

Abstract
Introduction. Noncontrast head CT (NCCT) is the standard radiologic test for patients presenting with acute stroke. Early ischemic changes (EIC) are often overlooked on initial NCCT. We determine the sensitivity and specificity of improved EIC detection by a standardized method of image evaluation (Stroke Windows). Methods. We performed a retrospective chart review to identify patients with acute ischemic stroke who had NCCT at presentation. EIC was defined by the presence of hyperdense MCA/basilar artery sign; sulcal effacement; basal ganglia/subcortical hypodensity; and loss of cortical gray-white differentiation. NCCT was reviewed with standard window settings and with specialized Stroke Windows. Results. Fifty patients (42% females, 58% males) with a mean NIHSS of 13.4 were identified. EIC was detected in 9 patients with standard windows, while EIC was detected using Stroke Windows in 35 patients (18% versus 70%; P < 0.0001). Hyperdense MCA sign was the most commonly reported EIC; it was better detected with Stroke Windows (14% and 36%; P < 0.0198). Detection of the remaining EIC also improved with Stroke Windows (6% and 46%; P < 0.0001). Conclusions. Detection of EIC has important implications in diagnosis and treatment of acute ischemic stroke. Utilization of Stroke Windows significantly improved detection of EIC.
1. Introduction
Noncontrast head CT (NCCT) is the first-line diagnostic test for emergency evaluation of acute stroke due to its speed of imaging, widespread availability, and low cost. The window width and center level settings—measured in Hounsfield units: HUs—used for computed tomographic (CT) scan review are known to influence both lesion conspicuity and diagnostic accuracy [1]. Numerous studies suggest that detection of early ischemic change (EIC) on NCCT can predict both functional outcome and the risk of intracranial hemorrhage (ICH) [2–4].
Specific features relevant to stroke assessment include hyperdense middle cerebral artery (MCA)/basilar signs, focal parenchymal hypoattenuation (notably of the insular ribbon or lenticular nuclei for MCA infarcts), and cerebral swelling manifested by sulcal or ventricular effacement or loss of cortical grey-white differentiation [5–7]. Decreases in CT attenuation accompanying early stroke are small; therefore, their conspicuity may be increased by using narrow window settings centered at approximately the mean attenuation in HUs of gray and white matter. We believe that the increase in lesion conspicuity achieved with this method can improve the accuracy of nonenhanced CT stroke detection [1]. In most academic stroke centers, on-call residents, radiologists, and ED physicians are the first providers to interpret NCCT in the setting of suspected acute ischemic stroke. We hypothesize that detection of EIC can be improved by a standardized method of image evaluation that can be implemented by the treating physicians (including trainees).
2. Materials and Methods
2.1. Study Description
A retrospective chart review of the University of Tennessee Health Science Center prospective database of acute ischemic stroke from January 2012 to July 2012 was performed. A total of 50 patients with NIH Stroke Scores (NIHSS) greater than 4 were identified who underwent NCCT within 4.5 hours of symptom onset. NCCT with significant motion artifacts and patients with NIHSS less than or equal to 4 were excluded from the study. Nonenhanced CT scanning was performed with a CT HiSpeed Advantage 16 slice scanner (GE Medical Systems, Milwaukee, WI) in the hospital emergency department using the nonhelical scanning technique: 120 KV, 300 mA, 1-second scanning time, and 5 mm section thickness.
At the time of image interpretation, the neurology resident was blinded to all patient information except for the reason of obtaining NCCT (which, in most cases, was the presenting complaint) in order to make the image comparable to the information available to the interpreting radiologists. Images were reviewed at a PACS workstation. Patients' name, sex, and date of birth were visible on the PACS screen (by default) to both the senior resident and the interpreting radiologist.
NCCTs were evaluated for evidence of EIC, which was defined by the presence of one or more of the following findings [5–7]: (1) hyperdense MCA/basilar artery sign; (2) sulcal effacement; (3) basal ganglia/subcortical hypodensity; and (4) loss of cortical gray-white differentiation. Images were first reviewed at the standard settings of 35 HU center and 100 HU width level. Following this, window settings were adjusted to width of 30 HU and center level of 35 HU, which was designated as Stroke Windows. Final interpretation of images was made by neurology resident based on the findings noted on Stroke Windows.
