

Abstract
Tobacco use is the most important preventable risk factor for premature death. The World Health Organization (WHO) Framework Convention on Tobacco Control (FCTC), the first international public health treaty, came into force in 2005. This paper reviews the present status of tobacco control policies in Korea according to the WHO FCTC recommendations. In Korea, cigarette use is high among adult males (48.2% in 2010), and cigarette prices are the lowest among the Organization for Economic Cooperation and Development countries with no tax increases since 2004. Smoke-free policies have shown incremental progress since 1995, but smoking is still permitted in many indoor public places. More than 30% of non-smoking adults and adolescents are exposed to second-hand smoke. Public education on the harmful effects of tobacco is currently insufficient and the current policies have not been adequately evaluated. There is no comprehensive ban on tobacco advertising, promotion, or sponsorship in Korea. Cigarette packages have text health warnings on only 30% of the main packaging area, and misleading terms such as "mild" and "light" are permitted. There are nationwide smoking cessation clinics and a Quitline service, but cessation services are not covered by public insurance schemes and there are no national treatment guidelines. The sale of tobacco to minors is prohibited by law, but is poorly enforced. The socioeconomic inequality of smoking prevalence has widened, although the government considers inequality reduction to be a national goal. The tobacco control policies in Korea have faltered recently and priority should be given to the development of comprehensive tobacco control policies.
Keywords: Tobacco, Korea, Smoke-free policy
INTRODUCTION
Tobacco use is the most important preventable risk factor for premature mortality as it kills approximately 5 million people worldwide every year [1]. Approximately 21% of all deaths are attributable to tobacco in Korea [2]. Moreover, cigarette smoking contributes to nearly 35% of the mortality inequality among middle-aged, Korean men [3]. The Framework Convention on Tobacco Control (FCTC) was the first international treaty by the World Health