

Abstract
Hepatitis E virus (HEV) infection is an important public health concern in many developing countries, causing waterborne outbreaks as well as sporadic autochthonous hepatitis. HEV is mainly transmitted by the fecal–oral route in endemic areas through drinking of contaminated water. However, zoonotic transmission from animal reservoirs to humans has also been suggested. Three additional routes of HEV transmission have been proposed to occur: blood borne, human to human, and vertical transmission from mother to child. Acute HEV infection is usually diagnosed by detecting specific anti-HEV antibodies. However, the performance of the available assays in different settings is not optimal. Analysis of HEV ribonucleic acid in biologic specimens such as stools, serum, and liver biopsy by using nucleic acid amplification techniques is also employed. Nonetheless, additional consensus regarding the best technologies suitable for serosurveys and diagnosis of acute HEV infection is also needed. This review article summarizes the current status of HEV infection end epidemiology with particular emphasis in transmission, diagnosis, and clinical management.
Keywords: HEV, epidemiology, clinical features, routes of infection
Introduction
Hepatitis E virus (HEV) is the etiological agent of acute hepatitis E, an infection considered to be endemic in many developing countries in Africa and Asia.1 HEV is transmitted primarily by the fecal–oral route and has been reported to occur as large waterborne epidemics and small outbreaks in developing areas.2–4 However, over the last decade, it has occurred in several high income countries, in an increasing number of sporadic locally acquired cases in which it is often not possible to establish the route of acquisition of infection.5,6 Besides humans, HEV strains have also been isolated from several other animal species including wild and domestic swine, deer, chicken, rat, ferret, and rabbit.7–9 Hepatitis E is considered a zoonotic infection with pig and wild boar serving as the main reservoir for human infections. The global burden of HEV infection is thought to be due to sporadically transmitted hepatitis E cases rather than to cases due to hepatitis E epidemic. It has been estimated that two billion people, representing one third of the world’s population, live in endemic areas for HEV and, therefore, are at risk of infection.10 It is not clear whether HEV incidence rates in nonendemic areas are actually changing or if more cases are detected through increased surveillance.11
HEV typically causes an acute and self-limiting infection in immune-competent individuals, with low mortality rates in general, though fulminant hepatitis and high mortality are described in some settings. However, in the last few years, unknown aspects regarding HEV infection have been uncovered in nonendemic and industrialized countries, such as the possibility of the disease becoming chronic in transplant patients and the immunocompromised.12 Chronic HEV infection in these individuals is indeed an emerging and significant clinical problem.
This review article summarizes recent advancements in the knowledge of the biology and epidemiology of HEV, with special emphasis on the transmission routes, diagnosis, and management of the infection.
Biology and molecular virology
HEV is currently classified as a member of the genus Hepevirus in the family Hepeviridae.13,14 It is a small, nonenveloped, spherical particle of approximately 32–34 nm in diameter and has a single-stranded, positive sense ribonucleic acid (RNA) genome surrounded by an icosahedral capsid.1
HEV genome organization
The HEV genome is ∼7,200 nucleotides (nt) in length, consisting of a short 5′ untranslated region (27–35 nt), three discontinuous and partially overlapping open reading frames (ORFs) 1, 2, and 3, and a short 3′ untranslated region (65–74 nt) that is terminated by a polyadenylated tract (Figure 1). The capped 5′ end, essential for viral infectivity, and the 3′ end of the viral genome are noncoding regions and cis-acting elements involved in the regulation of viral replication and translation.15,16
Figure 1.
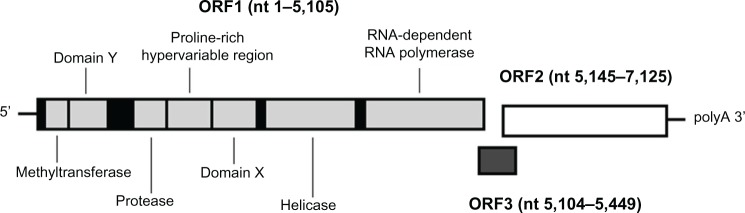
Organization of the hepatitis E virus genome.
Notes: Scheme showing the organization of the three viral open reading frames (ORFs); ORF1 encodes a nonstructural polyprotein comprising a methyltransferase, Domain Y (nonfunction assigned), papain-like protease, proline-rich hypervariable region (HVR, in text), Domain X (nonfunction assigned), RNA helicase, and an RNA-dependent RNA polymerase; ORF2 encodes the capsid protein and ORF3 encodes a small phosphoprotein; nucleotide positions are relative to the genotype 1 Burmese SAR-55 isolate.
Abbreviations: RNA, ribonucleic acid; nt, nucleotides.
ORF1, the largest coding unit, encompassing approximately two thirds of the viral genome, is located at the 5′ end and is approximately 5,000 nt in length. This region is involved in viral replication and protein processing, and it encodes nonstructural proteins including putative methyltransferase, guanylyl transferase, papain-like cysteine protease, RNA helicase, and RNA-dependent RNA polymerase.17,18 Also, some uncharacterized domains homologous to other animal and plant positive-strand RNA viruses have been identified in the ORF1.16 The hypervariable region, a noncoding region within ORF1 that displays substantial genetic diversity, was recently proposed to modulate the efficiency of HEV replication.19 Notably, the differences in the genome size among different HEV strains are confined mainly to this region.20
The viral ORF2 encodes the viral capsid protein of 660 amino acids that encapsidates the viral RNA genome.16 Capsid is the only structural protein and was shown to assemble into a highly structured multimer (60 copies).21,22
ORF3 overlaps the other two ORFs and encodes a small phosphoprotein of 123 amino acids that may cooperate in replication and cytoskeleton synthesis,23,24 and it is thought to interact with cellular mitogen-activated protein kinase phosphatase and other extracellular kinases, promoting cell survival through activation of intracellular signaling pathways.25
Genetic variability
Although a single serotype has been proposed,26 extensive genomic diversity has been observed among HEV isolates.23 Human infecting HEV sequences have been classified into four major genotypes (1–4) according to analysis of the complete genome sequence and/or variable partial HEV genomic regions within the ORF1 and ORF2.27–29 However, the existence of a new HEV genotype infecting wild boar was recently been proposed.30 This, together with the increasing number of HEV and HEV-like sequences published in the last few years, which increase the number of potential new genotypes or genetic groups, brought into question the current system of classification within the Hepevirus genus.31
According to the currently accepted system of classification, the four major HEV genotypes are further subclassified into subtypes, defined on the basis of five different phylogenetic reconstructions: 5′ ORF1, 3′ ORF1, 5′ ORF2, 3′ ORF2, and complete genome.28
HEV genotype 1 sequences are divided into five subtypes, 1a–e, and genotype 2 into two subtypes, 2a and 2b.28 Genotype 1 is responsible for most endemic and epidemic cases of HEV infection in Asia and has been also detected in small outbreaks from Cuba and sporadic cases from Venezuela and Uruguay, respectively1,32,33 (Figure 2). Genotype 2 is prevalent in Mexico (probably subtype 2a, based on the characterization of a single strain) and Africa (subtype 2b).1 By contrast, genotype 3 is widely distributed, and sequences of this genotype are extremely diverse,23 comprising ten (3a–j) subtypes. Genotype 4 sequences, even though they display high heterogeneity (subtypes 4a–g), are geographically restricted to Asia and Central Europe (Figure 2).28,34 Recently, this subtype-based classification has also been challenged by Smith et al, in which an exhaustive molecular and phylogenetic analysis revealed several inconsistencies with the currently defined subtype designations.35 This observation was also supported by other similar studies.31
Figure 2.
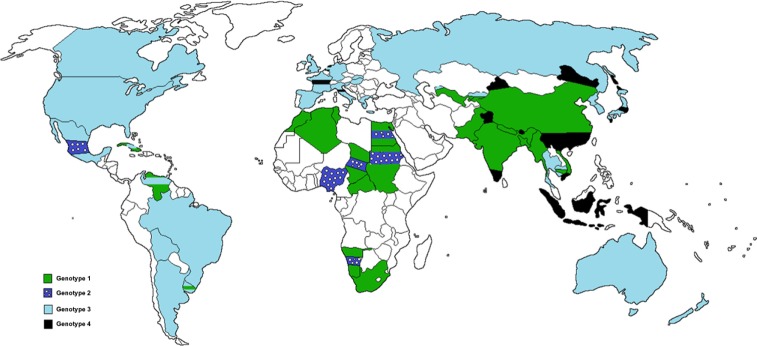
Geographical distribution of hepatitis E virus genotypes.
Notes: Genotypes 1 and 2 consist of epidemic strains reported in Asia and several Latin American countries and Africa and Mexico, respectively; genotypes 3 and 4 comprise of zoonotic strains and have been isolated from sporadic cases of acute human hepatitis E viral infection and from several animal reservoirs, particularly domestic and wild pigs and deer; genotype 3 is distributed worldwide in human and pigs while genotype 4 was reported in East Asia and Central Europe.
HEV epidemiology
HEV is considered hyperendemic in many developing countries such as India, Bangladesh, and the People’s Republic of China, where major waterborne outbreaks occur, generally associated to isolates of genotypes 1 and 2. In turn, the case of Mexico, a country which is usually qualified also as highly endemic, is questionable; hepatitis E outbreaks have never been reported again in the last two decades. Genotype 2 appears to be anthroponotic since it has been isolated exclusively from human cases while genotype 1 infects mainly humans but also has been detected in pigs.28,36,37
In developed and nonendemic countries, occurrence of HEV infection has usually been associated with travelers returning from endemic countries.38 Recently, accumulating lines of evidence indicate that sporadic and locally acquired cases of genotype 3 and 4 HEV infection also occurs among individuals from industrialized countries who have no history of travel to endemic areas.1,7,39–41 In fact, in the last decade, the number of autochthonous cases of genotype 3 and 4 infection reported in developed areas has increased dramatically, and evidence for animal reservoirs and zoonotic transmission has been brought to light. HEV strains of these zoonotic genotypes have been found in humans and other animal reservoirs including swine, wild boar, and deer.9,42–45 Most episodes of zoonotic transmission associated to genotypes 3 and 4 are foodborne and have been linked to ingestion of raw or undercooked meat from wild and domestic pigs and deer.46,47 Table 1 summarizes epidemiological features of the four recognized human HEV genotypes.
