

Abstract
Age-related cognitive changes may contribute to impairments in making complex social decisions. Interpersonal conflict is a key factor behind suicidal behavior in old age, with suicidal motivations ranging from escape to revenge. Such conflicts may prove catastrophic for people prone to suicide, in part because of their tendency to make disadvantageous decisions. Yet, little is known about social decision-making in older suicidal individuals. We assessed economic bargaining behavior using the Ultimatum Game, where players decide whether to accept or punish (reject) unfair monetary offers from another player. Our sample included depressed older adults with a history of high-medical lethality suicide attempts, low- medical lethality suicide attempts, non-suicidal depressed older adults, and those with no psychiatric history, who served as control groups. Participants in all groups punished their counterparts in response to unfair offers. However, low-lethality attempters, non-suicidal depressed, and non-psychiatric controls punished less as the cost of punishment increased, accepting more unfair offers as the stakes grew large. High-lethality attempters did not adjust their choices based on stake magnitude, punishing unfair offers without regard to the cost. Two-thirds of the difference between the high-lethality attempters and non-psychiatric controls was explained by individual differences in fairness judgments: the comparison group judged offer fairness as a joint function of inequality and magnitude, whereas the high-lethality attempter participants judged offer fairness on the basis of inequality. In real life, high-lethality attempters' relative insensitivity to the cost of retaliation may lead to uncompromising, catastrophic responses to conflict.
Worldwide, suicide rates rise with increasing age (World Health Organization, 2005). Medically serious suicide attempts that carry a significant risk of death are more prevalent in old age than in younger age groups, reflecting a greater degree of premeditation and lower ambivalence about dying by suicide (De Leo, 2001). Bereavement, illness, and disability typical of aging contribute only modestly to suicide risk, leaving unanswered the question of what other factors may account for this pattern. These data also indicate that attempted suicide in old age is more representative of death by suicide than in other age groups. Aggressive-impulsive traits play a greater role in attempted and completed suicide in younger compared to older adults (McGirr et al., 2008). The nature of the vulnerability factors for suicide remains poorly understood, although age-related cognitive decline may be one of them (Dombrovski et al., 2008; Erlangsen, Zarit, & Conwell, 2008; Gujral et al., 2012; King et al., 2000), along with decrements in decision making.
Suicide always occurs in a social context. As in Greek tragedy, it is often a solution to mounting conflicts, albeit at a catastrophic personal cost. These conflicts give rise to a range of social motivations, from a need to escape and relieve others of burden, to revenge and a wish to know that others care (Holden & Delisle, 2006). Our clinical experience suggests that a common precursor of suicidal behavior in old age is the tension between the need for support and care from children, and a distressing sense of dependence and being a burden. In this context, poor social decisions may escalate conflicts and precipitate a suicidal crisis. Perceived unfairness is a common theme, and suicide notes often describe feelings of being treated unjustly (Etkind, 1997; Holden & Delisle, 2006). One of the patients in our study thus described the feelings leading to her suicide attempt: “I was extremely hurt, angry, and felt abandoned by everyone, including God… The unfairness of the situation … made me feel stupid and used.” At the same time, attempted suicide in late life has been associated with poor social problem solving (Gibbs et al., 2009), as well as life-long patterns of interpersonal struggles and difficulties connecting to family members and to the broader environment, frequently resulting in feelings of social isolation (Duberstein et al., 2004; Harrison et al., 2010; Szanto et al., 2012). These observations motivate a general prediction that individuals prone to suicide will display an increased insensitivity to the costs of resolving social injustice. Within this framework, one can conceptualize suicide as an extreme reaction to stressors that employs a distorted cost-benefit analysis.
Perceived social injustice compels one to punish offenders, often at a cost to oneself. Economic bargaining games can model these social influences on decision-making. These paradigms are beginning to shed light on social decision processes in psychiatric illness (King-Casas & Chiu, 2012; Kishida, King-Casas, & Montague, 2010), such as distrust in borderline personality disorder (Unoka, Seres, Aspan, Bodi, & Keri, 2009). We were interested in whether suicidal individuals' disadvantageous tendencies in resolving conflicts (Gibbs et al., 2009) could be captured with the Ultimatum Game (UG), an economic bargaining game involving unfairness (see Figure 1). In the UG, one player (the proposer) suggests how to split a sum of money with a second player (the responder). The responder then decides whether to accept or reject the proposer's offer (Guth, Schmittberger, & Schwarze, 1982). If the responder accepts the offer, each player keeps their respective amounts, whereas if he rejects, neither player receives any money. Offers may be equitable (e.g., 50/50) or inequitable (e.g., 80/20), forcing the responder to trade personal gain against social equality. Despite the fact that rejection is personally costly, responders typically punish proposers who violate fairness norms by rejecting inequitable offers (usually less than 20–30% of the total stake).
Figure 1.
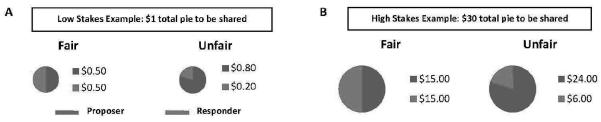
Participants Respond to Fair and Unfair Offers of High or Low Stake Size in Ultimatum Game. If the responder accepts, portions are distributed as proposed; otherwise, neither party receives any payment. For example, A) if proposer offers $0.20 out of $1.00 and the responder accepts, both parties receive the proposed amounts, B) if $6.00 out of $30.00 is offered and the responder rejects, neither party receives any amount.
Studies using the UG demonstrate that fairness is the primary motivation of rejection in diverse populations, (Pillutla & Murnighan, 1996), including younger (M. C. Crockett, L.; Hauser MD.; Robbins TW., 2010) and older individuals (Beadle et al., 2012). Specifically, the decision to reject may arise from a conflict between the emotional reaction to unfairness (e.g. anger, disgust) and cognitive efforts to accrue money. To separate these sets of factors, we used a fairness questionnaire to measure the perceptions of unfair offers in the absence of an actual incentivized choice. We also examined additional factors that may mediate the response to unfair offers including cognitive control, impulsivity and other personality characteristics, and income. For example, individuals with better cognitive control are less likely to reject unequal splits, thus maximizing their own payoff (De Neys, Novitskiy, Geeraerts, Ramautar, & Wagemans, 2011), whereas impulsivity is positively correlated with rejection rates (M. J. Crockett, Clark, Lieberman, Tabibnia, & Robbins, 2010).
Aiming to understand the role of social decision-making in suicide, our study focused on older adults because of the high proportion of medically serious suicide attempts in this age group (De Leo, 2001). Previous research on social decision-making in the UG, combined with existing knowledge about cognition in suicide attempters, leads to two independent hypotheses in the current research. Because the suicide diathesis involves impairments in executive control (Gujral et al., 2012; Keilp et al., 2001; Westheide et al., 2008) and maladaptive decision-making (Dombrovski et al., 2010; Jollant et al., 2005), suicidal older adults may be more likely to reject inequitable offers than non-suicidal older adults. Second, there is evidence that rejection decisions are sensitive not only to offer fairness, but also to the costs of rejection: responders reject small inequitable offers, but may accept comparable divisions as the amount of money to be split (i.e. stake size), increases (Andersen, Ertaç, Gneezy, Hoffman, & List, 2011). In other words, the demand for social equality is sensitive to price. People who choose suicidal acts over alternative solutions often show a diminished concern about the consequences or the cost of their choices (Linehan, Goodstein, Nielsen, & Chiles, 1983). Thus, we predicted that suicide attempters will be similarly insensitive to the monetary cost of rejecting unfair offers.