For each patient, the resident's final interpretation using Stroke Windows was compared with the final staff radiologist's report. Accuracy of diagnosis and identification of stroke mimics was then confirmed by review of the final discharge diagnosis. Correlative modalities used to determine the accuracy of EICs included follow-up NCCT and MRI. Statistical analysis was performed using Fisher's exact score.
2.2. Standard Protocol Approvals, Registrations, and Patient Consents
This study was approved by the IRB as the part of the University of Tennessee Health Sciences Center's Acute Ischemic Stroke Registry.
3. Results
A total of 50 patients were identified; 21 patients were females (42%) with a mean age of 75.4 years; the NIHSS ranged from 5 to 27 with a mean of 13.4. Mean time to CT from symptom onset was 97.7 minutes. Thirty-nine patients had large vessel anterior circulation stroke; 3 patients had posterior circulation stroke; 7 patients had lacunar stroke; 1 patient had no stroke on follow-up imaging. The detection of EICs with Stroke Windows was significantly higher: 70% (35 out of 50 patients) compared to 18% (9 out of 50 patients) in the standard window group (P < 0.0001). Rate of detection of individual components of EIC is depicted in Table 1.
Table 1.
Comparison of the number of detected EICs (N = 50).
| EIC | Number of resident-detected EICsa | Number of staff radiologist-detected EICsb | Significance |
|---|---|---|---|
| Hyperdense MCA sign | 18 (36%) | 7 (14%) | P < 0.0198 |
| Hyperdense basilar sign | 1 (2%) | 0 (0%) | P < 1.0 |
| Sulcal effacement | 7 (14%) | 0 (0%) | P < 0.0125 |
| Basil ganglia hypodensity | 7 (14%) | 2 (4%) | P < 0.15 |
| Loss of grey-white differentiation | 10 (20%) | 2 (4%) | P < 0.027 |
aEIC detected with author-established Stroke Window settings.
bEIC detected with standard windows settings.
Hyperdense MCA sign was seen in 18 patients using Stroke Windows, whereas only 7 radiology reports mentioned hyperdense MCA sign (36% versus 14%; P < 0.0198). Hyperdense basilar sign was seen in 1 patient using Stroke Windows, whereas the final radiology report detected none (P < 1.0). Similarly, sulcal effacement was seen in 7 patients by the resident using Stroke Windows, whereas none were reported in the final radiology report (P < 0.0125). Basal ganglia hypodensity was reported in 7 patients by the resident and in 2 patients' final reports (14% versus 4%; P < 0.15). Finally, loss of grey-white differentiation was graded in 10 patients by the resident and in 2 patients by the staff radiologist (20% versus 4%; P < 0.027). Figure 1 illustrates representative cases demonstrating how standard Stroke Windows may increase the diagnostic yield of NCCT in the setting of acute ischemic stroke. Chart review demonstrated a 100% correlation between both the resident and radiologists' interpretation with the final discharge diagnosis.
Figure 1.
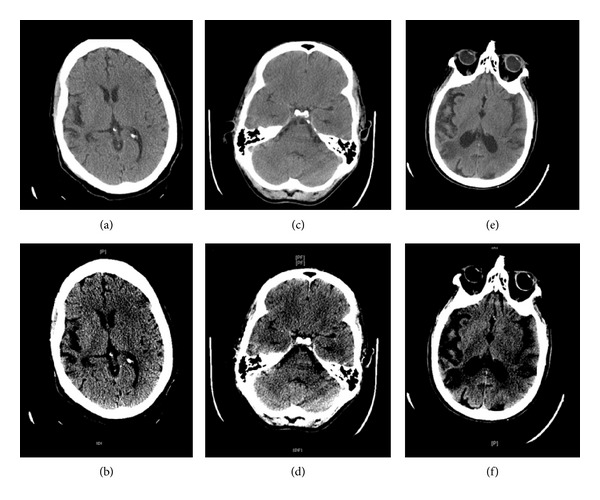
Noncontrast head CTs (NCCTs). (a) NCCT of head viewed on standard windows (35/100). (b) NCCT of head viewed on Stroke Windows (35/30) demonstrating left sulcal effacement of the insular ribbon and hypodensity of left basal ganglia. (c) NCCT of head viewed on standard windows (35/100). (d) NCCT of head viewed on Stroke Windows (35/30) demonstrating right MCA sign. (e) NCCT of head viewed on standard windows (35/100). (f) NCCT of head viewed on Stroke Windows (35/30) demonstrating hypodensity of left basal ganglia.
