

Abstract
Introduction:
Vitamin D deficiency is expected to be higher in patients with diabetes and pulmonary tuberculosis (TB). Studies estimating prevalence in the subset of patients with both diabetes and pulmonary TB are scarce.
Materials and Methods:
A total of 155 subjects were recruited; 46 patients with type 2 diabetes, 39 non-diabetic healthy controls, 30 patients of pulmonary TB and 40 patients with both pulmonary TB and type 2 diabetes. Vitamin D level (25 OH vitamin D) levels were done for all the 4 groups.
Results:
Mean vitamin D levels were not different between groups with TB, diabetes mellitus or combination of both, but the prevalence of severe vitamin D deficiency was higher in the group with both diabetes and TB (45%) as compared with the group with only TB (26.66%) and diabetes (17.39%) and healthy controls (7.69%).
Conclusion:
The prevalence of patients with severe vitamin D deficiency is higher in patients with dual affection of TB and diabetes mellitus as compared with either disorder alone implying that patients with type 2 diabetes with the most severe vitamin D deficiency are the one of the most predisposed to pulmonary TB.
Keywords: Diabetes, pulmonary tuberculosis, vitamin D deficiency
INTRODUCTION
India has the largest diabetic population, with about 61.3 million patients and expected to increase to 101.2 million by 2030.[1] As per World Health Organization estimate, India (1.98 million) and China (1.3 million) constitute 35% of tuberculosis (TB) cases world-wide. India has 0.87 million infectious cases and stands at fifth position of the global burden of TB.[2] Diabetes mellitus and TB are two diverse epidemics of different etio-pathogenesis that have grown exponentially in developing countries like India in recent times and not only have they grown simultaneously, but also merged imperceptibly into one another. Although of different etiology there are many possible linking features and vitamin D deficiency is one such link between the two.[3] The rising prevalence of vitamin D deficiency makes these 3 disorders commonly co existent in a single patient. The prevalence of vitamin D in type 2 diabetics is expected to be high. Furthermore in chronic diseases like TB the prevalence of vitamin D deficiency is expected to be high.
In this observational study, we wish to study the vitamin D status of patients with both TB and type 2 diabetes and compare it to patients with only diabetes, only TB and healthy volunteers.
MATERIALS AND METHODS
Patients
The study was conducted at Sir Sunder Lal Hospital, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India. Patients were recruited from endocrinology outdoors and pulmonary medicine outdoors.
Patients with either type 2 diabetes or newly diagnosed treatment naïve pulmonary TB (sputum positive on two early morning samples) or both the disorders together were screened for exclusion criteria. Healthy controls were the family members of these patients. Diabetes was diagnosed by American diabetes association criteria or by past history and records. Patients with drug resistant TB or extra pulmonary TB were excluded. Patients with significant renal, cardiac disease or respiratory diseases other than TB were excluded. Pregnant and lactating mothers and seriously ill-patients were also excluded. Use of any drug that interferes with vitamin D metabolism including alcohol, vitamin supplements, calcium preparations or steroids were excluded from the study. The study protocol was approved by the institutional ethics committee. All patients gave an informed written consent for participation in this study.
Methods
A total of 170 subjects were screened out of which 155 subjects were recruited; 46 patients with type 2 diabetes, 39 non-diabetic healthy controls, 30 patients of pulmonary TB and 40 patients with both pulmonary TB and type 2 diabetes.
Clinical anthropometric examination and fasting and post prandial plasma glucose, along with vitamin D level (25 OH vitamin D) levels were done for all the four groups.
Laboratory analysis
Serum 25 OH vitamin D was measured by radioimmunoassay using Diasorin kit as per manufacturer's protocol. All the tests were run in triplicates and tubes were counted for 60 s. The mean of the three readings was taken to plot the graph and calculate the concentration of samples. Intra-assay and inter-assay coefficient of variation were 11.7 and 12.5%, respectively.
Statistics
All quantitative data was reported as mean ± standard deviation. Comparisons between the four groups were performed by one-way analysis of variance (ANOVA). Rates and proportions compared using Chi-square test. Intra group comparison in ANOVA was performed by Holm Sidak method.