We tested the hypotheses that (a) more unfair offers will be rejected by the suicidal group versus other older adults in our sample; (b) as the stake size increases, the number of rejections of unfair offers will decrease in all groups but the suicide attempters. Suicidal behavior is heterogeneous, ranging from low-lethality attempts that carry no significant risk of death to high-lethality attempts (“failed suicides”), that have been linked to a distinct cognitive profile (Dombrovski et al., 2011; McGirr, Dombrovski, Butters, Clark, & Szanto, 2012). Low-medical lethality suicide attempts have been associated with behavioral impulsivity (Dombrovski et al., 2011), while high medical lethality suicide attempters have shown deficits in cognitive performance (Keilp et al., 2001; McGirr et al., 2012; Richard-Devantoy et al., 2011; Richard-Devantoy et al., 2012). Thus, we examined the heterogeneity related to the medical seriousness of the attempt – high- and low-lethality. In addition, we examined potential differences in fairness perception, as well as potential explanatory cognitive, social, and interpersonal variables.
Method
Participants
One hundred and three participants between the ages 42 and 89 [mean age 64.5 (8.9)] gave their informed consent as required by the University of Pittsburgh's Institutional Review Board. Depressed participants were required to meet criteria for lifetime non-psychotic unipolar major depression as diagnosed by the Structural Clinical Interview (SCID) for the DSM IV Axis I Disorders (First M, 1995). They were recruited from the inpatient clinic of the University hospital and from outpatient clinics. Patients who had received electroconvulsive therapy in the previous 6 months and those with neurological disorders, such as stroke, epilepsy, known neurodegenerative disorders, and brain tumors, as well as those with sensory disorders that precluded cognitive testing, were excluded. To increase the representativeness of the study groups, we allowed comorbid substance abuse/dependence. To ensure that there was no acute effect of substance intoxication or withdrawal on cognitive performance, we delayed testing if there was indication of intoxication or withdrawal within 72 hours, based on clinical presentation, withdrawal assessment scales or urine drug screen.
Suicide attempters had performed a self-injurious act with the intent to die (O'Carroll et al., 1996) and endorsed current suicidal ideation. The severityof suicidal intent associated with the attempt was assessed using the Suicidal Intent Scale (Beck, Shuyler, & Herman, 1974). Suicide attempt history was verified by a psychiatrist based on an interview, medical records, and information from the treatment team, family and friends. We excluded participants with significant history discrepancies between these sources. Twenty-six suicide attempters had made high lethality suicide attempts and 20 had made low lethality attempts as defined by the Beck Lethality Scale (Beck, Beck, & Kovacs, 1975). For participants with multiple attempts, data for the highest-lethality attempt are presented. High-lethality attempts resulted in coma, need for resuscitation, unstable vital signs, penetrating wounds of abdomen or chest, third-degree burns, and/or major bleeding, as defined by a score of ≥4 on the Beck Lethality Scale. All other attempts are classified as low-lethality. None of the attempts caused direct head injuries. To account for possible effects of brain injury related to the suicide attempt, study psychiatrists (KS or AYD) assessed participants for any attempts with hypotension lasting >5 minutes, asphyxia, or neurotoxic ingestion.
In order to account for the effect of depression, we included a non-suicidal depressed control group (35 non-suicidal depressed adults), as well as a benchmark group of non-psychiatric control subjects (N=22). Non-suicidal depressed participants had no current or lifetime history of suicide attempts, suicidal ideation, or indirect self-destructive behaviors as established by the clinical interview, review of medical records, SCID, and Beck's Scale for Suicidal Ideation (Beck, Kovacs, & Weissman, 1979). At the time of the administration of the UG task, participants' depressive symptoms ranged from severe to partial remission as measured by the 16-item version of the 17-item Hamilton Rating Scale for Depression (Hamilton, 1960), excluding the suicide item because it is collinear with group membership. Non-psychiatric control subjects had no lifetime history of any psychiatric disorder as determined by SCID DSM IV and no history of suicide attempts or ideation. They were recruited from primary care practices.
Procedure
Ultimatum Game (Figure 1)
Participants played the role of responder in the UG, which required players to make accept/reject decisions in a series of 24 monetary offers. They were told that they would receive the financial outcome of one trial selected randomly at the end of the game. Each trial commenced with a photograph of the proposer, followed by presentation of the stake, and finally, the proposer's offer. The same 24 offers were presented randomly to each participant and paired randomly to a photograph of the proposer. Proposers of both genders and a variety of ethnic groups were represented in the photographs.
Participants then responded to each offer by pressing one of two buttons (labeled “accept” and “reject”). Of the 24 offers, 8 were equitable (ranging from 40--50% of the stake, with a mean of 48%), 8 moderately inequitable (ranging from 26--33%; mean: 30%), and 8 very inequitable (20--25%; mean: 21%). Half of the trials presented low stakes, ranging from $1 to $10, and the other half presented large stakes, ranging from $11 to $30; this orthogonalized offer inequality and offer magnitude, as the same monetary amount could appear as an equitable offer of a low stake (e.g., $5/10) or an inequitable offer of a large stake ($5/30) (Tabibnia, Satpute, & Lieberman, 2008). Trained research assistants confirmed that all participants understood the task, however no manipulation checks were performed to test participants' engagement in the game.
Fairness questionnaire
After the UG experiment, we also elicited participants' perception of offer fairness separately from their choices. Thus they rated the fairness of six offers representative of those used in the study using a 7-point Likert-type scale (M. J. Crockett et al., 2010; M. J. Crockett, Clark, Tabibnia, Lieberman, & Robbins, 2008).
Impulsivity and interpersonal characteristics
We aimed to capture pertinent facets of impulsivity that have been empirically linked to suicidal behavior (Gibbs et al., 2009; Wilson et al., 2007). We assessed non-planning impulsivity with the Barratt Impulsivity scale (Patton, Stanford, & Barratt, 1995), and used a shortened 15-item version of the Inventory of Interpersonal Problems (IIP) to assess chronic interpersonal difficulties and screen for personality disorders (Morse & Pilkonis, 2007). Sub-scales of the IIP-15 include measures of interpersonal sensitivity, interpersonal ambivalence, and aggression.
Cognitive assessments
In order to assess cognitive factors that may influence social decisions, we measured global cognition with the Mattis Dementia Rating Scale, or DRS. To exclude individuals with clinical dementia and to ensure that participants could engage in the task, all were required to have scored ≥24 on the Mini-Mental State Exam (Folstein, Folstein, & McHugh, 1975). We assessed executive control function with the Executive Interview (EXIT) (Royall, Mahurin, & Gray, 1992), a 25-item screening test that includes items such as number/letter sequencing, Stroop, fluency test, go/no-go test, and Luria's hand sequencing.
Medical Illness Burden and Socioeconomic Status
Burden of physical illness was assessed with the Cumulative Illness Rating Scale adapted for Geriatrics (Miller et al., 1992). Socioeconomic status (SES) was measured with the McArthur's Socio-demographic questionnaire (MacArthur Network on SES and Health.). We used income per person for the last year as an estimate of SES.
Statistical analyses
We conducted analyses using MATLAB 7.6 (Wallisch et al., 2009), Mplus 7.0 (Muthén & Muthén, 2012) and SPSS 19.0 (IBM, 2010). For demographic, clinical, and socioeconomic indicators, continuous measures were compared across the four groups using analyses of variance (ANOVA); categorical data were compared with chi-square tests. All tests were two-tailed. For ANOVAs, we examined post-hoc contrasts with the Tukey Honestly Significant Difference (HSD) test, and for non-parametric tests, with adjusted pair-wise comparisons. In our analysis of the UG behavior, we took advantage of complete trial-by-trial data, using a hierarchical model with 24 trials nested within each subject. In particular, to estimate whether suicide attempters responded differently to unfairness and stake during the UG, we implemented a binary logistic generalized mixed model (GLMM), using the SAS GLIMMIX procedure. Each trial consisted of a decision to accept or reject an offer, yielding a binary response variable. To account for within-subject dependency among trials, random effects for intercept and trial were included in GLMMs, representing inter-individual differences in the average acceptance rate and linear shifts in offer acceptance over the experiment, respectively. Parameter estimates were derived using maximum likelihood estimation based on an adaptive Gauss-Hermite quadrature rule.
