

Abstract
Background
Many underage drinkers obtain alcohol from legal-age family, friends, and acquaintances. This study aimed to understand the attitudes and behaviors of young adults related to providing alcohol to underage drinkers.
Methods
Participants were 755 current or recent college students of legal drinking age (ages 22 to 26) who were approached by a minor to provide alcohol at least once since turning 21. Interviewers assessed frequency of providing alcohol, relationship to the recipients, and general attitudes about providing alcohol to minors. Separate questions asked about younger (under 18) and older (18 to 20) minors. Correlates and predictors of provision and frequency of provision were examined via logistic regression and Poisson regression, focusing on demographics, sensation-seeking, behavioral dysregulation, age at first drink, parental history of alcohol problems, fraternity/sorority involvement, attitudes about provision, violations, peer drinking norms, and alcohol use disorder (AUD) risk during and post-college.
Results
Most participants (84.6%) provided alcohol to minors at least once. Provision to older minors was more prevalent (82.8%) than to younger minors (20.7%); it was also more frequent. Few (2.4%) were ever caught providing alcohol. Recipients were more commonly friends or family members rather than acquaintances or strangers. Legal concerns about providing alcohol (82.5% and 53.7% for younger and older minors, respectively) were more prevalent than health concerns (55.7% and 9.5%). Legal concerns consistently predicted lower likelihood of provision, independent of demographics. Health concerns and lower post-college AUD risk scores also independently predicted lower likelihood of provision, but only to older minors. Fraternity/sorority involvement and higher peer drinking norms were associated with higher provision frequency, whereas legal concerns and college violations were associated with lower provision frequency.
Conclusions
Young adults who have recently turned 21 could represent an important target for prevention strategies to reduce underage drinking on college campuses. More research is needed to understand the motivations of young adults who provide alcohol to underage drinkers.
Keywords: alcohol, provision to minors, underage drinking, young adults
INTRODUCTION
Since the U.S. implemented the National Minimum Drinking Age Act of 1984, all states have adopted a minimum legal drinking age of 21 for the purposes of purchase and public possession. However, underage drinking continues to be a serious public health problem in the U.S. Results from the 2012 National Survey on Drug Use and Health estimate that among 12- to 20-year-olds, 9.3 million (24.3%) were past-month users of alcohol, and 5.9 million (15.3%) engaged in heavy episodic drinking [five or more drinks on the same occasion; Substance Abuse and Mental Health Services Administration, 2013; (SAMHSA)]. Furthermore, most people who tried alcohol for the first time were younger than 21 (79.3%), and many were younger than 18 (53.3%; SAMHSA, 2013).
The public health consequences of underage drinking are numerous and well-documented. First, the acute consequences of alcohol use include academic problems, injuries and hospitalization, risky sexual behavior or sexual assault, and harm to others (Committee on Developing a Strategy to Reduce and Prevent Underage Drinking, 2004; Hingson and White, 2014; Kim et al., 2012; Miller et al., 2007; Mouilso et al., 2012). Second, earlier age at onset of drinking predicts a greater risk for alcohol use disorders (Arria, 2008; Hingson et al., 2006; King and Chassin, 2007; Pitkanen et al., 2005). Third, underage drinking results in DUI crashes and deaths. Annually, approximately 5,000 people under age 21 die from injuries related to alcohol use, including 1,900 deaths from motor vehicle crashes (U.S. Department of Health and Human Services, 2007). Moreover, drinking alcohol before the brain is fully developed (i.e., before age 25) can raise the risk for neurocognitive impairment (Bava and Tapert, 2010; De Bellis et al., 2000; Hanson et al., 2011; Silveri, 2012).
One major driver of underage drinking is the widespread availability of alcohol. In 2012, the majority of twelfth graders (90.6%) and tenth graders (78.2%) had either “fairly easy” or “very easy” access to alcohol (Johnston et al., 2013). While little research has focused on how underage drinkers obtain their alcohol, friends who are of legal drinking age are one of the most common sources for both high school students and 18- to 20-year-olds (SAMHSA, 2013; Williams and Mulhall, 2005).
Underage college students are an important prevention target for several reasons. Problem drinking is more prevalent among college students than their non-college attending peers (SAMHSA, 2013), likely due in part to environmental factors such as a campus culture that perceives underage drinking as normative. On residential campuses, students are typically free of adult supervision, and underage students mingle closely with legal-age peers (i.e., 21 and older), which facilitates their access to alcohol.
Two qualitative studies have shed light on the importance of social connections as a means of obtaining alcohol for underage college students. In one study utilizing focus groups, the majority of underage participants cited “social access,” a network of friends and acquaintances, as the easiest source for obtaining alcohol (Fabian et al., 2008). In a second qualitative study of legal-age drinkers ages 21 to 25 on a Midwestern college campus, provision of alcohol to underage students was an integral part of the drinking culture; almost all participants had provided or were willing to provide alcohol illegally to their underage peers (Brown et al., 2009). Furthermore, most participants denied moral responsibility for any negative consequences—either health, social, or academic—that recipients might experience. Rather, they attributed full responsibility to the recipient, whom they regarded as an “adult” expected to make his or her own decisions regarding alcohol (Brown et al., 2009).
Limited evidence suggests that the likelihood of providing alcohol to an underage drinker might depend on age and gender. In a “shoulder tapping” experiment in which actors who appeared to be 18 to 20 years old asked adult patrons entering liquor or convenience stores to purchase alcohol for them, only 8% of patrons complied with the actor’s request. However, the corresponding proportion was 19% for young male patrons (i.e., apparent ages 21 to 30; Toomey et al., 2007). Little or no research has examined other factors that might be related to provision. Problem behavior theory would support the hypothesis that individual propensity for risk-taking behavior (e.g., as manifested by violations, sensation-seeking, and behavioral dysregulation characteristics as measured in the present study) might be related to providing alcohol to a minor. Moreover, regular involvement in social organizations such as fraternities or sororities might increase opportunities for providing alcohol to minors.