Organization (WHO) and was adopted in 2003, entered into force in 2005, and was ratified by 178 parties. The WHO FCTC is an evidence-based treaty that incorporates tobacco control policies (Table 1) [4], thus enormously advancing the worldwide implementation of tobacco control. According to reports to the Conference of the Parties and the WHO Global Progress Reports, 68% of the ratifying parties have implemented these provisions and more than 75% have strengthened existing legislation or adopted new tobacco control policies after ratifying this framework [1].
Table 1.
Evidence-based tobacco control policies
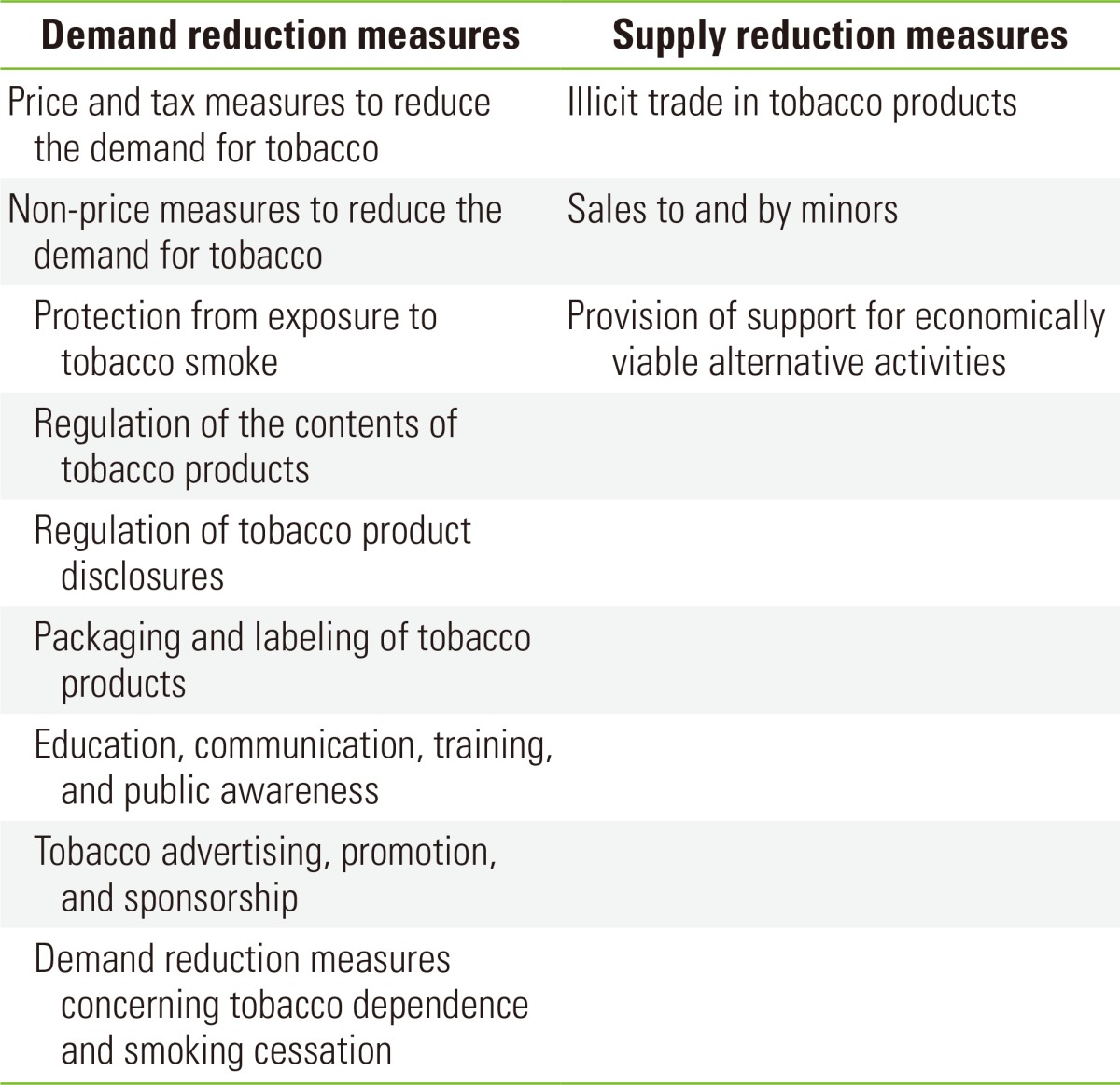
From World Health Organization. WHO framework convention on tobacco control; 2005 [4].
In 2008, the WHO introduced the acronym MPOWER measures, which has been extremely effective in reducing tobacco use. The acronym MPOWER represents the following strategies: monitoring tobacco use and tobacco control policies; protecting people from the dangers of tobacco smoke; offering help to quit tobacco; warning the public about the dangers of tobacco; enforcing bans on tobacco advertising, promotion, and sponsorship; and raising taxes on tobacco [5].
The aim of this paper was to review current tobacco control policies in Korea with respect to the WHO FCTC provisions and MPOWER measures and as well as to suggest future directions for tobacco control in Korea.
TOBACCO USE IN KOREA
The prevalence of cigarette smoking in Korea was 48.3% among adult men and 6.3% among adult women in 2010 [6]. Among males, the smoking rate has decreased dramatically from 80% in 1980 to 45% in 2005, but has plateaued since 2007. Among females, the smoking rate decreased from 12.5% in 1980 to between 5% and 8% since 1985. However, cigarette smoking among Korean women is typically under reported, and the cotinine-verified smoking rate was suspected to be nearly 20% for young females [7]. Moreover, socioeconomic inequalities in smoking prevalence exist, with the highest income quartile and the lowest income quartile being 43.5% and 54.2% among men, and 5.3% and 10.3% among women, respectively [6]. Since 1998, these inequalities have increased both relatively and absolutely [8].