In additional models comparing high-lethality attempters and controls, we examined effects of potential intervening variables (e.g. impulsivity, interpersonal difficulties, and executive control). Our design required for the groups to be equated on age and sex; thus, we could not examine age and sex as intervening variables. To probe whether the effect of stake on acceptance was influenced by income, impulsivity, executive control, and interpersonal dysfunction, we examined UG acceptance rate in a multilevel structural equation modeling (MLSEM) framework using Mplus 7.0 software. In the MLSEM each participant contributed 16 trials for a total of 768 observations. We only included the 8 moderately equitable and 8 very unequitable trials in these analyses, as variance in rejection rates of the fair (equitable) trials was minimal.
MLSEM decomposes the data into within-subject and between-subject components, allows one to specify different structural models for each level, and provides a robust framework for testing mediation (Preacher, Zyphur, & Zhang, 2010; Rabe-Hesketh, Skrondal, & Pickles, 2004). More specifically, we tested whether the effect of stake on acceptance (a within-subject effect) was mediated by between-subjects factors, namely group status (i.e. attempt lethality) and fairness perceptions. Thus, we allowed the regression of trial acceptance on stake to be a random effect such that interindividual differences could be modeled at the between-subjects level. To test for mediation, the indirect effect of high-lethality (relative to controls) on the association between stake and trial acceptance via a candidate mediator (e.g., fairness perception) was computed as the product of the two coefficients representing these paths (e.g., high lethality -> fairness and fairness -> stake-acceptance) using the delta method (MacKinnon, Fairchild, & Fritz, 2007). This is technically a form of cross-level mediated moderation such that the strength of the within-subjects effect of stake on acceptance across UG trials depended on the indirect effect of group (high lethality versus control) on stake-acceptance strength via a mediator, such as fairness perception. Testing these effects is straightforward in MLSEM because of its ability to model cross-level interactions involving random slopes and compound parameters.
Results
Demographic and Clinical Characteristics
The groups did not differ significantly on demographic variables (see Table 1). Compared to the non-suicidal depressed group, high- and low-lethality suicide attempters experienced more severe depressive symptoms at the time of testing, but the lifetime prevalence of substance use and anxiety disorders (GAD, PTSD, Panic Disorder and OCD), and burden of physical illness, did not differ significantly across the depressed groups (data not shown). Global cognition measured by the Dementia Rating Scale was lower in the attempter groups than in the non-psychiatric control group. As expected, the depressed groups reported higher impulsivity and lower levels of interpersonal functioning than the non-psychiatric controls. Both high- and low-lethality attempters described more interpersonal ambivalence than non-psychiatric controls. Very few self-reported characteristics differentiated the depressed groups. Low-lethality attempters had higher levels of aggression than non-suicidal depressed participants, and low- and high-lethality attempters reported higher levels of non-planning impulsivity. As expected, high-letality attempters demonstrated higher intent to die as measured by the Beck Suicide Intent Scale (Beck et al., 1974) than low-lethality suicide attempters (18.5±5.4 vs. 13.8+5.8, F(1)=6.41, p=0.02). In addition, both high and low-lethality attempters showed high levels of suicidal ideation as measured by the Beck Suicide Ideation Scale (Beck et al., 1979) contrasting with non-suicidal depressed older adults who did not endorse suicidal ideation (high-lethality 24.0+6.8, low-lethality 22.0±8.5 vs. non-suicidal depressed 0.09±0.4, F(2)=58.6, p<0.01, D<LL, HL).
Table 1.
Demographic and Clinical Characteristics of the 103 Participants who completed the Ultimatum Game
| Non-Psychiatric Controls (C) N = 22 | Non-suicidal Depressed (D) N = 35 | Low-Lethality Attempters (LL) N = 20 | High-Lethality Attempters (HL) N = 26 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Measure | M | SD | M | SD | M | SD | M | SD | F or X2 (df) | P Value | Post Hoc, Tukey HSD |
| Age | 64.6 | 11.0 | 66.9 | 7.2 | 62.5 | 6.4 | 62.8 | 10.1 | F(3) = 1.51 | 0.22 | |
| Education, yrs | 15.0 | 1.8 | 14.1 | 2.5 | 13.7 | 2.6 | 13.0 | 3.5 | F(3) = 2.13 | 0.10 | |
| %Men | 46% | 40% | 60% | 65% | X2(2) = 4.8 | 0.19 | |||||
| %White | 77% | 83% | 85% | 100% | X2(2) = 6.01 | 0.12 | |||||
| Global cognition MDRS | 139 | 3.4 | 134 | 4.5 | 133 | 6.5 | 134 | 7.2 | F(3) = 3.68 | 0.02 | C > LL,HL |
| Current depressive severity Hamilton (16Q) | 2.3 | 2.2 | 16.7 | 5.4 | 20.3 | 6.7 | 20.2 | 5.7 | F(3) = 53.2 | <0.01 | C<D<LL,HL |
| IIP Sensitivity | 3.1 | 2.5 | 5.6 | 3.8 | 9.8 | 4.2 | 7.8 | 4.5 | F(3) = 13.8 | <0.01 | C < LL,HL & D < LL |
| Ambivalence | 2.9 | 4.2 | 3.4 | 3.2 | 6.8 | 5.5 | 6.2 | 5.3 | F(3) = 3.66 | 0.02 | C < LL,HL |
| Aggression | 1.4 | 1.5 | 3.8 | 3.4 | 6.8 | 3.2 | 5.0 | 5.4 | F(3) = 8.49 | <0.01 | C<LL.HL & LL>D |
| BIS (total) | 18.2 | 3.0 | 20.9 | 3.3 | 22.9 | 2.9 | 20.8 | 4.9 | F(3) = 9.57 | <0.01 | C < D,LL,HL |
| BIS Non-planning | 11.5 | 6.9 | 16.3 | 7.3 | 18.8 | 9.0 | 21.7 | 8.7 | F(3) = 6.53 | <0.01 | C < LL,HL |
| Household income per capita* (x$ 1000) | 34.6 | 8.3 | 19.9 | 15.3 | 24.6 | 15.7 | 20.5 | 14.9 | F(3) = 0.69 | 0.60 | |
Note. MDRS: Mattis Dementia Rating Scale, SSI: Scale of Suicidal Ideation, SIS: Suicidal Intent Scale, Hamilton: Hamilton Rating Scale for Depression, IIP: Inventory of Interpersonal Problems, BIS: Barratt Impulsiveness Scale, MacArthur Sociodemographic Questionnaire, Household income per person: MacArthur Sociodemographic Questionnaire. HSD: Honestly Significantly Different. Values are given as N, mean (standard deviation), or percentages. Post hoc comparisons were significant at p < 0.05.
Rejection behavior across groups
Participants were significantly more likely to reject very inequitable offers (74.4% rejection), relative to moderately inequitable offers (64.2% rejection) and equitable offers (12.3% rejection), F(2, 198) = 223.14, p < 0.0001. We also found a significant main effect of offer Magnitude on rejection, F(1, 99) = 18.64, p < 0.0001, such that high-magnitude offers were rejected less often that low-magnitude offers. The main effect of Group on rejection was non-significant, F(3, 99) = 0.05, p = 0.98. The Inequality × Group interaction was significant, F(6, 198) = 2.16, p = 0.05. Visual inspection indicated that participants in the three depressed groups rejected a higher proportion of equitable offers, but simple effects analysis did not reveal significant differences between groups at any levels of inequality.
