Further, our sample may not reflect preferences of patients who are not enrolled in primary care and those from other regions of the United States.
Results may not reflect preferences for other types of therapies and treatments not included in the survey or the option of no treatment. Previous studies suggest that low-income patients and those with less knowledge about treatment are more likely to prefer watchful waiting to active treatment [16], a preference that may influence entry into care. Our survey did not address preferences for the combination of medications and psychotherapy, although previous studies suggest that many patients prefer this option [10] and that it may be an effective approach for some patients [42,43]. Differences between the white and Mexican origin groups in depressive disorder status, treatment experience, education and language preference may have contributed to differences in preferences between the two groups that may not have been fully accounted for by controlling for these variables in regression models.
To address these limitations, our formative results should be replicated in larger studies of older men from multiple sites and other ethnic groups, especially African Americans, who along with Mexican Americans have the lowest rates of depression treatment among all ethnic groups in the United States [5]. Additional efforts may be needed to encourage participation of Latino men, especially those with less formal education and who are Spanish speaking. Because disparities in depression care vary among subpopulations of Latinos, future work should include Latino older men from diverse backgrounds [5,44]. We plan to further explore the values and experiences that underlie treatment preferences in our sample of older men in future analyses of in-depth qualitative interviews conducted in this study. Previous studies in younger ethnically diverse primary care patients suggest that preference for treatment type appears to be associated with patients’ explanatory model for depression [45]. Those who viewed depression as resulting from the physical effects of stress on their bodies were more likely to seek help from a physician and prefer medication, while those who viewed depression as a social or psychological problem were more likely to prefer psychotherapy [45]. Furthermore, older adults who perceive depression as having a spiritual origin may also wish to incorporate religion or spirituality into their depression treatment [46,47].
Future studies should also examine whether treatment programs tailored to accommodate treatment preferences among older men would encourage entry, retention and improved outcomes among this at-risk group. Among younger, ethnically diverse primary care patients, collaborative care interventions that include patient education, activation, and choice of medication or psychotherapy can improve treatment outcomes and increase the likelihood of patients receiving preferred treatment [8,10,48–51].
Acknowledgments
Thank you to Cindy Tran for assistance with project support, data management and manuscript preparation and Mauricio Rodriguez for assistance with screening. Thank you to Dr. Sergio Aguillar-Gaxiola for expert advice.
Footnotes
Funding: National Institute of Mental Health, MHR01080067 “Reducing disparities in depression care for diverse older men”.
Prior presentations: Unützer J., Dwight-Johnson, M., Apesoa-Varano C., Hay J., Hinton L: Older men’s preferences for depression care: preliminary comparison of conjoint survey and qualitative interviews. American Association of Geriatric Psychiatry, San Antonio TX, March 18–21, 2011.
Funders: This study was supported by Award Number R01MH080067 from the National Institute of Mental Health (NIMH).
Conflicts of interest: none for any author.
References
- 1.Crystal S, Sambamoorthi U, Walkup JT, Akincigil A. Diagnosis and treatment of depression in the elderly medicare population: predictors, disparities, and trends. J Am Geriatr Soc. 2003;51(12):1718–28. doi: 10.1046/j.1532-5415.2003.51555.x. PMCID: 2486833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hinton L, Arean PA. Epidemiology, assessment, and treatment of depression in older Latinos. In: Aguilar-Gaxiola S, Gullotta T, editors. Depression in Latinos: prevention, assessment and treatment (issues in children’s and families’ lives) New York: Springer; 2008. [Google Scholar]
