

Abstract
Objective
The purpose of the present study was to examine readiness to change as a predictor of post-intervention alcohol consumption among Hispanic college student drinkers taking part in a brief harm reduction intervention.
Method
Participants of the intervention study were 109 Hispanic college students residing on the US/Mexico border who self-identified as regular drinkers. This manuscript reports findings from a subset of participants who had complete data at 3-month follow-up (N=84). Participants completed the Readiness to Change Questionnaire, the Rutgers Alcohol Problem Index, and the Form-90 Steady Pattern drinking assessment prior to receiving an intervention.
Results
Hierarchical least-squares regression was used to predict baseline readiness to change scores from alcohol consumption and related consequences, and then to predict 3-month post-intervention drinking from baseline drinking and readiness to change. Alcohol consumption and consequences significantly predicted readiness to change at baseline, and follow-up drinking was significantly predicted from baseline drinking, readiness to change, and an interaction between the two variables. Findings indicated that readiness to change may function differently in people with varying levels of alcohol involvement.
Conclusions
Greater readiness to change predicted reduced alcohol consumption only among the heaviest drinkers; among lighter drinkers, greater readiness to change predicted increased alcohol consumption. Possible explanations for this finding are discussed.
Keywords: Alcohol, Hispanics, College students, Readiness to change
1. Introduction
Excessive alcohol use and binge drinking among college students are both common and dangerous. It is estimated that nearly half of US college students report engaging in binge drinking (defined as consuming five or more standard drinks in one sitting for men and four or more standard drinks for women) within the past two weeks (McNally & Palfai, 2001; Wechsler & Nelson, 2001). The negative consequences associated with binge drinking in this population include health problems, legal problems, academic problems, negative social consequences, unwanted or unsafe sexual experiences, violence and aggression, and accidents/personal injury (Alexander & Bowen, 2004; Blume, Schmaling, & Marlatt, 2003; O’Malley & Johnston, 2002; Park, 2004). Negative consequences related to drinking also have been noted among college students who do not meet the binge criterion, suggesting that consuming less alcohol than the five/four drink binge criterion is not a safe level of drinking for all college students (Caldwell, 2002). Despite the potential harms associated with excessive alcohol consumption, binge drinking remains a common occurrence among college students and has become a national public health concern (Courtney & Polich, 2009; Hingson, Heeren, Winter, & Wechsler, 2005).
1.1. Drinking among Hispanic college students
Hispanics comprise the largest and fastest-growing ethnic minority group in the US, and problem drinking in this population warrants attention from alcohol researchers. People of Hispanic heritage accounted for half of all US population growth between 2000 and 2007, and now comprise 15% of the overall population (Bernstein, 2008). It is expected that the Hispanic population will triple by 2050, and that by mid-century nearly one in three US residents will be Hispanic (Day, 1996). While overall drinking rates of Hispanic college students have been shown to be lower than those of Anglo students (O’Malley & Johnston, 2002), Hispanic students report more binge drinking than students from any other ethnic group (Bennett, Miller, & Woodall, 1999). Also, research has shown that Hispanics who are more acculturated to mainstream US culture experience more severe drinking problems than Hispanics outside of the United States or those with lower levels of acculturation (e.g., Caetano, Ramisetty-Mikler, & McGrath, 2004; Vega & Sribney, 2003). As language and peer groups are typical indicators of acculturation, people of Hispanic ethnicity attending college in the US commonly have relatively high levels of acculturation and, therefore, are at risk for having increased alcohol problems.
Hispanic college students residing on the US/Mexico border are at even greater risk for consequences associated with excessive drinking than college students residing elsewhere in the nation (Lange, Voas, & Johnson, 2002; McKinnon, O’Rourke, & Byrd, 2003; McKinnon, O’Rourke, Thompson, & Berumen, 2004). High school and college students living on the border have reported alcohol consumption rates that are higher than national and state averages (McKinnon et al., 2003; McKinnon et al., 2004). Further, college students residing on the US/Mexico border report consuming more alcohol in Mexico than in the US due to the increased availability of alcohol, the lower minimum drinking age, and the reduced cost of alcohol in Mexico (Clapp, Voas, & Lange, 2001; Lange et al., 2002). One study conducted by the Pacific Institute for Research and Evaluation (as reported in McKinnon et al., 2003) found that 2000 to 3000 young people cross the border from El Paso, TX, to Ciudad Juarez, Mexico, to consume alcohol on a typical weekend night. A survey of drinkers crossing the border back into El Paso found that 40% of those between the ages of 18 and 20 had blood alcohol content (BAC) levels above .08, the legal limit in Texas; of those, 20% reported planning to drive themselves home (McKinnon et al., 2003). Another survey of high school students residing in a US/Mexico border community found that consuming alcohol while in Mexico was significantly associated with binge drinking, drinking and driving, and riding in a car with an intoxicated driver (McKinnon et al., 2004).