BRIEF HISTORY OF TOBACCO CONTROL POLICIES IN KOREA
In 1976, the Tobacco Monopoly Act, at the request of the WHO, introduced cigarette warning labels in Korea (Table 2). However, the health warnings were quite moderate and did not reflect the real health effects of tobacco; rather, it simply stated that cigarette use should be limited for health reasons. In 1988, the Tobacco Business Act introduced stronger cigarette health warnings and restricted the advertising of tobacco products. However, this law did not aim to regulate tobacco or protect public health, but instead aimed to develop the tobacco business further. In 1988, the Korean tobacco market was opened to the multinational tobacco industry following pressures from the US government and tobacco companies. In 1995, Korea enacted the National Health Promotion Act that introduced comprehensive tobacco control measures including stronger restriction on indoor smoking; restrictions on advertisement, promotion, and sponsorship; ban on cigarette sales to minors; and a campaign highlighting the adverse health effects of tobacco use. Moreover, the Korea Tobacco and Ginseng (KT & G) company which was owned by the Korean government and was monopolized the Korean tobacco market before 1988, was privatized in 2001.
Table 2.
Principal governmental tobacco control polices in Korea

KT & G, Korea Tobacco and Ginseng; WHO, World Health Organization; FCTC, Framework Convention on Tobacco Control.
Korea signed and ratified the WHO FCTC in 2003 and 2005, respectively. A large 500 Korean won (KRW, approximately 0.5 US dollar [USD]) increase in price per cigarette pack was added as a tax in 2004. The following year, smoking cessation services opened in 253 health centers nationwide providing free nicotine replacement therapy and counseling services. In 2006, the National Health Promotion Plan was revised with the aim of reducing the socioeconomic differences in the smoking prevalence and the overall smoking prevalence nationwide. The same year, Korea introduced the National Quitline Service. Furthermore, in 2010, local governments were given the power to enact ordinances on outdoor smoking restrictions. In 2011, some public places were designated as completely smoke free, including government offices, nurseries, medical facilities, schools, and large restaurants and bars. Since the late 1970s, policies to control tobacco have been incrementally introduced and strengthened. However, these policies in Korea require further evaluation and should be compared with countries that are leading tobacco control.
CURRENT TOBACCO CONTROL POLICIES IN KOREA
Tobacco Control Revenues
Tobacco control expenditure was 8 billion KRW in 2004, and increased considerably to 23.1 billion KRW in 2005 and 31.5 billion KRW in 2006 after the substantial increase in 2004. However, tobacco control expenditure has decreased steadily since 2006 with 22.8 billion KRW in total revenue in 2012 [9]. Government funding for tobacco control policies is essential to implement tobacco control programs effectively. In 2014, the US Centers for Disease Control and Prevention (CDC) recommended that a minimum level of funding of approximately 7.41 USD per capita is required to maintain comprehensive tobacco control programs and policies [10]. In comparison with the US, level of tobacco control expenditure in Korea is less than 20% of the minimum level recommended by the US CDC.
Tobacco Pricing and Taxation
Pricing and taxation measures are an effective and important means of reducing tobacco consumption. The WHO FCTC recommends that tax and price polices on tobacco products be implemented to reduce tobacco consumption [4]. For example, a 10% increase in the price of tobacco was proven to reduce tobacco consumption by approximately 4% in developed countries, with an even greater decrease in developing countries [11]. In addition, the price elasticity of tobacco consumption is much greater for adolescents than adults and also in low-income groups than high-income adults [12]. Tobacco price increases also delay the initiation of smoking among children and adolescents.
Tobacco taxes comprise 62% of the current retail price of cigarettes in Korea (2.10 USD per pack), which is the lowest out of the 36 Organization for Economic Cooperation and Development countries and only 15% of the price in Norway (Figure 1) [12]. In Korea, the last tobacco tax increased in 2004 (500 KRW); therefore, cigarettes have become relatively more affordable due to the inflation and increased income in Korea since 2004. This lack of a further tobacco tax over the past decade in Korea may be one of important factor contributing to the static smoking prevalence that was noted since 2007.
Figure 1.

Comparison of cigarette prices among Organization for Economic Cooperation and Development countries. From World Health Organization. Global health observatory data repository [12].
