

INTRODUCTION
Patients exposed to bisphosphonates or other antiresorptive medications are at risk for developing osteonecrosis of the jaws (ONJ). ONJ is also associated with other diseases or etiologies [1–3]. For the purposes of this paper, the term ONJ only applies to those patients exposed to antiresorptive medications who develop osteonecrosis. ONJ is a complex disease involving multiple tissue and cell-type responses to wound healing and/or infection. The American Association of Oral and Maxillofacial Surgeons (AAOMS) defines BRONJ as exposed, necrotic bone in the maxillofacial region that has persisted for more than eight weeks in a patient with current or previous bisphosphonate treatment, without a history of radiation therapy to the jaws [4, 5]. Since the first reported ONJ cases in 2003 and 2004, there has been little advancement in understanding the etiology and pathophysiology of ONJ [6, 7]. Many hypotheses are proposed, including bisphosphonate (BP) toxicity to oral epithelium, altered wound healing after tooth extraction, high turnover of the mandible and maxilla, oral biofilm formation, infection and inflammation, and suppression of angiogenesis and bone turnover [8, 9].
The current classification system of ONJ involves Stages 0–3, and is based on patient clinical presentation. While a stage 0 ONJ patient will not present with any exposed bone, making it difficult to diagnose, stages 1–3 are all defined, in part, by a patient with bone exposed to the oral cavity. Stage 1 patients are asymptomatic and show no signs of infection, but a Stage 2 ONJ patient will present with infection that is often associated with pain, erythema, and purulent drainage. Stage 3 ONJ involves necrotic bone extending past the alveolus, pathological fracture, extraoral fistula, oral antral/oral nasal communication, or osteolysis extending to the inferior border of the mandible or the sinus floor [5].
Since the initial reports in BP treated patients, ONJ has been reported in patients receiving the osteoclast inhibitor denosumab. BPs and denosumab target osteoclasts through distinct mechanisms. BPs are released from hydroxyapatite in bone during remodeling and induce osteoclast apoptosis and inhibit osteoclast differentiation and function [10–13]. In contrast, denosumab targets osteoclast precursors by binding RANK, preventing the RANKL-RANK complex formation to inhibit osteoclast formation, differentiation, and function [14, 15]. Notwithstanding pharmacologic differences, both of these drugs ultimately prevent osteoclasts from resorbing bone, making inhibition of bone remodeling a critical factor in the pathogenesis of ONJ [9].
We, and others, have described ONJ in patients receiving denosumab therapy [5, 16–19]. Published literature indicates that both osteoclast inhibitors induce similar severity and prevalence of classic ONJ disease with bone exposure [20–23]. From all published descriptions, it appears that the clinical and radiographic appearance of exposed, necrotic bone in patients receiving denosumab is similar to BP associated disease. However, it is not clear if denosumab treatment can result in stage 0 ONJ.
Here, we extend the spectrum of parallel clinical presentation to stage 0 disease, as we present a case of ONJ without clinical bone exposure in a patient on denosumab. This case further demonstrates the full-spectrum similarities in the clinical, radiographic, and histologic manifestations of BP- and denosumab-associated ONJ. Our findings are significant in two folds. From a pathophysiological perspective, these similarities point to osteoclast inhibition as a central mechanism in ONJ development. From a clinical perspective, as denosumab use is becoming more common, awareness of the likelihood of stage 0 disease in these patients should readily enter the diagnostic realm of possibility.
REPORT OF A CASE
A 26 year-old male presented to the oral and maxillofacial surgery clinic at the University of California, Los Angeles (UCLA) School of Dentistry to evaluate some fractured and painful teeth, especially dull pain in the lower right. His medical history was significant for a left sacral giant cell tumor (GCT) diagnosed in 2009. He had been treated with 120mg subcutaneous denosumab every 3 months until January 2011. His therapy was suspended for almost a year until he resumed denosumab treatment in December 2011, now at 120mg subcutaneous every 1–2 months. In March 2013, he presented with several fractured teeth, with pain mostly in the lower right. He had not seen a dentist in several years. His medical history was not significant, and his only surgery was placement of a ventriculoperitoneal shunt as a child. His medications at the time of presentation included oxycodone, dilaudid, neurontin, methacarbamol, calcium, vitamin D, and a history of denosumab (Amgen, Thousand Oaks, CA). His oncologist had suspended the denosumab therapy in December 2012 until he could be dentally cleared.
Upon examination, there were multiple carious and fractured teeth that were sensitive to palpation including teeth 4 and 14, with only root tips present of 5, 12, 19, and 30 (Fig 1). There were no active signs of infection, without purulence, erythema, or edema. There was no paresthesia, anesthesia, or dysesthesia at the time of presentation. The panoramic radiograph revealed multiple grossly carious teeth (Fig 2, white arrows) with widening of the periodontal ligament (PDL) space and loss of lamina dura, suggestive of periapical disease. In particular, increased alveolar bone density was observed around teeth # 19 and 30 (Fig 2B and C, black arrows). The sclerotic bone changes appeared more extensive on the right side.
Figure 1.

Clinical presentation of the patient. Root fragments in the areas of #19 and 30 can be seen. However, no evidence of bone exposure or fistula formation is present.
Figure 2.