1.2. Interventions for college student problem drinkers
Interventions for college student drinkers based on harm reduction may be more effective in achieving desirable outcomes than abstinence-only approaches (Dimeff, Baer, Kivlahan, & Marlatt, 1999; Marlatt & Witkiewitz, 2002). Harm reduction interventions typically aim to guide at-risk drinkers toward changing unsafe drinking patterns in order to avoid negative consequences associated with drinking without requiring abstinence from alcohol (Larimer et al., 1998). College students who engage in problematic drinking are often unaware of the risks associated with their behavior, reporting that they do not believe they are drinking at dangerous levels (Caldwell, 2002). Moreover, college students with significant alcohol problems are often uninterested and unwilling to participate in traditional abstinence-based treatment programs (Marlatt et al., 1998). They frequently report lacking motivation or readiness to change their drinking (Caldwell, 2002). To address the low levels of readiness to change evidenced among college student drinkers, researchers have incorporated motivational enhancement techniques into brief harm reduction interventions tailored to this population, with promising results (e.g., Brief Alcohol Screening and Intervention for College Students; BASICS; Dimeff et al., 1999). Motivational enhancement, based on principles of motivational psychology and grounded in motivational interviewing (Miller & Rollnick, 2002), is intended to promote internal motivation to change (Borsari & Carey, 2000; Murphy et al., 2001). Research supports the implementation of harm reduction and motivational enhancement interventions for college students (and other drinkers) who are not interested in achieving abstinence and who are relatively unmotivated to change (Borsari & Carey, 2000; Marlatt & Witkiewitz, 2002; Marlatt et al., 1998; Walters, Bennett, & Miller, 2000).
1.3. Readiness to change
Drinkers with higher levels of readiness to change may benefit from different intervention strategies than those who are less ready to change (Laudet, 2003; Maisto et al., 2001). One study by Heather, Rollnick, Bell, and Richmond (1996) examined the moderator effect of readiness to change in a brief alcohol intervention study with general hospital patients. They compared a brief motivational intervention with a skills-based counseling intervention and found that intervention type was a significant predictor of alcohol consumption at 6-month follow-up only among patients who were less ready to change—these relatively unmotivated patients evidenced greater decreases in their drinking when they received the motivational intervention. Patients reporting greater readiness to change fared equally well when given the skills-based counseling and motivational interventions (Heather et al., 1996).
Another study of brief interventions for problem drinking among primary care patients found contradictory findings (Maisto et al., 2001). An experiment was conducted to determine whether readiness to change moderated the relationship between type of intervention (standard care, brief advice, or brief motivational) and alcohol consumption at 12-month follow-up. The authors found that the brief advice intervention resulted in decreased alcohol consumption at follow-up for patients who were relatively low in readiness to change compared to those who were higher (Maisto et al., 2001). Readiness to change was unrelated to follow-up drinking for patients in the standard care or brief motivational conditions, however. The authors speculated that the brief advice intervention may have been well matched to those patients low in readiness to change because of its brevity and low intensity. It was concluded that matching brief alcohol interventions to patient characteristics such as readiness to change may be warranted among hospital patients (Maisto et al., 2001). The present study aims to examine the relationship between readiness to change and post-intervention drinking outcomes among college student drinkers.
Harm reduction and motivational enhancement interventions often involve the assessment of readiness to change in order to implement treatment strategies that are appropriate for different levels of readiness (Caldwell, 2002). Some researchers (and instruments) characterize readiness to change in terms of discrete stages. For instance, the Transtheoretical Model of Behavior Change (TTM; Prochaska & DiClemente, 1983) posits that behavior change takes place through a series of stages, and that people become increasingly motivated to change unhealthy behaviors as they progress through the stages. Other researchers characterize readiness to change as a continuum of motivation, ranging from not at all motivated to already having taken steps to change the undesirable behavior (Carey, Purnine, Maisto, & Carey, 1999). Measures of readiness to change often yield subscale scores corresponding to a TTM-defined stage of change (i.e., Precontemplation, Contemplation, Action) as well as an overall score representing the continuous construct of readiness (Carey et al., 1999). The Readiness to Change Questionnaire (RTCQ; Rollnick, Heather, Gold, & Hall, 1992) is one such measure. It has been utilized in research with college student samples to assess motivation to change drinking behavior (e.g., Blume, Marlatt, & Schmaling, 2000; McNally & Palfai, 2001) and has been shown to predict changes in alcohol consumption over time (Heather, Rollnick, & Bell, 1993).
The present study used the RTCQ as a continuous measure of readiness to change among Hispanic college students residing on the US/Mexico border. These students were participants in a culturally-tailored harm reduction intervention for college student drinkers at risk for negative consequences attributable to their drinking. Predictors of readiness to change at baseline were examined, as well as the effect of baseline readiness to change on alcohol consumption at 3-month follow-up while controlling for alcohol consumption at baseline. Also, an analysis was performed to test the interaction between baseline drinking and baseline readiness to change in a regression model predicting post-intervention follow-up drinking. It was hypothesized that greater drinking and greater drinking-related consequences at baseline would significantly predict greater readiness to change one’s drinking; that drinking behavior at baseline would significantly predict drinking behavior at follow-up; and that higher RTCQ scores at baseline would significantly predict relatively lower levels of weekly alcohol consumption during the three months between the baseline and follow-up assessments when controlling for baseline drinking.
2. Method
2.1. Overview of the ASTP study
The data discussed here were gathered during a pilot test of a modified version of the Alcohol Skills Training Program (ASTP), a brief harm reduction intervention developed at the University of Washington for college students who are likely to experience negative consequences due to their drinking behavior (Fromme, Marlatt, Baer, & Kivlahan, 1994). The ASTP was culturally and linguistically tailored for Hispanic college students, and the pilot study involved a comparison of alcohol consumption over time between drinkers who received only the intervention manual and drinkers who received the intervention manual plus two sessions of peer-led alcohol skills training (there was no control condition).
