

Abstract
Background
Physical inactivity levels are rising in many countries with major implications for the prevalence of non-communicable diseases and the general health of the population worldwide. We conducted this study to examine leisure-time physical activity levels among African adults in an urban setting.
Methods
We conducted a cross-sectional study among a random sample of 1,058 adults at a government worksite, in Abuja, an urban Nigerian city. We used log-binomial regression models to estimate the multivariable-adjusted associations of correlates of physical activity.
Results
The mean age of the study population was 42 ± 9.3 years, 60% were men and 40% were women. The mean metabolic equivalent hours per week for all the participants was 6.8 ± 7.2. In univariate analysis comparing the lowest to highest tertiles of physical activity, the prevalence ratio (PR) and (95% confidence interval, CI) was 0.95 (0.81-1.11) p = 0.49, comparing women to men; compared to those aged <30 years the PR (95% CI) was 0.70 (0.57-0.86), 0.70 (0.58-0.85) and 0.78 (0.63-0.96) for age 30–39, 40–49 and ≥50 years respectively, p for trend = 0.03; compared to those who were normal weight, the PR was 0.93 (0.79-1.10) and 0.90 (0.74-1.09) for overweight and obese persons respectively, p = 0.26. The PR for age was attenuated to non-significant levels in multivariable analyses. Being married was a statistically significant correlate of higher physical activity levels, the PR comparing unmarried to married persons in multivariate analysis was 0.81 (0.67-0.97), p = 0.03.
Conclusions
More than 80% of urban, professional Nigerian adults do not meet the WHO recommendations of physical activity. Urbanized Africans in this study population had low levels of leisure-time physical activity, independent of age, sex and body-mass index. This has major implications for the prevalence of non-communicable diseases in this population.
Keywords: Prevalence, Physical inactivity, Correlates, Nigeria
Background
Worldwide, the contribution of different risk factors for disease burden has changed substantially, leading to a shift away from factors associated with high prevalence of communicable diseases which were particularly prevalent in children, towards those for non-communicable diseases that predominate in adulthood [1]. One of these risk factors is physical inactivity which is now the fourth leading risk factor for global morbidity and mortality. Physical inactivity was estimated to be associated with 21 to 25% of breast and colon cancer burden, 27% of diabetes and about 30% of ischemic heart disease burden in 2004 [2]. In 2010, physical inactivity and low physical activity accounted for 3 · 2 million (2 · 7 million to 3 · 7 million) deaths, and 2 · 8% (2 · 4 to 3 · 2%) of Disability-Adjusted Life Years (DALYs) globally [1]. Worldwide, 31% of adults are estimated to be physically inactive and these levels are rising with major public health implications [3]. The WHO recommends adults aged 18 to 64 years should do at least 150 minutes of moderate-intensity or 75 minutes of vigorous-intensity aerobic physical activity, or an equivalent combination of moderate- and vigorous-intensity activity weekly, in order to improve cardiorespiratory and muscular fitness, bone health and reduce the risk of NCDs and depression [4].
It is difficult to estimate trends in physical inactivity in sub-Saharan Africa due to the dearth of data. In a recent systematic review of the prevalence of physical activity in Ghana and Nigeria, 25 to 57% of Nigerians were estimated to be physically inactive though data from the various studies were considered to be limited, poorly reported and not easily comparable [5-9]. Another recent study reported that 68.6% of Nigerian adults living in a metropolitan city in Northern Nigeria were sufficiently active [10]. This wide variation of physical activity prevalence may be due to different socio-demographic characteristics and lifestyle among the groups studied, as well as differences in the definition of physical inactivity and the tools used to measure physical activity.
Objective methods of measuring physical activity, such as accelerometry and heart rate monitoring are considered to be more accurate than self-report methods [11], but as the use of these methods are not feasible in large epidemiology studies involving thousands of participants, physical activity is usually measured by self-reports with questionnaires. A summary of the reliability and criterion validity results for 7 self-report physical activity measures evaluated in adults, reported reliability correlations ranging from 0.34 to 0.89, and criterion validity correlations of 0.14 to 0.53 [12]. The International Physical Activity Questionnaire Short Form (IPAQ-SF), which has been translated to over 20 languages [13], has been used for cross-national assessment of physical activity. A study carried out in 12 countries to determine the reliability and validity of the IPAQ-SF, showed that it had an agreement of about 80% and a correlation coefficient of 0.61 [14]. However, other investigators showed that in this study, the IPAQ-SF overestimated the prevalence of physical inactivity by 50% [15]. In addition, a systematic review showed that the IPAQ-SF typically overestimated physical activity as measured by objective criterion, by an average of 84% [16]. Nevertheless, the IPAQ is still being widely used to measure physical activity variation globally [17-21].