Table 1.
Epidemiological and clinical features of the four human hepatitis E virus genotypes
| Genotype | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Host | Human; also isolated from pigs | Human | Human, swine, and other mammalian species | |
| Route of transmission | Waterborne (fecal contaminated water); human to human; maternofetal; probably zoonotic (genotype 1) | Zoonotic: mainly via consumption of raw or undercooked contaminated animal meat; environmental (shellfish); to date environmental shellfish has been reported exclusively for genotype 3; blood transfusion | ||
| Geographical distribution | Asia and Latin America (Cuba, Venezuela, and Uruguay) | Mexico and several African countries | Worldwide | East Asia and Central Europe |
| Epidemiological features | Endemic in Asia and Cuba; causes outbreaks and sporadic cases in developing countries; more common in young people and travelers | Endemic in Mexico? Causes outbreaks and sporadic cases in developing countries; more common in young people | Causes autochthonous sporadic cases in developed and nonendemic areas; highest attack rate in middle-aged and elderly men; higher overall mortality rate compared to genotype 1 | |
| Clinical presentation in humans | Mostly asymptomatic infections; acute self-limited hepatitis; high mortality in pregnancy and in patients with underlying chronic liver disease | Mostly asymptomatic infections; moderately severe acute self-limited hepatitis | Moderately severe acute self-limited hepatitis; asymptomatic; infection may lead to chronicity in solid organ transplant recipients (to date, only reported for genotype 3) and immunocompromised patients | |
Recent advancements in the understanding of global epidemiology of HEV infection reveals a picture quite more complex than initially assumed. Nevertheless, distinct epidemiological patterns are clearly distinguished in endemic regions compared to nonendemic areas.
Endemic countries were shown to have an overall HEV prevalence of 25% of all non-A, non-B acute hepatitis cases,48 and while the anti-HEV immunoglobulin (Ig)G prevalence among healthy blood donors may be as high as 45% in some hyperendemic countries, reports from industrialized countries, although highly variable from study to study, show prevalence ranging from 1% to 4%.49
Additional dramatic differences were observed in the size and frequency of outbreaks, overall attack rates, and duration of viremia.49 These issues are extensively reviewed by Kumar et al.9
Clinical features
Historically, data on clinical manifestations of hepatitis E are available from basically two sources of evidence: 1) reports of HEV infection outbreaks and sporadic disease from highly endemic areas and 2) case reports and case series from developed nonendemic countries. However, the recent observation that HEV infection may progress to chronicity in transplant and immunocompromised patients has increased the complexity of the disease and has rendered it to be a public health problem of major concern.15 Clinical outcomes associated with HEV infection from the two sources are reviewed here. In addition, recent advancements in the comprehension of the chronic course of HEV infection and the identification of its distinct clinical features are also discussed.
HEV infection in highly endemic regions
In moderate and high endemic areas, HEV infection is the most common cause of acute viral hepatitis.12,50 The infection varies in severity, ranging from subclinical to fulminant hepatitis. Most acute HEV hepatitis cases have a clinically silent course, and patients clear the virus rapidly.51,52 Symptomatic disease is reported in about 20% of patients and is observed most frequently in youths and adults (14–40 years old).50 Symptoms associated with HEV infection are moderately severe and generally self-limiting, with case fatality rates of 0.5%–4%. In symptomatic cases, the incubation period ranges from 2 to 8 weeks (mean 40 days), and initial symptoms are mainly unspecific. Typically, these include flu-like myalgia, arthralgia, anorexia, hepatomegaly, fever, weakness, and vomiting, but also patients may present more specific signs such as jaundice, itching, pale stools, and darkened urine. Additionally, clinical symptoms are usually accompanied by increased levels of liver enzymes, especially bilirubin, aspartate aminotransferase, and alanine aminotransferase.50–52 However, HEV infection can lead to more severe liver disease in pregnant women or patients with underlying chronic liver diseases, sometimes progressing to fulminant hepatic failure (FHF).53
Of major concern, is the relationship between HEV genotype 1 and 2 infections and pregnancy. In pregnant patients, acute liver disease can lead to FHF, and increased mortality (up to 30%) is observed in endemic regions.9 This link was first reported during several outbreaks in India but has also been found in sporadic cases in highly prevalent areas.54 HEV infection during pregnancy is also associated with abortion, prematurity, low birth weight, and an increased risk of perinatal mortality.55 Unfortunately, despite the suggested roles and association of immunological and/or hormonal factors, it is not currently understood why pregnancy results in severe hepatitis E manifestation.56,57
HEV infection in low endemic areas
The differences in clinical and epidemiological features of acute HEV infection between patients living in nonendemic countries and highly endemic areas are noticeable.58 The highest attack rates in middle and elderly males, highest overall mortality rates, and greater frequency of unspecific symptoms are clearly distinguishable. Additionally, severe clinical manifestations during pregnancy have only been occasionally reported for HEV genotype 3.59
Chronic HEV infection
Though HEV infection was conventionally believed to be a self-limited infection with spontaneous clearance in most of the patients, in recent years episodes of persistent viral shedding have been recognized in low endemic countries and in sporadic cases from endemic regions.60–62
The ability of HEV to progress to chronic state is of major concern in organ transplant recipients who receive immunosuppressive medication to prevent rejection. This group is thought to be the main population at risk for chronic hepatitis E, which is well documented among patients with liver and kidney transplants.63–65 Recently, it was also suggested that HEV chronic infection is an important cause of abnormalities in liver enzyme tests observed after lung and heart transplantation, sometimes leading to rapid liver fibrosis.66 Furthermore, HEV chronic infection has been shown to occur in patients with other conditions associated with immunosuppression, such as HIV infection and lymphoma and leukemia.59,61 However, the establishment of persistent viral infection seems to be much less common in this group than in those patients with solid organ transplantation.
Therefore, chronic HEV infection in immunocompromised individuals is an emerging and significant clinical problem. Recently, González Tallón et al reported the first case of a healthy, immunocompetent man who developed an episode of acute HEV hepatitis, which progressed to chronic liver disease within a 1-year period.67
Nonhepatic manifestations of HEV infection
There is some evidence that both acute and chronic infections are associated with extrahepatic manifestations, particularly acute pancreatitis and neurological disorders including encephalitis, polyradiculopathy, Guillain–Barré syndrome, bilateral brachial neuritis, and proximal myopathy.68,69 These issues are extensively discussed in greater detail in other reviews.12,70
HEV transmission
Drinking fecal contaminated water in highly-endemic regions with poor sanitation practices (waterborne transmission) and the consumption of raw or undercooked meat of HEV-infected animals (zoonotic, foodborne transmission), especially in industrialized countries, account for most HEV transmissions, resulting in an important public health problem.
Occasionally, the exact mode of HEV transmission remains controversial, and sources of viral infection are often not well identified, particularly in sporadic cases of acute hepatitis E. In this setting, the infection may be also related to the level of population immunity, sanitary conditions, living conditions, and others factors.71 Recent investigations reinforce the notion of the existence of three additional routes of HEV transmission: parenteral (blood borne transmission),72 human to human,73 and vertical transmission from mother to child (perinatal transmission).74 Even though these routes of transmission are thought to be less frequent, the existence of growing lines of evidence in this matter encourages prophylactic measures that contribute to the prevention of HEV infection.
Waterborne transmission
The earliest well-documented report of the disease was of a large epidemic of waterborne hepatitis occurring in New Delhi, India in 1955.75 Even though it was initially believed to be related to hepatitis A virus, subsequent testing of stored sera from this epidemic and another outbreak during 1978 to 1979 in Kashmir, India failed to demonstrate serological markers for hepatitis A and B viruses.54 HEV is mainly an enterically-transmitted pathogen and has been reported to occur as large waterborne epidemics and small outbreaks. In addition, in developing regions, it is occasionally associated with hepatitis A virus outbreaks in the form of dual infection, which increases the complexity of the HEV epidemiology and makes it more difficult to understand.32 These waterborne outbreaks, have been exclusively associated with genotype 1 and 2 strains.76–79 Nonetheless, environmental presence of HEV has also been demonstrated both in industrialized and developing countries, and raw sewage and seawater have been shown to contain infectious HEV strains that are closely related to the strains circulating in humans and other animals.80–85 Many reports have described genotype 3 as the main type that circulates in several environmental conditions, playing a potential role in the spread of HEV infection among humans.82–84 Although it has been suggested that the HEV virion is stable enough to be transmitted from environmental sources, additional studies should be performed to evaluate the ability to transmit and cause infection in cases where the virus contamination levels are low.85
Zoonotic and foodborne transmission
Since HEV is unique among the known hepatitis viruses, with several susceptible animal species capable of functioning as reservoir of the disease (swine, wild boar, and deer),86 the zoonotic transmission caused by genotype 3 and 4 HEV strains has been uncovered.5,6,36,42,43,87,88
HEV remains infectious at up to 60°C, suggesting the possibility of HEV transmission by consumption of raw and slightly steamed contaminated food.85 Indeed, the foodborne transmission by consumption of raw or undercooked meat of wild (deer and boar) and domestic (pig and probably rabbit) animals contaminated with HEV has been clearly demonstrated, and compelling evidence exists.7,89 More recently, fully infective HEV virions were detected, isolated, and characterized from pork liver sausage produced in France, suggesting that the consumption of these products may be a risk factor for HEV infection in humans, and for which measures to eliminate the source of viral origin must be warranted.47
Zoonotic transmission through direct contacts with infected animals has also been reported. Farmers, veterinarians, and workers attending animals comprise the highly at-risk, exposed group for HEV infection.90–92 Shellfish consumption has also been suggested as a potential source of HEV infection to human and other animal reservoirs. Said et al, identified HEV-contaminated shellfish as the almost exclusive risk factor involved in an outbreak occurring aboard a cruise ship in European waters.93 Afterwards, several HEV strains were detected in commercial mussels of different European countries.94,95
In summary, zoonotic risk for HEV transmission is currently well known and broadly studied, with an ever-expanding host range and newly identified animal reservoir species, revealing a health problem of major concern.