Most importantly, there was a significant Group × Magnitude interaction, F(3, 99) = 4.63, p = 0.005. While non-psychiatric controls, non-suicidal depressed, and low-lethality attempters rejected a lower proportion of high magnitude offers than low magnitude offers, controlling for inequality (post hoc contrast adj. ps = .007, .005, and .0007, respectively), the high-lethality attempters did not differ significantly in their rejection of high- versus low-stake trials (p = .40) and the difference in magnitude sensitivity between high-lethality attempters and the other groups was significant, t(99) = −3.66, p = .0004 (see Figure 2). The Inequality × Magnitude interaction, F(2, 198) = 2.65, p = .07, and Inequality × Magnitude × Group interaction, F(6, 198) = 0.67, p = .68, were non-significant. Net win earnings in the game mirrored these results as high-lethality attempters earned $38, while non-psychiatric controls and non-suicidal depressed earned $42, and low-lethality attempters earned $43.
Figure 2.

Probability of offer rejection in the Ultimatum Game based on offer (trial) size. Darkened circles represent the mean probability of offer rejection at a given level of stake, whereas the vertical bars denote the standard errors of these estimates.
Mediating effects of fairness perceptions on rejection behavior
Adjustment of choices based on offer magnitude (stake) may be driven by an altered perception of fairness, or an altered choice process in high-lethality attempters. To distinguish between these alternatives, we explored the effects of fairness perception (measured with a questionnaire after the UG experiment) on rejection behavior in high-lethality attempters, as well as other factors possibly influencing choice. We tested whether the fairness perception of high-versus low-magnitude offers (controlling for inequality) differed between high lethality attempters and the other comparison groups by comparing the average quotient of high-magnitude/low-magnitude fairness ratings across groups. A value greater than 1.0 indicates that high-magnitude offers were generally perceived as more fair (the quotients were 1.18 for non-psychiatric controls, 1.11 for non-suicidal depressed, 1.32 for low-lethality attempters, and 0.95 for high-lethality attempters). Using a linear contrast based on a general linear model, we found that the tendency for high-magnitude offers to bias fairness perception was somewhat weaker in the high lethality attempters, relative to the average of the other three groups, but this effect did not reach significance (p = 0.053).
To explore demographic, clinical, and psychological factors that might explain the behavioral differences observed in high lethality attempters relative to the other groups, we fit the trial-level UG data using an MLSEM contrasting high-lethality attempters with the benchmark group of non-psychiatric controls. Factors included in the MLSEM were sex, age, fairness perception, income, executive control function, non-planning impulsivity, and chronic interpersonal difficulties. Whereas the within-subjects variability in the MLSEM reflected the relative proportion of high- versus low-stakes offers accepted, the between-subjects variability represented individual differences in the overall rate of trial acceptance. Thus, we also explored whether the groups differed in their acceptance rates, irrespective of stake, and whether individual differences in trial acceptance were related to the covariates mentioned above. As expected based on our initial group comparisons, in the MLSEM comparing high-lethality attempters with controls, attempters had significantly higher non-planning impulsivity and interpersonal ambivalence than controls (see Table 2ai: Average differences between high-lethality attempters and controls). Crucially, the tendency to rate high-magnitude offers as fairer than low-magnitude offers was significantly stronger in non-psychiatric controls than high-lethality attempters, mirroring their rejection behavior. In terms of the effects of covariates on the within-subject association between stake size and acceptance, we found that fairness perceptions were associated with rejection behavior. Participants who perceived higher-stake offers as more fair were less likely to reject them, acting in a way that can be thought of as more greedy (p < .001; see Table 2aii: Effects of between-subjects predictors on the within-subject association of offer stake and acceptance). In addition, higher income was associated with the acceptance of a larger proportion of high-stake relative to low-stake offers.
Table 2a.
Models examining effects of demographic variables, fairness perception, income, executive control, impulsivity, and interpersonal ambivalence on overall acceptance of unfair offers and stake effect (high lethality versus non-psychiatric controls).
| Predictor | Parameter estimate | Standard error | z | p | |
|---|---|---|---|---|---|
| 2a i. Average differences between high lethality attempters and controls | Income | −0.22 | 0.12 | −1.80 | 0.07 |
| Fairness perception | −0.23 | 0.11 | −2.18 | 0.03 | |
| EXIT | 2.06 | 1.30 | 1.60 | 0.11 | |
| BIS Non-planning | 10.22 | 2.28 | 4.49 | 0.00 | |
| IIP Ambivalence | 3.42 | 1.55 | 2.20 | 0.03 | |
|
| |||||
| 2a ii. Effects of between-subjects predictors on the within-subject association of offer stake and acceptance | High Lethality | ||||
| Status | 0.21 | 0.34 | 0.61 | 0.55 | |
| Age | −0.02 | 0.02 | −1.36 | 0.17 | |
| Female sex | 0.00 | 0.28 | 0.01 | 0.99 | |
| Income | 1.41 | 0.40 | 3.51 | 0.00 | |
| Fairness perception | 3.58 | 0.46 | 7.72 | 0.00 | |
| EXIT | 0.01 | 0.04 | 0.28 | 0.78 | |
| BIS Non-planning | −0.01 | 0.02 | −0.21 | 0.83 | |
| IIP Ambivalence | −0.05 | 0.03 | −1.54 | 0.12 | |
|
| |||||
| 2a iii. Indirect effects of high lethality status on the within-subject association of offer stake and acceptance via a possible mediator | Income | −0.31 | 0.19 | −1.67 | 0.10 |
| Fairness perception | −0.83 | 0.41 | −2.04 | 0.04 | |
| EXIT | 0.02 | 0.08 | 0.28 | 0.78 | |
| BIS Non-planning | −0.05 | 0.25 | −0.22 | 0.83 | |
| IIP Ambivalence | −0.16 | 0.12 | −1.32 | 0.19 | |
EXIT: Executive Function Test
BIS: Barratt Impulsivity Scale
IIP: Inventory of Interpersonal Problems
Note. Fairness perception, income, and interpersonal ambivalence completely explained stake-related behavioral differences between groups (group effect of stake on acceptance p = .99). Only fairness perception mediated the stake-related differences between groups, whereas the other covariates exercised independent effects that dominated group effects. More specifically, higher income was associated with acceptance of a greater proportion of high-stake offers relative to low-stake offers. Note: income was log-transformed. Standard errors of the indirect effects of high lethality status on the within-subject association between trial stake and acceptance via a mediator were computed using the delta method.
To test whether income, cognitive control function (EXIT), impulsivity (BIS non-planning subscale), and/or interpersonal ambivalence (IIP Ambivalence) mediated group differences in the effect of stake size on trial acceptance, we tested indirect paths from group (high lethality versus controls) to the stake-acceptance association via each potential mediator (e.g., fairness perception). A significant indirect effect would indicate that high-lethality attempters differed from controls on some covariate, such as fairness perception, and that this group difference explained the tendency for high-lethality attempters to reject high stakes offers more than controls. Group differences in fairness perception significantly explained the tendency for high-lethality attempters to reject a greater proportion of high-stake offers relative to controls (see Figure 3, Table 2a iii: Indirect effects of high lethality status on the within-subject association of offer stake and acceptance via a possible mediator). That is, whereas controls' perception of high-magnitude offers as more fair led to their rejecting a smaller proportion of them, high-lethality attempters' relative insensitivity to magnitude in fairness perception led to their rejecting a more equal proportion of high magnitude and low magnitude offers. Critically, 67% of the differential effect of magnitude in controls versus high-lethality attempters was mediated by lower fairness perception in attempters. This effect was evident even after controlling for other factors that influenced behavior, such as income level. The data indicated a trend that interpersonal ambivalence was associated with greater rejection of high-stakes offer.
Figure 3.

Effect of high lethality status on rejection of high- versus low-stake offers is mediated by fairness perception. Indirect effect of high-lethality status on trail stake-acceptance association via fairness perception. B= −.83, p=.04, *p < .05
In an MLSEM comparing high-lethality attempters versus controls that included just age and sex as covariates, the offer magnitude effect was significantly different between groups (B = −1.42, S.E. = .62, p = .02), consistent with the GLMM above. Yet, in the more comprehensive MLSEM that included all of the above covariates, the group difference in magnitude was not significantly different from zero. That is, fairness perception, income, and interpersonal ambivalence completely explained magnitude-related behavioral differences between groups (see Table 2a iii). Only fairness perception mediated the offer magnitude effect, whereas the other covariates exercised independent effects that dominated that of group. While non-significant (p = .17), the parameter estimate for the effect of age indicated that older participants were less likely to adjust their rejection rates based on offer magnitude.