The purpose of this research was to fill gaps in the literature about the prevalence and predictors of provision of alcohol to minors, especially among college students who have recently turned 21. Specifically, the study aimed to: 1) describe the attitudes and behaviors of a sample of young adults regarding provision of alcohol to minors; 2) examine how the frequency of providing alcohol varies by the provider’s relationship to the recipient; and 3) examine factors associated with likelihood and frequency of provision, including demographics, drinking behaviors, personality factors, and attitudes about provision.
MATERIALS AND METHODS
Design
Data were derived from the College Life Study, a longitudinal prospective study of 1,253 young adults who were originally recruited as incoming first-year students (ages 17 to 19) at one large public university in the mid-Atlantic region of the U.S. Most of the incoming first-year class completed a brief pre-college online survey during summer orientation (n=3,401; 88.7% response rate). Individuals who used an illicit drug at least once during high school were oversampled for the longitudinal study, beginning with a baseline assessment (two-hour personal interview and self-administered questionnaires) administered during their freshman year (i.e., Year 1; n=1,253; 86.5% response rate). Similar assessments were administered annually even after departure from college, with high follow-up rates (Year 2=91.1%; Year 7=78.4%). Interviewers were trained extensively in human subjects protection. Cash incentives were provided. The study was approved by the university’s IRB and a federal Certificate of Confidentiality was obtained. Additional sampling and recruitment information is available elsewhere (Arria et al., 2008; Vincent et al., 2012).
Participants
The sample for the present analysis was restricted to 755 individuals who reported in Years 6 and/or 7 (modal ages 23 to 24) that they had been approached for alcohol by a minor at least once since they turned 21 and had consumed alcohol at least once in their lifetime by Year 7. The vast majority of the inclusion sample (96.7%) completed both assessments (i.e., Years 6 and 7); 50.9% were still in school in Years 6 and/or 7. Compared with the inclusion sample, the 239 individuals who were excluded due to non-response in Years 6 or 7 were more likely to be male (62.3% vs. 48.9%, p<.001), but were similar with respect to race/ethnicity and socioeconomic status (as measured by neighborhood income and mother’s education). The 258 individuals who were excluded due to never having been asked by a minor to provide alcohol were significantly more likely to be female (65.5% vs. 51.1%, p<.001), identify as a racial/ethnic minority (33.3% vs. 26.9%, p=.048), and have a less educated mother (i.e., 31.8% vs. 24.0% lacking a bachelor’s degree, p=.018), as compared with the inclusion sample, and were less likely to meet DSM-IV criteria for alcohol use disorder in Years 6 or 7 (43.8% vs. 63.4%, p<.001). However, they were similar with respect to neighborhood income. One additional individual was excluded due to never having consumed alcohol.
Measures
Provision of Alcohol to Minors
In Years 6 and 7, participants were asked how many times they provided alcohol to someone who was not of legal drinking age, with separate questions for providing to minors in two age groups: “someone under 18 years old” and “someone 18 to 20 years old”. Participants were instructed to consider times when they bought the alcohol as well as times they served their own alcohol to someone under 21, “like at a party.” To avoid temporal overlap, the Year 6 questions referenced the entire time since they turned 21, and the Year 7 questions referred to the past 12 months. All participants were at least 22 years old by Year 6 (age 22=3%, age 23=73%, age 24=23%, and age 25<1%). To calculate the cumulative sample prevalence of providing alcohol, responses were later dichotomized as either never or one or more times. Frequency of provision among those who provided was calculated as the sum of responses between Years 6 and 7. In the few cases (3.3%) where one assessment was missing, the frequency value reflects the response from whichever assessment was available.
Two additional sets of questions were asked for individuals who provided alcohol to minors at least once. First, to understand the nature of the relationships between providers and recipients, participants were asked how often they provided alcohol to family members, friends, acquaintances, strangers, and others (“never”, “once or twice”, “sometimes”, or “regularly”). Responses from both years were later combined in order to describe provision patterns cumulatively, using the higher frequency in cases where responses differed over time. Because only four individuals provided to an “other” person, this group is not shown in the results. Second, participants were asked whether they had ever been caught for providing alcohol to minors and, if yes, by whom (police, sellers, their parents, parents of the minor, or someone else). Multiple responses were permitted.
Attitudes Regarding Provision
In Year 6 participants were asked, “What is your personal opinion about someone your age providing alcohol for someone who is under 18?” followed by “What about providing it for someone who is 18 to 20 years old?” Response options for both items were: “It’s not a problem”, “Shouldn’t do it for health reasons”, “Shouldn’t do it for legal reasons”, or “Shouldn’t do it for both health and legal reasons.” Four dichotomous variables were later derived representing health concerns (yes, no) and legal concerns (yes, no) separately for recipients in both age groups.
Age at First Drink and Alcohol Use Disorders (AUD)
Age at onset of drinking (i.e., the first time they tried alcohol) was initially captured at baseline and supplemented thereafter with age at assessment for the few individuals whose onset occurred sometime after baseline. All annual assessments included a series of questions adapted from the National Survey on Drug Use and Health (SAMHSA, 2003) to identify AUD (abuse and dependence), as defined by DSM-IV criteria (American Psychiatric Association, 1994). Individuals who used alcohol fewer than five times during the past year skipped out of this series of questions and were coded as not having a disorder. For each year, an AUD risk “score” was coded as follows: 0=Did not drink during the past year, 1=Drank fewer than five times during the past year, 2=Drank five or more times during the past year but endorsed no DSM-IV criteria, 3=Diagnostic orphans (endorsed one or two criteria but not meeting the definition of abuse or dependence), 4=Abuse, 5=Dependence. For the present analyses, we consolidated the seven annual AUD variables into two variables representing the maximum AUD risk score during college (Years 1 through 4) and post-college (Years 6 and 7).
Peer Drinking Norms
During Years 2 through 4, participants were asked “How many alcoholic drinks, would you say, does the average (male/female) fourth-year student at [this university] drink on a typical Saturday? (Include the whole day and night.)” Responses were later averaged across Years 2 through 4 for each individual to represent their peer drinking norms during college.
Violations during College
Annually in Years 1 through 4, participants were asked about three different types of violations they might have received during the past 12 months: housing violation due to alcohol use, citation for alcohol use, and being arrested. Arrests were not necessarily related to alcohol, but of the 45 arrested participants, 14 voluntarily mentioned an alcohol-related reason for their arrest (e.g., drunk driving, underage drinking). An index (count) of the total number of types of violations they experienced (0 to 3) was later computed to represent the degree of college violations. Of the three violations in this index, housing violations were the most prevalent (26%), followed by citations (20%) and arrests (6%); overall 37% experienced at least one of the three violations.