Vertical transmission
In endemic areas, HEV is the most common cause of hepatitis during pregnancy, but the cause of increased severity of the virus is not known.9 Notably, to date, the high mortality in pregnant woman has been associated with genotype 1 HEV infections only, and there have been no reports of HEV genotype 3 or 4 infections.96,97 However, HEV genotype 2 infection was also associated with acute liver failure in a pregnant woman during an outbreak in Namibia.79
HEV infection is commonly transmitted from mother to child via the intrauterine and perinatal routes, and in fetuses and neonates it causes severe liver disease with high rates of mortality.55,74,98–100 The clinical course in vertically transmitted HEV infection in survivor neonates is self-limiting with short lasting viremia.74
In developing countries, HEV may be responsible for 2,400–3,000 stillbirths each year, with many additional fetal deaths linked to antenatal maternal mortality; it remains unclear if the increase of stillbirths is attributable to vertically transmitted infection or if it is the result of maternal complications of hepatitis E.96 Other studies suggest that the severity of HEV infection in mother and baby may be related to each other, and fetal disease influenced the course of maternal HEV infection.101,102
Furthermore, there are no reliable data on whether HEV can be transmitted through breast milk, and there is no information about the influence of asymptomatic infection in pregnancy.96 In this direction, serologic surveillance and monitoring the entire pregnancy period and neonatal outcomes may be necessary to understand these issues.
Additional investigations of the mechanisms of HEV pathogenesis in pregnant women are needed to understand the role of transplacental transmission in fetal loss and stillbirth.
Person-to-person transmission
The role of person-to-person transmission in HEV infection is still controversial and is thought to not contribute significantly to morbidity in epidemics.71,103 However, in developing countries, poor hand hygiene and common drinking, hand washing, and eating vessels may offer repeated opportunities for cross-contamination of water and food with the virus, increasing the human-to-human transfer during an HEV outbreak.104
Many lines of evidence have indicated that person-to-person transmission is uncommon, especially in sporadic cases of hepatitis E.103,105 However, in endemic areas, even though most outbreaks of HEV infection have displayed a short course and are linked to a common drinking water source, some multimodal and prolonged outbreaks have also occurred that could be the result of continued person-to-person transmission.106
Indeed, some studies have suggested that person-to-person transmission is possible in HEV epidemics.103,107 Recently, the first direct evidence of this mode of transmission was reported from an HEV outbreak in northern Uganda.71 The lack of a clear continuing common source of infection necessary to sustain the epidemic for many months, the high estimated secondary attack rate, and the absence of HEV detection in zoonotic sources provided supporting data to the hypothesis. Nevertheless, additional studies are required to better understand the probable mechanisms and vehicles of transmission.71
Although uncommon, the intrafamilial spread of sporadic HEV infection has been suggested as a likely mode of transmission by several lines of evidence.73,105
Parenteral transmission
In industrialized countries, despite that only in a few cases of sporadic HEV infections where the source of infection could be certainly identified, most cases are probably linked to foodborne transmission through consumption of raw meat of reservoir animals. This mode of transmission, in which most of the infections will be asymptomatic, may lead to the spread of HEV infection by subclinically infected individuals. Indeed, several investigations have reported remarkably high HEV seroprevalence rates (5%–50%) among healthy individuals, suggesting a widespread circulation of HEV strains.108,109 This issue is of great significance to transfusion transmissibility of HEV because potentially infected donors may never have shown clinical signs. Thus, considering that HEV cannot be fully inactivated in blood-derived products, this virus has recently emerged as a transfusion-transmitted pathogen of concern and has led to a resurgence of interest to researchers in this field.
Although the parenteral route of transmission is not thought to be a frequent occurrence, and its clinical consequences have not been systematically evaluated, the potential risk of transmission of HEV by transfusion has been suggested by several studies.2,110–112 Additionally, comparative molecular analysis of HEV sequences from blood donor and recipient have been performed, and direct evidence for parenteral transmission (HEV genotypes 1 and 3) has been reported.72,113
Certainly, in the last few years, the knowledge regarding HEV epidemiology, its biology, and its modes of transmission, especially in nonendemic regions, has been remarkably increased. Thus, in the near future, it will be necessary to establish standardized guidelines and policies for, when possible, routine HEV RNA screening of blood banks and organ donors. Indeed, recently, a novel approach for routine detection of HEV infection in German blood donors has been performed.114 However, especially in developing countries, it still remains very expensive to efficiently perform nucleic acid amplification techniques (NATs)-based screening programs aimed to prevent HEV transmission by blood transfusion. Although currently available evidence indicates that transfusion-transmitted HEV infection indeed occurs and is more frequent than initially recognized, cost-effective analysis should be conducted in each case by local public health policy makers.115 In spite of this, and considering that fatal HEV outcomes such as FHF or chronicity may be triggered in recipients who are immunosuppressed, pregnant, or have chronic liver disease, special measures and considerations must be taken into account in these high-risk patients.
Diagnosis of HEV
Acute HEV infection is usually diagnosed by detecting specific anti-HEV antibodies (IgM and IgG). However, the performance of the available assays in different settings is not optimal, and highly variable values are observed depending on the commercial assay employed.116,117 Analysis of HEV RNA in biologic specimens such as stools, serum, and liver biopsy using NATs is also used for diagnosis. Even though in light of recent advancements in the understanding of HEV epidemiology and viral pathogenesis several diagnostic flow charts have been proposed,118 the standardization of diagnostic criteria still remains critical. Additional consensus regarding the best technologies suitable for serosurveys and diagnosis of acute HEV infection is also needed. Besides this, the diagnosis of HEV infection in immunocompromised patients and solid organ transplant recipients in whom seroconversion to anti-HEV antibodies is delayed or may not occur at all is of particular concern. In this review, we summarize the most common available diagnostic tools currently employed for the identification of acute HEV infection, discussing their performance in different settings on the basis of recent findings.
Serologic tests
Little was known concerning the immunological aspects of the HEV infection until the last few years, when a pattern of antibody response to HEV has been identified and understood. Anti-HEV IgM appears during acute stage of the infection and is detectable 4 days after the onset of jaundice and persists for up to 5 months.119 However, strongly positive reactions are rare after 3 months.59 Overall, 90% of patients coursing an acute hepatitis E infection have detectable anti-HEV IgM within 2 weeks of illness onset119 while anti-HEV IgG antibodies are detectable shortly after the appearance of anti-HEV IgM. Therefore, the fact that both classes of antibodies probably develop simultaneously in acute infection makes it difficult to establish an accurate serological diagnosis of acute HEV infection. Moreover, while the anti-HEV IgM antibodies rapidly decline within a few months, IgG persists for longer, a variable period within 1 to 14 years postinfection.120
Currently, commercially available immunoassays for the detection of specific anti-HEV antibodies during acute infection differ dramatically in their sensitivity and specificity, which may partly explain the discrepancies in the HEV seroprevalence observed in different studies.121
Traditional immunoassays for IgM have a sensitivity ranging from 90% to 97%, with false positive results of up to 2.5%,122,123 and several of them have been shown to produce false negative results in patients infected with genotype 1 strains.124 In fact, many diagnostic methodologies are based on HEV genotype-specific antigens, thus limiting the detection of all HEV genotypes.
Intrinsic genetic variability of HEV leads to significant modifications of antigenic sites that have important implications in the development of reliable immunoassays. Despite this variability, the four HEV genotypes share cross-reactive domains within capsid protein (ORF2), which include a minimum neutralizing domain comprising amino acids 458–607.49,125 ORF2 and ORF3 antigens or immunodominant peptides were widely used in commercial HEV serological tests for the detection of IgM, IgG, and IgA antibodies against HEV.126,127
Recent developments have focused on the construction and improvement of recombinant ORF2-derived antigens expressed either in baculovirus or Escherichia coli, which include the minimum neutralizing domain.16 In particular, the approaches that use virus-like particles (VLPs) technologies in the eukaryotic-expressing system, such as baculovirus, seem to be the more appropriate methods for constructing HEV antigens for diagnostic devices.118
Even though all the ORF2-based immunoassays have indeed improved sensitivity, the specificity still needs to be increased, especially in low endemic regions where the occurrence of IgM false positive cases are more frequent.128
In a recent study aimed to evaluate the performance of currently available commercial kits for the detection of specific anti-HEV IgG/M, 300 serum samples from patients from nonendemic areas stored at the Center for Disease Control of Taiwan were tested.118 Six immunoassays based on different immunodominant determinants were included: the EIAgen HEV IgG/M (Adaltis, Bologna, Italy) included the HEV ORF2 (amino acids 619–660) and ORF3 (amino acids 101–123), derived from the Burmese strain (genotype 1) and the Mexican genotype 2 prototype strain, respectively; the recomWell HEV IgG/M (Mikrogen, Neuried, Germany) used purified recombinant HEV-ORF2 virus antigens derived from genotype 1 and 3 strains; the MP Biomedicals HEV IgM ELISA 3.0 (Santa Ana, CA, USA) detected antibodies targeting recombinant peptides coded by ORF2 and the complete recombinant protein specified by ORF3 from genotypes 1 and 3; and the rest were in-house hepatitis E VLP IgG/M assays, which used highly purified empty VLPs of HEV as an antigen expressed by a recombinant baculovirus, and self-assembled with an ORF2-coded recombinant protein consisting of amino acid residues 112–660 of the Burmese strain. This study showed that recomWell IgM, which had the highest sensitivity (93.3%), exhibited the best overall performance for diagnosing and screening of acute HEV infection in Taiwan. However, the hepatitis E VLP IgM had the highest specificity (95.6%) and positive predictive value (40%) in spite of its relatively low sensitivity rate (66%). Beyond evident differences in the sensitivity and specificity among assays, all anti-HEV IgM detection systems in this study were better than anti-HEV IgG assays for the purpose of screening. Additionally, it was possible to raise the sensitivity up to 100% and improve specificity as much as possible by combining IgM and IgG assays from the same brand or two different IgM detection systems. Thus, at least in nonendemic areas, these approaches seem to have reasonable robustness for use as screening tools for acute HEV infection in immunocompetent patients.