The study’s main findings suggested that both ASTP conditions resulted in significantly (and equally) reduced alcohol consumption among the students, with the greatest change occurring between the baseline and 3-month follow-up assessments (for a complete summary of the intervention study, see Hernandez et al., 2006). In addition to alcohol consumption, participants provided information on alcohol-related consequences and readiness to change. Readiness to change has been shown to predict changes in alcohol consumption in some populations (e.g., male hospital patients; Heather et al., 1993), but this relationship has not been consistently observed in studies with college student samples (Carey, Henson, Carey, & Maisto, 2009). Little is known about readiness to change among Hispanic college student drinkers. The present research involves secondary analysis of the ASTP intervention data for the purpose of understanding the relationships between drinking, alcohol-related consequences, and readiness to change in this population.
2.2. Participants
Participants in the original study included 109 volunteers from introductory psychology classes who received partial course credit for their participation at a Hispanic-serving university on the US/Mexico border. Inclusion criteria included self-identifying as Hispanic and as a “regular drinker,” defined as having consumed alcohol within the previous week. Other research opportunities with comparable course credit were available to students who did not meet these inclusion criteria. Students were excluded from participating if they met criteria for alcohol dependence as determined by prescreening items selected from the Substance Use Disorder Module of the Structured Clinical Interview for the DSM (SCID; Martin, Kaczynski, Maisto, Bukstein, & Moss, 1995). For the present secondary analyses, only data from participants who completed both the baseline and 3-month follow-up assessments were included (N=84). T-tests indicated that there were no differences between study completers and non-completers on demographic or drinking-related variables.
Participants in this sample were mostly male (57.1%) and freshmen or sophomores in college (90.4%). Ages ranged from 18 to 36 (M=20.39, SD=3.06). Mean weekly alcohol consumption was 34.72 (Md=30.40, SD=25.86) standard drinks (defined as 12 ounces of beer, 5 ounces of wine, or 1.5 ounces of spirits). Although men did consume more standard drinks per week than women, the difference in means was not statistically significant; similarly, there were no statistically significant gender differences in readiness to change or consequences at any time point. Of the 84 participants who had complete 3-month follow-up data, 47 (56%) had been assigned to the full ASTP intervention condition and 37 (44%) had been assigned to the manual-only condition. Although all Hispanic participants were invited to participate, 100% of the sample reported being of Mexican descent, likely due to the proximity of the university to Mexico (approximately two miles).
2.3. Measures
2.3.1. Form 90 (Miller, 1996)
The Form 90 is a structured assessment interview for drinking and related behaviors. The Form 90 was used in Project MATCH to quantify alcohol consumption, and has demonstrated excellent psychometric properties (Project MATCH Research Group, 1997). In the present research, this instrument was self-administered by participants in small groups with instruction from a bilingual graduate student researcher, who was also available to answer questions about the procedure. The self-administered version of the Form 90 used in this study included a calendar grid, called the Steady Pattern, which prompted respondents to indicate the number of standard drinks typically consumed on each day of the week. Participants were then asked to indicate whether their reported pattern of drinking was consistent from week to week. If not, additional information was gathered about atypical drinking days (days in which the respondent remembered drinking more or less than they reported on the Steady Pattern). Participants’ responses were used to calculate an estimate of the number of standard drinks consumed per week in the previous 90 days.
2.3.2. The Readiness to Change Questionnaire (RTCQ; Rollnick et al., 1992)
The RTCQ was used to assess motivation to change one’s drinking. This 12-item measure includes three subscales (Precontemplation, Contemplation, and Action) that are assessed with four items each (coefficient alphas range from .73 to .85 for each subscale; Bombardier & Heinemann, 2000). Participants were asked to indicate their agreement with each item by choosing a response on a five-point Likert scale with response options ranging from −2 (strongly disagree) to +2 (strongly agree), with the mid-point (0) indicating that the respondent was unsure. Scores were summed for each subscale and a total RTCQ score was calculated by summing the Contemplation and Action subscale scores and then subtracting the Precontemplation subscale score. The resulting overall score (from a possible range of −24 to +24) represented the participant’s motivation to change, with higher scores indicating greater motivation or readiness (Bombardier & Heinemann, 2000). Sample items from this measure include “I am trying to drink less than I used to,” and “My drinking is a problem sometimes.”
2.3.3. Rutgers Alcohol Problem Inventory (RAPI; White & Labouvie, 1989)
The RAPI was used to assess the negative consequences of drinking participants had experienced, such as problems with relationships or school performance. The RAPI, a self-report instrument originally developed for use with adolescent drinkers, has been successfully used to assess alcohol consequences among college students (e.g., Baer, Kivlahan, Blume, McKnight, & Marlatt, 2001; Geisner, Larimer, & Neighbors, 2004; Simons, Christopher, & Mclaury, 2004). The RAPI includes 23 items that are scored on a 5-point Likert scale with response options indicating the frequency with which a respondent has experienced common consequences resulting from excessive alcohol use. Responses range from 0 (Never) to 4 (More than 10 times) and are summed for a possible range of 0 to 92. Greater values on the RAPI indicate more frequent consequences experienced. Sample items include “Not able to do your homework or study for a test,” and “Got into fights, acted bad, or did mean things.”