- 3.Hinton L, Zweifach M, Oishi S, Unutzer J. Gender disparities in the treatment of late-life depresion: qualitative and quantitative findings from the IMPACT trial. Am J Geriatr Psychiatry. 2006;14(884–892) doi: 10.1097/01.JGP.0000219282.32915.a4. [DOI] [PubMed] [Google Scholar]
- 4.Unutzer J, Katon W, Callahan CM, Williams JWJ, Hunkeler E, Harpole L, et al. Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial. JAMA. 2002;288(22):2836–45. doi: 10.1001/jama.288.22.2836. [DOI] [PubMed] [Google Scholar]
- 5.Gonzalez HM, Vega WA, Williams DR, Tarraf W, West BT, Neighbors HW. Depression care in the United States: too little for too few. Arch Gen Psychiatry. 2010;67(1):37–46. doi: 10.1001/archgenpsychiatry.2009.168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hinton L, Apesoa-Varano EC, Gonzalez HM, Aguilar-Gaxiola S, Dwight-Johnson M, Barker JC, et al. Falling through the cracks: gaps in depression treatment among older Mexican-origin and white men. Int J Geriatr Psychiatry. 2012 doi: 10.1002/gps.3779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Iacoviello BM, McCarthy KS, Barrett MS, Rynn M, Gallop R, Barber JP. Treatment preferences affect the therapeutic alliance: implications for randomized controlled trials. J Consult Clin Psychol. 2007;75(1):194–8. doi: 10.1037/0022-006X.75.1.194. [DOI] [PubMed] [Google Scholar]
- 8.Lin P, Campbell DG, Chaney EF, Liu CF, Heagerty P, Felker BL, et al. The influence of patient preference on depression treatment in primary care. Ann Behav Med. 2005;30(2):164–73. doi: 10.1207/s15324796abm3002_9. [DOI] [PubMed] [Google Scholar]
- 9.Dwight-Johnson M, Lagomasino IT, Aisenberg E, Hay J. Using conjoint analysis to assess depression treatment preferences among low-income Latinos. Psychiatr Serv. 2004;55(8):934–6. doi: 10.1176/appi.ps.55.8.934. [DOI] [PubMed] [Google Scholar]
- 10.Dwight-Johnson M, Lagomasino IT, Hay J, Zhang L, Tang L, Green JM, et al. Effectiveness of collaborative care in addressing depression treatment preferences among low-income Latinos. Psychiatr Serv. 2010;61(11):1112–8. doi: 10.1176/ps.2010.61.11.1112. [DOI] [PubMed] [Google Scholar]
- 11.Gum AM, Arean PA, Hunkeler E, Tang L, Katon W, Hitchcock P, et al. Depression treatment preferences in older primary care patients. Gerontologist. 2006;46(1):14–22. doi: 10.1093/geront/46.1.14. [DOI] [PubMed] [Google Scholar]
- 12.Dobscha SK, Corson K, Gerrity MS. Depression treatment preferences of VA primary care patients. Psychosomatics. 2007;48(6):482–8. doi: 10.1176/appi.psy.48.6.482. [DOI] [PubMed] [Google Scholar]
- 13.Unutzer J, Katon W, Williams JWJ, Callahan CM, Harpole L, Hunkeler EM, et al. Improving primary care for depression in late life: the design of a multicenter randomized trial. Med Care. 2001;39(8):785–99. doi: 10.1097/00005650-200108000-00005. [DOI] [PubMed] [Google Scholar]
- 14.Apesoa-Varano EC, Hinton L, Barker JC, Unutzer J. Clinician approaches and strategies for engaging older men in depression care. Am J Geriatr Psychiatry. 2010 doi: 10.1097/JGP.0b013e3181d145ea. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Louviere JHD, Swait J. Stated choice methods. New York: Cambridge University Press; 2000. [Google Scholar]
- 16.Dwight-Johnson M, Sherbourne CD, Liao D, Wells KB. Treatment preferences among depressed primary care patients. J Gen Intern Med. 2000;15(8):527–34. doi: 10.1046/j.1525-1497.2000.08035.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lowe GA, Gibson RC. Depression in adolescence: new developments. West Indian Med J. 2005;54(6):387–91. doi: 10.1590/s0043-31442005000600009. [DOI] [PubMed] [Google Scholar]
- 18.Kroenke K, Spitzer RL, Williams JB. The patient health questionnaire-2: validity of a two-item depression screener. Med Care. 2003;41(11):1284–92. doi: 10.1097/01.MLR.0000093487.78664.3C. [DOI] [PubMed] [Google Scholar]