Impulsive Sensation-Seeking and Behavioral Dysregulation
At baseline, participants self-administered the Zuckerman-Kuhlman Personality Questionnaire (ZKPQ) Short Form and the Dysregulation Inventory, both of which have good psychometric properties among college students and correlate with heavy drinking and other high-risk behaviors (Mezzich et al., 2001; Zuckerman, 2002). For the present analyses, we used the seven-item impulsive sensation-seeking subscale (α=0.74) from the ZKPQ and the 34-item behavioral dysregulation subscale (α=0.89) of the Dysregulation Inventory (Mezzich et al., 2001). For both subscales, higher scores denote higher levels of the characteristic.
Parental History of Alcohol Problems
Parental history of alcohol problems was assessed in Year 2 with a family tree questionnaire (Mann et al., 1985) in which participants were asked to characterize their biological mother and father as never using alcohol, using without problems, using with possible problems, or using with definite problems. Responses were later dichotomized as no problems (0) and possible or definite problems (1), due to the small number endorsing “definite” problems (2% for mothers, 7% for fathers). “Don’t know” responses (3% for mothers, 4% for fathers), were coded as missing.
Demographic Characteristics
Sex was recorded as observed at baseline. Race was self-reported in Year 3 and later dichotomized to non-Hispanic white versus all others, a category which included participants who identified as Hispanic, Black, Asian, or any other identity; this was due to the preponderance of non-Hispanic whites in the sample (73.1%). As a proxy for socioeconomic status, mother’s education level was self-reported at college entry and later dichotomized to Bachelor’s degree or higher and less than a Bachelor’s degree. Fraternity or sorority affiliation was captured in Years 2 through 4, and later dichotomized cumulatively as any involvement (regular or irregular) versus none.
Analytic Strategy
Analyses proceeded in three stages. First, descriptive statistics were tabulated, and comparisons between participants who did and did not provide alcohol were evaluated with ANOVA (continuous variables) or Chi-square tests (categorical variables), with α=.05. Second, predictors for the likelihood of provision were analyzed in a series of multivariable logistic regression models with provision to younger minors under 18 (yes vs. no) and older minors ages 18 to 20 (yes vs. no) as dichotomous dependent variables. Hypothesized predictors were all entered simultaneously, and subsequently subjected to a stepwise selection procedure in which non-significant variables (p≥.05) were excluded from the model and then re-entered one at a time (setting α=.05), in order to obtain a more parsimonious model that was more likely to give rise to the data (Draper and Smith, 1966). Sex, race/ethnicity, and mother’s education were retained regardless of statistical significance. Third, due to the high sample prevalence of provision to older minors, we evaluated the predictors of the frequency of provision in a Poisson regression model under the assumption that the frequency, as a count variable, followed a Poisson distribution in the population using a similar effect selection procedure while retaining demographic variables in the model. Missing data were minimal (<9% for any given variable) and were imputed for the Poisson regression analysis using EM estimation (Schafer and Graham, 2002). Descriptive and logistic regression analyses were performed in SPSS 19; imputation and Poisson regression were performed in SAS 9.3.
RESULTS
As mentioned earlier, only participants who had been approached for alcohol by a minor were included in the analytic sample. Twice as many participants were approached by older minors (n=710) as by younger minors (n=360). Among those approached by older minors, the vast majority (86.9%) chose to provide alcohol at least once, whereas the corresponding proportion was much lower among participants approached by younger minors (39.2%). In the overall sample, 84.6% provided alcohol to someone under 21 at least once: 82.8% to older minors and 20.7% to younger minors. Alcohol provision was also much less frequent for younger than older minors—in addition to being less prevalent. Figure 1 depicts the frequency of providing alcohol, by age of recipient, among those who ever provided. Provision to younger minors typically occurred no more than five times, but more frequent patterns of provision were apparent in relation to older minors, with half providing more than five times.
Fig 1.
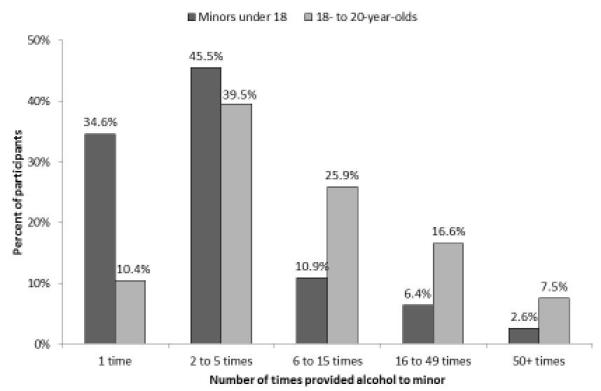
Frequency of providing alcohol to minors (% of sample), by age of the recipient, among individuals who ever provided to 18- to 20-year-olds (n=625) and minors under 18 (n=156).
As illustrated in Figure 2, most participants provided alcohol to underage friends (66%) and family members (52%); those who provided to acquaintances (21%) or strangers (4%) were in the minority. With respect to more frequent patterns of provision, 29.4% provided alcohol “sometimes” or “regularly” to an underage family member, and 38.6% provided “sometimes” or “regularly” to a friend.
Fig 2.
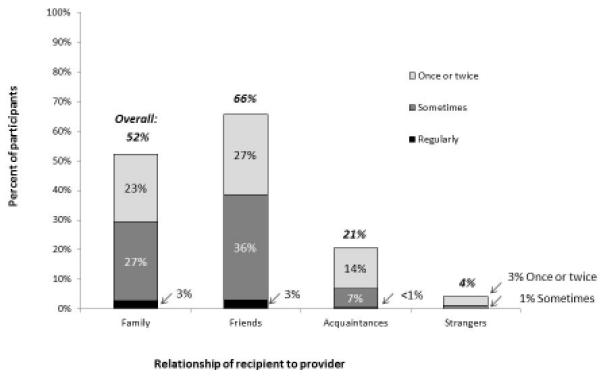
Frequency of providing alcohol to minors (% of sample), by relationship to recipient, among individuals who provided alcohol to a minor at least once (n=639).