RESULTS
A total of 170 patients were screened of which 155 qualified for the study, which were divided into four groups with an intension to determine the vitamin D status of patient of T2DM with pulmonary Koch's with other three groups serving as the control. There was no significant difference between the four groups. There was no difference in terms of age between healthy, only diabetes and diabetes with pulmonary Koch's, however patients with pulmonary Koch's were younger than other groups. Mean vitamin D level of all the groups was < 30 ng/dl. Healthy subjects were having a higher mean vitamin D level than the other groups. However, there was no difference between diabetic group, pulmonary Koch's group and diabetic patients with pulmonary Koch's group in terms of vitamin D level [Table 1]. Sub group analysis of the severity of vitamin D level between the groups were done by dividing vitamin D into 3 sub-groups, >30 ng/dl, 20-30 ng/dl, 10-20 ng/dl and <10 ng/dl [Table 2]. Incidence of vitamin D deficiency was 61.5% among healthy individuals, 87.5% among T2DM with pulmonary Koch's, 80.5% among patients with only diabetes and 93.4% among patients with only pulmonary Koch's group. Interestingly, we also found the 45% of patients with T2DM with pulmonary Koch's, 26.6% diabetics, 17.39% with only pulmonary Koch's and 7.69% healthy subjects were having severe vitamin D deficiency defined as vitamin D level below 10 ng/dl [Table 2] suggesting patients having double disease were more severely affected [Figure 1].
Table 1.
Age, Sex and Vitamin D status of the study group and Control groups

Table 2.
Comparison of severity of vitamin D deficiency between groups

Figure 1.
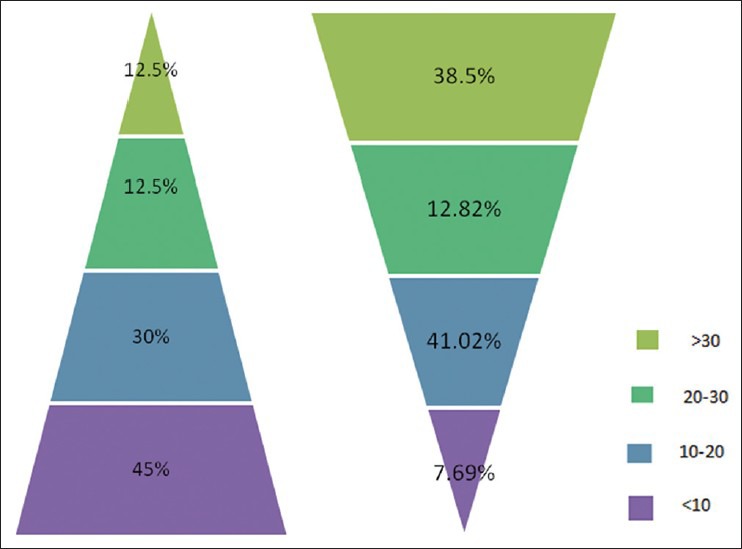
Pulmonary tuberculosis with type 2 diabetes and healthy control
DISCUSSION
The vitamin D endocrine system is an essential component of the interactions among the kidney, bone, parathyroid gland and intestine that maintain extracellular calcium levels within narrow limits, a process vital for normal cellular physiology and skeletal integrity.
The prevalence of vitamin D deficiency is very high in Indian population as shown by various studies several studies have shown that in North India 96% of neonates,[4] 91% of healthy school girls,[5] 78% of healthy hospital staff and[6] 84% of pregnant woman[4] were found to have hypovitaminosis using criteria of defining 25 (OH) vitamin D deficient as serum level below 20 ng/ml. In South India, hypovitaminosis D is equally prevalent among different population groups as shown by Harinarayan et al.[7,8,9]
Serum concentrations of 25-OH vitamin D in patients presenting with TB are on average lower than in healthy matched controls and the prevalence of TB is higher among those with low serum 25-OH vitamin D concentrations such as elderly subjects and Asian immigrants to the UK.[10] Incidence of pulmonary TB is 2-3 higher in diabetic patients.[11] It can be attributable to vitamin D deficiency. There is good evidence to suggest that fall in serum vitamin D levels compromises cell mediated immunity and leads to activation of latent TB.[12]
In our study, 94.33% patients with pulmonary Koch's were vitamin D deficient/insufficient. Our results were similar to the various studies showing the presence of 25 (OH) vitamin D deficiency in pulmonary Koch's as compared with the healthy individuals shown by Davies et al., Kenya (P < 0.05),[13] Davies et al., Thailand (P < 0.001);[14] Chan et al., Hong Kong;[15] Sasidharan et al., India (P < 0.005).[16]
Nearly 46.66% patients with diabetes plus pulmonary Koch's group were having vitamin D level <10 ng/ml, which may suggest that patients with diabetes mellitus and severe vitamin D deficiency are more susceptible to develop tubercular infection than those having normal or low vitamin D status.