A study to evaluate the reliability and validity of 5 commonly used physical activity questionnaires, showed that the Nurses’ Health Study (NHS) II physical activity questionnaire had statistically significant moderate reproducibility, correlation with average daily pedometer steps, total accelerometer counts per day and cardiovascular fitness [22]. To examine the prevalence and correlates of leisure-time physical activity in Nigeria, we conducted a cross-sectional survey in Abuja, Nigeria’s capital city using the NHS II physical activity questionnaire.
Methods
Study population
Between April 2010 and February 2011, we conducted a cross-sectional study among 1,058 individuals at the federal secretariat complex, Abuja, Nigeria, which houses the offices of federal public sector workers in central Nigeria. We generated a list of all offices at the federal secretariat and assigned a random number to each using a random number generator [23]. At each office assigned an odd number, workers and visitors aged over 18 years were approached to participate in the survey. The participation rate was 99% and the participants had a wide range of occupations including skilled labor and professionals. Because it is a federal establishment, the staff distribution is representative of Nigeria’s ethnic and cultural diversity.
Demographic and socio-economic factors
To verify that we had sampled a diverse population, we collected data on ethnicity, religion, marital status, level of education, and profession. To evaluate socio-economic status (SES), we asked about household possessions including fan, refrigerator, television, bicycle, motorcycle, car, source of drinking water, type of sanitation, type of residence, home ownership, separate room for cooking, source of cooking fuel, respondent self-reported and interviewer-perceived social class [24].
Physical activity
To assess physical activity levels, interviewers administered the NHS II physical activity questionnaire to the study participants. The questionnaire is a past-year physical activity recall, which measures the average amount of time per week spent on moderate and vigorous leisure time activities, and sedentary activities. Participants reported the average time per week spent on each of the following activities, in the past year: walking, hiking, jogging, running, bicycling, dancing, playing tennis, soccer, squash; golf, swimming, aerobics, weight lifting or resistance exercise. The reproducibility and validity of the NHS physical activity questionnaire has been examined and the correlations between activity reported on questionnaires and that reported on past-week recalls and 7-day diaries were 0.79 and 0.62, respectively [25]. Intensity categories were created by including activities corresponding to the range in metabolic equivalents (METs) for each category (<3 for low, 3–6 for moderate, and >6 for high), based on the recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine [26].
Anthropometric measurements
Trained research nurses measured individual height with a rigid tape measure, in accordance to the World Health Organization (WHO) multinational monitoring of trends and determinants in cardiovascular disease criteria [27]. To measure height, the participants’ were asked to take off his/her shoes, hats or head ties, stand with back to the tape measure, and hold their head in a position where he/she can look straight at a spot, head high, on the opposite wall. A flat rule was placed on the participant’s head, so that the hair (if present) was pressed flat. Height was measured to the nearest centimeter, at the level where the flat rule touched the rigid tape.
To measure weight, participants’ were asked to remove heavy outer garments, empty their pockets and step on a weighing scale, which was placed on a hard, even surface. Weight was estimated using the Omron HBF-510 W Full Body Sensor Body Composition Monitor Scale. Body-mass index categories were defined using the WHO cut points in units of kg/m2, normal weight = 18.5 - <25, overweight = 25 - < 30 and obese ≥ 30.
Statistical analysis
We excluded 17 persons who were underweight, defined as having a body-mass index < 18.5 kg/m2. We generated a wealth index using the factor analysis (principal components) procedure and varimax rotation as previously described by Filmer and Pritchett [24], to compute socio-economic status. MET hours were calculated as the product of the duration and frequency of each leisure time physical activity, weighted by an estimate of METs of the activity [28], and summed to give a total activity score in MET hours per week (MET h/wk). Physical activity was analyzed in tertiles, according to the distribution of the study population. Body-mass index was estimated as a ratio of an individual’s weight (kg) and height (m2).
We used mean and standard deviation (SD) for descriptive analyses of the continuous variables and t-tests to assess the significance of differences between groups in the distribution of continuous variables; χ2 tests were used for categorical variables. Univariate and multivariate analyses with log-binomial regression models were conducted to examine the associations between potential correlates and the prevalence physical activity, comparing the lowest tertile to the middle and highest tertiles [29-31]. All variables that were associated with physical activity in the univariate analyses with p-value ≤ 0.2, were included in the multivariate model [32]. Prevalence ratios (PRs) and their 95% confidence intervals (CIs) were calculated with the lowest tertile as the reference for all variables. All analyses were conducted with SAS for UNIX statistical software (version 9.2; SAS Institute).