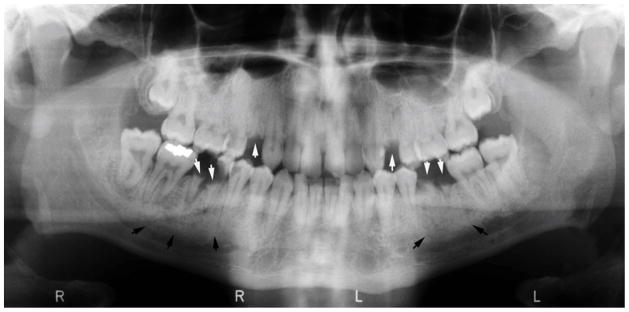


A) Panoramic radiograph of patient at the time of presentation. B) and C) magnified areas of the panoramic radiograph focusing on the posterior right and left mandible, respectively. White arrows point to the root fragments, while black arrows show areas of increased bone density.
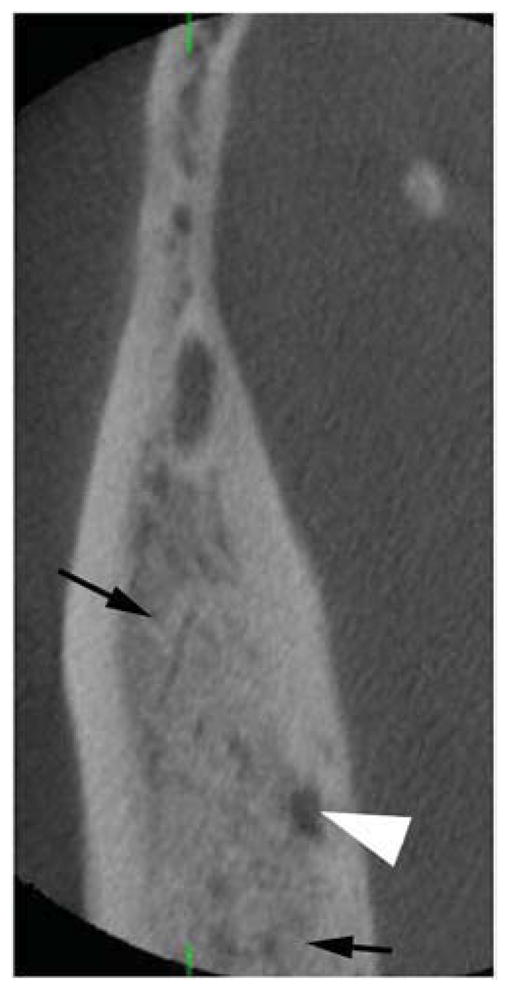
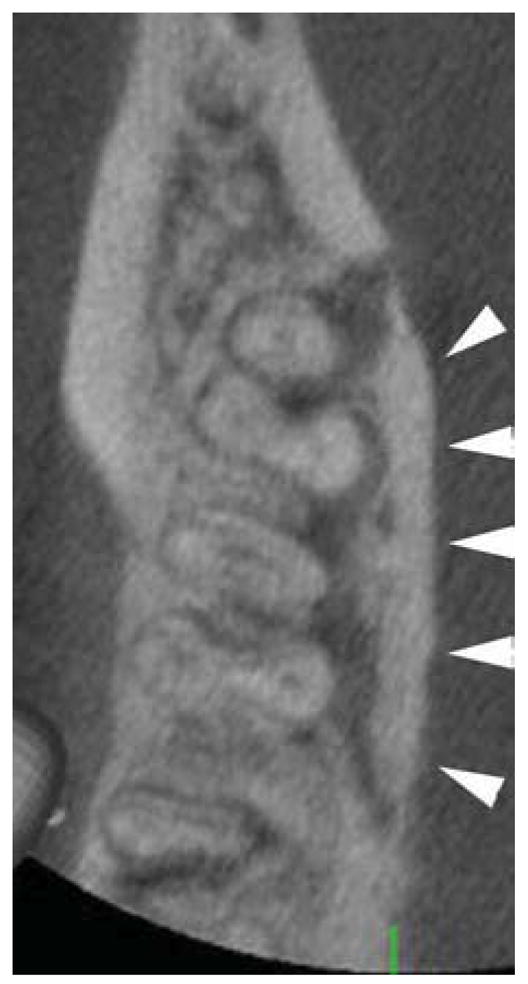
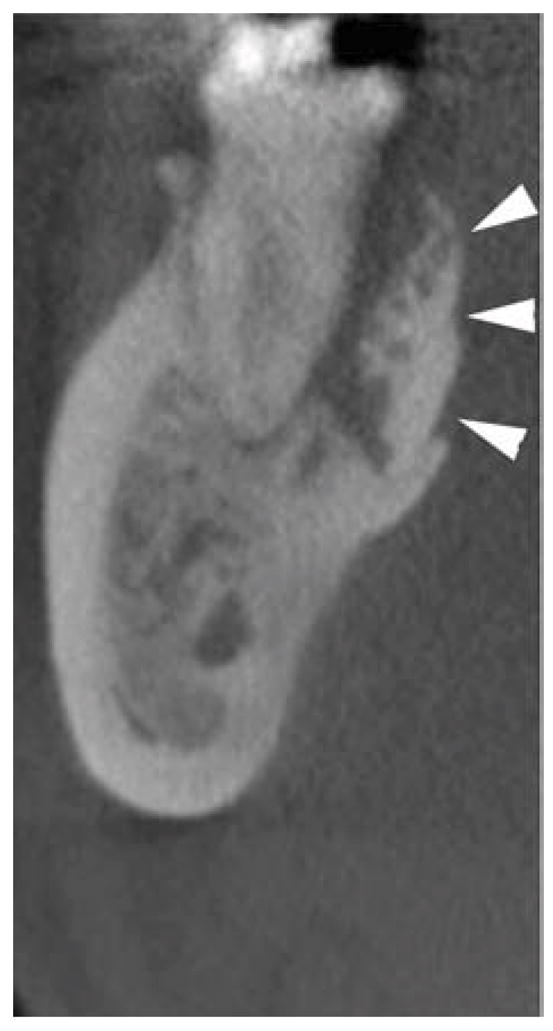
To further examine the alveolar bone architecture in detail, high-resolution, limited field of view (FOV) cone-beam CT (CBCT) scans were obtained, utilizing the Morita Accuitomo 170 scanner at a 4×4 cm FOV. The CBCT scans showed the root fragments of teeth 19 and 30 (Fig 3, white arrows) and increased trabecular density of the alveolar ridge with loss of trabecular architecture (Fig 3, black arrows). Multiple small areas of osteolysis were also observed (Fig 3, white arrowheads). These changes were more extensive on the right side extending from the retromolar area to the area of the premolars, and from the alveolar crest to the inferior border of the mandible, through the full bucco-lingual width of the mandible. In contrast, on the left side, trabecular changes were mostly localized to the area of #18–20. Importantly, CBCT scans revealed the presence of a large segment of the lingual cortical plate that was separated from the adjacent cortical and trabecular bone. This bone fragment extended from the distal surface of # 30 to the distal surface of # 32 (Fig 4, white arrowheads), highly suggestive of a bone sequestrum.