Smoke-free Policies
Reducing the exposure of second-hand cigarette smoke through smoking bans in indoor public places improves the health of the workers, reduces asthma admissions in children, improves birth outcomes (e.g., by reducing the incidence of low birth weights and stillbirths), and benefits the health of the general population by reducing the rate of ischemic heart attacks [13]. Moreover, such a policy reduces tobacco consumption [13] and changes social norms surrounding cigarette use in public places [14]. The rate of exposure to second-hand smoke among Korean adults was 38.1% in 2010 [6], and 30.7% of adolescents reported being exposed to second-hand smoke at the home [15].
With the adoption of the National Health Promotion Act, smoking became restricted in indoor public places from 1995 in Korea. Since 1995, these restrictions have widened. However, previous smoke-free policies were not comprehensive and divided indoor environments into smoking and non-smoking sections. This partial ban does not completely protect non-smokers from second-hand smoke. In 2011, a comprehensive ban was introduced for some public places, including public transport, government buildings, medical care facilities, nurseries, all schools except university campuses, large restaurants and bars, and large buildings and theaters. However, designated smoking rooms are still permitted [16]. Moreover, cigarette smoking is still allowed in small restaurants and bars, small buildings, and theaters. In contrast, the WHO FCTC recommends that a comprehensive smoking ban that encompass all indoor public places including public transport and that no designated smoking areas be allowed.
In Korea, outdoor smoking bans are becoming of great interest to local governments since they were given the power to enact ordinances from 2010 [16]. Of the 246 local governments in Korea, 199 (80.9%) developed ordinances to restrict cigarette use in outdoor places in 2013 [17]. The most commonly protected places include bus stops (97%), public parks (95%), school clean zones (94.0%), gas stations (56.3%), and playgrounds (54.3%). Because there is no evidence of public health harm caused by outdoor second-hand smoke exposure [18], outdoor smoking bans continue to be open to criticism as a potentially misdirected tobacco control policy and a waste of the local government's revenue and time.
Education, Communication, Training, and Public Awareness
Campaigns to educate the public about the hazards of tobacco use are effective in reducing tobacco consumption and changing social norms regarding tobacco use. However, the effectiveness of mass media campaigns depends on their reach, intensity, duration, and message. The most effective approach involves negative health messages with a sufficient population exposure [19]. In Korea, various public awareness campaigns highlighting the hazards of tobacco have been undertaken, including mass media campaigns involving television and radio, advertisements on buses and in subway, and the dissemination of information and smoking cessation programs through the internet and self-help leaflets at health centers. However, some of the content reported in these campaigns is not based on scientific evidence and the effectiveness of these campaigns have not been adequately evaluated. Overall, knowledge of the adverse health effects of tobacco use is still limited in Korea [20]; thus, more efforts to raise awareness are needed.
Tobacco Advertisement, Promotion, and Sponsorship
Tobacco advertising bans have been proven to reduce tobacco consumption if comprehensive [21]. In contrast, tobacco promotion tends to increase tobacco consumption, especially among adolescents [22]. Tobacco advertisements on the TV and radio are banned in Korea but are allowed in magazines and at the point of sale. In retail stores, cigarette displays are also allowed. There are restrictions on tobacco sponsorship, but only for events that exclusively involve women and adolescents (article 9-4, National Health Promotion Act) [16]. KT & G, the leading tobacco company in Korea, very actively supports low-income individuals and cultural events through the KT & G Social Security Foundation.
The WHO FCTC recommends that all advertising, promotion, and sponsorships by the tobacco industry be completely banned because these activities promote the sale of cigarettes, especially to adolescents. The WHO FCTC also recommended that advertisement, promotion, and sponsorship bans be introduced within 5 years of the WHO FCTC ratification (by 2010 for Korea), but no further measures have been taken in Korea since the WHO FCTC was ratified.