2.4. Procedure
The study was approved by the appropriate Institutional Review Board prior to data collection, and informed consent was obtained from each participant. Data collection took place in small groups with a bilingual facilitator present to guide participants through the instruments and to explain how to complete the Form 90 and to answer questions. Students were assessed at baseline and then randomized to condition. Participants in the manual-only condition were given the ASTP manual and instructed to return approximately three months and again 12 months later to complete follow-up assessments. Participants in the full ASTP condition were given the ASTP manual and also attended two educational peer-led sessions designed to challenge alcohol expectancies, promote self-monitoring of one’s drinking, and provide individualized feedback about the student’s drinking behavior as compared with his or her peers. These participants were similarly instructed to return for follow-up assessments approximately three months and one year following the final peer-led ASTP session. The follow-up assessments consisted of the same measures administered at baseline. Participants were given gift cards to the university bookstore for each assessment packet they completed. Because the primary analyses found no significant differences between the conditions with regard to drinking behavior, readiness to change, or consequences, the groups were analyzed as one in the present research. Similarly, because the changes in alcohol consumption reported in the original research study took place between the baseline and 3-month follow-up assessments (and remained stable between the 3-month and 12-month assessments), the outcome data analyzed in the present research included only those gathered at the 3-month follow-up.
2.5. Analyses
First, descriptive statistics and bivariate (zero-order) correlations were calculated for all variables of interest, and coefficient alpha was calculated for the RAPI and the subscales of the RTCQ. Then, hierarchical least-squares regression was used to determine whether baseline readiness to change was significantly predicted by alcohol consumption and associated consequences. Weekly alcohol consumption was entered in the first step; total RAPI scores were entered in the second step; and total RTCQ scores were entered as the outcome variable. Hierarchical least-squares regression was used again to assess the effect of baseline readiness to change on drinking behavior reported at 3-month follow-up, controlling for baseline drinking. Weekly alcohol consumption at baseline was entered in the first step; total RTCQ scores were entered in the second step; a variable representing the interaction between baseline drinking and total RTCQ scores was entered in the third step; and weekly alcohol consumption at follow-up was entered as the outcome variable. Alpha was set at .05 for all statistical tests.
3. Results
3.1. Descriptives and correlations
As reported previously, participants were drinking a mean of 34.73 (SD=25.86) standard drinks per week at baseline; by the follow-up assessment, the mean number of drinks per week decreased to 26.73 (SD=20.79) across conditions. This difference was statistically significant, t(83)=3.44, p=.001. Frequency of alcohol-related consequences at baseline (i.e., RAPI scores) ranged from 0 to 66 (M=23.24, SD=14.87) and total baseline RTCQ scores ranged from −23.00 to 22.00 (M=−.17, SD=9.88). The RAPI demonstrated excellent internal consistency in the present sample (coefficient alpha=.90). The RTCQ subscale scores had adequate estimates of internal consistency as well (Precontemplation: alpha=.69; Contemplation: alpha=.77; Action: alpha=.88). Baseline drinking was positively associated with baseline consequences (r=.24, p=.026), baseline readiness to change (r=.29, p=.008), and post-intervention alcohol consumption (r=.60, p<.001). Similarly, there was a positive correlation between consequences and readiness to change at baseline (r=.41, p<.000) and between baseline consequences and follow-up drinking (r=.34, p=.002). See Table 1 for a summary of correlations between all study variables.
Table 1.
Variable correlations (N=84).
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| 1. Weekly alcohol consumption (baseline) |
– | ||||||
| 2. Weekly alcohol consumption (follow-up) |
.60** | – | |||||
| 3. RAPI scores (baseline) | .24* | .34** | – | ||||
| 4. Total RTCQ scores (baseline) |
.29** | .18 | .41** | – | |||
| 5. Precontemplation scores (baseline) |
−.36** | −.19 | −.36** | −.83** | – | ||
| 6. Contemplation scores (baseline) |
.36** | .34** | .54** | .84** | −.64** | – | |
| 7. Action scores (baseline) |
.02 | −.07 | .13 | .79** | −.49** | .45** | – |
Note. p<.05,
p<.01.
3.2. Hierarchical least-squares regression analyses
Results from the regression analyses support the first and second hypotheses and partially support the third. Drinking (weekly alcohol consumption reported in the prior 90 days) and consequences (total RAPI scores) at baseline significantly predicted baseline readiness to change (total RTCQ scores; see Table 2). These two predictors accounted for 20.4% of the variance in readiness to change scores (R2=.204, p<.001). Greater baseline drinking predicted greater readiness, as did greater drinking-related consequences. Furthermore, weekly alcohol consumption at baseline significantly predicted weekly alcohol consumption at follow-up (β=.60, p=.001), but there was no main effect of readiness to change on follow-up drinking (β=.01, p>.05). There was a significant baseline drinking by readiness to change interaction, however. See Table 3 for a summary of these findings.
Table 2.
Hierarchical regression analysis predicting total RTCQ scores at baseline (N=84).
| Step and predictor variable | B | SE B | β | t | p | R 2 | Δ R2 |
|---|---|---|---|---|---|---|---|
| Step 1 | .08 | ||||||
| Weekly alcohol consumption at baseline | .11 | .04 | .29 | 2.70 | .01 | ||
| Step 2 | .20 | .12* | |||||
| Weekly alcohol consumption at baseline | .08 | .04 | .20 | 1.96 | .06 | ||
| Total RAPI scores at baseline | .24 | .07 | .36 | 3.53 | .00 |
Note. RAPI = Rutgers Alcohol Problem Index;
p<.01.