Figure 3.
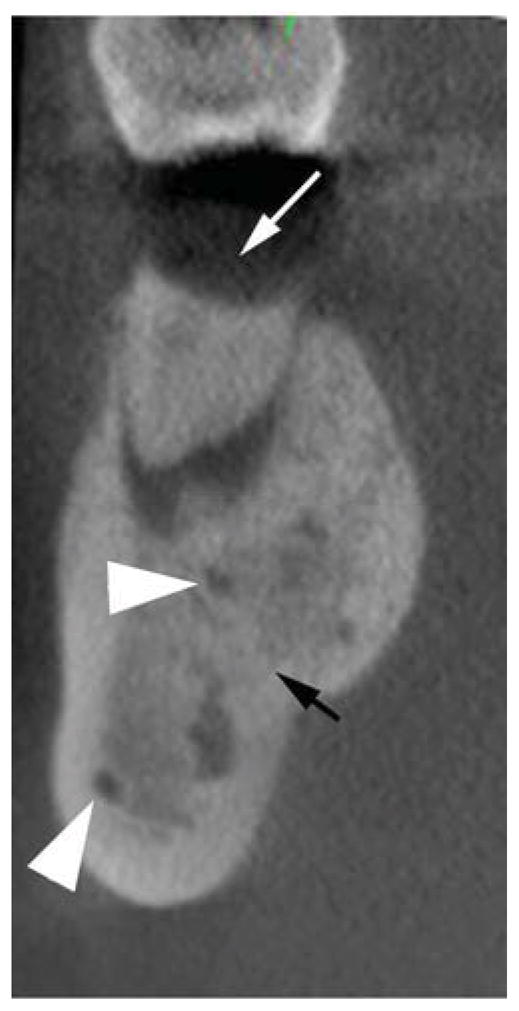
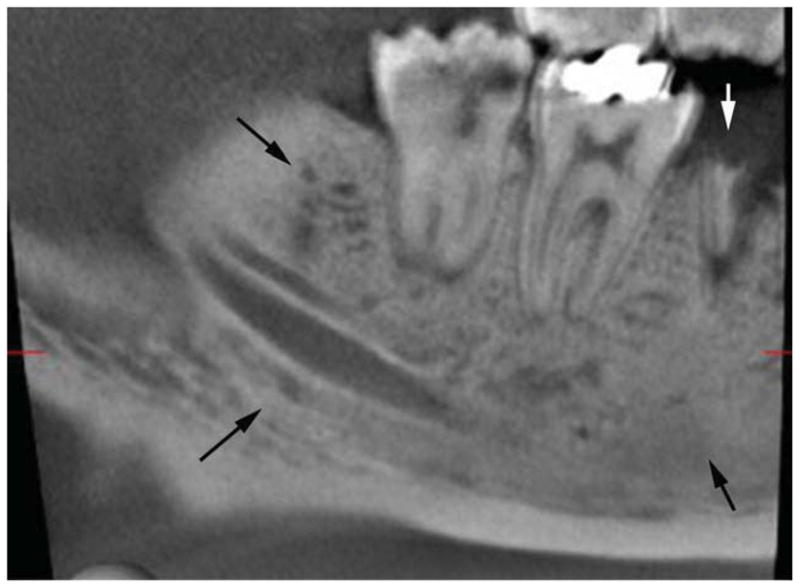
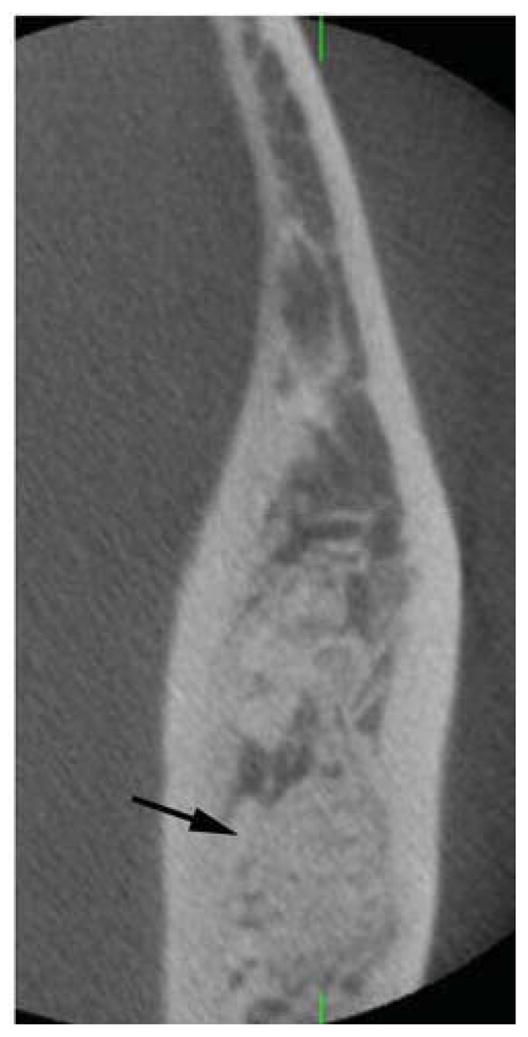


Axial (A, D), cross-sectional (B, E) and sagittal (C, F) cone beam CT (CBCT) slices of the patient’s right (A, B, C) and left (D, E, F) posterior mandible. White arrows point to root fragments, black arrows to areas of increased trabecular density and loss of trabecular architecture, and white arrowhead to radiolucent areas.
Figure 4.
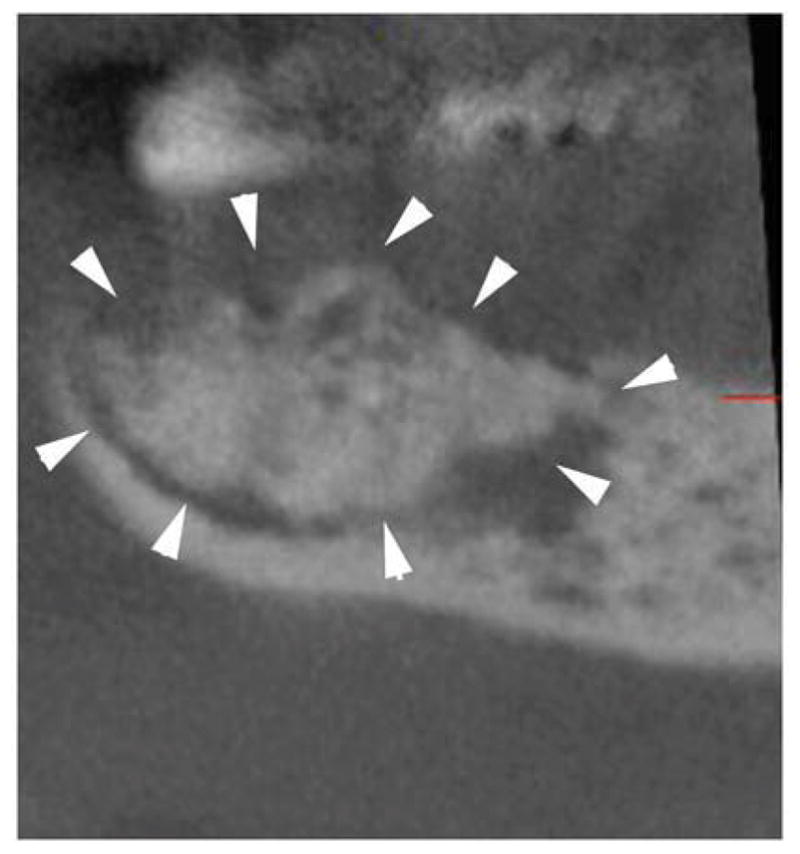
Axial (A), cross-sectional (B) and sagittal (C) CBCT slices through the area of the lingual cortical plate of the posterior right mandible. White arrowheads delineate the sequestrum outline.
From the patient history and exam, coupled with the radiographic findings, we developed a differential diagnosis, which included chronic sclerosing osteomyelitis, fibro-osseous disease, primary or metastatic malignancy, and stage 0 ONJ [5, 18, 24]. Due to the risk of infection and potentially increased severity of ONJ, it was deemed necessary to extract the teeth with significant dental disease, and biopsy the bone sequestrum that was seen radiographically. First, the denosumab was not used for an additional 2 months, and the patient was started on amoxicillin therapy 500 mg orally three times per day and chlorhexidine 0.12% mouthrinse twice per day. After 2 months, teeth 5, 12, 19, and 30 were extracted with debridement of the sockets and removal of the loose bone sequestrum. The bone fragment was submitted to pathology for histologic examination. Hematoxylin and eosin staining revealed complete osteonecrosis with empty osteocytic lacunae (Fig 5, blue arrows) and rimming by neutrophils (Fig 5, green arrows) throughout the full extent of the bone fragment. No osteocytes, osteoblasts, or osteoclasts were present. With the combination of imaging and biopsy results, coupled with antiresorptive therapy, a diagnosis of Stage 0 ONJ was confirmed.
Figure 5.