In addition to the inconsistent performances of sensitivity and specificity among different available immunoassays,124,125 false reactivity for anti HEV IgM with other hepatotropic viruses such as Epstein–Barr virus (EBV) and cytomegalovirus (CMV) has been reported. This is clinically problematic and relevant since these viruses form the differential diagnosis for acute hepatitis once hepatitis A virus infection is excluded.129 The cross-serological reactivity of HEV with other viruses known to cause hepatitis was further investigated.130 In this retrospective study of HEV serology testing, 1,423 samples were analyzed with a commercially available kit. Of them, 1.9% were unequivocally IgM-positive and 9.3% were IgG-positive. Overall, the degree of EBV and CMV IgM cross-reactivity to anti-HEV IgM was strikingly high, with 33.3% and 24.2% of samples that were HEV IgM-positive also showing reactivity to EBV and CMV, respectively. Additionally, in only 13.3% of the samples, anti-HEV IgM serology correlated to HEV polymerase chain reaction (PCR) positivity. These results are concerning and highlight the unreliability of anti-HEV IgM testing given high false positive reaction rates with EBV and CMV IgM and the extremely low level of correlation with PCR-confirmed HEV infections.130
The diagnosis of acute HEV infection in patients with conditions associated with immunosuppression, such as HIV infection and lymphoma and leukemia as well as solid organ transplant recipients, is of particular interest and to which much research has been focused. In these patients, seroconversion to anti-HEV antibodies during infection is delayed or may not occur at all, and thus while using serological tests for screening, this condition must be considered. Abravanel et al131 evaluated the performance of the EIAgen HEV IgG and IgM kits (Adaltis) and anti-HEV IgM and IgG ELISA 3.0 Wantai kits (Wantai Biological Pharmacy Enterprise, Beijing, People’s Republic of China), the two main anti-HEV IgM and IgG assays employed in Europe for diagnosing acute HEV infections in immunosuppressed patients. In the study, 40 samples from 35 solid organ transplant recipients and five hematological patients were analyzed for anti-HEV antibodies, with two additional panels consisting of 44 acute HEV-infected immunocompetent patients and 233 HEV-negative blood donors used for comparison. Both anti-HEV IgM tests showed good specificity and sensitivity (85%–87.5% and 85%, respectively) in these immunocompromised patients; although as expected, they were markedly lower than that observed for the immunocompetent HEV-infected group.
By contrast, the assays had failed in detecting specific IgG antibodies in the acute phase, with only half of the patients testing positive for HEV. Thus, the performance of these commercially available tests indicate that in this setting, the anti-HEV IgM assays could be used as first line tools for the routine diagnosis of acute HEV infection, even in immunocompromised patients. However, according to this and several others studies,65,109 the molecular detection of HEV RNA is essential for the diagnosis of acute hepatitis E in anti-HEV IgM-negative immunocompromised patients. In this setting, HEV RNA detection and quantification may also have a critical role in monitoring the response to antiviral therapy.64
RNA-based detection tests
The accumulating information concerning the highly variable performance of the currently available serological tests in endemic and nonendemic regions, together with the false negative results and cross-reactivity with other hepatotropic viruses reported in different clinical settings, raises the question as to whether HEV RNA testing should be conducted in all patients suspected of HEV infection.
However, the sensitivity of molecular tests for the detection of HEV RNA is highly dependent on patients’ early presentation and timely collection of serum or stool samples as well as on appropriate transport and processing. Therefore, undetectable viral RNA does not rule out HEV infection.72 Even though HEV RNA may be detected at the onset of illness and up to 6 and 4 weeks in stool and serum, respectively, the viral RNA levels can be low and thus reduce the capture window for HEV.132
Nonetheless, detecting viral RNA in biologic samples is the gold standard for the confirmation of acute HEV hepatitis since NATs can accurately identify active infection and help confirm serological findings.133 Unfortunately, NAT-based detection is an expensive approach that might not be available for diagnostic laboratories, and additionally it demands highly specialized techniques and trained personnel.
In the last few years, several NAT assays have been reported for the detection and identification of HEV RNA in serum and stool samples, including reverse transcription followed by PCR (RT-PCR), real-time RT-PCR, and reverse transcription loop-mediated isothermal amplification. These NATs include assays designed and optimized to broadly detect the four human HEV genotypes.134–136
However, methods of HEV nucleic acid detection have not been well standardized, and extreme variability has been observed in the performance of in-house tests.137 In 2009, the Paul-Ehrlich-Institut (Langen, Hesse, Germany) initiated the development of an international standard (IS) for HEV RNA for use in NAT assays, with the approval of World Health Organization (WHO) Expert Committee on Biological Standardization. The initial study that investigated the performance of several in-house-developed NAT assays used in the detection of HEV infection was completed.137 In their work, Baylis et al included four viruses belonging to genotypes 3 (subtypes 3a, 3b, and 3f) and 4 (subtype 4c) that underwent blinded independent testing in several laboratories. Even though it was concluded that any of these strains could be used for the development of an IS, genotype 3 strains seemed to be the best candidates since they have the widest distribution worldwide, and genotype 3 is identified in chronic infections. On the other hand, wide variations in assay sensitivity (100- to 1,000-fold) were observed.137 Recently, two virus strains (of subtypes 3a and 3b) included in the panel, together with a Japanese national standard, were selected by the WHO as potential IS candidates and were further investigated.138 This international collaborative study, aimed to demonstrate the suitability of these IS candidates, evaluate their potency, and assign an internationally agreed upon unit, established a genotype 3a HEV strain as the IS for HEV RNA for use in NAT-based assays, with an assigned unit of 250,000 IU/mL.138 Furthermore, this WHO IS was employed to validate two new commercially available HEV RNA assays and to evaluate their suitability in detecting and quantifying 3c, 3e, and 3f.139 These strains were chosen since they are the most prevalent among genotype 3 isolates in industrialized countries. Both methodologies, Hepatitis@ceeram Tools kit by Ceeram (La Chapelle sur Erdre, France) and the RealStar HEV RT-PCR kit, version 1.0, by Altona Diagnostics (Hamburg, Germany) showed good analytical sensitivity with high reproducibility for detecting genotype 3 HEV RNA.
On the other hand, again, the extremely high variability observed in sensitivity among the assays highlights the need for the standardization of genotype-specific NAT assays and the development of methodologies capable of accurately detecting all HEV genotypes. To this end, much more study involving other HEV strains is required.