Ethics
The study was conducted according to the Nigerian National Code for Health Research Ethics and the Declaration of Helsinki. Ethical approval to conduct this study was obtained from the Institute of Human Virology Nigeria Health Research Ethics Committee. Individuals were informed about the study and were requested to consent before participating in the study.
Results
The mean age (SD) of the participants was 41.6 (9.3) years; 40% (416/1041) were women and 60% (625/1041) were men. Majority of the study population were Christians, married, completed university education and had professional jobs. The mean (SD) MET hours/week (h/wk) for all the participants was 6.8 (7.2) and it was not significantly different for women 6.5 (6.9) compared to men 6.9 (7.4), p-value = 0.12. The mean (SD) MET h/wk were 0.9 (0.7), 5.2 (1.7) and 11.5 (6.7) among those in the lowest, middle and highest tertiles of physical activity respectively, p-value = <0.001. The mean (SD) BMI of all the participants was 26.8 (7.2); it was significantly different for women, 29 (5.4), compared to men 26 (4.6), p-value = <0.001. Most women (74%) and men (56%) in this study were either overweight or obese. The mean (SD) BMI of the participants in the lowest tertile of physical activity was 27.4 (4.8), 27.3 (5.0) for those in the middle tertile and 26.7 (4.6) for those in the highest tertile of physical activity p-value = 0.62, suggesting that physical activity was not a major correlate of BMI in this population. Table 1 shows the characteristics of this population overall and by tertiles of MET h/wk.Few of the participants (4%, 40/1041) spent 150 minutes or more on moderate-intensity physical activity per week, 28% (11/40) of these were women and 72% (29/40) were men. Some 13% (139/1041) of the participants spent 75 minutes or more on vigorous-intensity physical activity per week, 26% (36/139) of these were women and 73% (103/139) men. Walking was the most common leisure-time physical activity engaged in by this population. Figure 1 shows the average MET hours/week from different leisure-time physical activities.
Table 1.
Characteristics of the study population by tertiles of MET-hours* per week (MET- h/wk)
| |
|
Tertile 1 |
Tertile 2 |
Tertile 3 |
|---|---|---|---|---|
|
Characteristics |
Overall |
<2 |
2 - 8 |
>8 |
| n = 334 | n = 355 | n = 352 | ||
| |
Mean ± SD |
|||
|
Age (years) |
41.6 ± 9.3 |
41.5 ± 8.3 |
42.9 ± 9.2 |
40.2 ± 10.3 |
|
Physical activity (METs/week) |
6.8 ± 7.2 |
0.9 ± 0.7 |
5.2 ± 1.7 |
15.5 ± 6.7 |
|
Body-mass index (kg/m
2
) |
26.8 ± 7.2 |
27.4 ± 4.8 |
27.3 ± 5.0 |
26.7 ± 4.6 |
| |
Percentages |
|||
|
Age categories (years) |
|
|
|
|
| - <30 |
11 |
8 |
9 |
17 |
| - 30 – 39 |
28 |
31 |
27 |
26 |
| - 40 – 49 |
40 |
42 |
41 |
37 |
| - ≥ 50 |
21 |
19 |
23 |
20 |
|
Sex |
|
|
|
|
| - Male |
60 |
63 |
52 |
66 |
| - Female |
40 |
37 |
48 |
34 |
|
Body-mass index |
|
|
|
|
| - Normal weight |
36 |
33 |
38 |
37 |
| - Overweight |
38 |
40 |
36 |
39 |
| - Obese |
26 |
27 |
26 |
24 |
|
Religion |
|
|
|
|
| - Christianity |
80 |
71 |
85 |
84 |
| - Islam |
20 |
29 |
15 |
16 |
|
Marital status |
|
|
|
|
| - Married |
77 |
83 |
76 |
71 |
| - Not married |
23 |
17 |
24 |
29 |
|
Education |
|
|
|
|
| - None |
0.4 |
0 |
1 |
0 |
| - Primary (Elementary school) |
0.6 |
2 |
0 |
0 |
| - Secondary (High school) |
22 |
16 |
24 |
25 |
| - ≥ Tertiary (College) |
77 |
82 |
75 |
75 |
|
Occupation |
|
|
|
|
| - Self-employed |
3 |
3 |
2 |
2 |
| - Unskilled manual |
7 |
9 |
6 |
6 |
| - Skilled manual |
40 |
38 |
42 |
41 |
| - Professional/executive |
50 |
50 |
50 |
51 |
|
Socio-economic status |
|
|
|
|
| - Low |
40 |
37 |
41 |
41 |
| - Middle |
40 |
39 |
41 |
41 |
| - High |
20 |
24 |
18 |
18 |
|
Smoking |
|
|
|
|
| - Non-smoker |
96 |
97 |
98 |
95 |
| - Current smoker |
4 |
3 |
2 |
5 |
|
Alcohol |
|
|
|
|
| - None |
65 |
71 |
67 |
57 |
| - 1 unit/day |
12 |
9 |
13 |
15 |
| - 2–5 units/day |
21 |
17 |
19 |
25 |
| - 5+ units/day | 2 | 3 | 1 | 3 |
*Metabolic equivalent (MET)-hours is sum of the average time per week spent in each leisure-time physical activity multiplied by the MET value for each activity.