Of the 639 individuals who ever provided alcohol to minors, only 15 (2.4%) were ever caught for doing so. Most were caught by their parents or the parents of the minor (n=10). A few were caught by other relatives (n=1), servers/sellers (n=1), the police (n=2), or campus police (n=1).
Table 1 presents results pertaining to the comparisons between individuals who did and did not provide alcohol to minors. In general, compared with non-providers, individuals who provided alcohol were more likely to be male and had more permissive attitudes about providing alcohol to minors, regardless of the recipient minor’s age group. They also tended to have more severe levels of alcohol involvement as measured by younger age at onset of drinking, greater likelihood of meeting criteria for AUD, and higher AUD scores, although these comparisons were not always statistically significant for both age groups of recipient minors. Accordingly, providers also tended to score higher on sensation-seeking and behavioral dysregulation and had more violations during college, relative to non-providers, although, again, comparisons were not always statistically significant for both age groups. Importantly, Greek affiliation was not related to likelihood of provision to either age group, and although whites were slightly overrepresented among both groups of providers, this difference was only significant for provision to older minors.
Table 1.
Results of Comparisons between Participants Who Did and Did Not Provide Alcohol to Minors Under 18 and Ages 18 to 20, Respectively (n=755)
| Comparison 1: Provided to Minors Under 18 |
Comparison 2: Provided to Minors 18 to 20 |
||||
|---|---|---|---|---|---|
| Total (n=755) |
Yes (n=156) |
No (n=599) |
Yes (n=625) |
No (n=130) |
|
| % (n) | % (n) | % (n) | % (n) | % (n) | |
|
|
|
|
|||
| Sex (% Female) | 386 (51.1) | 41.0 ( 64) | 53.8 (322)* | 49.0 (306) | 61.5 ( 80)** |
| Race/ethnicity (% Non-Hispanic White) | 552 (73.1) | 76.9 (120) | 72.1 (432) | 75.7 (473) | 60.8 ( 79)*** |
| Mother’s education (% Bachelor’s degree or higher) |
536 (76.0) | 81.6 (120) | 74.5 (415) | 77.0 (453) | 70.7 ( 82) |
| Greek affiliation (% Yes) | 260 (34.4) | 34.6 ( 54) | 34.4 (206) | 35.5 (222) | 29.2 ( 38) |
| Attitudes about providing alcohol to minors under 18 |
|||||
| % Legal concerns | 618 (82.5) | 73.1 (114) | 85.0 (504)*** | -- | -- |
| % Health concerns | 417 (55.7) | 44.2 ( 69) | 58.7 (348)*** | -- | -- |
| Attitudes about providing alcohol to minors ages 18 to 20 |
|||||
| % Legal concerns | 402 (53.7) | -- | -- | 47.8 (297) | 82.0 (105)*** |
| % Health concerns | 71 ( 9.5) | -- | -- | 5.8 ( 36) | 27.3 ( 35)*** |
| Parental history of alcohol problems (% possible/ definite) |
|||||
| Maternal | 44 ( 6.3) | 6.4 ( 9) | 6.3 ( 35) | 6.4 ( 37) | 5.8 ( 7) |
| Paternal | 114 (16.4) | 15.5 ( 22) | 16.7 ( 92) | 16.8 ( 97) | 14.5 ( 17) |
| AUD during collegea | |||||
| % Alcohol abuse | 267 (35.4) | 35.3 ( 55) | 35.4 (212) | 37.4 (234) | 25.4 ( 33)** |
| % Alcohol dependence | 258 (34.2) | 39.1 ( 61) | 32.9 (197) | 34.4 (215) | 33.1 ( 43) |
| AUD post-collegea | |||||
| % Alcohol abuse | 424 (56.2) | 57.1 ( 89) | 55.9 (335) | 57.9 (362) | 47.7 ( 62)* |
| % Alcohol dependence | 55 ( 7.3) | 9.0 ( 14) | 6.8 ( 41) | 8.2 ( 51) | 3.1 ( 4)* |
|
M (SD) |
M (SD) |
M (SD)
|
M (SD) |
M (SD)
|
|
| Age at first drink | 14.9 ( 2.5) | 14.4 ( 2.4) | 15.0 ( 2.5)** | 14.9 ( 2.5) | 14.9 ( 2.5) |
| Sensation-seeking | 3.7 ( 2.2) | 4.1 ( 2.2) | 3.6 ( 2.1)** | 3.7 ( 2.1) | 3.5 ( 2.2) |
| Behavioral dysregulation | 28.5 (11.7) | 29.8 (12.1) | 28.2 (11.6) | 28.9 (11.7) | 26.5 (11.6)* |
| Peer drinking normsb | 6.5 ( 2.4) | 6.9 ( 2.4) | 6.5 ( 2.4) | 6.6 ( 2.5) | 6.3 ( 2.3) |
| Violations during college (index) | 0.5 (0.8) | 0.6 ( 0.8) | 0.5 ( 0.7)* | 0.5 ( 0.8) | 0.4 ( 0.7) |
| AUD during college (score)a | 3.9 ( 1.0) | 4.1 ( 0.9) | 3.9 ( 1.0)* | 4.0 ( 0.9) | 3.6 ( 1.3)*** |
| AUD post-college (score)a | 3.4 ( 1.0) | 3.5 ( 1.0) | 3.4 ( 1.0) | 3.5 ( 1.0) | 3.1 ( 1.2)*** |
| Number of times provided alcohol to minors under 18 |
1.2 ( 4.8) | 5.6 ( 9.3) | -- | -- | -- |
| Number of times provided alcohol to minors ages 18 to 20 |
14.1 (36.1) | -- | -- | 17.1 (39.0) | -- |
Note. Missing data were imputed. The number of cases with missing data was <9% for any given variable, and was greatest for father’s and mother’s history of alcohol problems (n=58 and 55, respectively). Results of dichotomous comparisons between individuals who did and did not provide alcohol to minors in each age group are based on chi-square tests of independence and oneway ANOVAs for categorical and scale variables, respectively, and denoted as follows:
p<.05;
p<.01;
p<.001.
