

Abstract
Calcified amorphous tumor of the heart (cardiac CAT) is a rare non-neoplastic cardiac mass that mimics malignancy on imaging and can cause symptoms due to flow obstruction or embolization of calcific fragments. We report a 57-year-old female with multiple medical problems affected by cardiac CAT. The echocardiogram showed a 2 x 1.7 cm right atrial mass. Under the clinical diagnosis of cardiac myxoma, a mass resection was performed. Microscopic examination of the resected mass showed nodular calcified amorphous debris with admixed degenerated fibrin and focal chronic inflammation. At the 1-year follow-up, the patient was free of disease.
We performed a literature review of 16 previously reported cases. Histologically, a cardiac CAT consists of calcification and eosinophilic amorphous material in the background of dense collagenous fibrous tissue. A review of these cases shows a wide range of age at diagnosis and slight female predominance. The patients are either asymptomatic at presentation or complain of shortness of breath. The tumors have been found in all chambers of the heart, most commonly in the left ventricle. The sizes of the tumors range from 0.17 to 4 cm, with 62.5% of the tumors being mobile. Among the nine cases with documented follow-up study, all but one was free of disease and only one case of relapse was recorded. In conclusion, cardiac CATs are frequently asymptomatic at presentation, size is equal to or less than 4 cm, they can be located in all four chambers and are usually mobile, and they may relapse when not completely excised.
Keywords: calcified tumor, cardiac tumor, non-neoplastic


Introduction
Calcified amorphous tumor of the heart (cardiac CAT) is a rare non-neoplastic cardiac tumor that may be confused with a primary cardiac neoplasm, such as a cardiac myxoma, in clinical presentation. The tumor may be an incidental finding on imaging, or imaging may have been warranted due to symptoms of flow obstruction or embolization of calcific fragments. Here we report a case of a cardiac CAT and describe its characteristics. A review of the literature of 16 previously reported cases is also included.1-15
Clinical and Radiologic Findings
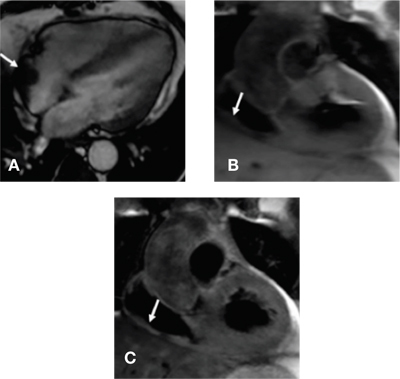
A 57-year-old female patient with multiple medical problems was admitted to the hospital due to complaints of fever, shortness of breath, and cough. An extensive work-up was performed, and she was treated for tracheobronchitis or early pneumonia. The work-up had included an echocardiogram, and the imaging showed a 2 x 1.7 cm right atrial mass. Cardiac magnetic resonance (CMR) imaging showed a structure in the posterior aspect of the right atrium that appeared to be broad-based with extension into the right atrium. It moved with the right atrial wall contraction, but there was no prolapse through the tricuspid valve into the right ventricle and no obvious stalk was identified (Fig 1).
Figure 1.
Cardiac MRI: Image A is four-chamber steady state free precision showing mass in the posterior aspect of the right atrium that appears to be broad-based with extension into the right atrium (white arrow). Images B and C are T1 and T2 turbo-spin echo images showing the mass in the right atrium has intermediate intensity (white arrow).
After completion of the cardiac MRI and a cardiac catheterization study, the patient underwent surgical resection of the mass under the clinical diagnosis of cardiac myxoma. The patient was successfully treated and discharged home, and she is free of disease after 1 year of postsurgical follow-up.
Gross and Histopathologic Findings of Cardiac Mass
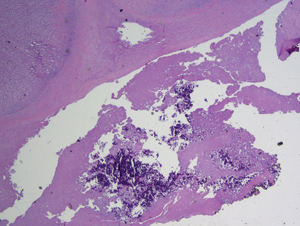
Gross examination revealed a 1.9 x 1.3 x 0.8 cm tan-pink piece of soft tissue mass with a glistening, smooth pericardium on one side and scattered gritty calcifications on the opposite side. Also submitted in the same container were several tan-pink muscle fragments (1.0 x 0.9 x .5 cm in aggregate, ranging from 0.2 cm to 1.1 cm in greatest dimension). Microscopic examination of the cardiac mass showed nodular calcified amorphous debris with admixed degenerated fibrin and focal chronic inflammation (Figure 2). This organizing fibrinous process extended to the periphery of the sampled tissue; however, it did not involve the underlying myocardial tissue or the pericardium. No frank necrosis, pleomorphism, or mitoses was seen.
Figure 2.