The Labeling and Packaging of Cigarettes
Packaging has become a key marketing tool for cigarette companies because of the increased advertising and sponsorship bans that have been enacted worldwide. Unregulated package coloring and imagery contribute to consumers' misperception that certain cigarettes are safer than others are. Removing colors and misleading terms from cigarette packs would reduce false beliefs in the safety of cigarettes [23]. In Korea, health warnings on cigarette packs are written in text and comprise 30% of the main part of the packaging. Although misleading or deceptive terms such as "mild" or "light" are still permitted [16], they will be banned from January 2015. The WHO FCTC recommended that terms such as "mild," "low tar," and "light" be banned within 3 years of the WHO FCTC ratification (by 2008 for Korea). Moreover, they suggest the introduction of pictorial health warnings that cover 50% of the main part of tobacco packaging. By 2013, 63 countries had adopted pictorial warnings, and most have introduced these labels only recently [24]. Australia introduced "plain packaging" on cigarette packs in 2012, which required the removal of all branding (colors, imagery, corporate logos, and trademarks), and permits only the brand name in a mandated size, font, and placement on the pack.
Promoting Smoking Cessation Treatments
Smoking cessation is an important component of comprehensive tobacco control measures despite its limited effect on tobacco consumption at the population level. Pharmacotherapy, including nicotine replacement therapy, bupropion, and varenicline as well as behavioral counseling are effective at aiding smoking cessation [25]. Korea introduced national Smoking Cessation Clinics in 253 health centers in 2005 that provide free nicotine replacement therapy and individual counseling. In addition, Korea operates a small-scale National Quitline Service. National Smoking Cessation Clinics cover approximately 3% of the smoking population at present (427 571 persons as of 2012) [9].
The WHO FCTC recommends the promotion of smoking cessation treatments, the development and dissemination of national treatment guidelines, and the establishment of sustainable funding for cessation services. Korea has a relatively strong national cessation program compared with other countries, but its service coverage is currently limited, mainly due to a lack of insurance coverage for smoking cessation services. Moreover, there are no national guidelines for tobacco treatment, and the participation of health professionals in smoking cessation services remains limited.
Tobacco Sales to Minors
Bans on tobacco sales to minors have been shown to effectively reduce sales by retailers [26]. However, this reduction can only be sustained when the ban is strongly enforced. In contrast, voluntary retailer compliance programs do not reduce tobacco sales to minors [27]. The monthly smoking rates are 23.9% for male high school students and 11.1% for middle school students in Korea. Among Korean females, the smoking rates are 13.8% for high school students and 5.5% for middle school students [15]. Half of all male students and 40% of all female students can directly buy cigarettes at retail stores. In 2013, more than 75% of adolescents said that they encountered no problems in purchasing cigarettes at retail stores, even though the Adolescent Protection Act prohibits the sale of cigarettes to minors (<19 years old). These data indicate that this law is poorly enforced in Korea.
Reducing the Socioeconomic Inequalities in Cigarette Smoking
Reducing the socioeconomic inequalities in health is one of the overarching goals of the Korean National Health Promotion Plan 2020. The specific targets of this plan in terms of smoking inequalities were to reduce the differences in smoking prevalence between the highest and lowest income quartiles from 15.4% in 2008 to 8.0% in 2020 among adult men and from 2.6% in 2008 to 1.5% in 2020 among adult women [28]. For adult men, the difference in smoking prevalence between the highest and lowest income quartiles was found to have decreased to 10.7% (54.2% to 43.5%), however, for adult women, the difference increased to 5.0% (10.3% to 5.3%) in 2010 [6]. The tobacco tax increase of 2004 contributed to a marginal reduction in the socioeconomic inequality of smoking in Korea [29], but other tobacco control policies may have widened the inequalities of tobacco use. For example, smoke-free policies do not cover small restaurants and bars, which may be more commonly visited by Koreans from a low socioeconomic background. In addition, anti-smoking campaigns and smoking cessation programs have not targeted low-income Koreans. National Smoking Cessation Clinics in Seoul, the capital of Korea, tended to recruit more smokers from more privileged backgrounds, and the smoking cessation rate was found to be lower in less privileged areas than it was in more privileged areas [30].