Discussion
We investigated how individuals with a history of suicidal behavior integrate information about social inequality and reward or cost when perceiving and punishing unfairness. In our study, high-lethality suicide attempters' rejection behavior suggests a disregard for the cost of punishment when considering unfair offers. This tendency distinguished them from non-psychiatric controls, depressed non-suicidal patients, and low-lethality suicide attempters, whose punishment decisions were sensitive to personal cost, i.e., more likely to reject when costs were low. The effect of depression on rejection behavior was not statistically significant, similar to an earlier study (Destoop, Schrijvers, Grave, Sabbe, & Bruijn, 2012).
Our finding that the decision-making in the high-lethality attempters was less sensitive to the cost of punishment contrasts with normative demonstrations of reward-magnitude effects on choice. Healthy volunteers reject fewer high-magnitude than low-magnitude offers at similar fairness levels (Andersen et al., 2011), suggesting that at high stakes, immediate monetary payoffs outweigh any potential benefits drawn from retaliation. Similarly, stake size increases self-interest in trust games where the proportion of money sent to another player decreases as the stake size increases (Johansson-Stenman, Mahmud, & Martinsson, 2005). Higher stakes cause people to be less impulsive, reducing risk-taking (Binswanger, 1981) and delay discounting (Kirby, 1997; Liu, Vassileva, Gonzalez, & Martin, 2012), an effect that is modulated by dopamine (Campbell-Meiklejohn et al., 2012). Thus, larger rewards normally lead to selfish, non-impulsive preferences across a wide range of decision settings. However, the current results parallel findings with substance-dependent suicide attempters, in whom delay discounting was not sensitive to reward magnitude (Liu et al., 2012).
We found that fairness perceptions mediated behavioral differences in response to magnitude, as participants who perceived higher magnitude offers as less unfair were significantly less likely to reject them. There was a significant difference in fairness perception between non-psychiatric controls and high-lethality attempters: controls rated higher magnitude offers as more fair, whereas high-lethality attempters were less affected by reward magnitude and based their fairness perceptions primarily on inequality. It is likely that the modulation of fairness perception by offer magnitude in controls reflects an implicit bias toward rewards. Such biases can be adaptive, akin to optimistic biases or illusions of control that are sometimes diminished in patients with mood disorders (“depressive realism”) (Alloy & Abramson, 1988). This bias, reflecting perceived action-reward contingencies (Matute, 1996), was attenuated in high-lethality suicide attempters. This may be due to the interference of the social emotional context (unfairness) with the processing of expected reward, as has been noted in neuroeconomic research. Delgado and colleagues (Delgado, Frank, & Phelps, 2005), for example, found that information about the opposing players' social reputation interfered with striatal reward responses during an economic exchange.
In addition, high-lethality attempters may continue to reject unfair offers, even of higher magnitude, because they may be less likely to empathize with the proposers and, hence, less likely to strategically forgive social unfairness. Forgiveness is associated with better interpersonal relations (Lawler-Row & Piferi, 2006) and greater emotional stability (Ashton, Paunonen, Helmes, & Jackson, 1998) – attributes in which high-lethality attempters display certain impairment. Unfair offers in the UG can elicit two distinct responses: forgiveness or punishment of the offender. When stakes are high, a forgiving responder may infer that high stakes compel proposers to act in self-interest, and accept an unfair offer -- a shift in behavior that could reflect “strategic” empathy. In the current study, the high-lethality attempters were the only group to not show a reliable effect of reduced retaliation when the stakes were high.
In this sample we had the opportunity to observe how personality and socioeconomic variables affected social punishment behavior. Our findings are consistent with previous work demonstrating associations between impulsivity and the tendency to reject inequitable offers (M. J. Crockett et al., 2010). However, impulsivity did not emerge as a significant mediator of the relationship between offer magnitude and rejection rates. There was an interesting, and not previously described, association between income and offer magnitude. Higher income was associated with a greater sensitivity to the reward at stake, indicating that these persons effectively maximize financial utility. Income did not, however, significantly predict the perception of inequality.
Social decision-making in suicide is a neglected area, and few studies have investigated age effects in social decision-making using tools such as the UG. Literature indicates that older adults may have higher “other-serving” motivations, make more “economically rational” decisions, and are more likely to avoid negative stimuli in reward-based learning than their younger counterparts (Bailey, Ruffman, & Rendell, 2013; Frank & Kong, 2008; Roalf, Mitchell, Harbaugh, & Janowsky, 2012). Beadle and colleagues hypothesized that compared to younger adults, older individuals will show more prosocial behavior by rejecting less offers in the UG (Beadle et al., 2012), as they put more emphasis on relationships than financial gains (Carstensen, Isaacowtiz, & Charles, 1999). While no age-related group differences were observed, this study did note that older adults with higher cognitive empathy were more likely to maximize financial gains (Beadle et al., 2012). Similarly, Harlé and Sanfey found no significant age difference in rejection rates, though older participants tended to reject more moderately unfair offers than younger counterparts (Harle & Sanfey, 2012). In contrast to the age-related “other serving” motivations, older adults' greater propensity to make “economically rational” decisions would lead to lower rejection rates in the UG.
Limitations and Strengths
These results extend earlier findings of decision-making deficits in suicide attempters (Dombrovski et al., 2010; Jollant et al., 2005), as well as our previous findings of emotion recognition deficits in older suicide attempters (Szanto et al., 2012). Yet, these findings hardly indicate a general impairment in social decision-making of high-lethality attempters. Although the UG models real-life decisions that involve weighing monetary gains and fairness, it is an artificial task. Our study focused on older adults with unipolar depression, as it is the most common antecedent of late-life suicide (Conwell et al., 1996); however, it is unclear to what extent our findings can be generalized to other psychiatric disorders. The detailed characterization of clinical presentation and suicide attempts, the use of depressed as well as non-depressed control groups, and the relatively large sample size all serve to strengthen our observations.
This study extends to social decision processes our previous observations, that suggest that the tendency to make disadvantageous decisions (failing to maximize rewards) is a common characteristic of those who are vulnerable to suicidal behavior (Dombrovski, Szanto, Clark, Reynolds, & Siegle, 2013). Our findings provide preliminary evidence that older high-lethality attempters, who most resemble suicide victims, make disadvantageous social decisions. The choices of comparison participants reflected a flexible, utilitarian cost-benefit analysis, punishing only when it was worth the cost. From an ethical perspective, high-lethality attempters seem to be missing the utilitarian perspective (where the morality of action is determined by its consequences) and instead show the deontological approach (principles such as fairness are valuable in themselves) (Tobler, Kalis, & Kalenscher, 2008). Our data are consistent with the idea that impaired social decision-making contributes to the poor psychosocial functioning observed in suicide attempters. The restricted age range and relatively small sample size in our study may have limited our ability to observe age effects. It is unclear whether accelerated age-related changes in decision competence contribute to interpersonal dysfunction and deficient problem-solving in suicidal older adults. The ability to make cognitively demanding decisions declines in old age even in non-demented elderly (Brown & Ridderinkhof, 2009; Denburg et al., 2007; Fein, McGillivray, & Finn, 2007). This is partly explained by an age-related decline in cognitive control (MacPherson, Phillips, & Della Sala, 2002) related to a disproportionate effect of aging on the prefrontal cortex relative to other brain areas (Raz et al., 1997), and to changes in other cognitive domains. Further studies including younger suicidal patients should investigate the contribution of age in general, and age-related cognitive changes in particular, to poor social decision-making in suicide.
Table 2b.