4. Discussion
NCCT is recommended by the American Heart Association as the initial modality of choice for stroke investigation [8] because of its accessibility, speed, and patient tolerance, thereby permitting the rapid triage of patients suspected of having experienced a stroke. Several studies have shown an association between baseline infarct size and final infarct volume, clinical outcome, and hemorrhagic transformation risk when using intravenous thrombolysis with tissue plasminogen activator and/or intra-arterial stroke interventions [2, 9, 10]. Additionally, studies suggest that hypoattenuation on CT is highly specific for irreversible ischemic brain damage if detection occurs within the first 6 hours. Patients without hypoattenuating brain tissue have a more favorable clinical course [11]. The absence of an identifiable infarct on initial imaging does not preclude stroke treatment in the appropriate clinical context; however, visualization of infarct confirms the clinical diagnosis and allows for a more nuanced treatment decision regarding thrombolysis and endovascular intervention to be made on the basis of the size and severity of infarct on presentation [11, 12].
In this study, we have demonstrated that the detection of EIC by NCCT is significantly improved by utilization of standard Stroke Windows and can be easily utilized by the initial providers assessing acute stroke, including the trainees. This has important implications concerning the delivery of acute stroke care, especially considering that residents are often the first clinicians to see these patients and that the majority of acute stroke thrombolysis in the United States is delivered at academic institutions [13].
This study has several important limitations. First, this is a single center study with a single neurology resident performing image interpretation. Secondly, the patients do not represent a random population, rather a group of individuals with known history of stroke or acute stroke; therefore, the blinding of the resident reviewer was not complete. This introduces bias which may have resulted in the resident reporting more positive findings than the staff radiologist. Additionally, we did not limit our study to specific vascular distribution and included all patients with NIHSS > 4, including stroke mimics (1 patient had no stroke at the time of discharge). Also, the NCCT interpretation by the senior resident using standard windows was not compared with the staff radiologists' interpretation at the same window settings to establish user-dependent variability in image interpretation. We know from previously well-established studies that the total time taken for image interpretation is an important factor in detection of EIC [14]. Our study did not take CT scan reading time into consideration. Finally, not all interpreting radiologists were subspecialty trained in Neuroradiology, which may have contributed to low rates of EIC detection but may also represent a real-world setting in regard to the radiology workforce that interprets the bulk of acute ischemic stroke CTs [15].
5. Conclusion
Despite some limitations, the rate of detection of EIC significantly improved with the use of Stroke Windows in the authors' experience. Further randomized studies using Stroke Windows may help in establishing a gold standard for CT interpretation in the setting of acute ischemic stroke. At this time, based on our single center experience, the authors would recommend the use of Stroke Windows by neurology trainees, stroke neurologists, radiologists, and ED physicians to improve the detection of EIC in the setting of acute ischemic stroke.
Disclosure
This was a retrospective chart review of a prospective database of University of Tennessee Health Science Center; no funding was received for this study.
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
Authors' Contribution
Drs. Mainali and Elijovich participated in design or conceptualization of this study, analysis or interpretation of the data, and drafting or revising of the paper for intellectual content. Dr. Wahba participated in drafting or revising of the paper for intellectual content. Shraddha Mainali, M.D., provided statistical analysis via Fisher's exact test for this paper.