Figure 1.
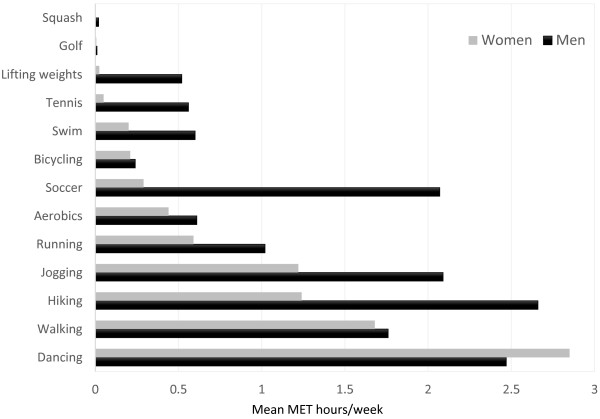
Mean MET hours/week for leisure-time physical activity, by sex.
In analysis comparing extreme tertiles, age, religion and marital status were significantly associated with levels of physical activity. Unmarried individuals and those aged less than 30 years were more likely to engage in vigorous physical activity, compared to older persons. These results are shown in Table 2. In multivariate analysis, comparing the lowest (<2 MET h/wk) to highest tertiles (>8 MET h/wk) of physical activity, being married or older than 30 years were associated with higher levels of leisure time physical activity.
Table 2.
Correlates of the lowest vs. highest tertile of physical activity
|
Characteristics |
N |
Univariate |
|
Multivariate |
|
|---|---|---|---|---|---|
| PR (95% CI) | p-value | PR (95% CI) | p-value | ||
|
Age categories (years) |
|
|
0.03 |
|
0.64 |
| - <30 |
85 |
1.00 |
|
1.00 |
|
| - 30 – 39 |
195 |
0.70 (0.57, 0.86) |
|
0.86 (0.68, 1.08) |
|
| - 40 – 49 |
270 |
0.70 (0.58, 0.85) |
|
0.87 (0.69, 1.11) |
|
| - ≥ 50 |
136 |
0.78 (0.63, 0.96) |
|
0.92 (0.72, 1.17) |
|
|
Marital status |
|
|
0.0001 |
|
0.03 |
| - Not married |
156 |
1.00 |
|
1.00 |
|
| - Married |
530 |
0.73 (0.63, 0.85) |
|
0.81 (0.67, 0.97) |
|
|
Religion |
|
|
<.0001 |
|
0.0002 |
| - Christianity |
533 |
1.00 |
|
|
|
| - Islam |
153 |
0.65 (0.52, 0.81) |
|
0.68 (0.54, 0.85) |
|
|
Socio-economic status |
|
|
0.14 |
|
0.23 |
| - Low |
268 |
1.00 |
|
1.00 |
|
| - Middle |
273 |
0.97 (0.83, 1.13) |
|
1.00 (0.86, 1.17) |
|
| - High |
145 |
0.82 (0.66, 1.01) |
|
0.85 (0.70, 1.05) |
|
|
Sex |
|
|
0.49 |
|
|
| - Male |
441 |
1.00 |
|
|
|
| - Female |
243 |
0.95 (0.81, 1.11) |
|
|
|
|
Body-mass index (kg/m
2
) |
|
|
0.26 |
|
|
| - Normal weight |
242 |
1.00 |
|
|
|
| - Overweight |
271 |
0.93 (0.79, 1.10) |
|
|
|
| - Obese |
173 |
0.90 (0.74, 1.09) |
|
|
|
|
Occupation |
|
|
0.32 |
|
|
| - Skilled manual |
272 |
1.00 |
|
|
|
| - Self-employed |
18 |
0.94 (0.58, 1.51) |
|
|
|
| - Unskilled manual |
51 |
0.74 (0.51, 1.05) |
|
|
|
| - Professional/executive |
345 |
0.97 (0.83, 1.13) |
|
|
|
|
Alcohol |
|
|
0.48 |
|
|
| - None |
432 |
1.00 |
|
|
|
| - 1 unit/day |
83 |
1.09 (0.90, 1.31) |
|
|
|
| - 2–5 units/day |
146 |
1.16 (0.75, 1.80) |
|
|
|
| - 5+ units/day | 19 | 2.20 (1.99, 2.44) | |||
PR = Prevalence ratio; CI = Confidence interval.