Maximum AUD scores for college (Years 1 through 4) and post-college (Years 6 and 7), respectively.
The number of drinks consumed on a typical Saturday by a typical student of the same age, sex, and year at the same college.
With respect to attitudes about provision among the sample, legal concerns were considerably more prevalent than health concerns for both age groups (82.5% vs. 55.7%, respectively, for younger minors, and 53.7% vs. 9.5% for older minors). Interestingly, attitudes were less accepting in relation to younger minors than older minors, especially regarding health concerns (55.7% vs. 9.5%).
When hypothesized predictors of provision were evaluated simultaneously in a logistic regression model (Table 2), only male gender and legal concerns remained significantly associated with provision recipients under 18. For provision to older minors, the reduced model retained four significant predictors: race/ethnicity, legal concerns, health concerns, and post-college AUD score.
Table 2.
Results of Multivariable Logistic Regression Models Predicting Provision of Alcohol to Minors Under 18 (n=360) and Ages 18 to 20 (n=710)
| Provision to Minors Under 18 | Provision to Minors Ages 18 to 20 | |||
|---|---|---|---|---|
| Full Model | Reduced Model | Full Model | Reduced Model | |
| AOR (95% CI) | AOR (95% CI) | AOR (95% CI) | AOR (95% CI) | |
| Demographics | ||||
| Sex=Male | 1.98 (1.04, 3.76)* | 1.91 (1.23, 2.95)** | 0.75 (0.46, 1.23) | 0.76 (0.46, 1.24) |
| Race/ethnicity=Non-Hispanic White | 1.52 (0.73, 3.19) | 1.22 (0.74, 2.02) | 1.86 (1.14, 3.01)* | 1.85 (1.14, 3.02)* |
| Mother’s education=Bachelor’s degree or higher | 1.29 (0.62, 2.68) | 1.38 (0.81, 2.34) | 1.19 (0.71, 1.99) | 1.16 (0.69, 1.95) |
| Pre-college predictors | ||||
| Sensation-seeking | 1.08 (0.93, 1.26) | 0.92 (0.82, 1.04) | ||
| Behavioral dysregulation | 0.99 (0.97, 1.02) | 1.00 (0.98, 1.02) | ||
| Age at first drink | 0.94 (0.82, 1.08) | 1.04 (0.95, 1.15) | ||
| Maternal alcohol problems (Ref.= No problems) | 0.71 (0.21, 2.41) | 1.81 (0.52, 6.27) | ||
| Paternal alcohol problems (Ref.=No problems) | 0.67 (0.31, 1.46) | 1.38 (0.7, 2.74) | ||
| College predictors | ||||
| Greek affiliation (Ref.=No affiliation) | 0.88 (0.47, 1.66) | 1.27 (0.78, 2.08) | ||
| Legal concerns (Ref.=No legal concerns) | 0.46 (0.23, 0.94)* | 0.40 (0.24, 0.69)** | 0.29 (0.17, 0.50)** | 0.24 (0.13, 0.43)** |
| Health concerns (Ref.=No health concerns) | 0.7 (0.38, 1.29) | 0.70 (0.38, 1.29)** | 0.22 (0.12, 0.39)** | |
| Violations during college | 0.97 (0.64, 1.48) | 0.97 (0.64, 1.48) | ||
| Peer drinking norms | 1.03 (0.90, 1.17) | 1.03 (0.90, 1.17) | ||
| AUD during college (score)a | 0.98 (0.69, 1.4) | 0.98 (0.69, 1.40) | ||
| Post-college predictors | ||||
| AUD post-college (score)a | 0.97 (0.71, 1.33) | 0.97 (0.71, 1.33) | 1.28 (1.03, 1.60)* | |
p<0.05;
p<0.01
Maximum AUD scores for college (Years 1 through 4) and post-college (Years 6 and 7), respectively.
With respect to the Poisson regression on frequency of provision to minors ages 18 to 20 (see Table 3 and Figure 3), individuals with legal concerns about provision tended to provide alcohol less often than those without legal concerns. However, no corresponding decrease in risk was seen for health concerns (unlike in the earlier logistic model predicting provision in this age group). Similar to the logistic models described above, males and whites tended to provide alcohol more frequently than their counterparts (see Figure 3). But unlike in the previous models, three college variables emerged as independent predictors of provision frequency: Greek affiliation, peer drinking norms, and violations. Individuals who perceived their peers as drinking more heavily and had been affiliated with a fraternity or sorority had a subsequent tendency—two to three years post-college—to provide alcohol to minors more frequently than their counterparts. On the other hand, the number of college violations was negatively associated with the frequency of provision.
Table 3.
Results of Poisson Regression Predicting Frequency of Provision of Alcohol to Minors Ages 18 to 20 (n=710)
| Full model b (SE) |
Reduced model b (SE) |
|
|---|---|---|
| Demographics | ||
| Sex=Male | 0.53 (0.16)** | 0.50 (0.16)* |
| Race=Non-Hispanic White | 0.46 (0.18)* | 0.50 (0.18)* |
| Mother’s education=Bachelor’s degree or higher | −0.11 (0.16) | −0.09 (0.16) |
| Pre-college predictors | ||
| Behavioral dysregulation | −0.01 (0.01)* | |
| Age at first drink | −0.01 (0.03) | |
| No maternal alcohol problems (Ref.=Problems) | −0.07 (0.25) | |
| No paternal alcohol problems (Ref.=Problems) | −0.15 (0.17) | |
| Sensation-seeking | 0.03 (0.03) | |
| College predictors | ||
| Greek affiliation (Ref.=No affiliation) | 0.40 (0.13)* | 0.44 (0.13)* |
| Legal concerns (Ref.=No legal concerns) | −0.73 (0.15)** | −0.72 (0.15)** |
| Health concerns (Ref.=No health concerns) | −0.31 (0.35) | |
| Violations during college | −0.24 (0.09)* | −0.19 (0.09)* |
| Peer drinking norms | 0.14 (0.02)** | 0.14 (0.02)** |
| AUD during college (score)a | 0.12 (0.08) | |
| Post-college predictors | ||
| AUD post-college (score)a | −0.24 (0.09) |
p<.05;
p<.001
Note. Full model includes all hypothesized predictors simultaneously as shown. Reduced model includes only those effects that attained statistical significance and retains demographic variables regardless of statistical significance.