Management of HEV infection
Acute HEV is a self-limiting illness in immunocompetent patients. Some patients might require treatment of symptoms, but almost all are able to clear the HEV infection spontaneously. However, in patients with poor prognostic factors such as immunosuppressed status or underlying liver disease, HEV infection can develop to fulminant hepatitis or acute or chronic liver failure. In this setting, a short course of ribavirin has been shown to produce complete recovery and avoid the need for liver transplantation in case reports and small series.70,140,141 However, many more investigative and prospective studies are needed to evaluate if ribavirin treatment can indeed prevent progression to liver failure in patients with severe acute hepatitis E. Currently, liver transplantation is the only validated treatment option for patients with FHF.140,141
Of major concern is the ability of HEV, especially genotype 1 strains, to cause fulminant hepatitis in pregnant women with high mortality rates. To date no data are available on the role of treatment in pregnant women with acute hepatitis E, non-pregnant patients with acute liver failure, or during neonatal HEV infection. These cases, which mainly occur in areas where HEV is highly endemic, differ from patients with chronic HEV infection in that the window of time available for the treatment to be effective may be much shorter.70
As mentioned, the chronic course of HEV genotype 3 infection has been described in solid organ transplant recipient patients with hematological disease and with HIV-positive patients who had low CD4 counts.70,140–142 Chronic HEV infection can result in progressive liver fibrosis, cirrhosis, and subsequent liver failure, which occasionally requires liver transplantation.70,140,143,144 Therefore, therapeutic interventions should be considered for immunocompromised patients with HEV infection.70,140,141 The treatment goal for chronic HEV infection is the complete removal of the virus. Even though various treatment options have been attempted, and several methods were described, systematic guidelines have not yet been reported.140,141,145
Decreasing the doses of immunosuppressive drugs that are aimed at T cells (mainly calcineurin inhibitors) has been proposed as the first-line therapeutic approach in transplant patients. This leads to spontaneous HEV clearance in 30% of patients but also to rejection under certain circumstances.141,145
Currently, it is widely agreed that antiviral therapy should be considered for patients who fail to eliminate the virus from their system after reduction in immunosuppressive drugs or for those who cannot tolerate a reduced dose of immunosuppressive drugs.146,147 In these cases, antiviral therapy for chronic infection consists of monotherapy with interferon-alpha or ribavirin or a combination of these medications, with a recommended dosage period of usually 2–3 months.70,140,141,148 However, both of these medications induce some severe adverse effects. In transplant recipients, interferon-alpha has been shown to increase the risk of rejection, and severe hemolytic anemia was observed in patients undergoing ribavirin treatment.70,140,146,149
PEGylated interferon-alpha 2a (PEG-IFNa2a) has been used as monotherapy for liver transplant recipients with chronic HEV. In a small case series, three patients who received 3 months of therapy with PEG-IFNa2a were included, and while two had a virological response at 24 and 20 weeks after completion of treatment, respectively, one experienced acute rejection after the completion of the treatment.65,150 A group from the Netherlands, has recently reported the findings and clinical outcomes of treatment with PEG-IFNa2b of two liver transplant recipients with chronic HEV. One patient treated for 1 year had normalization of liver enzymes tests and a complete virological response at week 20. On the contrary, no evidence of a virological response was detected in the second patient, and PEG-IFNa2b treatment was stopped at week 16; however, after the immunosuppression dose was decreased, there was a normalization of liver enzymes, and HEV RNA became undetectable in serum.65,151 Treatment with interferon, however, has been considered as a possible risk for inducing acute rejection in liver transplant recipients and is particularly contraindicated by clinicians in kidney, lung, and heart transplant recipients patients.65,150
Several studies have been carried out with the aim to evaluate the efficacy of treatment with ribavirin under a monotherapy approach. A study carried out in France evaluated this drug in six kidney transplant patients who were HEV RNA-positive. After 6 months of treatment, four patients had a sustained virological response, and two patients presented a viral relapse after the completion of their ribavirin treatment.65,152
A prospective study done in Germany evaluated 33 solid organ transplant recipients with posttransplant HEV infection during the period from 2008 to 2012. Fifteen out of 33 patients (45%) had elevated alanine aminotransferase levels and active HEV infection (detectable RNA) for more than 2 months (prolonged HEV viremia), which was cleared in three of them after a reduction of immunosuppression. On the other hand, nine of eleven patients who received ribavirin became HEV RNA-negative after 3 to 6 weeks, and none of these patients had a recurrent HEV infection after the end of the treatment. The administered dose of ribavirin was 600 to 1,000 mg daily.150
Another interesting study showed that in a group of ten HEV RNA-positive patients of a cohort of 468 adult lung transplant recipients, eight patients developed a chronic HEV infection for more than 6 months. Thereafter, two of these patients were treated with ribavirin (400 mg twice daily) for 4 months and experienced a clearance of HEV RNA after 2 months as well as normalization of aminotransferases levels.149
The mechanism by which ribavirin suppresses HEV replication is not fully understood and requires further investigation.141 For kidney, lung, and heart transplant recipients with chronic HEV infections, in which treatment with interferon is contraindicated because of the high risk of rejection, ribavirin could be an option as the first line of treatment since it seems to be well tolerated, safe, and capable of inducing a sustained virological response.152,153 However, the optimal dosage and duration of the treatment still need to be determined and standardized. In Figure 3, an algorithm of management of HEV infection is proposed.
Figure 3.
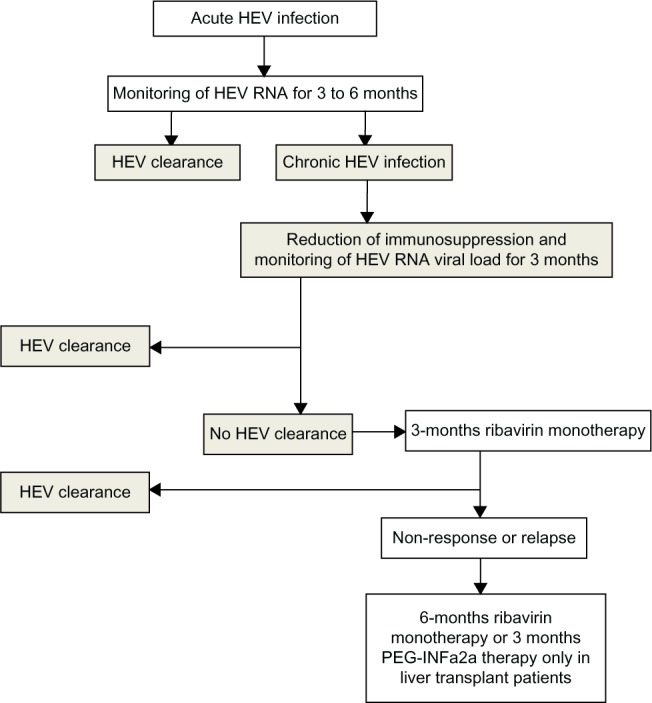
Proposed algorithm for the management of hepatitis E viral infection after solid organ transplantation.
Note: © Copyright 2012 The American Society of Transplantation and the American Society of Transplant Surgeons. Adapted with permission from Kamar N, Legrand-Abravanel F, Izopet J, Rostaing L. Hepatitis E virus: what transplant physicians should know. Am J Transplant. 2012;12(9):2281–2287.155
Abbreviations: HEV, hepatitis E virus; PEG-INFa2a, pegylated interferon-alpha 2a; RNA, ribonucleic acid.
Appropriate prophylactic strategies and measures must be exercised in order to avoid HEV infection, particularly in high-risk groups such as pregnant women, immunosuppressed individuals, and solid organ transplant recipients. To date, two types of recombinant HEV vaccine have been developed. The first, developed by GlaxoSmithKline (Brentford, UK) and the Walter Reed Army Institute of Research (Washington, DC, USA), was tested in Nepalese males (n=1,900) with high safety and efficacy levels after three doses. However, this vaccine has not been further developed.154 The second vaccine was tested in more than 112,000 Chinese participants, irrespective of HEV titers, and demonstrated a very high efficacy of around 94%–100% (95% confidence interval; 72.1–100) with a good safety profile. This vaccine, known as HEV 239, was licensed in the People’s Republic of China in December 2011 and is approved for high-risk groups and will soon be available to other countries highly endemic for HEV.52 However, both vaccines are genotype 1-based, and though they would be very useful in pregnant women and travelers to endemic regions, their efficacy in preventing HEV infection in nonendemic areas (where other genotypes predominate) is a matter of debate and needs to be investigated. Future developments including other genotypes, particularly genotype 3, will enable chronic HEV infection prevention and could be considered as an immunoprophylaxis measure in pretransplant recipients.70
Concluding remarks
HEV is the leading cause of non-A, non-B enterically-transmitted acute viral hepatitis in endemic regions and is considered a major global health problem that causes significant morbidity worldwide. Zoonotic transmission seems to be a major cause of HEV infections in industrialized countries, in the form of sporadic autochthonous cases. Prevention of foodborne HEV transmission should rely on avoiding consumption of raw or undercooked animal meat and the revision of the minimum safety industry standards required for the production of ready-to-eat products of animal source. In addition, the currently increasing global burden of epidemic and sporadic forms of hepatitis E, the high mortality among pregnant women, the severity of autochthonous hepatitis E, and the ability of the virus to induce chronic infections highlights the need to give special attention to persons at higher risk of severe illness by giving priority to the prevention of infection in this vulnerable group during HEV outbreaks. Serological and NAT-based HEV tests should therefore be included in the evaluations of all patients with increased levels of liver transaminases. In this sense, it is particularly relevant that the test for HEV RNA be carried out in immunocompromised patients, such as HIV-infected individuals, solid organ transplant recipients, and people with hematological diseases. Patients with chronic hepatitis E should be considered for treatment with ribavirin since prolonged viremia has been associated with the development of liver cirrhosis and severe hepatic failure. The threat caused by the widespread prevalence of HEV infection reinforces the need to perform broad epidemiological studies in endemic and nonendemic regions and to conduct clinical trials of currently developing vaccines. Additional research to find the most highly effective and protective candidates for HEV vaccines, which include the immunodominant epitopes of the four human genotypes, should be pursued.
Acknowledgments
The authors would like to thank the Agencia Nacional de Investigación e Innovación (ANII) for its support in the form of research fellowships (SM and NR).
Footnotes
Disclosure
JA is a Level 3 Researcher at Sistema Nacional de Investigadores-ANII. The authors report no other conflicts of interest in this work.