Correlation matrix of the variables in the model.
| Income | Fairness perception | EXIT | BIS Non-planning | IIP Ambivalence | High Lethality Status | Age | Female sex | |
|---|---|---|---|---|---|---|---|---|
| Income | 1.000 | |||||||
| Fairness perception | 0.291 | 1.000 | ||||||
| EXIT | 0.043 | −0.048 | 1.000 | |||||
| BIS Non-planning | −0.378 | −0.347 | 0.130 | 1.000 | ||||
| IIP Ambivalence | −0.063 | 0.006 | 0.278 | 0.353 | 1.000 | |||
| High Lethality Status | −0.226 | −0.295 | 0.253 | 0.544 | 0.348 | 1.000 | ||
| Age | 0.189 | −0.054 | 0.298 | −0.235 | 0.110 | −0.088 | 1.000 | |
| Female sex | −0.329 | −0.039 | −0.155 | 0.031 | −0.071 | −0.200 | −0.169 | 1.000 |
Acknowledgements
The authors would like to thank Swathi Gujral and Natalie Truty for their hard work on recruitment and assessments, and Jan Kalkus, for his help with data processing and plots.
This work was supported by the National Institute of Mental Health R01 MH085651 and K23 MH086620 and the National Institute on Aging K18 AG042166.
Footnotes
Declaration of Interest: None of the authors report any competing interests.
References
- Alloy LB, Abramson LY. Cognitive processes in depression. Guilford Press (New York, NY, US); New York, NY: Jan 1, 1988. Depressive realism: Four theoretical perspectives; pp. 223–265. 1988. [Google Scholar]
- Andersen S, Ertaç S, Gneezy U, Hoffman M, List JA. Stakes Matter in Ultimatum Games. American Economic Review. 2011;101(7):3427–3439. doi: 10.1257/aer.101.7.3427. [Google Scholar]
- Ashton MC, Paunonen SV, Helmes E, Jackson DN. Kin altruism, reciprocal altruism, and the Big Five personality factors. Evolution and Human Behavior. 1998;19:243–255. doi: http://dx.doi.org/10.1016/S1090-5138(98)00009-9. [Google Scholar]
- Bailey PE, Ruffman T, Rendell PG. Age-Related Differences in Social Economic Decision Making: The Ultimatum Game. Journals of Gerontology Series B-Psychological Sciences & Social Sciences. 2013;68(3):356–363. doi: 10.1093/geronb/gbs073. doi: 10.1093/geronb/gbs073. [DOI] [PubMed] [Google Scholar]
- Beadle JN, Paradiso S, Kovach C, Polgreen L, Denburg N, Tranel D. Effects of Age-related Differences in Empathy on Social Economic Decision-Making. International Psychogeriatrics. 2012;24(5):822–833. doi: 10.1017/S1041610211002547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beck AT, Beck R, Kovacs M. Classification of suicidal behaviors: I. Quantifying intent and medical lethality. American Journal of Psychiatry. 1975;132(3):285–287. doi: 10.1176/ajp.132.3.285. [DOI] [PubMed] [Google Scholar]
- Beck AT, Kovacs M, Weissman A. Assessment of suicidal intention: the Scale for Suicide Ideation. Journal of Consulting and Clinical Psychology. 1979;47(2):343–352. doi: 10.1037//0022-006x.47.2.343. [DOI] [PubMed] [Google Scholar]
- Beck AT, Shuyler D, Herman I. Development of suicidal intent scales. In: Beck AT, Resnik HLP, Lettieri DJ, editors. The prediction of suicide. Charles Press; Bowie, MD: 1974. pp. 45–56. [Google Scholar]
- Binswanger HP. Attitudes Toward Risk: Theoretical Implications of an Experiment in Rural India. The Economic Journal. 1981;91(364):867–890. [Google Scholar]
- Brown SBRE, Ridderinkhof KR. Aging and the neuroeconomics of decision making: A review. Cognitive, Affective and Behavioral Neuroscience. 2009;9(4):365–379. doi: 10.3758/CABN.9.4.365. doi: 10.3758/CABN.9.4.365. [DOI] [PubMed] [Google Scholar]
- Campbell-Meiklejohn D, Simsonen A, Scheel-Kruger J, Wohlert V, Gjerloff T, Frith CD, Moller A. In for a Penny, in for a Pound: Methylphenidate Reduces the Inhibitory Effect of High Stakes on Persistent Risky Choice. Journal of Neuroscience. 2012;32(38):13032–13038. doi: 10.1523/JNEUROSCI.0151-12.2012. doi: 10.1523/JNEUROSCI.0151-12.2012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carstensen LL, Isaacowtiz DM, Charles ST. Taking time seriously: A theory of socioemotional selectivity. American Psychologist. 1999;54:165–181. doi: 10.1037//0003-066x.54.3.165. [DOI] [PubMed] [Google Scholar]
- Conwell Y, Duberstein PR, Cox C, Herrmann JH, Forbes NT, Caine ED. Relationships of age and axis I diagnoses in victims of completed suicide: a psychological autopsy study. American Journal of Psychiatry. 1996;153(8):1001–1008. doi: 10.1176/ajp.153.8.1001. [DOI] [PubMed] [Google Scholar]
- Crockett MJ, Clark L, Lieberman MD, Tabibnia Golnaz, Robbins TW. Impulsive Choice and Altruistic Punishment are Correlated and Increase in Tandem with Serotonin Depletion. Emotion. 2010;10(6):855–862. doi: 10.1037/a0019861. doi: 10.1037/a0019861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crockett MJ, Clark L, Tabibnia G, Lieberman MD, Robbins TW. Serotonin modulates behavioral reactions to unfairness. Science. 2008;320(5884):1739. doi: 10.1126/science.1155577. doi: 1155577 [pii] 10.1126/science.1155577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crockett MJ, Clark L, Hauser MD, Robbins TW. Serotonin selectively influences moral judgement and behavior through effects on harm aversion. Proceedings of the National Academy of Sciences. 2010;5(107):17433–17438. doi: 10.1073/pnas.1009396107. doi: 10.1073/pnas.1009396107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Leo D, Padoani W, et al. Attempted and completed suicide in older subjects: results from the WHO/EURO Multicentre Study of Suicidal Behaviour. Int J Geriatr Psychiatry. 2001;16(3):300–310. doi: 10.1002/gps.337. [DOI] [PubMed] [Google Scholar]
- De Neys W, Novitskiy N, Geeraerts L, Ramautar JR, Wagemans J. Cognitive Control and Individual Differences in Economic Ultimatum Decision-Making. Public Library of Science ONE. 2011;6(11) doi: 10.1371/journal.pone.0027107. doi: 10.1371/journal.pone.0027107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Delgado MR, Frank RH, Phelps EA. Perceptions of moral character modulate the neural systems of reward during the trust game. Nature Neuroscience. 2005;8(11):1611–1618. doi: 10.1038/nn1575. doi: 10.1038/nn1575. [DOI] [PubMed] [Google Scholar]
- Denburg NL, Cole CA, Hernandez M, Yamada TH, Tranel D, Bechara A, Wallace RB. The orbitofrontal cortex, real-world decision making, and normal aging. Annals of the New York Academy of Sciences. 2007;1121:480–498. doi: 10.1196/annals.1401.031. doi: annals.1401.031 [pii] 10.1196/annals.1401.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Destoop M, Schrijvers D, Grave CD, Sabbe B, Bruijn E. Better to give than to take? Interactive social-decision making in severe major depressive disorder. Journal of Affective Disorders. 2012;137:98–105. doi: 10.1016/j.jad.2011.12.010. doi: 10.1016/j.jad.2011.12.010. [DOI] [PubMed] [Google Scholar]