- 19.Corson K, Gerrity MS, Dobscha SK. Screening for depression and suicidality in a VA primary care setting: 2 items are better than 1 item. Am J Manag Care. 2004;10(11):839–45. [PubMed] [Google Scholar]
- 20.First MB, Spitzer RL, Gibbon M, Williams JBW. Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition. (SCID-I/P) New York: New York State Psychiatric Institute; 2002. [Google Scholar]
- 21.Callahan CM, Unverzagt FW, Hui SL, Perkins AJ, Hendrie HC. Six-item screener to identify cognitive impairment among potential subjects for clinical research. Med Care. 2002;40(9):771–81. doi: 10.1097/00005650-200209000-00007. [DOI] [PubMed] [Google Scholar]
- 22.Wells KB. The design of Partners in Care: evaluating the cost-effectiveness of improving care for depression in primary care. Soc Psychiatry Psychiat Epidemiol. 1999;34(1):20–9. doi: 10.1007/s001270050107. [DOI] [PubMed] [Google Scholar]
- 23.Unutzer J, Katon W, Callahan AM, et al. Depression treatment in a sample of 1,801 depressed older adults in primary care. J Am Geriatr Soc. 2003;51:505–14. doi: 10.1046/j.1532-5415.2003.51159.x. [DOI] [PubMed] [Google Scholar]
- 24.Blazer DG, Steffens DC. The American Psychiatric Publishing textbook of geriatric psychiatry. 4. Washington (DC): American Psychiatric Pub; 2009. [Google Scholar]
- 25.Schulberg HC, Katon W, Simon GE, Rush AJ. Treating major depression in primary care practice — an update of the agency for health care policy and research practice guidelines. Arch Gen Psychiatry. 1998;55(12):1121–7. doi: 10.1001/archpsyc.55.12.1121. [DOI] [PubMed] [Google Scholar]
- 26.Interian A, Martinez IE, Guarnaccia PJ, Vega WA, Escobar JI. A qualitative analysis of the perception of stigma among Latinos receiving antidepressants. Psychiatr Serv. 2007;58(12):1591–4. doi: 10.1176/appi.ps.58.12.1591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Vega WA, Kolody B, Aguilar-Gaxiola S. Help seeking for mental health problems among Mexican Americans. J Immigr Health. 2001;3(3):133–40. doi: 10.1023/A:1011385004913. [DOI] [PubMed] [Google Scholar]
- 28.Vega WA, Kolody B, Aguilar-Gaxiola S, Catalano R. Gaps in service utilization by Mexican Americans with mental health problems. Am J Psychiatry. 1999;156(6):928–34. doi: 10.1176/ajp.156.6.928. [DOI] [PubMed] [Google Scholar]
- 29.Sacco P, Bucholz KK, Spitznagel EL. Alcohol use among older adults in the National Epidemiologic Survey on Alcohol and Related Conditions: a latent class analysis. J Stud Alcohol Drugs. 2009;70(6):829–38. doi: 10.15288/jsad.2009.70.829. PMCID: 2776115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kaplan MS, McFarland BH, Huguet N. Characteristics of adult male and female firearm suicide decedents: findings from the National Violent Death Reporting System. Inj Prev. 2009;15(5):322–7. doi: 10.1136/ip.2008.021162. [DOI] [PubMed] [Google Scholar]
- 31.Garrido MM, Kane RL, Kaas M, Kane RA. Perceived need for mental health care among community-dwelling older adults. J Gerontol B Psychol Sci Soc Sci. 2009;64(6):704–12. doi: 10.1093/geronb/gbp073. PMCID: 2763014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Keyes KM, Hatzenbuehler ML, McLaughlin KA, Link B, Olfson M, Grant BF, et al. Stigma and treatment for alcohol disorders in the United States. Am J Epidemiol. 2010;172(12):1364–72. doi: 10.1093/aje/kwq304. PMCID: 2998202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Dwight-Johnson M, Aisenberg E, Golinelli D, Hong S, O’Brien M, Ludman E. Telephone-based cognitive–behavioral therapy for Latino patients living in rural areas: a randomized pilot study. Psychiatr Serv. 2011;62(8):936–42. doi: 10.1176/ps.62.8.pss6208_0936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ciechanowski P, Wagner E, Schmaling K, Schwartz S, Williams B, Diehr P, et al. Community-integrated home-based depression treatment in older adults: a randomized controlled trial. JAMA. 2004;291(13):1569–77. doi: 10.1001/jama.291.13.1569. [DOI] [PubMed] [Google Scholar]
- 35.Oslin DW, Sayers S, Ross J, Kane V, Ten Have T, Conigliaro J, et al. Disease management for depression and at-risk drinking via telephone in an older population of veterans. Psychosom Med. 2003;65(6):931–7. doi: 10.1097/01.psy.0000097335.35776.fb. [DOI] [PubMed] [Google Scholar]