Discussion
In this cross-sectional study of physical activity among urbanized adult Nigerians, we found that 4% of the participants spent at least 150 minutes on moderate-intensity physical activity; while 13% spent at least 75 minutes on vigorous-intensity physical activity. To improve cardiorespiratory and muscular fitness, bone health and reduce the risk of NCDs and depression, the WHO recommends adults aged 18 to 64 years should do at least 150 minutes of moderate-intensity or 75 minutes of vigorous-intensity aerobic physical activity, or an equivalent combination of moderate- and vigorous-intensity activity weekly [4].
Although physical inactivity is common in high and low income countries, its prevalence varies worldwide [3,33]. Contrary to expectations that physical inactivity is more common in countries of high income because of the level of development than in those of low income, we found up to two-thirds of our study population did not engage in significant leisure-time physical activity [3], where physical inactivity was defined as not meeting any of three criteria: 30 minutes of moderate-intensity physical activity on at least 5 days every week, 20 minutes of vigorous-intensity physical activity on at least 3 days every week, or an equivalent combination achieving 600 metabolic equivalent minutes per week [4,34]. We also found a high prevalence of overweight and obesity, 74% of the women and 56% of the men were either overweight or obese.
Our results are consistent with other studies in this environment which also found that age, sex, and ethnic origin were associated with physical activity [35]. Previous studies reported that 25–57% of Nigerians were physically inactive [5-10]. However, the methods used in these studies differ from ours. These studies estimated physical activity as significant physical activity at least once a week [9]; or determined from occupational and leisure physical activity [6-8]; or used the IPAQ-SF [10]. A systematic review showed that the IPAQ-SF typically overestimated physical activity as measured by objective criterion, by an average of 84% [16]. Nevertheless, the IPAQ is still being widely used to measure physical activity variation globally [17-21].
Walking was the most common physical activity reported by participants. Walking is a common, accessible, inexpensive form of physical activity and is an important component of total physical activity in adult populations [36]. The comprehensive and neighborhood planning of Abuja facilitates walking and may contribute to the high prevalence of this activity in this study population. Although several studies have shown that neighborhood safety [37], walkability [38], traffic speed and volume [39], and residential density were associated with walking and other forms of physical activity [40], these have not been studied in Abuja. A recent study based on a population in Northern Nigeria showed that perceived safety from crime and traffic were inversely associated with physical activity among Nigerian adults [41].
Dancing was also a commonly reported form of physical activity, especially among women. Given that women are more likely to attend church compared to men [42,43] and the high proportion of Christians in this population, it is likely that most of the weekly dancing occurs at churches. Studies on church based interventions to increase physical activity among African American women in the United States yielded variable results [44]. Interventions to improve physical activities should consider organizations that serve as foci of community engagement similar to the role of churches among African American populations.
A systematic review showed that adults’ leisure-time physical activity, including sports participation, has increased in five high-income countries in the past 20–30 years [45]. In the study population, men were more likely to participate in soccer, tennis and swimming, compared to women. This suggests that women return home and engage in household chores, while men are more likely to participate in sports or engage in physical activity at health clubs [46]. Efforts to promote leisure time physical activity among populations like urbanized Nigerians may build on activities that are already prevalent in the community like walking and dancing instead of introducing new modalities.
Our study is limited by its cross-sectional design and focus on adults in an urban population, thus the results do not account for leisure-time physical activity among children or individuals in rural populations. However, we objectively measured the characteristics of the study population using standardized guidelines and techniques and measured physical activity using validated tools.
Conclusions
In this population, the proportion of people who engage in leisure time physical activity is low, this has major implications for the prevalence of NCDs in this population. More studies investigating factors associated with physical activity, prevalent and preferred types of physical activities, and intervention studies to increase it should be implemented. Results from such studies may help promote participation in physical activity and support policy choices that can effectively prevent NCDs in African populations.
Abbreviations
BMI: Body mass index; CI: Confidence interval; DALY: Disability-adjusted life years; IPAQ: International physical activity questionnaire; IPAQ-SF: International physical activity questionnaire short form; MET: Metabolic equivalent; NCD: Non communicable diseases; NHS: Nurses’ health study; PR: Prevalence ratios; SD: Standard deviation.