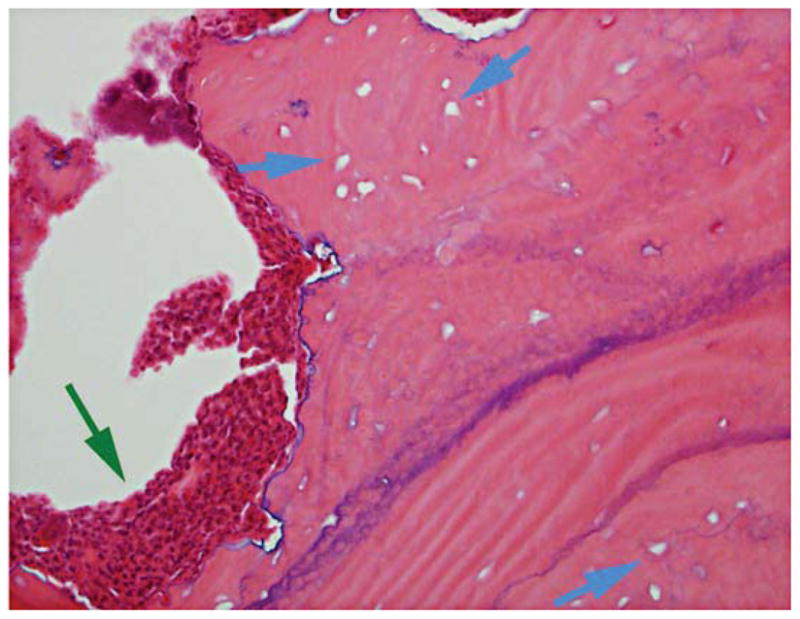
4X (A), 10X (B), and 20X (C) magnification of H&E stained histologic sections of the bone fragment. Blue arrows point to empty osteocytic lacunae, while green arrows point to neutrophil rimming of the bone. No osteoblasts, osteocytes or osteoclasts are seen.
DISCUSSION
BP treated patients can present with ONJ-like radiographic or clinical symptoms, but without orally exposed bone [17, 18, 24, 25], compelling modification of the original ONJ classification to add stage 0 disease [5]. Stage 0 ONJ is characterized by absence of clinically exposed bone in patients presenting with non-specific symptoms or clinical and radiographic findings [5]. Stage 0 disease has been reported in patients receiving intravenous and oral BPs, but may be underestimated [24–28]. In fact, up to 30% of ONJ cases may present without exposed bone [17, 29]. This non-exposed bone variant, or stage 0 ONJ, underscores the importance of early diagnosis. Other than clinical symptoms [17, 25, 28], radiographic evaluation has been most valuable in diagnosing stage 0 disease [18].
To date, stage 0 ONJ has only been reported in patients on BP therapy. The clinical symptoms may be nonspecific such as odontalgia not explained by an odontogenic cause, dull and aching bone pain in the body of the mandible that may radiate to the TMJ region, sinus pain which could be associated with inflammation and thickening of the maxillary sinus wall, or altered neurosensory function. More specific clinical findings may include loosening of teeth not explained by chronic periodontal disease or periapical/periodontal fistula not associated with pulpal necrosis due to caries [5]. Our patient presented with dull bone pain, especially in the lower right posterior region. Although he is taking denosumab and not BP, this further supports the full spectrum similarities between BP-associated ONJ and denosumab-associated ONJ.
Several studies have investigated stage 0 ONJ in BP-treated patients. The AAOMS defines stage 0 radiographic features in BP-treated patients as alveolar bone loss not attributable to chronic periodontal disease, trabecular bone alterations including dense woven bone, and persistent unremodeled bone in extraction sites, thickening of the lamina dura, and inferior alveolar canal narrowing [5]. Furthermore, sequestration of necrotic non-exposed bone has been reported [25]. These findings were substantiated in a radiographic study of BP-treated patients with concerning clinical symptoms. Findings on panoramic radiographs, computed tomography, and cone beam computed tomography included regional or diffuse osteosclerosis of the alveolar margins or lamina dura, cortical disruption, uniform periradicular radiolucencies, prominent inferior alveolar nerve canal, persisting alveolar socket, and thickened buccal or lingual cortices [18]. Similar findings were noted in our denosumab-treated patient with stage 0 disease. A panoramic radiograph revealed diffuse trabecular architecture and osteosclerosis, but failed to detect the presence of sequestreation. This underscores the limitations of 2-dimensional radiography, including intraoral and panoramic radiographs in ONJ diagnosis, especially in evaluation of stage 0 disease. Indeed, conventional radiographs can underestimate the presence and extent of cortical and trabecular changes in ONJ patients [30, 31]. However, high-resolution CBCT scans clearly delineated the presence of a bony sequestrum on the lingual aspect of the alveolus. The radiographic detection of bone sequestration had a major impact on the management of this patient. Because of the difficulty in diagnosing stage 0 ONJ clinically or with conventioanal radiographs, we recommend advanced imaging for all patients on anti-resorptive therapy with non-specific symptomatology.
The hallmark of ONJ in both human and animal histopathological studies is the presence of necrotic bone with osteocyte loss and empty lacunae [32–35]. Although stage 0 ONJ was not in the original disease description, animal studies suggest that stage 0 ONJ is not uncommon [36–44]. Due to the recommended conservative treatment of ONJ, large histologic studies in stage 0 patients are lacking. However, animal data report the presence of necrotic bone in the absence of bone exposure that can be as high as 66% [36, 41]. In patients, stage 0 disease often progresses to stage 1, 2, or 3, and 30% of ONJ cases may initially present without clinical evidence of exposed necrotic bone [17, 24]. Here we report the confirmed histologic diagnosis of ONJ in a stage 0 patient receiving denosumab.