References
- 1.Lev MH, Farkas J, Gemmete JJ, et al. Acute stroke: improved nonenhanced CT detection—benefits of soft-copy interpretation by using variable window width and center level settings. Radiology. 1999;213(1):150–155. doi: 10.1148/radiology.213.1.r99oc10150. [DOI] [PubMed] [Google Scholar]
- 2.Tanne D, Kasner SE, Demchuk AM, et al. Markers of increased risk of intracerebral hemorrhage after intravenous recombinant tissue plasminogen activator therapy for acute ischemic stroke in clinical practice: the multicenter rt-PA acute stroke survey. Circulation. 2002;105(14):1679–1685. doi: 10.1161/01.cir.0000012747.53592.6a. [DOI] [PubMed] [Google Scholar]
- 3.Derex L, Nighoghossian N. Intracerebral haemorrhage after thrombolysis for acute ischaemic stroke: an update. Journal of Neurology, Neurosurgery and Psychiatry. 2008;79(10):1093–1099. doi: 10.1136/jnnp.2007.133371. [DOI] [PubMed] [Google Scholar]
- 4.Barber PA, Demchuk AM, Zhang J, Buchan AM. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. The Lancet. 2000;355(9216):1670–1674. doi: 10.1016/s0140-6736(00)02237-6. [DOI] [PubMed] [Google Scholar]
- 5.Truwit CL, Barkovich AJ, Gean-Marton A, Hibri N, Norman D. Loss of the insular ribbon: another early CT sign of acute middle cerebral artery infarction. Radiology. 1990;176(3):801–806. doi: 10.1148/radiology.176.3.2389039. [DOI] [PubMed] [Google Scholar]
- 6.Tomura N, Uemura K, Inugami A, Fujita H, Higano S, Shishido F. Early CT finding in cerebral infarction: obscuration of the lentiform nucleus. Radiology. 1988;168(2):463–467. doi: 10.1148/radiology.168.2.3393665. [DOI] [PubMed] [Google Scholar]
- 7.Moulin T, Cattin F, Crépin-Leblond T, et al. Early CT signs in acute middle cerebral artery infarction: predictive value for subsequent infarct locations and outcome. Neurology. 1996;47(2):366–375. doi: 10.1212/wnl.47.2.366. [DOI] [PubMed] [Google Scholar]
- 8.Adams HP, Jr., del Zoppo G, Alberts MJ, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke. 2007;38:1655–1711. doi: 10.1161/STROKEAHA.107.181486. [DOI] [PubMed] [Google Scholar]
- 9.Hacke W, Kaste M, Fieschi C, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II) The Lancet. 1998;352(9136):1245–1251. doi: 10.1016/s0140-6736(98)08020-9. [DOI] [PubMed] [Google Scholar]
- 10.Hacke W, Kaste M, Fieschi C, et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke: the European Cooperative Acute Stroke Study (ECASS) Journal of the American Medical Association. 1995;274(13):1017–1025. [PubMed] [Google Scholar]
- 11.von Kummer R, Bourquain H, Bastianello S, et al. Early prediction of irreversible brain damage after ischemic stroke at CT. Radiology. 2001;219(1):95–100. doi: 10.1148/radiology.219.1.r01ap0695. [DOI] [PubMed] [Google Scholar]
- 12.von Kummer R. Early major ischemic changes on computed tomography should preclude use of tissue plasminogen activator. Stroke. 2003;34(3):820–821. doi: 10.1161/01.STR.0000059430.55671.56. [DOI] [PubMed] [Google Scholar]
- 13.Schumacher HC, Bateman BT, Boden-Albala B, et al. Use of thrombolysis in acute ischemic stroke: analysis of the Nationwide Inpatient Sample 1999 to 2004. Annals of Emergency Medicine. 2007;50(2):99–107. doi: 10.1016/j.annemergmed.2007.01.021. [DOI] [PubMed] [Google Scholar]
- 14.Wardlaw JM, Farrall AJ, Perry D, et al. Factors influencing the detection of early CT signs of cerebral ischemia: an internet-based, international multiobserver study. Stroke. 2007;38(4):1250–1256. doi: 10.1161/01.STR.0000259715.53166.25. [DOI] [PubMed] [Google Scholar]
- 15.Erly WK, Ashdown BC, Lucio RW, II, Carmody RF, Seeger JF, Alcala JN. Evaluation of emergency CT scans of the head: is there a community standard? American Journal of Roentgenology. 2003;180(6):1727–1730. doi: 10.2214/ajr.180.6.1801727. [DOI] [PubMed] [Google Scholar]