Competing interests
The authors’ have no competing interests.
Authors’ contributions
SNA designed the study, analyzed the data and drafted the manuscript. CAA obtained funds, contributed to the study design and provided critical revisions of the manuscript. Both authors contributed to the study design, read and approved the final manuscript.
Pre-publication history
The pre-publication history for this paper can be accessed here:
Contributor Information
Sally N Akarolo-Anthony, Email: sna094@mail.harvard.edu.
Clement A Adebamowo, Email: CAdebamowo@ihv.umaryland.edu.
Acknowledgement and funding
The project described was supported by the Training Research Program (TRAPING-NCD) Grant awarded to Clement A. Adebamowo (D43TW009106), from the Fogarty International Centre, National Institutes of Health, United States.
References
- Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, Amann M, Anderson HR, Andrews KG, Aryee M, Atkinson C, Bacchus LJ, Bahalim AN, Balakrishnan K, Balmes J, Barker-Collo S, Baxter A, Bell ML, Blore JD, Blyth F, Bonner C, Borges G, Bourne R, Boussinesq M, Brauer M, Brooks P, Bruce NG, Brunekreef B, Bryan-Hancock C, Bucello C. et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2224–2260. doi: 10.1016/S0140-6736(12)61766-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WHO. Book Global Health Risks: Mortality And Burden Of Disease Attributable To Selected Major Risks (Editor Ed.^Eds.) City: World Health Organization Press; 2009. Global health risks: mortality and burden of disease W. [Google Scholar]
- Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012;380:247–257. doi: 10.1016/S0140-6736(12)60646-1. [DOI] [PubMed] [Google Scholar]
- WHO. Book Global Recommendations on Physical Activity for Health (Editor ed.^eds.) City: Geneva; 2010. Global recommendations on physical activity for health. [Google Scholar]
- Abubakari AR, Bhopal RS. Systematic review on the prevalence of diabetes, overweight/obesity and physical inactivity in Ghanaians and Nigerians. Public health. 2008;122:173–182. doi: 10.1016/j.puhe.2007.06.012. [DOI] [PubMed] [Google Scholar]
- Ezenwaka CE, Akanji AO, Akanji BO, Unwin NC, Adejuwon CA. The prevalence of insulin resistance and other cardiovascular disease risk factors in healthy elderly southwestern Nigerians. Atherosclerosis. 1997;128:201–211. doi: 10.1016/S0021-9150(96)05991-6. [DOI] [PubMed] [Google Scholar]
- Forrest KY, Bunker CH, Kriska AM, Ukoli FA, Huston SL, Markovic N. Physical activity and cardiovascular risk factors in a developing population. Med Sci Sports Exerc. 2001;33:1598–1604. doi: 10.1097/00005768-200109000-00025. [DOI] [PubMed] [Google Scholar]
- Nyenwe EA, Odia OJ, Ihekwaba AE, Ojule A, Babatunde S. Type 2 diabetes in adult Nigerians: a study of its prevalence and risk factors in Port Harcourt, Nigeria. Diabetes Res Clin Pract. 2003;62:177–185. doi: 10.1016/j.diabres.2003.07.002. [DOI] [PubMed] [Google Scholar]
- Olatunbosun ST, Kaufman JS, Cooper RS, Bella AF. Hypertension in a black population: prevalence and biosocial determinants of high blood pressure in a group of urban Nigerians. J Hum Hypertens. 2000;14:249–257. doi: 10.1038/sj.jhh.1000975. [DOI] [PubMed] [Google Scholar]
- Oyeyemi AL, Oyeyemi AY, Jidda ZA, Babagana F. Prevalence of physical activity among adults in a metropolitan Nigerian city: a cross-sectional study. J Epidemiol. 2013;23:169–177. doi: 10.2188/jea.JE20120116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plasqui G, Bonomi AG, Westerterp KR. Daily physical activity assessment with accelerometers: new insights and validation studies. Obes Rev. 2013;14:451–462. doi: 10.1111/obr.12021. [DOI] [PubMed] [Google Scholar]
- Sallis JF, Saelens BE. Assessment of physical activity by self-report: status, limitations, and future directions. Res Q Exerc Sport. 2000;71:S1–14. doi: 10.1080/02701367.2000.10608875. [DOI] [PubMed] [Google Scholar]
- Njoh J. Complications of hypertension in adult urban Liberians. J Hum Hypertens. 1990;4:88–90. [PubMed] [Google Scholar]