CONCLUSION
Although Korea has ratified the WHO FCTC, its tobacco control policies have not made appreciable progress, particularly in relation to the WHO recommended "best buy" policies, which include tobacco tax increases; smoke-free policies; a ban on the advertising, promotion, and sponsorship of tobacco products; and warnings about the dangers of tobacco. Moreover, it does not seem likely that the national target of reducing male adult smoking prevalence less than 29% and of reducing differences in female adult smoking prevalence less than 1.5% between the highest and lowest quartilesuntil 2020 will be achieved under the current policies. Many effective tobacco control policies that increase smoking cessation rates, reduce tobacco consumption, and delay smoking initiation among adolescents have been proven; therefore, priority should be given to create comprehensive tobacco control policies along these lines in Korea. Among them, an emphasis should be placed upon increasing tobacco taxes, enacting comprehensive smoke-free policies, and comprehensively banning tobacco advertisements, promotions, and sponsorship.
Footnotes
The author has no conflicts of interest with the material presented in this paper.
References
- 1.World Health Organization. WHO report on the global tobacco epidemic 2013. 2013. [cited 2014 Feb 20]. Available from: http://www.who.int/tobacco/global_report/2013/en/
- 2.World Health Organization. WHO global report: mortality attributable to tobacco. 2012. [cited 2014 Feb 20]. Available from: http://whqlibdoc.who.int/publications/2012/9789241564434_eng.pdf.
- 3.Khang YH, Lynch JW, Jung-Choi K, Cho HJ. Explaining age-specific inequalities in mortality from all causes, cardiovascular disease and ischaemic heart disease among South Korean male public servants: relative and absolute perspectives. Heart. 2008;94(1):75–82. doi: 10.1136/hrt.2007.117747. [DOI] [PubMed] [Google Scholar]
- 4.World Health Organization. WHO framework convention on tobacco control. 2005. [cited 2014 Feb 21]. Available from: http://whqlibdoc.who.int/publications/2003/9241591013.pdf.
- 5.World Health Organization. Tobacco: fact sheet N°339. 2013. [cited 2014 Feb 22]. Available from: http://www.who.int/mediacentre/factsheets/fs339/en/
- 6.Korean Center for Disease Control. 2010 National health statistics: Korea National Health and Nutrition Examination Survey (KNHANES) V-1. Seoul: Korean Center for Disease Control; 2011. pp. 82–83. (Korean) [Google Scholar]
- 7.Jung-Choi KH, Khang YH, Cho HJ. Hidden female smokers in Asia: a comparison of self-reported with cotinine-verified smoking prevalence rates in representative national data from an Asian population. Tob Control. 2012;21(6):536–542. doi: 10.1136/tobaccocontrol-2011-050012. [DOI] [PubMed] [Google Scholar]
- 8.Khang YH, Cho HJ. Socioeconomic inequality in cigarette smoking: trends by gender, age, and socioeconomic position in South Korea, 1989-2003. Prev Med. 2006;42(6):415–422. doi: 10.1016/j.ypmed.2006.02.010. [DOI] [PubMed] [Google Scholar]
- 9.Ministry of Health and Welfare. 2013 Community integrated health promotion program guide: tobacco control section. Sejong: Ministry of Health and Welfare; 2013. p. 131. (Korean) [Google Scholar]
- 10.Centers for Disease Control and Prevention. Best practice for comprehensive tobacco control program 2014. Atlanta: US Department of Health and Human Services; 2014. p. 138. [Google Scholar]
- 11.Chalopka FJ, Hu T, Warner KE, Jacobs R, Yurekli A. The taxation of tobacco products. In: Jha P, Chaloupka FJ, editors. Tobacco control in developing countries. Oxford: Oxford University Press; 2000. pp. 237–272. [Google Scholar]
- 12.World Health Organization. Global health observatory data repository. [cited 2014 May 26]. Available from: http://apps.who.int/gho/data/node.main.1300?lang=en.