References
- 1.Purcell RH, Emerson SU. Animal models of hepatitis A and E. ILAR J. 2001;42(2):161–177. doi: 10.1093/ilar.42.2.161. [DOI] [PubMed] [Google Scholar]
- 2.Hino K, Kondo T, Niwa H, et al. A small epidemic of enterically transmitted non-A, non-B acute hepatitis. Gastroenterol Jpn. 1991;26(Suppl 3):139–141. doi: 10.1007/BF02779284. [DOI] [PubMed] [Google Scholar]
- 3.Dawson GJ, Mushahwar IK, Chau KH, Gitnick GL. Detection of long-lasting antibody to hepatitis E virus in a US traveller to Pakistan. Lancet. 1992;340(8816):426–427. doi: 10.1016/0140-6736(92)91507-5. [DOI] [PubMed] [Google Scholar]
- 4.Donati MC, Fagan EA, Harrison TJ. Sequence analysis of full length HEV clones derived directly from human liver in fulminant hepatitis E. In: Rizzetto M, Purcell RH, Gerin JL, Verme G, editors. Viral Hepatitis and Liver Disease. Torino: Edizioni Minerva Medica; 1997. pp. 313–316. [Google Scholar]
- 5.Okamoto H, Takahashi M, Nishizawa T, Fukai K, Muramatsu U, Yoshikawa A. Analysis of the complete genome of indigenous swine hepatitis E virus isolated in Japan. Biochem Biophys Res Commun. 2001;289(5):929–936. doi: 10.1006/bbrc.2001.6088. [DOI] [PubMed] [Google Scholar]
- 6.Smith JL. A review of hepatitis E virus. J Food Prot. 2001;64(4):572–586. doi: 10.4315/0362-028x-64.4.572. [DOI] [PubMed] [Google Scholar]
- 7.Meng XJ. Zoonotic and foodborne transmission of hepatitis E virus. Semin Liver Dis. 2013;33(1):41–49. doi: 10.1055/s-0033-1338113. [DOI] [PubMed] [Google Scholar]
- 8.Meng XJ. From barnyard to food table: the omnipresence of hepatitis E virus and risk for zoonotic infection and food safety. Virus Res. 2011;161(1):23–30. doi: 10.1016/j.virusres.2011.01.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kumar S, Subhadra S, Singh B, Panda BK. Hepatitis E virus: the current scenario. Int J Infect Dis. 2013;17(4):e228–e233. doi: 10.1016/j.ijid.2012.11.026. [DOI] [PubMed] [Google Scholar]
- 10.Holla RP, Ahmad I, Ahmad Z, Jameel S. Molecular virology of hepatitis E virus. Semin Liver Dis. 2013;33(1):3–14. doi: 10.1055/s-0033-1338110. [DOI] [PubMed] [Google Scholar]
- 11.Pischke S, Heim A, Bremer B, et al. Hepatitis E: an emerging infectious disease in Germany? Z Gastroenterol. 2011;49(9):1255–1257. doi: 10.1055/s-0031-1273394. [DOI] [PubMed] [Google Scholar]
- 12.Aggarwal R. Clinical presentation of hepatitis E. Virus Res. 2011;161(1):15–22. doi: 10.1016/j.virusres.2011.03.017. [DOI] [PubMed] [Google Scholar]
- 13.Fauquet CM, Mayo MA, Maniloff J, Desselberger U, Ball LA, editors. Virus Taxonomy: Eighth Report of the International Committee on Taxonomy of Viruses. London: Elsevier Academic Press; 2005. [Google Scholar]
- 14.Yamashita T, Mori Y, Miyazaki N, et al. Biological and immunological characteristics of hepatitis E virus-like particles based on the crystal structure. Proc Natl Acad Sci U S A. 2009;106(31):12986–12991. doi: 10.1073/pnas.0903699106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tam AW, Smith MM, Guerra ME, et al. Hepatitis E virus (HEV): molecular cloning and sequencing of the full-length viral genome. Virology. 1991;185(1):120–131. doi: 10.1016/0042-6822(91)90760-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ahmad I, Holla RP, Jameel S. Molecular virology of hepatitis E virus. Virus Res. 2011;161(1):47–58. doi: 10.1016/j.virusres.2011.02.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Koonin EV, Gorbalenya AE, Purdy MA, Rozanov MN, Reyes GR, Bradley DW. Computer-assisted assignment of functional domains in the nonstructural polyprotein of hepatitis E virus: delineation of an additional group of positive-strand RNA plant and animal viruses. Proc Natl Acad Sci U S A. 1992;89(17):8259–8263. doi: 10.1073/pnas.89.17.8259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Agrawal S, Gupta D, Panda SK. The 3′ end of hepatitis E virus (HEV) genome binds specifically to the viral RNA-dependent RNA polymerase (RdRp) Virology. 2001;282(1):87–101. doi: 10.1006/viro.2000.0819. [DOI] [PubMed] [Google Scholar]
- 19.Pudupakam RS, Kenney SP, Córdoba L, et al. Mutational analysis of the hypervariable region of hepatitis e virus reveals its involvement in the efficiency of viral RNA replication. J Virol. 2011;85(19):10031–10040. doi: 10.1128/JVI.00763-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Huang FF, Sun ZF, Emerson SU, et al. Determination and analysis of the complete genomic sequence of avian hepatitis E virus (avian HEV) and attempts to infect rhesus monkeys with avian HEV. J Gen Virol. 2004;85(Pt 6):1609–1618. doi: 10.1099/vir.0.79841-0. [DOI] [PubMed] [Google Scholar]
- 21.Reyes GR. Hepatitis E virus (HEV): molecular biology and emerging epidemiology. Prog Liver Dis. 1993;11:203–213. [PubMed] [Google Scholar]
- 22.Mushahwar IK, Dawson GJ, Reyes GR. Hepatitis E virus: molecular biology and diagnosis. Eur J Gastroenterol Hepatol. 1996;8(4):312–318. [PubMed] [Google Scholar]
- 23.Okamoto H. Genetic variability and evolution of hepatitis E virus. Virus Res. 2007;127(2):216–228. doi: 10.1016/j.virusres.2007.02.002. [DOI] [PubMed] [Google Scholar]
- 24.Nagashima S, Takahashi M, Jirintai S, et al. Tumour susceptibility gene 101 and the vacuolar protein sorting pathway are required for the release of hepatitis E virions. J Gen Virol. 2011;92(Pt 12):2838–2848. doi: 10.1099/vir.0.035378-0. [DOI] [PubMed] [Google Scholar]
- 25.Korkaya H, Jameel S, Gupta D, et al. The ORF3 protein of hepatitis E virus binds to Src homology 3 domains and activates MAPK. J Biol Chem. 2001;276(45):42389–42400. doi: 10.1074/jbc.M101546200. [DOI] [PubMed] [Google Scholar]
- 26.Purcell RH. Hepatitis viruses: changing patterns of human disease. Proc Natl Acad Sci U S A. 1994;91(7):2401–2406. doi: 10.1073/pnas.91.7.2401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Schlauder GG, Mushahwar IK. Genetic heterogeneity of hepatitis E virus. J Med Virol. 2001;65(2):282–292. doi: 10.1002/jmv.2031. [DOI] [PubMed] [Google Scholar]
- 28.Lu L, Li C, Hagedorn CH. Phylogenetic analysis of global hepatitis E virus sequences: genetic diversity, subtypes and zoonosis. Rev Med Virol. 2006;16(1):5–36. doi: 10.1002/rmv.482. [DOI] [PubMed] [Google Scholar]
- 29.Zanetti AR, Schlauder GG, Romanò L, et al. Identification of a novel variant of hepatitis E virus in Italy. J Med Virol. 1999;57(4):356–360. doi: 10.1002/(sici)1096-9071(199904)57:4<356::aid-jmv5>3.0.co;2-d. [DOI] [PubMed] [Google Scholar]
- 30.Takahashi M, Nishizawa T, Sato H, et al. Analysis of the full-length genome of a hepatitis E virus isolate obtained from a wild boar in Japan that is classifiable into a novel genotype. J Gen Virol. 2011;92(Pt 4):902–908. doi: 10.1099/vir.0.029470-0. [DOI] [PubMed] [Google Scholar]
- 31.Oliveira-Filho EF, König M, Thiel HJ. Genetic variability of HEV isolates: inconsistencies of current classification. Vet Microbiol. 2013;165(1–2):148–154. doi: 10.1016/j.vetmic.2013.01.026. [DOI] [PubMed] [Google Scholar]
- 32.Echevarría JM, González JE, Lewis-Ximenez LL, et al. Hepatitis E virus infection in Latin America: a review. J Med Virol. 2013;85(6):1037–1045. doi: 10.1002/jmv.23526. [DOI] [PubMed] [Google Scholar]
- 33.Mirazo S, Mainardi V, Ramos N, Gerona S, Rocca A, Arbiza J. Indigenous hepatitis E virus genotype 1 infection, Uruguay. Emerg Infect Dis. 2014;20(1):171–173. doi: 10.3201/eid2001.131471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hakze-van der Honing RW, van Coillie E, Antonis AF, van der Poel WH. First isolation of hepatitis E virus genotype 4 in Europe through swine surveillance in The Netherlands and Belgium. PLoS One. 2011;6(8):e22673. doi: 10.1371/journal.pone.0022673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Smith DB, Purdy MA, Simmonds P. Genetic variability and the classification of hepatitis E virus. J Virol. 2013;87(8):4161–4169. doi: 10.1128/JVI.02762-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Teo CG. Much meat, much malady: changing perceptions of the epidemiology of hepatitis E. Clin Microbiol Infect. 2010;16(1):24–32. doi: 10.1111/j.1469-0691.2009.03111.x. [DOI] [PubMed] [Google Scholar]
- 37.Caron M, Enouf V, Than SC, Dellamonica L, Buisson Y, Nicand E. Identification of genotype 1 hepatitis E virus in samples from swine in Cambodia. J Clin Microbiol. 2006;44(9):3440–3442. doi: 10.1128/JCM.00939-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Bader TF, Krawczynski K, Polish LB, Favorov MO. Hepatitis E in a US traveler to Mexico. N Engl J Med. 1991;325(23):1659. doi: 10.1056/NEJM199112053252321. [DOI] [PubMed] [Google Scholar]