Considering recent upcoming role of vitamin D as an immune-modulator and its potential role in treatment of pulmonary TB in the literature; we can conclude that although we cannot go for vitamin D estimation in every patient, but can supplement vitamin D in those who are at high risk of having vitamin D deficiency and this may be of some therapeutic benefit with regards to treatment of TB and even glycemic control.
This study is limited by its small size, recruitment at a single institution.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Geneva: World Health Organization; 2009. World Health Organization. Global Tuberculosis Control: a Short Update to the 2009 Report. [Google Scholar]
- 2.Grad R. Cod and the consumptive: A brief history of cod-liver oil in the treatment of pulmonary tuberculosis. Pharm Hist. 2004;46:106–20. [PubMed] [Google Scholar]
- 3.Handel AE, Ramagopalan SV. Tuberculosis and diabetes mellitus: Is vitamin D the missing link? Lancet Infect Dis. 2010;10:596. doi: 10.1016/S1473-3099(10)70185-7. [DOI] [PubMed] [Google Scholar]
- 4.Sachan A, Gupta R, Das V, Agarwal A, Awasthi PK, Bhatia V. High prevalence of vitamin D deficiency among pregnant women and their newborns in Northern India. Am J Clin Nutr. 2005;81:1060–4. doi: 10.1093/ajcn/81.5.1060. [DOI] [PubMed] [Google Scholar]
- 5.Puri S, Marwaha RK, Agarwal N, Tandon N, Agarwal R, Grewal K, et al. Vitamin D status of apparently healthy schoolgirls from two different socioeconomic strata in Delhi: Relation to nutrition and lifestyle. Br J Nutr. 2008;99:876–82. doi: 10.1017/S0007114507831758. [DOI] [PubMed] [Google Scholar]
- 6.Arya V, Bhambri R, Godbole MM, Mithal A. Vitamin D status and its relationship with bone mineral density in healthy Asian Indians. Osteoporos Int. 2004;15:56–61. doi: 10.1007/s00198-003-1491-3. [DOI] [PubMed] [Google Scholar]
- 7.Harinarayan CV, Ramalakshmi T, Prasad UV, Sudhakar D, Srinivasarao PV, Sarma KV, et al. High prevalence of low dietary calcium, high phytate consumption, and vitamin D deficiency in healthy South Indians. Am J Clin Nutr. 2007;85:1062–7. doi: 10.1093/ajcn/85.4.1062. [DOI] [PubMed] [Google Scholar]
- 8.Harinarayan CV. Prevalence of vitamin D insufficiency in postmenopausal South Indian women. Osteoporos Int. 2005;16:397–402. doi: 10.1007/s00198-004-1703-5. [DOI] [PubMed] [Google Scholar]
- 9.Harinarayan CV, Ramalakshmi T, Prasad UV, Sudhakar D. Vitamin D status in Andhra Pradesh: A population based study. Indian J Med Res. 2008;127:211–8. [PubMed] [Google Scholar]
- 10.Martineau AR, Wilkinson RJ, Wilkinson KA, Newton SM, Kampmann B, Hall BM, et al. A single dose of vitamin D enhances immunity to mycobacteria. Am J Respir Crit Care Med. 2007;176:208–13. doi: 10.1164/rccm.200701-007OC. [DOI] [PubMed] [Google Scholar]
- 11.Jeon CY, Murray MB. Diabetes mellitus increases the risk of active tuberculosis: A systematic review of 13 observational studies. PLoS Med. 2008;5:e152. doi: 10.1371/journal.pmed.0050152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Restrepo BI. Convergence of the tuberculosis and diabetes epidemics: Renewal of old acquaintances. Clin Infect Dis. 2007;45:436–8. doi: 10.1086/519939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Davies PD, Church HA, Brown RC, Woodhead JS. Raised serum calcium in tuberculosis patients in Africa. Eur J Respir Dis. 1987;71:341–4. [PubMed] [Google Scholar]
- 14.Davies PD, Church HA, Bovornkitti S, Charumilind A, Byrachandra S. Altered vitamin D homeostasis in tuberculosis. Int Med Thailand. 1988;4:45–7. [Google Scholar]
- 15.Chan TY, Poon P, Pang J, Swaminathan R, Chan CH, Nisar M, et al. A study of calcium and vitamin D metabolism in Chinese patients with pulmonary tuberculosis. J Trop Med Hyg. 1994;97:26–30. [PubMed] [Google Scholar]
- 16.Sasidharan PK, Rajeev E, Vijayakumari V. Tuberculosis and vitamin D deficiency. J Assoc Physicians India. 2002;50:554–8. [PubMed] [Google Scholar]