- 13.Callinan JE, Clarke A, Doherty K, Kelleher C. Legislative smoking bans for reducing secondhand smoke exposure, smoking prevalence and tobacco consumption. Cochrane Database Syst Rev. 2010;(4):CD005992. doi: 10.1002/14651858.CD005992.pub2. [DOI] [PubMed] [Google Scholar]
- 14.Albers AB, Siegel M, Cheng DM, Biener L, Rigotti NA. Relation between local restaurant smoking regulations and attitudes towards the prevalence and social acceptability of smoking: a study of youths and adults who eat out predominantly at restaurants in their town. Tob Control. 2004;13(4):347–355. doi: 10.1136/tc.2003.007336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Korean Center for Disease Control. 2013 Korea Youth Risk Behavior Web-based Survey results. Seoul: Korean Center for Disease Control; 2013. pp. 60–63. (Korean) [Google Scholar]
- 16.National Health Promotion Act. 2013. Jul 30, Law No. 11973, Article 9-4. [Google Scholar]
- 17.Son HJ, Cho HJ, Kim HJ Society for Nicotine and Tobacco Research. Outdoor smoking bans in South Korea: current situation and public health implication; Proceedings of 20th Annual Meeting: RAPIDS; 2014 Feb 5-8; Seattle, USA. Society for Nicotine and Tobacco Research; 2014. p. 4. [Google Scholar]
- 18.Chapman S. Going too far? Exploring the limits of smoking regulations. William Mitchell Law Rev. 2008;34(4):1605–1620. [Google Scholar]
- 19.Durkin S, Brennan E, Wakefield M. Mass media campaigns to promote smoking cessation among adults: an integrative review. Tob Control. 2012;21(2):127–138. doi: 10.1136/tobaccocontrol-2011-050345. [DOI] [PubMed] [Google Scholar]
- 20.Seo HG, Cheong YS, Myung SK, Kim Y, Lee WB, Fong GT. Smoking-related characteristics in Korean adult smokers: findings from the 2005 International Tobacco Control Policy Evaluation Survey-Korea. J Korean Acad Fam Med. 2008;29(11):844–853. (Korean) [Google Scholar]
- 21.Quentin W, Neubauer S, Leidl R, König HH. Advertising bans as a means of tobacco control policy: a systematic literature review of time-series analyses. Int J Public Health. 2007;52(5):295–307. doi: 10.1007/s00038-007-5131-0. [DOI] [PubMed] [Google Scholar]
- 22.Lovato C, Watts A, Stead LF. Impact of tobacco advertising and promotion on increasing adolescent smoking behaviours. Cochrane Database Syst Rev. 2011;(10):CD003439. doi: 10.1002/14651858.CD003439.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Cancer Council Victoria. Plain packaging of tobacco products: a review of the evidence. [cited 2014 Feb 20]. Available from: http://www.heartfoundation.org.au/SiteCollectionDocuments/Evidence-Paper-Plain-Packaging.pdf.
- 24.Korea Health Promotion Foundation. Truth about cigarette package. Health Promot Ser. 2013;2(11):26–31. [Google Scholar]
- 25.Public Health Service. Clinical practice guideline. Rockville: US Department of Health and Human Services; 2008. Treating tobacco use and dependence: 2008 update; pp. 77–128. [Google Scholar]
- 26.Stead LF, Lancaster T. Interventions for preventing tobacco sales to minors. Cochrane Database Syst Rev. 2005;(1):CD001497. doi: 10.1002/14651858.CD001497.pub2. [DOI] [PubMed] [Google Scholar]
- 27.Feighery E, Altman DG, Shaffer G. The effects of combining education and enforcement to reduce tobacco sales to minors. A study of four northern California communities. JAMA. 1991;266(22):3168–3171. [PubMed] [Google Scholar]
- 28.Ministry of Health and Social Welfare. 3rd National Health Promotion Plan (2011-2020) Seoul: Ministry of Health and Welfare; 2011. pp. 96–119. (Korean) [Google Scholar]
- 29.Khang YH, Yun SC, Cho HJ, Jung-Choi K. The impact of governmental antismoking policy on socioeconomic disparities in cigarette smoking in South Korea. Nicotine Tob Res. 2009;11(3):262–269. doi: 10.1093/ntr/ntn036. [DOI] [PubMed] [Google Scholar]
- 30.Cho HJ, Jung-Choi K, Yang YS. Did Korean smoking cessation clinic reduce smoking inequalities? 2013. [cited 2014 Feb 20]. Available from: http://www.uknscc.org/uknscc2013_poster_221.php.