Cardiac CAT. Nodular calcified amorphous debris with admixed degenerated fibrin (hematoxylin and eosin stain; original magnification x20)
Discussion
Cardiac CAT is a rare entity first described by Reynolds et al. in 1997. They reported 11 intracardiac masses that had microscopic features of calcification and amorphous fibrinous material and suggested the current nomenclature of cardiac CAT to describe this entity.16
Histologically, a cardiac CAT consists of calcification and eosinophilic amorphous material in the background of dense collagenous fibrous tissue. There is a slight female predominance (62.5%) and wide range of age at diagnosis (18-78 years), with the mean age of presentation at 51 years (Table 1). The patient in our case was slightly older at age 57. The patients are mostly asymptomatic at presentation (43.75%). The masses may cause symptoms related to obstruction or embolization such as shortness of breath (31.25%), syncope (12.5%), and central retinal arterial occlusion (6.25%). A cardiac mass may induce recurrent ventricular arrhythmia (6.25%); however, the association between cardiac CAT and ventricular tachycardia is unknown.6 Our patient had multiple medical problems including rheumatoid arthritis, hypertension, diabetes, transient ischemic attacks, Arnold-Chiari malformation, fibromyalgia, microcytic anemia, morbid obesity, hyperlipidemia, reflux esophagitis, chronic kidney disease, and autoimmune hepatitis. Since there has been no close association with the above-mentioned medical problems in the literature, more cases are required to positively state any causal relationship with other medical conditions.
Table 1.
Literature review of cardiac CAT cases.
| Case | Author | Site | Age | Sex | Symptoms | Size (cm) | Mobile |
| 1 | Lewin | RV | 60 | F | Syncope | 4 x 3 x 2.5 | No |
| 2 | Fealey | RV | 20 | F | Shortness of breath and pulmonary embolism | 4 x 2.2 x 1.8 | n/a |
| 3 | Ho | LV | 44 | M | Shortness of breath | n/a | n/a |
| 4 | Gutierrez-Barrios | RA | 35 | M | None | 3.3 x 2.3 | No |
| 5 | Flynn | RV | n/a | M | Syncope | 3 x 2 x 1 | n/a |
| 6 | Habib | LV | 58 | F | Ventricular tachycardia | n/a | n/a |
| 7 | Sousa | tricuspid | 17 | M | None | 2.2 x 1.4 | n/a |
| 8 | Kubota | mitral | 64 | F | None | 2.7 x 0.3 | n/a |
| 9 | Kubota | LV | 44 | M | None | 2.8 x 0.5 | Yes |
| 10 | Gupta | RA | 40 | F | Shortness of breath | 3 x 3 x 1.5 | n/a |
| 11 | Vlasseros | LV | 65 | F | Left central retinal arterial occlusion | 2.6 x 1.7 x .5 | n/a |
| 12 | Greaney | mitral | 69 | F | Shortness of breath, left cerebral infarct | 2 | Yes |
| 13 | Ananthakrishna | LV | 45 | F | Shortness of breath | 4 x 3.5 x 2 | n/a |
| 14 | Lin | LA | 74 | F | None | 2.7 x 1.4 | Yes |
| 15 | Nishigawa | mitral | 78 | F | None | 0.17 | Yes |
| 16 | Kawata | mitral | 59 | M | None | 2.8 x 0.6 | Yes |
RV: right ventricle; LV: left ventricle; RA: right atrium; LA: left atrium; n/a: not available.
To date, the tumors have been found in all chambers of the heart but predominantly in the left ventricle (31.25%) and mitral valve (25%). Only 12.5% of the cases have cardiac CAT in the right atrium as seen in our case. Tumor sizes range from 0.17 to 4 cm in their greatest dimension, with the mean size of 2.8 cm. Our case was slightly smaller at 2 cm in dimension. Among the documented cases, 62.5% of the tumors were mobile. Among the nine cases with documented follow-up study, all but one were free of disease after surgical excision and only one case of relapse was recorded. In the case of relapsed cardiac CAT, the patient underwent resection of a right ventricular mass. However, intraoperative transesophageal echocardiogram demonstrated residual tumor. The tumor showed enlargement at 2 years after initial resection,2 requiring a re-resection of the mass. Our patient is alive and well without recurrence after resection of the mass.
Conclusion
Cardiac CAT is a non-neoplastic cardiac tumor of unknown etiology. The literature review highlights that the tumor is commonly an incidental finding and the treatment of choice is complete surgical resection. In summary, we report a case of CAT in the right atrium in a 57-year-old female who was successfully treated by a complete resection of the mass.
Funding Statement
Funding/Support: The authors have no funding disclosures.
Footnotes
Conflict of Interest Disclosure: The authors have completed and submitted the Methodist DeBakey Cardiovascular Journal Conflict of Interest Statement and none were reported.