- Dombrovski AY, Butters MA, Reynolds CF, 3rd, Houck PR, Clark L, Mazumdar S, Szanto K. Cognitive Performance in Suicidal Depressed Elderly: Preliminary Report. Am J Geriatr Psychiatry. 2008;16(2):109–115. doi: 10.1097/JGP.0b013e3180f6338d. doi: 16/2/109 [pii] 10.1097/JGP.0b013e3180f6338d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dombrovski AY, Clark L, Siegle GJ, Butters MA, Ichikawa N, Sahakian BJ, Szanto K. Reward/Punishment reversal learning in older suicide attempters. American Journal of Psychiatry. 2010;167(6):699–707. doi: 10.1176/appi.ajp.2009.09030407. doi: appi.ajp.2009.09030407 [pii] 10.1176/appi.ajp.2009.09030407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dombrovski AY, Szanto K, Clark L, Reynolds CF, Siegle GJ. Reward Signals, Attempted Suicide, and Impulsivity in Late-Life Depression. JAMA Psychiatry. 2013 doi: 10.1001/jamapsychiatry.2013.75. doi: 10.1001/jamapsychiatry.2013.75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dombrovski AY, Szanto K, Siegle GJ, Wallace ML, Forman SD, Sahakian B, Clark L. Lethal Forethought: Delayed Reward Discounting Differentiates High- and Low-Lethality Suicide Attempts in Old Age. Biological Psychiatry. 2011;70(2):138–144. doi: 10.1016/j.biopsych.2010.12.025. doi: S0006-3223(10)01327-2 [pii] 10.1016/j.biopsych.2010.12.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duberstein PR, Conwell Y, Conner KR, Eberly S, Evinger JS, Caine ED. Poor social integration and suicide: fact or artifact? A case-control study. Psychological Medicine. 2004;34(7):1331–1337. doi: 10.1017/s0033291704002600. [DOI] [PubMed] [Google Scholar]
- Erlangsen A, Zarit SH, Conwell Y. Hospital-Diagnosed Dementia and Suicide: A Longitudinal Study Using Prospective, Nationwide Register Data. American Journal of Geriatric Psychiatry. 2008;16(3):220–228. doi: 10.1097/JGP.0b013e3181602a12. doi: 16/3/220 [pii] 10.1097/JGP.0b013e3181602a12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Etkind M. …Or Not to Be: A collection of Suicide Notes. Riverhead Books; New York, NY: 1997. [Google Scholar]
- Fein G, McGillivray S, Finn P. Older adults make less advantageous decisions than younger adults: Cognitive and psychological correlates. Journal of the International Neuropsychological Society. 2007;13(3):480–489. doi: 10.1017/S135561770707052X. doi: Doi 10.1017/S135561770707052x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- First M, Spitzer RL, Gibbon M, Williams JBW. Structured clinical interview for DSM-IV Axis I Disorders - Patient Edition (SCID-I/P) Version 2.0 ed. 1995. [Google Scholar]
- Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research. 1975;12(3):189–198. doi: 10.1016/0022-3956(75)90026-6. [DOI] [PubMed] [Google Scholar]
- Frank MJ, Kong L. Learning to Avoid in Older Age. Psychology and Aging. 2008;23(2):392–398. doi: 10.1037/0882-7974.23.2.392. doi: 10.1037/0882-7974.23.2.392. [DOI] [PubMed] [Google Scholar]
- Gibbs LM, Dombrovski AY, Morse J, Siegle GJ, Houck PR, Szanto K. When the solution is part of the problem: problem solving in elderly suicide attempters. International Journal of Geriatric Psychiatry. 2009;24(12):1396–1404. doi: 10.1002/gps.2276. doi: 10.1002/gps.2276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gujral S, Dombrovski AY, Butters M, Clark L, Reynolds CF, 3rd, Szanto K. Impaired Executive Function in Contemplated and Attempted Suicide in Late Life. American Journal of Geriatric Psychiatry. 2012 doi: 10.1016/j.jagp.2013.01.025. doi: 10.1097/JGP.0b013e318265752f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guth W, Schmittberger R, Schwarze B. An experimental analysis of ultimatum bargaining. Journal of Economic Behavior & Organization. 1982;3(4):367–388. [Google Scholar]
- Hamilton M. A rating scale for depression. Journal of Neurology, Neurosurgery & Psychiatry. 1960;23:56–62. doi: 10.1136/jnnp.23.1.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harle KM, Sanfey AG. Social economic decision-making across the lifespan: An fMRI investigation. Neuropsychologia. 2012;50:1416–1424. doi: 10.1016/j.neuropsychologia.2012.02.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harrison KE, Dombrovski AY, Morse JQ, Houck P, Schlernitzauer M, Reynolds CF, 3rd, Szanto K. Alone? Perceived social support and chronic interpersonal difficulties in suicidal elders. International Psychogeriatrics. 2010;22(3):445–454. doi: 10.1017/S1041610209991463. doi: S1041610209991463[pii] 10.1017/S1041610209991463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holden RR, Delisle M. Factor Structure of the Reasons for Attempting Suicide Questionnaire (RASQ) with Suicide Attempters. Journal of Psychopathology and Behavioral Assessment. 2006;28(1):1–8. doi: 10.1007/s10862-006-4532-3. [Google Scholar]
- IBM . IBM SPSS Statistics for Windows, Version 19. Version 19.0 IBM Corp; Armonk, NY: Armonk, NY: 2010. [Google Scholar]
- Johansson-Stenman O, Mahmud M, Martinsson P. Does stake size matter in trust games? Economic Letters. 2005;88:365–369. [Google Scholar]
- Jollant F, Bellivier F, Leboyer M, Astruc B, Torres S, Verdier R, Courtet P. Impaired decision making in suicide attempters. American Journal of Psychiatry. 2005;162(2):304–310. doi: 10.1176/appi.ajp.162.2.304. [DOI] [PubMed] [Google Scholar]
- Keilp JG, Sackeim HA, Brodsky BS, Oquendo MA, Malone KM, Mann JJ. Neuropsychological dysfunction in depressed suicide attempters. American Journal of Psychiatry. 2001;158(5):735–741. doi: 10.1176/appi.ajp.158.5.735. [DOI] [PubMed] [Google Scholar]
- King-Casas B, Chiu PH. Understanding Interpersonal Function in Psychiatric Illness Through Multiplayer Economic Games. Biological Psychiatry. 2012;72(2):119–125. doi: 10.1016/j.biopsych.2012.03.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- King DA, Conwell Y, Cox C, Henderson RE, Denning DG, Caine ED. A neuropsychological comparison of depressed suicide attempters and nonattempters. Journal of Neuropsychiatry & Clinical Neurosciences. 2000;12(1):64–70. doi: 10.1176/jnp.12.1.64. [DOI] [PubMed] [Google Scholar]
- Kirby KN. Bidding on the future: Evidence against normative discounting of delayed rewards. Journal of Experimental Psychology-General. 1997;126(1):54–70. [Google Scholar]
- Kishida KT, King-Casas B, Montague PR. Neuroeconomic approaches to mental disorders. Neuron. 2010;67(4):543–554. doi: 10.1016/j.neuron.2010.07.021. doi: 10.1016/j.neuron.2010.07.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lawler-Row KA, Piferi RL. The forgiving personality: Describing a life well lived? Personality and Individual Differences. 2006;41(6):1009–1020. doi: 10.1016/j.paid.2006.04.007. [Google Scholar]
- Linehan Marsha M, Goodstein Judith L, Nielsen Stevan L, Chiles John A. Reasons for staying alive when you are thinking of killing yourself: the reasons for living inventory. Journal of consulting and clinical psychology. 1983;51(2):276. doi: 10.1037//0022-006x.51.2.276. [DOI] [PubMed] [Google Scholar]
- Liu RT, Vassileva J, Gonzalez R, Martin EM. A Comparison of Delay Discounting Among Substance Users With and Without Suicide Attempt History. Psychology of Addictive Behaviors. 2012 doi: 10.1037/a0027384. doi: 10.1037/a0027384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacArthur Network on SES and Health MacArthur Sociodemographic Questionnaire. http://www.macses.ucsf.edu/research/socialenviron/sociodemographic.php.