Table 3.
Hierarchical regression analysis predicting weekly alcohol consumption at follow-up (N=84).
| Step and predictor variable | B | SE B | β | t | p | R 2 | Δ R2 |
|---|---|---|---|---|---|---|---|
| Step 1 | .36 | ||||||
| Weekly alcohol consumption at baseline |
.48 | .07 | .60 | 6.81 | .00 | .36 | |
| Step 2 | .36 | .00 | |||||
| Weekly alcohol consumption at baseline |
.48 | .08 | .60 | 6.47 | .00 | ||
| Total RTCQ scores at baseline | .01 | .20 | .01 | .05 | .96 | ||
| Step 3 | .47 | .10** | |||||
| Weekly alcohol consumption at baseline |
.55 | .07 | .68 | 7.73 | .00 | ||
| Total RTCQ scores at baseline | .89 | .29 | .42 | 3.10 | .00 | ||
| Weekly consumption X RTCQ | −.03 | .01 | −.55 | −3.94 | .00 |
Note. p<.001.
Incorporating the baseline drinking by readiness to change interaction term in the regression model resulted in a significant interaction (β=−.55, p<.001; see Table 3).1 As is depicted in Fig. 1, greater readiness to change at baseline (RTCQ scores >1 SD above the mean) predicted reduced drinking at follow-up only among the heaviest drinkers (baseline drinking >1 SD above the mean). For the lightest drinkers (baseline drinking <1 SD below the mean), readiness to change operated in the opposite direction, such that increased readiness to change at baseline predicted relatively higher levels of drinking at follow-up among lighter drinkers.2
Fig. 1.
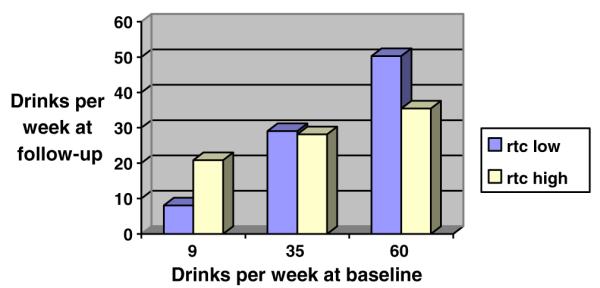
Baseline weekly alcohol consumption moderates the relationship between readiness to change and post-intervention weekly alcohol consumption. RTC=Readiness to Change Questionnaire scores.
4. Discussion
As expected, drinking behavior and consequences at baseline significantly predicted baseline readiness to change scores in the present sample of 84 Hispanic college students. Students who reported consuming more alcohol per week and experiencing more alcohol-related consequences at baseline reported greater readiness to change their drinking. Also, drinking reported at baseline significantly predicted drinking reported at 3-month follow-up, although there was a reduction in alcohol consumption between the two assessments that was not explained by experimental condition (Hernandez et al., 2006). Although participants, on average, reported significantly reduced alcohol consumption at the 3-month follow-up assessment when compared to baseline consumption, those who drank more at baseline also drank more at follow-up.
The relationship between readiness to change and follow-up alcohol consumption was moderated by levels of drinking at baseline. For the heaviest drinkers, higher readiness to change was associated with reduced drinking at follow-up. The negative association between readiness to change and post-intervention alcohol consumption is logical and was expected; students who reported greater motivation to reduce their alcohol intake had greater reductions in weekly alcohol consumption after the intervention. Because they were more motivated at the beginning of treatment, these students may have paid more attention during the intervention or read the manual more carefully. They may also have practiced implementing the skills taught during the intervention more diligently, or sought out further information on their own about how to reduce their intake. As a result, these students were more successful at reducing their drinking. Conversely, the students who reported the heaviest levels of alcohol consumption and lowest levels of readiness to change at baseline experienced more modest reductions in drinking between baseline and follow-up. These heavier drinking, less motivated participants may have been more dependent on alcohol, more doubtful that their drinking was potentially problematic, or less confident in their ability to reduce their intake. Regardless of the reason, it is logical that students who reported less motivation to change their drinking did not change as much as those who reported more motivation to change.
The direction of the relationship between readiness to change and alcohol consumption at follow-up was reversed for the lightest drinkers. For these lighter drinkers, greater readiness to change was associated with increased alcohol consumption at follow-up. Lighter drinkers who reported low readiness to change at baseline were drinking at about the same level at follow-up, suggesting that perhaps they were not motivated to change because they did not believe that change was necessary due to their comparably low levels of consumption. It is not surprising that light drinkers low in readiness to change would continue drinking at the same rate after a harm reduction intervention. Paradoxically, lighter drinkers who reported greater readiness to change at baseline were found to have increased alcohol consumption at follow-up. These participants with low baseline drinking and high baseline readiness to change, on average, were found to be drinking about twice as much after the intervention than beforehand. This unanticipated finding could be explained by the students’ drinking experiences prior to the study initiation. It is possible that these participants reported being highly motivated to change their drinking because they had previously been drinking at higher levels (prior to the baseline assessment) and were trying to control their drinking at the time the study began. The increased consumption noted at follow-up may indicate a relapse to previous drinking patterns among these participants. This conclusion is speculative, however. The interaction between baseline drinking and readiness to change warrants further exploration.