- Craig CL, Marshall AL, Sjostrom M, Bauman AE, Booth ML, Ainsworth BE, Pratt M, Ekelund U, Yngve A, Sallis JF, Oja P. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35:1381–1395. doi: 10.1249/01.MSS.0000078924.61453.FB. [DOI] [PubMed] [Google Scholar]
- Hallal PC, Victora CG. Reliability and validity of the International Physical Activity Questionnaire (IPAQ) Med Sci Sports Exerc. 2004;36:556. doi: 10.1249/01.MSS.0000117161.66394.07. [DOI] [PubMed] [Google Scholar]
- Lee PH, Macfarlane DJ, Lam TH, Stewart SM. Validity of the International Physical Activity Questionnaire Short Form (IPAQ-SF): a systematic review. Int J Behav Nutr Phys Activ. 2011;8:115. doi: 10.1186/1479-5868-8-115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chun MY. Validity and reliability of korean version of international physical activity questionnaire short form in the elderly. Korean J Fam Med. 2012;33:144–151. doi: 10.4082/kjfm.2012.33.3.144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chu AH, Moy FM. Reliability and Validity of the Malay International Physical Activity Questionnaire (IPAQ-M) among a Malay population in Malaysia. Asia Pac J Public Health. 2013. [DOI] [PubMed]
- Saglam M, Arikan H, Savci S, Inal-Ince D, Bosnak-Guclu M, Karabulut E, Tokgozoglu L. International physical activity questionnaire: reliability and validity of the Turkish version. Percept Mot Skills. 2010;111:278–284. doi: 10.2466/06.08.PMS.111.4.278-284. [DOI] [PubMed] [Google Scholar]
- Nicaise V, Crespo NC, Marshall S. Agreement Between the IPAQ and accelerometer for detecting intervention-related changes in physical activity in a sample of Latino women. J Phys Act Health. 2013. [DOI] [PubMed]
- Oyeyemi AL, Oyeyemi AY, Adegoke BO, Oyetoke FO, Aliyu HN, Aliyu SU, Rufai AA. The Short International Physical Activity Questionnaire: cross-cultural adaptation, validation and reliability of the Hausa language version in Nigeria. BMC Med Res Methodol. 2011;11:156. doi: 10.1186/1471-2288-11-156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pettee Gabriel K, McClain JJ, Lee CD, Swan PD, Alvar BA, Mitros MR, Ainsworth BE. Evaluation of physical activity measures used in middle-aged women. Med Sci Sports Exerc. 2009;41:1403–1412. doi: 10.1249/MSS.0b013e31819b2482. [DOI] [PubMed] [Google Scholar]
- Research randomizer. [ http://www.randomizer.org/]
- Filmer D, Pritchett LH. Estimating wealth effects without expenditure data–or tears: an application to educational enrollments in states of India. Demography. 2001;38:115–132. doi: 10.1353/dem.2001.0003. [DOI] [PubMed] [Google Scholar]
- Wolf AM, Hunter DJ, Colditz GA, Manson JE, Stampfer MJ, Corsano KA, Rosner B, Kriska A, Willett WC. Reproducibility and validity of a self-administered physical activity questionnaire. Int J Epidemiol. 1994;23:991–999. doi: 10.1093/ije/23.5.991. [DOI] [PubMed] [Google Scholar]
- Pate RR, Pratt M, Blair SN, Haskell WL, Macera CA, Bouchard C, Buchner D, Ettinger W, Heath GW, King AC, Kriska A, Leon AS, Marcus BH, Morris J, Paffenbarger RS, Patrick K, Pollock ML, Rippe JM, Sallis J, Wilmore JH. Physical activity and public health. A recommendation from the centers for disease control and prevention and the American college of sports medicine. JAMA. 1995;273:402–407. doi: 10.1001/jama.1995.03520290054029. [DOI] [PubMed] [Google Scholar]
- Molarius A, Kuulasmaa K, Sans S. Book Quality Assessment of Weight and Height Measurements in the WHO MONICA Project (Editor ed.^eds.) City: Helsinki; 1998. Quality assessment of weight and meight measurements in the WHO MONICA project. [Google Scholar]
- Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, O'Brien WL, Bassett DR Jr, Schmitz KH, Emplaincourt PO, Jacobs DR Jr, Leon AS. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc. 2000;32:S498–504. doi: 10.1097/00005768-200009001-00009. [DOI] [PubMed] [Google Scholar]
- Skinner S, Li R, Hertzmark E, Spiegelman D. The SAS RELRISK9 Macro. 2012.