As data are being collected in large clinical trials, the importance of stage 0 diagnosis for complete assessment of ONJ is apparent. These large studies demonstrate a similar prevalence in ONJ for BP vs. denosumab treatment [20–23]. However, these studies only include stage 1–3 disease. Diagnosis of stage 0 disease will more accurately reflect disease burden, and will allow earlier intervention with preventative or therapeutic modalities. In conclusion, we report a case of stage 0 ONJ confirmed radiographically and histologically in a patient on denosumab treatment. Importantly, our data add to the evidence that denosumab associated ONJ is similar to BP associated ONJ in the full spectrum of the disease, and emphasizes the central role of bone remodeling suppression in disease pathophysiology.
Acknowledgments
This work was supported by NIH/NIDCR DE019465 and DE021444.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Farah CS, Savage NW. Oral ulceration with bone sequestration. Aust Dent J. 2003;48:61. doi: 10.1111/j.1834-7819.2003.tb00011.x. [DOI] [PubMed] [Google Scholar]
- 2.Meer S, Coleman H, Altini M, Alexander T. Mandibular osteomyelitis and tooth exfoliation following zoster-CMV co-infection. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:70. doi: 10.1016/j.tripleo.2005.06.022. [DOI] [PubMed] [Google Scholar]
- 3.Schwartz HC. Osteonecrosis of the jaws: a complication of cancer chemotherapy. Head Neck Surg. 1982;4:251. doi: 10.1002/hed.2890040313. [DOI] [PubMed] [Google Scholar]
- 4.Advisory Task Force on Bisphosphonate-Related Ostenonecrosis of the Jaws AAoO, Maxillofacial S American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaws. J Oral Maxillofac Surg. 2007;65:369. doi: 10.1016/j.joms.2006.11.003. [DOI] [PubMed] [Google Scholar]
- 5.Ruggiero SL, Dodson TB, Assael LA, Landesberg R, Marx RE, Mehrotra B American Association of O Maxillofacial S. American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaws--2009 update. J Oral Maxillofac Surg. 2009;67:2. doi: 10.1016/j.joms.2009.01.009. [DOI] [PubMed] [Google Scholar]
- 6.Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. J Oral Maxillofac Surg. 2003;61:1115. doi: 10.1016/s0278-2391(03)00720-1. [DOI] [PubMed] [Google Scholar]
- 7.Ruggiero SL, Mehrotra B, Rosenberg TJ, Engroff SL. Osteonecrosis of the jaws associated with the use of bisphosphonates: a review of 63 cases. J Oral Maxillofac Surg. 2004;62:527. doi: 10.1016/j.joms.2004.02.004. [DOI] [PubMed] [Google Scholar]
- 8.Landesberg R, Woo V, Cremers S, Cozin M, Marolt D, Vunjak-Novakovic G, Kousteni S, Raghavan S. Potential pathophysiological mechanisms in osteonecrosis of the jaw. Ann N Y Acad Sci. 2011;1218:62. doi: 10.1111/j.1749-6632.2010.05835.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Yamashita J, McCauley LK. Antiresorptives and osteonecrosis of the jaw. J Evid Based Dent Pract. 2012;12:233. doi: 10.1016/S1532-3382(12)70046-5. [DOI] [PubMed] [Google Scholar]
- 10.Coxon FP, Helfrich MH, Van’t Hof R, Sebti S, Ralston SH, Hamilton A, Rogers MJ. Protein geranylgeranylation is required for osteoclast formation, function, and survival: inhibition by bisphosphonates and GGTI-298. J Bone Miner Res. 2000;15:1467. doi: 10.1359/jbmr.2000.15.8.1467. [DOI] [PubMed] [Google Scholar]
- 11.McClung M, Harris ST, Miller PD, Bauer DC, Davison KS, Dian L, Hanley DA, Kendler DL, Yuen CK, Lewiecki EM. Bisphosphonate therapy for osteoporosis: benefits, risks, and drug holiday. Am J Med. 2013;126:13. doi: 10.1016/j.amjmed.2012.06.023. [DOI] [PubMed] [Google Scholar]
- 12.Rogers MJ. From molds and macrophages to mevalonate: a decade of progress in understanding the molecular mode of action of bisphosphonates. Calcif Tissue Int. 2004;75:451. doi: 10.1007/s00223-004-0024-1. [DOI] [PubMed] [Google Scholar]
- 13.Rogers MJ, Gordon S, Benford HL, Coxon FP, Luckman SP, Monkkonen J, Frith JC. Cellular and molecular mechanisms of action of bisphosphonates. Cancer. 2000;88:2961. doi: 10.1002/1097-0142(20000615)88:12+<2961::aid-cncr12>3.3.co;2-c. [DOI] [PubMed] [Google Scholar]
- 14.Baron R, Ferrari S, Russell RG. Denosumab and bisphosphonates: different mechanisms of action and effects. Bone. 2011;48:677. doi: 10.1016/j.bone.2010.11.020. [DOI] [PubMed] [Google Scholar]
- 15.Lacey DL, Boyle WJ, Simonet WS, Kostenuik PJ, Dougall WC, Sullivan JK, San Martin J, Dansey R. Bench to bedside: elucidation of the OPG-RANK-RANKL pathway and the development of denosumab. Nat Rev Drug Discov. 2012;11:401. doi: 10.1038/nrd3705. [DOI] [PubMed] [Google Scholar]