It is important to note that the sample consisted of relatively heavy drinkers (participants consumed a mean of approximately 35 standard drinks per week at baseline and 27 standard drinks per week at follow-up). Even if consumed equally throughout the week, these means correspond to average drinking levels of approximately five standard drinks per day, a quantity that exceeds the binge criterion for both women and men. The heaviest drinkers were considered to be those who drank approximately 60 drinks per average week in the three months prior to the baseline assessment; “lighter” drinkers were those who drank approximately nine drinks per average week in the three months prior to baseline assessment. Even the lightest drinkers, if consuming their nine weekly drinks during a binge episode, may be drinking at dangerous levels. The heavy alcohol use found in this sample supports the speculation that the lighter drinkers may have been trying to restrain their drinking at baseline, resulting in the paradoxical increase in alcohol consumption noted at follow-up.
4.1. Conclusion
Drinking among Hispanic college students living on the US/Mexico border is a serious concern. Interventions such as the ASTP that have been developed and tested in Anglo college student populations may be effective for Hispanic students as well, especially if culturally tailored and made available in Spanish or bilingual formats. Still, further research is needed to explore the effect of readiness to change on intervention outcomes in this population. Motivation is an important predictor of treatment outcomes in other populations, and the present research suggests that readiness to change differentially predicts drinking outcomes for students with varying levels of alcohol use. Interventions for problem drinking in this population should assess and address motivation to change because it is an important construct for predicting successful outcomes, and because motivation can be significantly enhanced or improved via motivational interviewing and similar intervention strategies (Miller & Rollnick, 2002). Moreover, if drinkers are indeed trying to control their drinking and subsequently returning to prior levels of alcohol involvement, relapse prevention strategies may prove to be effective and important components of harm reduction interventions in this population.
The borderland community is a unique environment for young adult drinkers because of the increased accessibility, lower minimum drinking ages, and decreased cost of alcohol in Mexico. Results from studies conducted on the US/Mexico border may not be expected to generalize to other borders (i.e., US/Canada), other Hispanic groups (e.g., Cuban, Puerto Rican, South American), or even to Mexican American college students residing elsewhere in the state or nation. Generalizability may be limited also by the heavy drinking found in this sample; it is possible that different findings would result from an exploration of more moderate drinkers. However, the US/Mexico border spans an expansive geographical area with numerous universities and high schools, and it is expected that these students are drinking at comparable rates to those in the present sample. Therefore, these findings may generalize to other young adult and adolescent problem drinkers who drink in Mexico.
The distinctive attributes of the US/Mexico border communities offer unique opportunities to learn about translating interventions from one culture to another. Such research offers the potential to uncover the key ingredients in effective harm reduction and motivational interventions, thus furthering the state of knowledge about these therapeutic modalities as well as college student drinking in the US. This study involved the secondary analysis of data gathered during one such intervention study, and findings contribute to the literature on readiness to change in ethnic minority populations.
Acknowledgments
Statement of Funding Sources This project was funded by Grant N006, Texas Higher Education Coordinating Board. Preparation of this manuscript was supported by the National Institute of Alcohol Abuse and Alcoholism grant T32-AA007583.
Footnotes
Because the alcohol consumption variables were positively skewed, a supplementary analysis was conducted in which these variables were winsorized, such that two outliers at baseline and one outlier at follow-up (values greater than three standard deviations from the mean) were set to the next highest value. The pattern of means remained the same. The interaction in the analysis of winsorized data approached statistical significance (p=.053).
As a supplementary analysis, a three-way interaction between experimental condition, baseline drinking and readiness to change at baseline was tested in a regression model predicting drinking at 3-month follow-up, but the interaction was not significant.
Contributors Author C designed the study and wrote the protocol. Author A conducted literature searches and wrote the first draft of the manuscript. Authors A and B conducted the statistical analysis. Authors A, B, and C contributed to and have approved the final manuscript.
Conflict of Interest All authors declare that they have no conflicts of interest.
References
- Alexander EN, Bowen AM. Excessive drinking in college: behavioral outcome, not binge, as a basis for prevention. Addictive Behaviors. 2004;29:1199–1205. doi: 10.1016/j.addbeh.2004.03.018. [DOI] [PubMed] [Google Scholar]
- Baer JS, Kivlahan DR, Blume AW, McKnight P, Marlatt GA. Brief intervention for heavy-drinking college students: 4-year follow-up and natural history. American Journal of Public Health. 2001;91(8):1310–1316. doi: 10.2105/ajph.91.8.1310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bennett ME, Miller JH, Woodall WG. Drinking, binge drinking and other drug use among southwestern undergraduates: three-year trends. The American Journal of Drug and Alcohol Abuse. 1999;25:331–350. doi: 10.1081/ada-100101864. [DOI] [PubMed] [Google Scholar]
- Bernstein R. [Retrieved February 12, 2009];U.S. Hispanic population surpasses 45 million: now 15 percent of total. 2008 from. http://www.census.gov/Press-Release/www/releases/archives/population/011910.html.