- 39.Ijaz S, Arnold E, Banks M, et al. Non-travel-associated hepatitis E in England and Wales: demographic, clinical, and molecular epidemiological characteristics. J Infect Dis. 2005;192(7):1166–1172. doi: 10.1086/444396. [DOI] [PubMed] [Google Scholar]
- 40.Okamoto H, Takahashi M, Nishizawa T. Features of hepatitis E virus infection in Japan. Intern Med. 2003;42(11):1065–1071. doi: 10.2169/internalmedicine.42.1065. [DOI] [PubMed] [Google Scholar]
- 41.Amon JJ, Drobeniuc J, Bower WA, et al. Locally acquired hepatitis E virus infection, El Paso, Texas. J Med Virol. 2006;78(6):741–746. doi: 10.1002/jmv.20617. [DOI] [PubMed] [Google Scholar]
- 42.Meng XJ, Purcell RH, Halbur PG, et al. A novel virus in swine is closely related to the human hepatitis E virus. Proc Natl Acad Sci U S A. 1997;94(18):9860–9865. doi: 10.1073/pnas.94.18.9860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Meng XJ. Novel strains of hepatitis E virus identified from humans and other animal species: is hepatitis E a zoonosis? J Hepatol. 2000;33(5):842–845. doi: 10.1016/s0168-8278(00)80319-0. [DOI] [PubMed] [Google Scholar]
- 44.Lack JB, Volk K, Van Den Bussche RA. Hepatitis E virus genotype 3 in wild rats, United States. Emerg Infect Dis. 2012;18(8):1268–1273. doi: 10.3201/eid1808.120070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Izopet J, Dubois M, Bertagnoli S, et al. Hepatitis E virus strains in rabbits and evidence of a closely related strain in humans, France. Emerg Infect Dis. 2012;18(8):1274–1281. doi: 10.3201/eid1808.120057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Colson P, Borentain P, Queyriaux B, et al. Pig liver sausage as a source of hepatitis E virus transmission to humans. J Infect Dis. 2010;202(6):825–834. doi: 10.1086/655898. [DOI] [PubMed] [Google Scholar]
- 47.Berto A, Grierson S, Hakze-van der Honing R, et al. Hepatitis E virus in pork liver sausage, France. Emerg Infect Dis. 2013;19(2):264–266. doi: 10.3201/eid1902.121255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Teo CG, Hepatitis E. In: CDC Health Information for International Travel 2010. Brunette GW, Kozarsky P, Magill AJ, Shliml DR, Whatley AD, editors. St Louis, MO: Mosby; 2009. pp. 335–337. [Google Scholar]
- 49.Mushahwar IK. Hepatitis E virus: molecular virology, clinical features, diagnosis, transmission, epidemiology, and prevention. J Med Virol. 2008;80(4):646–658. doi: 10.1002/jmv.21116. [DOI] [PubMed] [Google Scholar]
- 50.Kumar S, Ratho RK, Chawla YK, Chakraborti A. The incidence of sporadic viral hepatitis in North India: a preliminary study. Hepatobiliary Pancreat Dis Int. 2007;6(6):596–599. [PubMed] [Google Scholar]
- 51.Rein DB, Stevens GA, Theaker J, Wittenborn JS, Wiersma ST. The global burden of hepatitis E virus genotypes 1 and 2 in 2005. Hepatology. 2012;55(4):988–997. doi: 10.1002/hep.25505. [DOI] [PubMed] [Google Scholar]
- 52.Zhu FC, Zhang J, Zhang XF, et al. Efficacy and safety of a recombinant hepatitis E vaccine in healthy adults: a large-scale, randomised, double-blind placebo-controlled, phase 3 trial. Lancet. 2010;376(9744):895–902. doi: 10.1016/S0140-6736(10)61030-6. [DOI] [PubMed] [Google Scholar]
- 53.Taniguchi M, Kim SR, Mishiro S, et al. Epidemiology of hepatitis E in Northeastern China, South Korea and Japan. J Infect. 2009;58(3):232–237. doi: 10.1016/j.jinf.2009.01.011. [DOI] [PubMed] [Google Scholar]
- 54.Khuroo MS. Study of an epidemic of non-A, non-B hepatitis. Possibility of another human hepatitis virus distinct from post-transfusion non-A, non-B type. Am J Med. 1980;68(6):818–824. doi: 10.1016/0002-9343(80)90200-4. [DOI] [PubMed] [Google Scholar]
- 55.Patra S, Kumar A, Trivedi SS, Puri M, Sarin SK. Maternal and fetal outcomes in pregnant women with acute hepatitis E virus infection. Ann Intern Med. 2007;147(1):28–33. doi: 10.7326/0003-4819-147-1-200707030-00005. [DOI] [PubMed] [Google Scholar]
- 56.Kar P, Jilani N, Husain SA, et al. Does hepatitis E viral load and genotypes influence the final outcome of acute liver failure during pregnancy? Am J Gastroenterol. 2008;103(10):2495–2501. doi: 10.1111/j.1572-0241.2008.02032.x. [DOI] [PubMed] [Google Scholar]
- 57.Navaneethan U, Al Mohajer M, Shata MT. Hepatitis E and pregnancy: understanding the pathogenesis. Liver Int. 2008;28(9):1190–1199. doi: 10.1111/j.1478-3231.2008.01840.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Pavio N, Mansuy JM. Hepatitis E in high-income countries. Curr Opin Infect Dis. 2010;23(5):521–527. doi: 10.1097/QCO.0b013e32833de683. [DOI] [PubMed] [Google Scholar]
- 59.Dalton HR, Stableforth W, Thurairajah P, et al. Autochthonous hepatitis E in Southwest England: natural history, complications and seasonal variation, and hepatitis E virus IgG seroprevalence in blood donors, the elderly and patients with chronic liver disease. Eur J Gastroenterol Hepatol. 2008;20(8):784–790. doi: 10.1097/MEG.0b013e3282f5195a. [DOI] [PubMed] [Google Scholar]
- 60.Schlosser B, Stein A, Neuhaus R, et al. Liver transplant from a donor with occult HEV infection induced chronic hepatitis and cirrhosis in the recipient. J Hepatol. 2012;56(2):500–502. doi: 10.1016/j.jhep.2011.06.021. [DOI] [PubMed] [Google Scholar]
- 61.le Coutre P, Meisel H, Hofmann J, et al. Reactivation of hepatitis E infection in a patient with acute lymphoblastic leukaemia after allogeneic stem cell transplantation. Gut. 2009;58(5):699–702. doi: 10.1136/gut.2008.165571. [DOI] [PubMed] [Google Scholar]
- 62.Koenecke C, Pischke S, Heim A, et al. Chronic hepatitis E in hematopoietic stem cell transplant patients in a low-endemic country? Transpl Infect Dis. 2012;14(1):103–106. doi: 10.1111/j.1399-3062.2011.00702.x. [DOI] [PubMed] [Google Scholar]
- 63.Gérolami R, Moal V, Colson P. Chronic hepatitis E with cirrhosis in a kidney-transplant recipient. N Engl J Med. 2008;358(8):859–860. doi: 10.1056/NEJMc0708687. [DOI] [PubMed] [Google Scholar]
- 64.Kamar N, Selves J, Mansuy JM, et al. Hepatitis E virus and chronic hepatitis in organ-transplant recipients. N Engl J Med. 2008;358(8):811–817. doi: 10.1056/NEJMoa0706992. [DOI] [PubMed] [Google Scholar]
- 65.Pischke S, Suneetha PV, Baechlein C, et al. Hepatitis E virus infection as a cause of graft hepatitis in liver transplant recipients. Liver Transpl. 2010;16(1):74–82. doi: 10.1002/lt.21958. [DOI] [PubMed] [Google Scholar]
- 66.Koning L, Pas SD, de Man RA, et al. Clinical implications of chronic hepatitis E virus infection in heart transplant recipients. J Heart Lung Transplant. 2013;32(1):78–85. doi: 10.1016/j.healun.2012.10.008. [DOI] [PubMed] [Google Scholar]
- 67.González Tallón AI, Moreira Vicente V, Mateos Lindemann ML, Achécar Justo LM. Chronic hepatitis E in an immunocompetent patient. Gastroenterol Hepatol. 2011;34(6):398–400. doi: 10.1016/j.gastrohep.2011.02.011. [DOI] [PubMed] [Google Scholar]
- 68.Kamar N, Bendall RP, Peron JM, et al. Hepatitis E virus and neurologic disorders. Emerg Infect Dis. 2011;17(2):173–179. doi: 10.3201/eid1702.100856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.van den Berg B, van der Eijk AA, Pas SD, et al. Guillain-Barré syndrome associated with preceding hepatitis E virus infection. Neurology. 2014;82(6):491–497. doi: 10.1212/WNL.0000000000000111. [DOI] [PubMed] [Google Scholar]
- 70.Arends JE, Ghisetti V, Irving W, et al. Hepatitis E: An emerging infection in high income countries. J Clin Virol. 2014;59(2):81–88. doi: 10.1016/j.jcv.2013.11.013. [DOI] [PubMed] [Google Scholar]
- 71.Teshale EH, Hu DJ, Holmberg SD. The two faces of hepatitis E virus. Clin Infect Dis. 2010;51(3):328–334. doi: 10.1086/653943. [DOI] [PubMed] [Google Scholar]
- 72.Colson P, Coze C, Gallian P, Henry M, De Micco P, Tamalet C. Transfusion-associated hepatitis E, France. Emerg Infect Dis. 2007;13(4):648–649. doi: 10.3201/eid1304.061387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Mansuy JM, Huynh A, Abravanel F, Recher C, Peron JM, Izopet J. Molecular evidence of patient-to-patient transmission of hepatitis E virus in a hematology ward. Clin Infect Dis. 2009;48(3):373–374. doi: 10.1086/595893. [DOI] [PubMed] [Google Scholar]
- 74.Khuroo MS, Kamili S, Khuroo MS. Clinical course and duration of viremia in vertically transmitted hepatitis E virus (HEV) infection in babies born to HEV-infected mothers. J Viral Hepat. 2009;16(7):519–523. doi: 10.1111/j.1365-2893.2009.01101.x. [DOI] [PubMed] [Google Scholar]
- 75.Ishwanathan R. Infectious hepatitis in Delhi (1955–1956): a critical study. Indian J Med Res. 1957;45:1–29. [Google Scholar]