Maximum AUD scores for college (Years 1 through 4) and post-college (Years 6 and 7), respectively.
Fig 3.
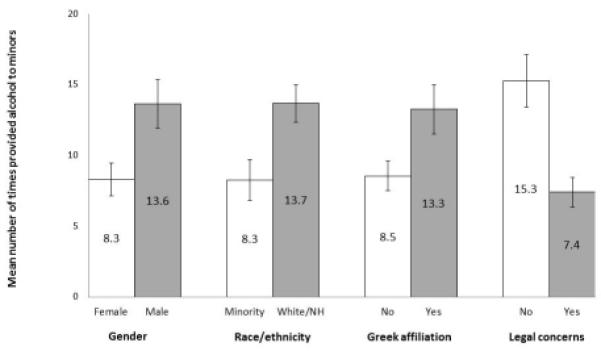
Estimated marginal means with standard error bars for frequency of provision to minors ages 18 to 20 (n=710).
Note. Estimates have been adjusted for all demographic variables shown and violations during college, peer drinking norms, and mother’s education level. NH=Non-Hispanic.
A consistent finding in both the logistic and Poisson regressions was that none of the pre-college variables (i.e., sensation-seeking, behavioral dysregulation, age at first drink, and parent’s alcohol problems) independently predicted provision or frequency of provision. College AUD also failed to attain statistical significance in any of the models, although post-college AUD did predict provision to older minors.
DISCUSSION
In this sample of post-collegiate young adults who had recently attained legal drinking age (i.e., 21 years old), provision of alcohol to underage recipients was common, although fewer individuals had provided alcohol to younger minors (i.e., under 18) than to older minors (i.e., 18- to 20-year-olds). Results confirm what other researchers have learned in qualitative studies with both underage and legal-age college students, namely that drinking is such an accepted part of the college culture that most legal-age young adults are willing to provide alcohol illegally to their underage peers. Furthermore, in this sample, individuals who provided alcohol to minors tended to have higher levels of alcohol involvement themselves both during and post-college, relative to individuals who did not provide alcohol.
Our findings extend prior evidence from qualitative research that young, white, college-educated men might represent an important target for preventing provision of alcohol to minors. One possibility is that they tend to have more opportunities to provide alcohol, whether for social or economic reasons, although results from one study suggest that opportunity is not the only factor (Toomey et al., 2007). In the present study, concurrent alcohol misuse (as measured by post-college AUD score) was another important predictor of providing alcohol to an older minor. On the other hand, several factors arising during college (Greek affiliation, peer drinking norms, and AUD score) did not independently distinguish providers from non-providers, but did predict more frequent provision. The finding that college violations were negatively associated with frequency of provision is unexpected, because it was originally hypothesized as a proxy for a general propensity for deviance. It is possible that individuals who had received sanctions for violations related to alcohol use during college were more motivated to avoid risking further legal trouble by providing alcohol to minors, yet this was not reflected in the models predicting likelihood of provision. Further study is needed to understand the interrelationships between first-hand experience with alcohol-related sanctions during college and consequent perceived risk of future sanctions—in terms of both susceptibility and severity—that might result from providing alcohol to minors.
Given the cultural expectations of drinking in the context of Greek life, we hypothesized that a participant’s affiliation with a fraternity or sorority would increase likelihood of provision. Previous college student studies have shown that involvement in Greek life is associated with greater alcohol use (Capone et al., 2007; Turrisi et al., 2006; Wechsler et al., 1998; Zakletskaia et al., 2011). Residing in a fraternity or sorority house might make it easier for underage drinkers to access alcohol from legal-age housemates, who in turn might experience pressure to provide alcohol for their younger housemates. Furthermore, younger guests attending fraternity/sorority house parties might not always be identified as being underage. Consistent with that scenario, in the present study, Greek affiliation was positively associated with frequency of provision. Although fraternity and sorority members in our sample were no more likely than non-members to provide alcohol, it is possible that Greek involvement might be a particularly relevant determinant of such provision while the individual is still in college and living in a fraternity/sorority house—where they face nearly constant opportunities to provide alcohol to underage members—whereas opportunities wane after graduation.
One important contribution of this study is the finding that participants were much less likely to acknowledge health risks than legal risks, and although health concerns appeared to weakly deter the likelihood of provision, very few participants (9.5%) acknowledged any health concerns about providing alcohol to older minors. Increasing the perception of health and safety risks such as DWI-related injury, sexual assault, accidents, and alcohol poisoning—and perhaps even neurodevelopmental effects—that could result from providing alcohol to minors might be a promising strategy for discouraging legal-age college students from providing alcohol to their underage peers. Nevertheless, the finding that health concerns were not strong deterrents suggests that other prevention strategies are necessary. It is encouraging that the perception of health risks was more prevalent in relation to younger minors.
Another important finding is that the actual risk of getting caught for providing alcohol to minors was practically non-existent in our sample (2.4%). This might help to explain why legal concerns were not a strong deterrent to provision, in that legal concerns were only slightly (albeit significantly) less prevalent among providers than non-providers. These results highlight an important opportunity to expand enforcement of social host laws. Although we have no information about participants’ whereabouts when they provided alcohol, state law in the home state of the majority of the sample stipulates that furnishing or allowing for underage consumption may result in a fine up to $2,500 for the first offense (except for adults providing alcohol to immediate family members within a private residence). Yet provision to minors typically takes place in private residences, which presents challenges to enforcement. Additionally, many young adults and parents might not be cognizant of these laws. Future research should evaluate the efficacy of parent-focused interventions for raising awareness about social host laws and other aspects of alcohol provision, such as the high prevalence of provision that occurs between legal-age and underage young adults—especially siblings—and the potential for their young-adult child to become legally culpable as a social host. More research is needed to evaluate whether greater enforcement and sanctions on provision could lead to fewer young adults being willing to provide alcohol to minors.