References
- 1.Lewin M, Nazarian S, Marine JE, Yuh DD, Argani P, Halushka MK. Fatal outcome of a calcified amorphous tumor of the heart (cardiac CAT). Cardiovasc Pathol. 2006 Sep-Oct;15(5):299–302.. doi: 10.1016/j.carpath.2006.05.004. [DOI] [PubMed] [Google Scholar]
- 2.Fealey ME, Edwards WD, Reynolds CA, Pellikka PA, Dearani JA. Recurrent cardiac calcific amorphous tumor: The CAT had a kitten. Cardiovasc Pathol. 2007 Mar-Apr;16(2):115–8.. doi: 10.1016/j.carpath.2006.09.002. [DOI] [PubMed] [Google Scholar]
- 3.Ho HH, Min JK, Lin F, Wong SC, Bergman G. Images in cardiovascular medicine. Calcified amorphous tumor of the heart. Circulation. 2008 Mar 4;117(9):e171–2.. doi: 10.1161/CIRCULATIONAHA.107.730838. [DOI] [PubMed] [Google Scholar]
- 4.Gutierrez-Barrios A, Muriel-Cueto P, Lancho-Novillo C, Sancho-Jaldon M. Calcified amorphous tumor of the heart. Rev Esp Cardiol. 2008 Aug;61(8):892–3.. [PubMed] [Google Scholar]
- 5.Flynn A, Mukherjee G. Calcified amorphous tumor of the heart. Indian J Pathol Microbiol. 2009 Jul-Sep;52(3):444–6.. doi: 10.4103/0377-4929.55026. [DOI] [PubMed] [Google Scholar]
- 6.Habib A, Friedman PA, Cooper LT, Suleiman M, Asirvatham SJ. Cardiac calcified amorphous tumor in a patient presenting for ventricular tachycardia ablation: intracardiac echocardiogram diagnosis and management. J Interv Card Electrophysiol. 2010 Dec;29(3):175–8.. doi: 10.1007/s10840-009-9418-3. [DOI] [PubMed] [Google Scholar]
- 7.Sousa JS, Tanamati C, Marcial MB, Stolf NA. Calcified amorphous tumor of the heart: case report. Rev Bras Cir Cardiovasc. 2011 Jul-Sep;26(3):500–3.. doi: 10.5935/1678-9741.20110031. [DOI] [PubMed] [Google Scholar]
- 8.Kubota H, Fujioka Y, Yoshino H, Koji H, Yoshihara K, Tonari K, et al. Cardiac swinging calcified amorphous tumors in end-stage renal failure patients. Ann Thorac Surg. 2010 Nov;90(5):1692–4.. doi: 10.1016/j.athoracsur.2010.04.097. [DOI] [PubMed] [Google Scholar]
- 9.Gupta R, Hote M, Ray R. Calcified amorphous tumor of the heart in an adult female: a case report. J Med Case Rep. 2010 Aug 19;4 doi: 10.1186/1752-1947-4-278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Vlasseros I, Katsi V, Tousoulis D, Tsiachris D, Bousiotou A, Souretis G, et al. Visual loss due to cardiac calcified amorphous tumor: a case report and brief review of the literature. Int J Cardiol. 2011 Nov 3;152(3):e56–7.. doi: 10.1016/j.ijcard.2010.12.005. [DOI] [PubMed] [Google Scholar]
- 11.Greaney L, Chaubey S, Pomplun S, St Joseph E, Monaghan M, Wendler O. Calcified amorphous tumour of the heart: Presentation of a rare case operated using minimal access cardiac surgery. BMJ Case Rep. 2011;2011 doi: 10.1136/bcr.02.2011.3882. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ananthakrishna R, Nanjappa MC, Kamalapurkar G, Bhat P, Panneerselvam A, Chander N, et al. Cardiac tumour in a patient with rheumatic heart disease. BMJ Case Rep. 2011 Sep 8 doi: 10.1136/bcr.04.2011.4146. 2011:10.1136/bcr.04.2011.4146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lin YC, Tsai YT, Tsai CS. Calcified amorphous tumor of left atrium. J Thorac Cardiovasc Surg. 2011 Dec;142(6):1575–6.. doi: 10.1016/j.jtcvs.2011.06.003. [DOI] [PubMed] [Google Scholar]
- 14.Nishigawa K, Takiuchi H, Kubo Y, Masaki H, Tanemoto K. Calcified amorphous tumor: three-dimensional transesophageal echocardiography. Asian Cardiovasc Thorac Ann. 2012 Jun;20(3) doi: 10.1177/0218492311423071. [DOI] [PubMed] [Google Scholar]
- 15.Kawata T, Konishi H, Amano A, Daida H. Wavering calcified amorphous tumour of the heart in a haemodialysis patient. Interact Cardiovasc Thorac Surg. 2013 Feb;16(2):219–20.. doi: 10.1093/icvts/ivs430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Reynolds C, Tazelaar HD, Edwards WD. Calcified amorphous tumor of the heart (cardiac CAT). Hum Pathol. 1997 May;28(5):601–6.. doi: 10.1016/s0046-8177(97)90083-6. [DOI] [PubMed] [Google Scholar]