- Skov T, Deddens J, Petersen MR, Endahl L. Prevalence proportion ratios: estimation and hypothesis testing. Int J Epidemiol. 1998;27:91–95. doi: 10.1093/ije/27.1.91. [DOI] [PubMed] [Google Scholar]
- Zou G. A modified poisson regression approach to prospective studies with binary data. Am J Epidemiol. 2004;159:702–706. doi: 10.1093/aje/kwh090. [DOI] [PubMed] [Google Scholar]
- Maldonado G, Greenland S. Simulation study of confounder-selection strategies. Am J Epidemiol. 1993;138:923–936. doi: 10.1093/oxfordjournals.aje.a116813. [DOI] [PubMed] [Google Scholar]
- Luke A, Bovet P, Forrester TE, Lambert EV, Plange-Rhule J, Schoeller DA, Dugas LR, Durazo-Arvizu RA, Shoham D, Cooper RS, Brage S, Ekelund U, Steyn NP. Protocol for the modeling the epidemiologic transition study: a longitudinal observational study of energy balance and change in body weight, diabetes and cardiovascular disease risk. BMC Public Health. 2011;11:927. doi: 10.1186/1471-2458-11-927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Global physical activity surveillance. [ http://www.who.int/chp/steps/GPAQ/en/index.html]
- Bauman AE, Reis RS, Sallis JF, Wells JC, Loos RJ, Martin BW. Correlates of physical activity: why are some people physically active and others not? Lancet. 2012;380:258–271. doi: 10.1016/S0140-6736(12)60735-1. [DOI] [PubMed] [Google Scholar]
- Monteiro CA, Conde WL, Matsudo SM, Matsudo VR, Bonsenor IM, Lotufo PA. A descriptive epidemiology of leisure-time physical activity in Brazil, 1996–1997. Rev Panam Salud Publica. 2003;14:246–254. doi: 10.1590/S1020-49892003000900005. [DOI] [PubMed] [Google Scholar]
- Harrison RA, Gemmell I, Heller RF. The population effect of crime and neighbourhood on physical activity: an analysis of 15,461 adults. J Epidemiol Community Health. 2007;61:34–39. doi: 10.1136/jech.2006.048389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sundquist K, Eriksson U, Kawakami N, Skog L, Ohlsson H, Arvidsson D. Neighborhood walkability, physical activity, and walking behavior: the Swedish Neighborhood and Physical Activity (SNAP) study. Soc Sci Med. 2011;72:1266–1273. doi: 10.1016/j.socscimed.2011.03.004. [DOI] [PubMed] [Google Scholar]
- Jongeneel-Grimen B, Busschers W, Droomers M, van Oers HA, Stronks K, Kunst AE. Change in neighborhood traffic safety: does it matter in terms of physical activity? PLoS One. 2013;8:e62525. doi: 10.1371/journal.pone.0062525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ding D, Sallis JF, Kerr J, Lee S, Rosenberg DE. Neighborhood environment and physical activity among youth a review. Am J Prev Med. 2011;41:442–455. doi: 10.1016/j.amepre.2011.06.036. [DOI] [PubMed] [Google Scholar]
- Oyeyemi AL, Adegoke BO, Sallis JF, Oyeyemi AY, De Bourdeaudhuij I. Perceived crime and traffic safety is related to physical activity among adults in Nigeria. BMC Public Health. 2012;12:294. doi: 10.1186/1471-2458-12-294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- D’Onofrio BM, Eaves LJ, Murrelle L, Maes HH, Spilka B. Understanding biological and social influences on religious affiliation, attitudes, and behaviors: a behavior genetic perspective. J Pers. 1999;67:953–984. doi: 10.1111/1467-6494.00079. [DOI] [PubMed] [Google Scholar]
- Levin JS, Taylor RJ. Gender and age differences in religiosity among black Americans. The Gerontologist. 1993;33:16–23. doi: 10.1093/geront/33.1.16. [DOI] [PubMed] [Google Scholar]
- Young DR, Stewart KJ. A church-based physical activity intervention for African American women. Fam Community Health. 2006;29:103–117. doi: 10.1097/00003727-200604000-00006. [DOI] [PubMed] [Google Scholar]
- Knuth AG, Hallal PC. Temporal trends in physical activity: a systematic review. J Phys Act Health. 2009;6:548–559. doi: 10.1123/jpah.6.5.548. [DOI] [PubMed] [Google Scholar]
- Akarolo-Anthony SN, Odubore FO, Yilme S, Aragbada O, Odonye G, Hu F, Willett W, Spiegelman D, Adebamowo CA. Pattern of dietary carbohydrate intake among urbanized adult Nigerians. Int J Food Sci Nutr. 2013;64:292–299. doi: 10.3109/09637486.2012.746290. [DOI] [PMC free article] [PubMed] [Google Scholar]