- Blume AW, Marlatt GA, Schmaling KB. Executive cognitive function and heavy drinking behavior among college students. Psychology of Addictive Behaviors. 2000;14(3):299–302. [PubMed] [Google Scholar]
- Blume AW, Schmaling KB, Marlatt AG. Predictors of change in binge drinking over a 3-month period. Addictive Behaviors. 2003;28:1007–1012. doi: 10.1016/s0306-4603(01)00287-8. [DOI] [PubMed] [Google Scholar]
- Bombardier CH, Heinemann AW. The construct validity of the Readiness to Change Questionnaire for persons with TBI. The Journal of Head Trauma Rehabilitation. 2000;15:696–709. doi: 10.1097/00001199-200002000-00008. [DOI] [PubMed] [Google Scholar]
- Borsari B, Carey KB. Effects of a brief motivational intervention with college student drinkers. Journal of Consulting and Clinical Psychology. 2000;68:728–733. [PubMed] [Google Scholar]
- Caetano R, Ramisetty-Mikler S, McGrath C. Acculturation, drinking, and intimate partner violence among Hispanic couples in the United States: a longitudinal study. Hispanic Journal of Behavioral Sciences. 2004;26:60–78. [Google Scholar]
- Caldwell PE. Drinking levels, related problems and readiness to change in a college sample. Alcoholism Treatment Quarterly. 2002;20:1–15. [Google Scholar]
- Carey KB, Henson JM, Carey MP, Maisto SA. Computer versus in-person intervention for students violating campus alcohol policy. Journal of Consulting and Clinical Psychology. 2009;77:74–87. doi: 10.1037/a0014281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carey KB, Purnine DM, Maisto SA, Carey MP. Assessing readiness to change substance abuse: a critical review of instruments. Clinical Psychology Scientific Practice. 1999;6:245–266. [Google Scholar]
- Clapp JD, Voas RB, Lange JE. Cross-border college drinking. Journal of Safety Research. 2001;32:299–307. [Google Scholar]
- Courtney KE, Polich J. Binge drinking in young adults: data, definitions, and determinants. Psychological Bulletin. 2009;135:142–156. doi: 10.1037/a0014414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Day JC. Population projections of the United States by age, sex, race, and Hispanic origin: 1995 to 2050. Current Population Reports, P25-1130. U.S. Bureau of the Census; U.S. Government Printing Office; Washington, DC: 1996. [Google Scholar]
- Dimeff LA, Baer JS, Kivlahan DR, Marlatt GA. Brief alcohol screening and intervention for college students (BASICS): a harm reduction approach. Guilford Press; New York: 1999. [Google Scholar]
- Fromme K, Marlatt GA, Baer JS, Kivlahan DR. The Alcohol Skills training Program: a group intervention for young adults. Journal of Substance Abuse Treatment. 1994;11(2):143–154. doi: 10.1016/0740-5472(94)90032-9. [DOI] [PubMed] [Google Scholar]
- Geisner IM, Larimer ME, Neighbors C. The relationship among alcohol use, related problems, and symptoms of psychological distress: gender as a moderator in a college sample. Addictive Behaviors. 2004;29(5):843–848. doi: 10.1016/j.addbeh.2004.02.024. [DOI] [PubMed] [Google Scholar]
- Heather N, Rollnick S, Bell A. Predictive validity of the Readiness to Change Questionnaire. Addiction. 1993;88:1667–1677. doi: 10.1111/j.1360-0443.1993.tb02042.x. [DOI] [PubMed] [Google Scholar]
- Heather N, Rollnick S, Bell A, Richmond R. Effects of brief counseling among male heavy drinkers identified on general hospital wards. Drug and Alcohol Review. 1996;15:29–38. doi: 10.1080/09595239600185641. [DOI] [PubMed] [Google Scholar]
- Hernandez DV, Skewes MC, Resor MR, Villanueva MR, Hanson BS, Blume AW. A pilot test of an alcohol skills training programme for Mexican–American college students. The International Journal on Drug Policy. 2006;17:320–328. [Google Scholar]
- Hingson R, Heeren T, Winter M, Wechsler H. Magnitude of alcohol-related mortality and morbidity among U.S. college students ages 18–24: changes from 1998 to 2001. Annual Review of Public Health. 2005;26:259–279. doi: 10.1146/annurev.publhealth.26.021304.144652. [DOI] [PubMed] [Google Scholar]
- Lange JE, Voas RB, Johnson MB. South of the border: a legal haven for underage drinking. Addiction. 2002;97:1195–1203. doi: 10.1046/j.1360-0443.2002.00182.x. [DOI] [PubMed] [Google Scholar]
- Larimer ME, Marlatt GA, Baer JS, Quigley LA, Blume AW, Hawkins EH. Harm reduction for alcohol problems: expanding access to and acceptability of prevention and treatment services. In: Marlatt GA, editor. Harm Reduction: Pragmatic approaches to managing high-risk behaviors. Guilford Press; New York: 1998. pp. 69–121. [Google Scholar]