- 16.Aghaloo TL, Felsenfeld AL, Tetradis S. Osteonecrosis of the jaw in a patient on Denosumab. J Oral Maxillofac Surg. 2010;68:959. doi: 10.1016/j.joms.2009.10.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fedele S, Porter SR, D’Aiuto F, Aljohani S, Vescovi P, Manfredi M, Arduino PG, Broccoletti R, Musciotto A, Di Fede O, Lazarovici TS, Campisi G, Yarom N. Nonexposed variant of bisphosphonate-associated osteonecrosis of the jaw: a case series. Am J Med. 2010;123:1060. doi: 10.1016/j.amjmed.2010.04.033. [DOI] [PubMed] [Google Scholar]
- 18.Hutchinson M, O’Ryan F, Chavez V, Lathon PV, Sanchez G, Hatcher DC, Indresano AT, Lo JC. Radiographic findings in bisphosphonate-treated patients with stage 0 disease in the absence of bone exposure. J Oral Maxillofac Surg. 2010;68:2232. doi: 10.1016/j.joms.2010.05.003. [DOI] [PubMed] [Google Scholar]
- 19.Neuprez A, Coste S, Rompen E, Crielaard JM, Reginster JY. Osteonecrosis of the jaw in a male osteoporotic patient treated with denosumab. Osteoporos Int. 2013 doi: 10.1007/s00198-013-2437-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dranitsaris G, Hatzimichael E. Interpreting results from oncology clinical trials: a comparison of denosumab to zoledronic acid for the prevention of skeletal-related events in cancer patients. Support Care Cancer. 2012;20:1353. doi: 10.1007/s00520-012-1461-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Fizazi K, Carducci M, Smith M, Damiao R, Brown J, Karsh L, Milecki P, Shore N, Rader M, Wang H, Jiang Q, Tadros S, Dansey R, Goessl C. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: a randomised, double-blind study. Lancet. 2011;377:813. doi: 10.1016/S0140-6736(10)62344-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Saad F, Brown JE, Van Poznak C, Ibrahim T, Stemmer SM, Stopeck AT, Diel IJ, Takahashi S, Shore N, Henry DH, Barrios CH, Facon T, Senecal F, Fizazi K, Zhou L, Daniels A, Carriere P, Dansey R. Incidence, risk factors, and outcomes of osteonecrosis of the jaw: integrated analysis from three blinded active-controlled phase III trials in cancer patients with bone metastases. Ann Oncol. 2012;23:1341. doi: 10.1093/annonc/mdr435. [DOI] [PubMed] [Google Scholar]
- 23.Smith MR, Saad F, Coleman R, Shore N, Fizazi K, Tombal B, Miller K, Sieber P, Karsh L, Damiao R, Tammela TL, Egerdie B, Van Poppel H, Chin J, Morote J, Gomez-Veiga F, Borkowski T, Ye Z, Kupic A, Dansey R, Goessl C. Denosumab and bone-metastasis-free survival in men with castration-resistant prostate cancer: results of a phase 3, randomised, placebo-controlled trial. Lancet. 2012;379:39. doi: 10.1016/S0140-6736(11)61226-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Patel S, Choyee S, Uyanne J, Nguyen AL, Lee P, Sedghizadeh PP, Kumar SK, Lytle J, Shi S, Le AD. Non-exposed bisphosphonate-related osteonecrosis of the jaw: a critical assessment of current definition, staging, and treatment guidelines. Oral Dis. 2012;18:625. doi: 10.1111/j.1601-0825.2012.01911.x. [DOI] [PubMed] [Google Scholar]
- 25.Junquera L, Gallego L. Nonexposed bisphosphonate-related osteonecrosis of the jaws: another clinical variant? J Oral Maxillofac Surg. 2008;66:1516. doi: 10.1016/j.joms.2008.02.012. [DOI] [PubMed] [Google Scholar]
- 26.Diniz-Freitas M, Lopez-Cedrun JL, Fernandez-Sanroman J, Garcia-Garcia A, Fernandez-Feijoo J, Diz-Dios P. Oral bisphosphonate-related osteonecrosis of the jaws: Clinical characteristics of a series of 20 cases in Spain. Med Oral Patol Oral Cir Bucal. 2012;17:e751. doi: 10.4317/medoral.18041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lazarovici TS, Yahalom R, Taicher S, Elad S, Hardan I, Yarom N. Bisphosphonate-related osteonecrosis of the jaws: a single-center study of 101 patients. J Oral Maxillofac Surg. 2009;67:850. doi: 10.1016/j.joms.2008.11.015. [DOI] [PubMed] [Google Scholar]
- 28.Mawardi H, Treister N, Richardson P, Anderson K, Munshi N, Faiella RA, Woo SB. Sinus tracts--an early sign of bisphosphonate-associated osteonecrosis of the jaws? J Oral Maxillofac Surg. 2009;67:593. doi: 10.1016/j.joms.2008.09.031. [DOI] [PubMed] [Google Scholar]
- 29.Fusco V, Galassi C, Berruti A, Ciuffreda L, Ortega C, Ciccone G, Angeli A, Bertetto O. Osteonecrosis of the jaw after zoledronic acid and denosumab treatment. J Clin Oncol. 2011;29:e521. doi: 10.1200/JCO.2011.35.1551. [DOI] [PubMed] [Google Scholar]