One unexpected finding was that relatively few of the hypothesized predictors we examined were independently associated with provision once demographic factors were taken into account. One possible explanation is that provision of alcohol to minors is so normative and acceptable among college students that there are few meaningful differences between students who do and do not provide. Alternatively, differences in provision might be related to personal factors not measured in this study, such as subjective beliefs about what it means to be an adult (and the privileges thereof), which should be a focus of future research. Another possibility is that differences in provision might be driven chiefly by differences in opportunities to provide alcohol rather than differences in personal characteristics per se. In this study we focused on individuals who were ever asked to provide alcohol, but future research on the predictors of being asked—including environmental factors not measured in this study—might shed additional light on these questions. For example, lower outlet density, more consistent server training, and stricter enforcement of social host laws might decrease the likelihood of being asked to provide alcohol, whereas stricter enforcement of false ID laws might have the unintended consequence of increasing such requests.
Another intriguing finding is the observed association between AUD and provision—but only for post-college AUD and only for older recipients. This finding might be due in part to a relatively large number of individuals who prolonged their engagement with the collegiate social environment well past their fourth year of college, and thereby maintained both heavier drinking patterns and continued opportunities to provide alcohol to older minors. This scenario is plausible given the heterogeneity of enrollment patterns previously observed in this sample, with many students still enrolled six or more years after college entry.
Limitations of this study include self-report measures and limited generalizability, as participants were recruited at one university with a predominantly white, non-Hispanic population. In the absence of corroborating information, we cannot evaluate participants’ ability to accurately estimate and recall the ages of minors to whom they provided alcohol. Although we have no reason to suspect that underreporting occurred, participants’ attitudes about provision suggest that any social desirability bias that might have been operating would likely be a more relevant concern in relation to younger minors than older minors. No information was gathered about the specific contexts in which alcohol was provided. Although our longitudinal design helped establish the temporal order between hypothesized predictors measured during college (Years 1 through 4) and subsequent provision measured two to three years later (Years 6 and 7), we acknowledge the potential for some overlap in actual provision behavior, because most participants had already turned 21 by the Year 4 assessment (e.g., 72.4% were 21, 23.6% were 22).
To our knowledge, this is the first quantitative study to address provision of alcohol to minors, a previously understudied aspect of underage drinking. The study’s longitudinal design is an important strength as it allowed us to examine factors that preceded the act of provision to underage individuals. Additional strengths were high follow-up rates throughout seven annual assessments and the introduction of novel measures assessing provision and attitudes towards provision.
Young adults who have recently turned 21 may represent an important new target for alcohol prevention strategies. First, parents should be more aware of the possibility that their 21 year old child could be a source of alcohol to younger children in the family. Many participants in this study were willing to provide alcohol to a minor if s/he was a family member. Parents should be encouraged to talk to their young-adult children, perhaps on or around their 21st birthday about the health and legal risks of providing alcohol to younger siblings, especially if the younger siblings have passed their 18th birthday. Second, it might be possible to develop effective messaging strategies about the negative effects of provision of alcohol. Educational messages about risks and legal penalties for provision could be disseminated through social media channels popular among young adults. Health care visits offer another opportunity to encourage responsible adult health behaviors and thus messages about provision of alcohol could be given in the context of broader conversations about limiting excessive drinking. In some states, 21 year olds are required to obtain a new driver’s license, which might be yet another opportunity to disseminate educational messages about responsible “adult” behavior and the legal and health risks of providing alcohol to minors. Finally, some interventions to reduce high-risk drinking among young people on their 21st birthday have shown promise (Neighbors et al., 2012) and thus, strategies to discourage provision of alcohol to minors might be modeled after such programs. Research to develop and evaluate new strategies of targeting young adults is warranted because decreasing underage access to alcohol is a critical component of preventing the consequences of underage drinking.
Acknowledgments
The investigators acknowledge funding from the National Institute on Alcohol Abuse and Alcoholism (R03AA019563, Dr. Arria, PI) and the National Institute on Drug Abuse (R01DA014845, Dr. Arria, PI). Special thanks are given to Kaitlin Hippen, the interviewing team, and the participants.
REFERENCES
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders: DSM-IV. 4th ed American Psychiatric Press; Washington, DC: 1994. [Google Scholar]
- Arria AM. Underage drinking and alcohol dependence among college students: An update from the College Life Study. Compass. 2008;2008(2):1–2. [Google Scholar]
- Arria AM, Caldeira KM, O’Grady KE, Vincent KB, Fitzelle DB, Johnson EP, Wish ED. Drug exposure opportunities and use patterns among college students: Results of a longitudinal prospective cohort study. Subst Abus. 2008;29(4):19–38. doi: 10.1080/08897070802418451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bava S, Tapert SF. Adolescent brain development and the risk of alcohol and other drug problems. Neuropsychol Rev. 2010;20(4):398–413. doi: 10.1007/s11065-010-9146-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown RL, Matousek TA, Radue MB. Legal-age students’ provision of alcohol to underage college students: An exploratory study. J Am Coll Health. 2009;57(6):611–618. doi: 10.3200/JACH.57.6.611-618. [DOI] [PubMed] [Google Scholar]