- Laudet AB. Attitudes and beliefs about 12-step groups among addiction treatment clients and clinicians: toward identifying obstacles to participation. Substance Use & Misuse. 2003;38:2017–2047. doi: 10.1081/ja-120025124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maisto SA, Conigliaro J, McNeil M, Kraemer K, Conigliaro RL, Kelley ME. Effects of two types of brief intervention and readiness to change on alcohol use in hazardous drinkers. Journal of Studies on Alcohol. 2001;62:605–614. doi: 10.15288/jsa.2001.62.605. [DOI] [PubMed] [Google Scholar]
- Marlatt GA, Baer JS, Kivlahan DR, Dimeff LA, Larimer ME, Quigley LA, et al. Screening and brief intervention for high-risk college student drinkers: results from a 2-year follow-up assessment. Journal of Consulting and Clinical Psychology. 1998;66:604–615. doi: 10.1037//0022-006x.66.4.604. [DOI] [PubMed] [Google Scholar]
- Marlatt GA, Witkiewitz K. Harm reduction approaches to alcohol use: health promotion, prevention, and treatment. Addictive Behaviors. 2002;27:867–886. doi: 10.1016/s0306-4603(02)00294-0. [DOI] [PubMed] [Google Scholar]
- Martin CS, Kaczynski NA, Maisto SA, Bukstein OM, Moss HB. Patterns of DSM-IV alcohol abuse and dependence symptoms in adolescent drinkers. Journal of Studies on Alcohol. 1995;56:672–680. doi: 10.15288/jsa.1995.56.672. [DOI] [PubMed] [Google Scholar]
- McKinnon S, O’Rourke K, Byrd T. Increased risk of alcohol abuse among college students living on the US–Mexico border: implications for prevention. Journal of American College Health. 2003;51:163–167. doi: 10.1080/07448480309596345. [DOI] [PubMed] [Google Scholar]
- McKinnon SA, O’Rourke KM, Thompson SE, Berumen JH. Alcohol use and abuse by adolescents: the impact of living in a border community. The Journal of Adolescent Health. 2004;34:88–93. doi: 10.1016/s1054-139x(03)00251-9. [DOI] [PubMed] [Google Scholar]
- McNally AM, Palfai TP. Negative emotional expectancies and readiness to change among college student binge drinkers. Addictive Behaviors. 2001;26(5):721–734. doi: 10.1016/s0306-4603(00)00157-x. [DOI] [PubMed] [Google Scholar]
- Miller WR. Form 90: a structured interview for drinking and related behaviours. In: Mattson ME, editor. Project MATCH Monograph Series. Vol. 5. National Institute on Alcohol Abuse and Alcoholism; Bethesda, MD: 1996. [Google Scholar]
- Miller WR, Rollnick S. Motivational interviewing: Preparing people to change. 2nd ed Guilford Press; New York: 2002. [Google Scholar]
- Murphy JG, Duchnick JJ, Vuchinich RE, Davison JW, Karg RS, Olson AM, et al. Relative efficacy of a brief motivational intervention for college student drinkers. Psychology of Addictive Behaviors. 2001;15:373–379. doi: 10.1037//0893-164x.15.4.373. [DOI] [PubMed] [Google Scholar]
- O’Malley PM, Johnston LD. Epidemiology of alcohol and other drug use among American college students. Journal of Studies on Alcohol. 2002;14:23–39. doi: 10.15288/jsas.2002.s14.23. [DOI] [PubMed] [Google Scholar]
- Park CL. Positive and negative consequences of alcohol consumption in college students. Addictive Behaviors. 2004;29:311–321. doi: 10.1016/j.addbeh.2003.08.006. [DOI] [PubMed] [Google Scholar]
- Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward an integrative model of change. Journal of Consulting and Clinical Psychology. 1983;51:390–395. doi: 10.1037//0022-006x.51.3.390. [DOI] [PubMed] [Google Scholar]
- Project MATCH Research Group Matching alcoholism treatments to client heterogeneity: Project MATCH posttreatment drinking outcomes. Journal of Studies on Alcohol. 1997;58:7–29. [PubMed] [Google Scholar]
- Rollnick S, Heather N, Gold R, Hall W. Development of a short “readiness to change” questionnaire for use in brief, opportunistic interventions among excessive drinkers. British Journal of Addiction. 1992;87(5):743–754. doi: 10.1111/j.1360-0443.1992.tb02720.x. [DOI] [PubMed] [Google Scholar]
- Simons JS, Christopher MS, Mclaury AE. Personal strivings, binge drinking, and alcohol-related problems. Addictive Behaviors. 2004;29:773–779. doi: 10.1016/j.addbeh.2004.02.006. [DOI] [PubMed] [Google Scholar]
- Vega WA, Sribney W. Parental risk factors and social assimilation in alcohol dependence of Mexican Americans. Journal of Studies on Alcohol. 2003;64:167–175. doi: 10.15288/jsa.2003.64.167. [DOI] [PubMed] [Google Scholar]
- Walters ST, Bennett ME, Miller JH. Reducing alcohol use in college students: a controlled trial of two brief interventions. Journal of Drug Education. 2000;30:361–372. doi: 10.2190/JHML-0JPD-YE7L-14CT. [DOI] [PubMed] [Google Scholar]
- Wechsler H, Nelson TF. Binge drinking in the American college student: what’s five drinks? Psychology of Addictive Behavior. 2001;15:287–291. doi: 10.1037//0893-164x.15.4.287. [DOI] [PubMed] [Google Scholar]
- White HR, Labouvie EW. Towards the assessment of adolescent problem drinking. Journal of Studies on Alcohol. 1989;50:30–37. doi: 10.15288/jsa.1989.50.30. [DOI] [PubMed] [Google Scholar]