- 36.Simon GE, Ludman EJ, Tutty S, Operskalski B, Von Korff M. Telephone psychotherapy and telephone care management for primary care patients starting antidepressant treatment: a randomized controlled trial. JAMA. 2004;292(8):935–42. doi: 10.1001/jama.292.8.935. [DOI] [PubMed] [Google Scholar]
- 37.Newman PA, Duan N, Lee SJ, Rudy ET, Seiden DS, Kakinami L, et al. HIV vaccine acceptability among communities at risk: the impact of vaccine characteristics. Vaccine. 2006;24(12):2094–101. doi: 10.1016/j.vaccine.2005.11.013. PMCID: 2819665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Bair RM, Mays RM, Sturm LA, Perkins SM, Juliar BE, Zimet GD. Acceptability to Latino parents of sexually transmitted infection vaccination. Ambul Pediatr. 2008;8(2):98–103. doi: 10.1016/j.ambp.2007.11.002. [DOI] [PubMed] [Google Scholar]
- 39.Ratcliffe J, Buxton M, McGarry T, Sheldon R, Chancellor J. Patients’ preferences for characteristics associated with treatments for osteoarthritis. Rheumatology (Oxford) 2004;43(3):337–45. doi: 10.1093/rheumatology/keh038. [DOI] [PubMed] [Google Scholar]
- 40.Phillips KA, Johnson FR, Maddala T. Measuring what people value: a comparison of “attitude” and “preference” surveys. Health Serv Res. 2002;37(6):1659–79. doi: 10.1111/1475-6773.01116. PMCID: 1464045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Phillips KA, Maddala T, Johnson FR. Measuring preferences for health care interventions using conjoint analysis: an application to HIV testing. Health Serv Res. 2002;37(6):1681–705. doi: 10.1111/1475-6773.01115. PMCID: 1464051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Cuijpers P, van Straten A, Warmerdam L, Andersson G. Psychotherapy versus the combination of psychotherapy and pharmacotherapy in the treatment of depression: a meta-analysis. Depress Anxiety. 2009;26(3):279–88. doi: 10.1002/da.20519. [DOI] [PubMed] [Google Scholar]
- 43.Manber R, Kraemer HC, Arnow BA, Trivedi MH, Rush AJ, Thase ME, et al. Faster remission of chronic depression with combined psychotherapy and medication than with each therapy alone. J Consult Clin Psychol. 2008;76(3):459–67. doi: 10.1037/0022-006X.76.3.459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Rodriguez MA, Vega WA. Confronting inequities in Latino health care. J Gen Intern Med. 2009;24(Suppl 3):505–7. doi: 10.1007/s11606-009-1128-0. PMCID: 2764046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Karasz A, Watkins L. Conceptual models of treatment in depressed Hispanic patients. Ann Fam Med. 2006;4(6):527–33. doi: 10.1370/afm.579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Wittink MN, Joo JH, Lewis LM, Barg FK. Losing faith and using faith: older African Americans discuss spirituality, religious activities, and depression. J Gen Intern Med. 2009;24(3):402–7. doi: 10.1007/s11606-008-0897-1. PMCID: 2642557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Stanley MA, Bush AL, Camp ME, Jameson JP, Phillips LL, Barber CR, et al. Older adults’ preferences for religion/spirituality in treatment for anxiety and depression. Aging Ment Health. 2011;15(3):334–43. doi: 10.1080/13607863.2010.519326. [DOI] [PubMed] [Google Scholar]
- 48.Aisenberg E, Dwight-Johnson M, Golinelli D, Ludman E, editors. Telephone cognitive behavioral therapy for rural Latinos: a randomized pilot study. Seattle (WA): Society of Behavioral Medicine; 2010. [Google Scholar]
- 49.Dwight-Johnson M, Unutzer J, Sherbourne C, Tang L, Wells KB. Can quality improvement programs for depression in primary care address patient preferences for treatment? Med Care. 2001;39(9):934–44. doi: 10.1097/00005650-200109000-00004. [DOI] [PubMed] [Google Scholar]
- 50.Arean PA, Ayalon L, Hunkeler E, Lin EH, Tang L, Harpole L, et al. Improving depression care for older, minority patients in primary care. Med Care. 2005;43(4):381–90. doi: 10.1097/01.mlr.0000156852.09920.b1. [DOI] [PubMed] [Google Scholar]
- 51.Unutzer J, Katon W, Callahan C, Williams JWJ, Hunkeler E, Harpole L, et al. Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial. J Am Med Assoc. 2002;288(22):2836–45. doi: 10.1001/jama.288.22.2836. [DOI] [PubMed] [Google Scholar]