- Capone C, Wood MD, Borsari B, Laird RD. Fraternity and sorority involvement, social influences, and alcohol use among college students: A prospective examination. Psychol Addict Behav. 2007;21(3):316–327. doi: 10.1037/0893-164X.21.3.316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Committee on Developing a Strategy to Reduce and Prevent Underage Drinking . Reducing underage drinking: A collective responsiblity. The National Academies Press; Washington, DC: 2004. [Google Scholar]
- De Bellis MD, Clark DB, Beers SR, Soloff PH, Boring AM, Hall J, Kersh A, Keshavan MS. Hippocampal volume in adolescent-onset alcohol use disorders. Am J Psychiatry. 2000;157(5):737–744. doi: 10.1176/appi.ajp.157.5.737. [DOI] [PubMed] [Google Scholar]
- Draper NR, Smith H. Applied regression analysis. John Wiley & Sons; New York, NY: 1966. [Google Scholar]
- Fabian LEA, Toomey TL, Lenk KM, Erickson DJ. Where do underage college students get alcohol? J Drug Educ. 2008;38(1):15–26. doi: 10.2190/DE.38.1.b. [DOI] [PubMed] [Google Scholar]
- Hanson KL, Medina KL, Padula CB, Tapert SF, Brown SA. Impact of adolescent alcohol and drug use on neuropsychological functioning in young adulthood: 10-year outcomes. J Child Adolesc Subst Abuse. 2011;20(2):135–154. doi: 10.1080/1067828X.2011.555272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hingson R, White A. New research findings since the 2007 Surgeon General’s Call to Action to Prevent and Reduce Underage Drinking: A review. J Stud Alcohol Drugs. 2014;75(1):158–169. doi: 10.15288/jsad.2014.75.158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hingson RW, Heeren T, Winter MR. Age at drinking onset and alcohol dependence: Age at onset, duration, and severity. Arch Pediatr Adolesc Med. 2006;160(7):739–746. doi: 10.1001/archpedi.160.7.739. [DOI] [PubMed] [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future: National survey results on drug use, 1975-2012: Volume I: Secondary school students. Institute for Social Research, The University of Michigan; Ann Arbor, MI: 2013. [Google Scholar]
- Kim JY, Asrani SK, Shah ND, Kim WR, Schneekloth TD. Hospitalization for underage drinkers in the United States. J Adolesc Health. 2012;50(6):648–650. doi: 10.1016/j.jadohealth.2011.10.250. [DOI] [PubMed] [Google Scholar]
- King KM, Chassin L. A prospective study of the effects of age of initiation of alcohol and drug use on young adult substance dependence. J Stud Alcohol Drugs. 2007;68(2):256–265. doi: 10.15288/jsad.2007.68.256. [DOI] [PubMed] [Google Scholar]
- Mann RE, Sobell LC, Sobell MB, Pavan D. Reliability of a family tree questionnaire for assessing family history of alcohol problems. Drug Alcohol Depend. 1985;15(1-2):61–67. doi: 10.1016/0376-8716(85)90030-4. [DOI] [PubMed] [Google Scholar]
- Mezzich AC, Tarter RE, Giancola PR, Kirisci L. The dysregulation inventory: A new scale to assess the risk for substance use disorder. J Child Adolesc Subst Abuse. 2001;10(4):35–43. [Google Scholar]
- Miller JW, Naimi TS, Brewer RD, Jones SE. Binge drinking and associated health risk behaviors among high school students. Pediatrics. 2007;119(1):76–85. doi: 10.1542/peds.2006-1517. [DOI] [PubMed] [Google Scholar]
- Mouilso ER, Fischer S, Calhoun KS. A prospective study of sexual assault and alcohol use among first-year college women. Violence Vict. 2012;27(1):78–94. doi: 10.1891/0886-6708.27.1.78. [DOI] [PubMed] [Google Scholar]
- Neighbors C, Lee CM, Atkins DC, Lewis MA, Kaysen D, Mittmann A, Fossos N, Geisner IM, Zheng C, Larimer ME. A randomized controlled trial of event-specific prevention strategies for reducing problematic drinking associated with 21st birthday celebrations. J Consult Clin Psychol. 2012;85(5):850–862. doi: 10.1037/a0029480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pitkanen T, Lyyra AL, Pulkkinen L. Age of onset of drinking and the use of alcohol in adulthood: A follow-up study from age 8-42 for females and males. Addiction. 2005;100(5):652–661. doi: 10.1111/j.1360-0443.2005.01053.x. [DOI] [PubMed] [Google Scholar]
- Schafer JL, Graham JW. Missing data: Our view of the state of the art. Psychol Methods. 2002;7(2):147–177. [PubMed] [Google Scholar]
- Silveri MM. Adolescent brain development and underage drinking in the United States: Identifying risks of alcohol use in college populations. Harv Rev Psychiatry. 2012;20(4):189–200. doi: 10.3109/10673229.2012.714642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Substance Abuse and Mental Health Services Administration . 2002 National Survey on Drug Use and Health Questionnaire. Office of Applied Studies; Rockville, MD: 2003. [Google Scholar]
- Substance Abuse and Mental Health Services Administration . Results from the 2012 National Survey on Drug Use and Health: Detailed tables. United States Department of Health and Human Services, Office of Applied Studies; Rockville, MD: 2013. [Google Scholar]
- Toomey TL, Fabian LE, Erickson DJ, Lenk KM. Propensity for obtaining alcohol through shoulder tapping. Alcohol Clin Exp Res. 2007;31(7):1218–1223. doi: 10.1111/j.1530-0277.2007.00420.x. [DOI] [PubMed] [Google Scholar]
- Turrisi R, Mallett KA, Mastroleo NR, Larimer ME. Heavy drinking in college students: Who is at risk and what is being done about it? J Gen Psychol. 2006;133(4):401–420. doi: 10.3200/GENP.133.4.401-420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services . The Surgeon General’s call to action to prevent and reduce underage drinking. Rockville, MD: 2007. [PubMed] [Google Scholar]
- Vincent KB, Kasperski SJ, Caldeira KM, Garnier-Dykstra LM, Pinchevsky GM, O’Grady KE, Arria AM. Maintaining superior follow-up rates in a longitudinal study: Experiences from the College Life Study. Int J Mult Res Approach. 2012;6(1):56–72. doi: 10.5172/mra.2012.6.1.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wechsler H, Dowdall GW, Maenner G, Gledhill-Hoyt J, Lee H. Changes in binge drinking and related problems among American college students between 1993 and 1997: Results of the Harvard School of Public Health College Alcohol Study. J Am Coll Health. 1998;47(2):57–68. doi: 10.1080/07448489809595621. [DOI] [PubMed] [Google Scholar]
- Williams SS, Mulhall PF. Where public school students in Illinois get cigarettes and alcohol: Characteristics of minors who use different sources. Prev Sci. 2005;6(1):47–57. doi: 10.1007/s11121-005-1252-y. [DOI] [PubMed] [Google Scholar]
- Zakletskaia L, Wilson E, Fleming MF. Alcohol use in students seeking primary care treatment at university health services. J Am Coll Health. 2011;59(3):217–223. doi: 10.1080/07448481.2010.502413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zuckerman M. Zuckerman-Kuhlman Personality Questionnaire (ZKPQ): An alternative five-factorial model. In: de Raad B, Perugini M, editors. Big five assessment. Hogrefe & Huber; Seattle, WA: 2002. pp. 377–396. [Google Scholar]