- 30.Arce K, Assael LA, Weissman JL, Markiewicz MR. Imaging findings in bisphosphonate-related osteonecrosis of jaws. J Oral Maxillofac Surg. 2009;67:75. doi: 10.1016/j.joms.2008.12.002. [DOI] [PubMed] [Google Scholar]
- 31.Bianchi SD, Scoletta M, Cassione FB, Migliaretti G, Mozzati M. Computerized tomographic findings in bisphosphonate-associated osteonecrosis of the jaw in patients with cancer. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:249. doi: 10.1016/j.tripleo.2007.01.040. [DOI] [PubMed] [Google Scholar]
- 32.Cho YA, Yoon HJ, Lee JI, Hong SP, Hong SD. Histopathological features of bisphosphonate-associated osteonecrosis: findings in patients treated with partial mandibulectomies. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114:785. doi: 10.1016/j.oooo.2012.08.457. [DOI] [PubMed] [Google Scholar]
- 33.Hansen T, Kunkel M, Weber A, James Kirkpatrick C. Osteonecrosis of the jaws in patients treated with bisphosphonates - histomorphologic analysis in comparison with infected osteoradionecrosis. J Oral Pathol Med. 2006;35:155. doi: 10.1111/j.1600-0714.2006.00391.x. [DOI] [PubMed] [Google Scholar]
- 34.Marx RE, Tursun R. Suppurative osteomyelitis, bisphosphonate induced osteonecrosis, osteoradionecrosis: a blinded histopathologic comparison and its implications for the mechanism of each disease. Int J Oral Maxillofac Surg. 2012;41:283. doi: 10.1016/j.ijom.2011.12.016. [DOI] [PubMed] [Google Scholar]
- 35.Paparella ML, Brandizzi D, Santini-Araujo E, Cabrini RL. Histopathological features of osteonecrosis of the jaw associated with bisphosphonates. Histopathology. 2012;60:514. doi: 10.1111/j.1365-2559.2011.04061.x. [DOI] [PubMed] [Google Scholar]
- 36.Aghaloo TL, Kang B, Sung EC, Shoff M, Ronconi M, Gotcher JE, Bezouglaia O, Dry SM, Tetradis S. Periodontal disease and bisphosphonates induce osteonecrosis of the jaws in the rat. J Bone Miner Res. 2011;26:1871. doi: 10.1002/jbmr.379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Aguirre JI, Akhter MP, Kimmel DB, Pingel JE, Williams A, Jorgensen M, Kesavalu L, Wronski TJ. Oncologic doses of zoledronic acid induce osteonecrosis of the jaw-like lesions in rice rats (Oryzomys palustris) with periodontitis. J Bone Miner Res. 2012;27:2130. doi: 10.1002/jbmr.1669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Ali-Erdem M, Burak-Cankaya A, Cemil-Isler S, Demircan S, Soluk M, Kasapoglu C, Korhan-Oral C. Extraction socket healing in rats treated with bisphosphonate: animal model for bisphosphonate related osteonecrosis of jaws in multiple myeloma patients. Med Oral Patol Oral Cir Bucal. 2011;16:e879. doi: 10.4317/medoral.17150. [DOI] [PubMed] [Google Scholar]
- 39.Bi Y, Gao Y, Ehirchiou D, Cao C, Kikuiri T, Le A, Shi S, Zhang L. Bisphosphonates cause osteonecrosis of the jaw-like disease in mice. Am J Pathol. 2010;177:280. doi: 10.2353/ajpath.2010.090592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Gotcher JE, Jee WS. The progress of the periodontal syndrome in the rice cat. II. The effects of a diphosphonate on the periodontium. J Periodontal Res. 1981;16:441. doi: 10.1111/j.1600-0765.1981.tb00995.x. [DOI] [PubMed] [Google Scholar]
- 41.Kang B, Cheong S, Chaichanasakul T, Bezouglaia O, Atti E, Dry SM, Pirih FQ, Aghaloo TL, Tetradis S. Periapical disease and bisphosphonates induce osteonecrosis of the jaws in mice. J Bone Miner Res. 2013;28:1631. doi: 10.1002/jbmr.1894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Pautke C, Kreutzer K, Weitz J, Knodler M, Munzel D, Wexel G, Otto S, Hapfelmeier A, Sturzenbaum S, Tischer T. Bisphosphonate related osteonecrosis of the jaw: A minipig large animal model. Bone. 2012;51:592. doi: 10.1016/j.bone.2012.04.020. [DOI] [PubMed] [Google Scholar]
- 43.Sonis ST, Watkins BA, Lyng GD, Lerman MA, Anderson KC. Bony changes in the jaws of rats treated with zoledronic acid and dexamethasone before dental extractions mimic bisphosphonate-related osteonecrosis in cancer patients. Oral Oncol. 2009;45:164. doi: 10.1016/j.oraloncology.2008.04.013. [DOI] [PubMed] [Google Scholar]
- 44.Kikuiri T, Kim I, Yamaza T, Akiyama K, Zhang Q, Li Y, Chen C, Chen W, Wang S, Le AD, Shi S. Cell-based immunotherapy with mesenchymal stem cells cures bisphosphonate-related osteonecrosis of the jaw-like disease in mice. J Bone Miner Res. 2010;25:1668. doi: 10.1002/jbmr.37. [DOI] [PMC free article] [PubMed] [Google Scholar]