- MacKinnon DP, Fairchild A, Fritz MS. Mediation Analysis. Annual Review of Psychology. 2007;58:593. doi: 10.1146/annurev.psych.58.110405.085542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacPherson SE, Phillips LH, Della Sala S. Age, executive function and social decision making: A dorsolateral prefrontal theory of cognitive aging. Psychology and Aging. 2002;17(4):598–609. doi: 10.1037/0882-7974.17.4.598. [PubMed] [Google Scholar]
- Matute H. Illusion of control: Detecting response-outcome independence in analytic but not in naturalistic conditions. Psychological Science. 1996;7(5):289–293. doi: DOI 10.1111/j.1467-9280.1996.tb00376.x. [Google Scholar]
- McGirr A, Dombrovski AY, Butters M, Clark L, Szanto K. Deterministic learning and attempted suicide among older depressed individuals: Cognitive assessment using the Wisconsin Card Sorting Task. Journal of Psychiatric Research. 2012;46(2):226–232. doi: 10.1016/j.jpsychires.2011.10.001. doi: http://dx.doi.org/10.1016/j.jpsychires.2011.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGirr A, Renaud J, Bureau A, Seguin M, Lesage A, Turecki G. Impulsive-aggressive behaviours and completed suicide across the life cycle: a predisposition for younger age of suicide. Psychological Medicine. 2008;38(3):407–417. doi: 10.1017/S0033291707001419. doi: S0033291707001419 [pii] 10.1017/S0033291707001419. [DOI] [PubMed] [Google Scholar]
- Miller MD, Paradis CF, Houck PR, Mazumdar S, Stack JA, Rifai AH, Reynolds CF., 3rd Rating chronic medical illness burden in geropsychiatric practice and research: application of the Cumulative Illness Rating Scale. Psychiatry Research. 1992;41(3):237–248. doi: 10.1016/0165-1781(92)90005-n. [DOI] [PubMed] [Google Scholar]
- Morse JQ, Pilkonis PA. Screening for personality disorders. J Personal Disord. 2007;21(2):179–198. doi: 10.1521/pedi.2007.21.2.179. doi: 10.1521/pedi.2007.21.2.179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus User's Guide. version 7.0 Muthén and Muthén; Los Angeles, CA: 2012. [Google Scholar]
- O'Carroll PW, Berman AL, Maris RW, Moscicki EK, Tanney BL, Silverman MM. Beyond the Tower of Babel: a nomenclature for suicidology. Suicide & Life-Threatening Behavior. 1996;26(3):237–252. [PubMed] [Google Scholar]
- Patton JH, Stanford MS, Barratt ES. Factor structure of the Barratt impulsiveness scale. Journal of Clinical Psychology. 1995;51(6):768–774. doi: 10.1002/1097-4679(199511)51:6<768::aid-jclp2270510607>3.0.co;2-1. [DOI] [PubMed] [Google Scholar]
- Pillutla MM, Murnighan JK. Unfairness, anger, and spite: emotional rejections of unfair offers. Organizational Behavior and Human Decision Processes. 1996;68:208–224. [Google Scholar]
- Preacher Kristopher J., Zyphur Michael J., Zhang Zhen. A general multilevel SEM framework for assessing multilevel mediation. Psychological Methods. 2010;15(3):209–233. doi: 10.1037/a0020141. [DOI] [PubMed] [Google Scholar]
- Rabe-Hesketh S, Skrondal A, Pickles A. U. C. Berkeley Division of Biostatistics Working Paper Series, Working Paper 160. 2004. GLLAMM Manual. [Google Scholar]
- Raz N, Gunning FM, Head D, Dupuis JH, McQuain J, Briggs SD, Acker JD. Selective aging of the human cerebral cortex observed in vivo: differential vulnerability of the prefrontal gray matter. Cereb Cortex. 1997;7(3):268–282. doi: 10.1093/cercor/7.3.268. [DOI] [PubMed] [Google Scholar]
- Richard-Devantoy S, Annweiler C, Beauchet O, Camus V, Le Gall D, Garre JB. P03- 470 - Cognitive inhibition in suicidal depressed elderly. European Psychiatry. 2011;26(1):1640. doi: 10.4088/JCP.10l06797. doi: http://dx.doi.org/10.1016/S0924-9338(11)73344-2. [DOI] [PubMed] [Google Scholar]
- Richard-Devantoy S, Jollant F, Kefi Z, Turecki G, Olie JP, Annweiler C, Le Gall D. Deficit of cognitive inhibition in depressed elderly: a neurocognitive marker of suicidal risk. Journal of Affective Disorders. 2012;140(2):193–199. doi: 10.1016/j.jad.2012.03.006. [DOI] [PubMed] [Google Scholar]
- Roalf DR, Mitchell SH, Harbaugh WT, Janowsky J, S. Risk, Reward, and Economic Decision Making in Aging. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences. 2012;67B(3):289–298. doi: 10.1093/geronb/gbr099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Royall DR, Mahurin RK, Gray KF. Bedside assessment of executive cognitive impairment: the executive interview. Journal of American Geriatrics Society. 1992;40(12):1221–1226. doi: 10.1111/j.1532-5415.1992.tb03646.x. [DOI] [PubMed] [Google Scholar]
- Szanto K, Dombrovski AY, Sahakian BJ, Mulsant BH, Houck PR, Reynolds CF, 3rd, Clark L. Social Emotion Recognition, Social Functioning, and Attempted Suicide in Late-Life Depression. American Journal of Geriatric Psychiatry. 2012;20(3):257–265. doi: 10.1097/JGP.0b013e31820eea0c. doi: 10.1097/JGP.0b013e31820eea0c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tabibnia Golnaz, Satpute Ajay B., Lieberman Matthew D. The Sunny Side of Fairness: Preference for Fairness Activates Reward Circuitry (and Disregarding Unfairness Activates Self-Control Circuitry) Psychological Science (Wiley-Blackwell) 2008;19(4):339–347. doi: 10.1111/j.1467-9280.2008.02091.x. doi: 10.1111/j.1467-9280.2008.02091.x. [DOI] [PubMed] [Google Scholar]
- Tobler PN, Kalis A, Kalenscher T. The role of moral utility in decision making: An interdisciplinary framework. Cognitive, Affective & Behavioural Neuroscience. 2008;8(4):390–401. doi: 10.3758/CABN.8.4.390. doi: 10.3758/CABN.8.4.390. [DOI] [PubMed] [Google Scholar]
- Unoka Z, Seres I, Aspan N, Bodi N, Keri S. Trust game reveals restricted interpersonal transactions in patients with borderline personality disorder. Journal of Personality Disorders. 2009;23(4):399–409. doi: 10.1521/pedi.2009.23.4.399. [DOI] [PubMed] [Google Scholar]
- Wallisch P, Lusignan M, Benayoun M, Baker TI, Dickey AS, Hatsopoulos NG. Matlab for Neuroscientists: An Introduction to Scientific Computing in Matlab. Academic Press; Burlington, MA; San Diego, CA; London, UK: 2009. [Google Scholar]
- Westheide J, Quednow BB, Kuhn KU, Hoppe C, Cooper-Mahkorn D, Hawellek B, Wagner M. Executive performance of depressed suicide attempters: the role of suicidal ideation. European Archives of Psychiatry and Clinical Neuroscience. 2008;258(7):414–421. doi: 10.1007/s00406-008-0811-1. doi: 10.1007/s00406-008-0811-1. [DOI] [PubMed] [Google Scholar]
- Wilson ST, Stanley B, Oquendo MA, Goldeberg P, Zalsman G, Mann JJ. Comparing impulsiveness, hostility, and depression in borderline personality disorder and bipolar II disorder. Journal of Clinical Psychiatry. 2007;68(10):1533–1539. doi: 10.4088/jcp.v68n1010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization Suicide prevention. 2005 from http://www.who.int/mental_health/prevention/suicide/suicideprevent/en/