- 76.Zhuang H, Cao XY, Liu CB, Wang GM. Epidemiology of hepatitis E in China. Gastroenterol Jpn. 1991;26(Suppl 3):135–138. doi: 10.1007/BF02779283. [DOI] [PubMed] [Google Scholar]
- 77.Bi SL, Purdy MA, McCaustland KA, Margolis HS, Bradley DW. The sequence of hepatitis E virus isolated directly from a single source during an outbreak in China. Virus Res. 1993;28(3):233–247. doi: 10.1016/0168-1702(93)90024-h. [DOI] [PubMed] [Google Scholar]
- 78.Guthmann JP, Klovstad H, Boccia D, et al. A large outbreak of hepatitis E among a displaced population in Darfur, Sudan, 2004: the role of water treatment methods. Clin Infect Dis. 2006;42(12):1685–1691. doi: 10.1086/504321. [DOI] [PubMed] [Google Scholar]
- 79.Maila HT, Bowyer SM, Swanepoel R. Identification of a new strain of hepatitis E virus from an outbreak in Namibia in 1995. J Gen Virol. 2004;85(Pt 1):89–95. doi: 10.1099/vir.0.19587-0. [DOI] [PubMed] [Google Scholar]
- 80.Ippagunta SK, Naik S, Sharma B, Aggarwal R. Presence of hepatitis E virus in sewage in Northern India: frequency and seasonal pattern. J Med Virol. 2007;79(12):1827–1831. doi: 10.1002/jmv.21017. [DOI] [PubMed] [Google Scholar]
- 81.Vaidya SR, Tilekar BN, Walimbe AM, Arankalle VA. Increased risk of hepatitis E in sewage workers from India. J Occup Environ Med. 2003;45(11):1167–1170. doi: 10.1097/01.jom.0000088874.43855.2f. [DOI] [PubMed] [Google Scholar]
- 82.Clemente-Casares P, Pina S, Buti M, et al. Hepatitis E virus epidemiology in industrialized countries. Emerg Infect Dis. 2003;9(4):448–454. doi: 10.3201/eid0904.020351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Ishida S, Yoshizumi S, Ikeda T, et al. Detection and molecular characterization of hepatitis E virus in clinical, environmental and putative animal sources. Arch Virol. 2012;157(12):2363–2368. doi: 10.1007/s00705-012-1422-8. [DOI] [PubMed] [Google Scholar]
- 84.Masclaux FG, Hotz P, Friedli D, Savova-Bianchi D, Oppliger A. High occurrence of hepatitis E virus in samples from wastewater treatment plants in Switzerland and comparison with other enteric viruses. Water Res. 2013;47(14):5101–5109. doi: 10.1016/j.watres.2013.05.050. [DOI] [PubMed] [Google Scholar]
- 85.Yugo DM, Meng XJ. Hepatitis E virus: foodborne, waterborne and zoonotic transmission. Int J Environ Res Public Health. 2013;10(10):4507–4533. doi: 10.3390/ijerph10104507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Pavio N, Meng XJ, Renou C. Zoonotic hepatitis E: animal reservoirs and emerging risks. Vet Res. 2010;41(6):46–60. doi: 10.1051/vetres/2010018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Erker JC, Desai SM, Schlauder GG, Dawson GJ, Mushahwar IK. A hepatitis E virus variant from the United States: molecular characterization and transmission in cynomolgus macaques. J Gen Virol. 1999;80(Pt 3):681–690. doi: 10.1099/0022-1317-80-3-681. [DOI] [PubMed] [Google Scholar]
- 88.Tei S, Kitajima N, Takahashi K, Mishiro S. Zoonotic transmission of hepatitis E virus from deer to human beings. Lancet. 2003;362(9381):371–373. doi: 10.1016/S0140-6736(03)14025-1. [DOI] [PubMed] [Google Scholar]
- 89.Lhomme S, Dubois M, Abravanel F, et al. Risk of zoonotic transmission of HEV from rabbits. J Clin Virol. 2013;58(2):357–362. doi: 10.1016/j.jcv.2013.02.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Christensen PB, Engle RE, Hjort C, et al. Time trend of the prevalence of hepatitis E antibodies among farmers and blood donors: a potential zoonosis in Denmark. Clin Infect Dis. 2008;47(8):1026–1031. doi: 10.1086/591970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Meng XJ, Wiseman B, Elvinger F, et al. Prevalence of antibodies to hepatitis E virus in veterinarians working with swine and in normal blood donors in the United States and other countries. J Clin Microbiol. 2002;40(1):117–122. doi: 10.1128/JCM.40.1.117-122.2002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Renou C, Cadranel JF, Bourlière M, et al. Possible zoonotic transmission of hepatitis E from pet pig to its owner. Emerg Infect Dis. 2007;13(7):1094–1096. doi: 10.3201/eid1307.070063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Said B, Ijaz S, Kafatos G, et al. Hepatitis E Incident Investigation Team Hepatitis E outbreak on cruise ship. Emerg Infect Dis. 2009;15(11):1738–1744. doi: 10.3201/eid1511.091094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Diez-Valcarce M, Kokkinos P, Söderberg K, et al. Occurrence of human enteric viruses in commercial mussels at retail level in three European countries. Food Environ Virol. 2012;4(2):73–80. doi: 10.1007/s12560-012-9078-9. [DOI] [PubMed] [Google Scholar]
- 95.Crossan C, Baker PJ, Craft J, Takeuchi Y, Dalton HR, Scobie L. Hepatitis E virus genotype 3 in shellfish, United Kingdom. Emerg Infect Dis. 2012;18(12):2085–2087. doi: 10.3201/eid1812.120924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Krain LJ, Atwell JE, Nelson KE, Labrique AB. Fetal and neonatal health consequences of vertically transmitted hepatitis E virus infection. Am J Trop Med Hyg. 2014;90(2):365–370. doi: 10.4269/ajtmh.13-0265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Ruggeri FM, Di Bartolo I, Ponterio E, Angeloni G, Trevisani M, Ostanello F. Zoonotic transmission of hepatitis E virus in industrialized countries. New Microbiol. 2013;36(4):331–344. [PubMed] [Google Scholar]
- 98.Menendez C, Sanchez-Tapias JM, Kahigwa E, et al. Prevalence and mother-to-infant transmission of hepatitis viruses B, C, and E in Southern Tanzania. J Med Virol. 1999;58(3):215–220. doi: 10.1002/(sici)1096-9071(199907)58:3<215::aid-jmv5>3.0.co;2-k. [DOI] [PubMed] [Google Scholar]
- 99.Kumar RM, Uduman S, Rana S, Kochiyil JK, Usmani A, Thomas L. Sero-prevalence and mother-to-infant transmission of hepatitis E virus among pregnant women in the United Arab Emirates. Eur J Obstet Gynecol Reprod Biol. 2001;100(1):9–15. doi: 10.1016/s0301-2115(01)00448-1. [DOI] [PubMed] [Google Scholar]
- 100.Rayis DA, Jumaa AM, Gasim GI, Karsany MS, Adam I. An outbreak of hepatitis E and high maternal mortality at Port Sudan, Eastern Sudan. Pathog Glob Health. 2013;107(2):66–68. doi: 10.1179/2047773213Y.0000000076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Cardenas I, Means RE, Aldo P, et al. Viral infection of the placenta leads to fetal inflammation and sensitization to bacterial products predisposing to preterm labor. J Immunol. 2010;185(2):1248–1257. doi: 10.4049/jimmunol.1000289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Cardenas I, Mor G, Aldo P, et al. Placental viral infection sensitizes to endotoxin-induced pre-term labor: a double hit hypothesis. Am J Reprod Immunol. 2011;65(2):110–117. doi: 10.1111/j.1600-0897.2010.00908.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Aggarwal R, Naik SR. Hepatitis E: does person-to-person spread occur? Indian J Gastroenterol. 1992;11(3):109–112. [PubMed] [Google Scholar]
- 104.Rodrigues A, Brun H, Sandstrom A. Risk factors for cholera infection in the initial phase of an epidemic in Guinea-Bissau: protection by lime juice. Am J Trop Med Hyg. 1997;57(5):601–604. doi: 10.4269/ajtmh.1997.57.601. [DOI] [PubMed] [Google Scholar]
- 105.Somani SK, Aggarwal R, Naik SR, Srivastava S, Naik S. A serological study of intrafamilial spread from patients with sporadic hepatitis E virus infection. J Viral Hepat. 2003;10(6):446–449. doi: 10.1046/j.1365-2893.2003.00458.x. [DOI] [PubMed] [Google Scholar]
- 106.Krawczynski K, Aggarwal R, Kamili S. Hepatitis E. Infect Dis Clin North Am. 2000;14(3):669–687. doi: 10.1016/s0891-5520(05)70126-4. [DOI] [PubMed] [Google Scholar]
- 107.Velázquez O, Stetler HC, Avila C, et al. Epidemic transmission of enterically transmitted non-A, non-B hepatitis in Mexico, 1986–1987. JAMA. 1990;263(24):3281–3285. [PubMed] [Google Scholar]
- 108.Emerson SU, Purcell RH. Hepatitis E virus. Rev Med Virol. 2003;13(3):145–154. doi: 10.1002/rmv.384. [DOI] [PubMed] [Google Scholar]
- 109.Kamar N, Bendall R, Legrand-Abravanel F, et al. Hepatitis E. Lancet. 2012;379(9835):2477–2488. doi: 10.1016/S0140-6736(11)61849-7. [DOI] [PubMed] [Google Scholar]
- 110.Khuroo MS, Kamili S, Yattoo GN. Hepatitis E virus infection may be transmitted through blood transfusions in an endemic area. J Gastroenterol Hepatol. 2004;19(7):778–784. doi: 10.1111/j.1440-1746.2004.03437.x. [DOI] [PubMed] [Google Scholar]
- 111.Takeda H, Matsubayashi K, Sakata H, et al. A nationwide survey for prevalence of hepatitis E virus antibody in qualified blood donors in Japan. Vox Sang. 2010;99(4):307–313. doi: 10.1111/j.1423-0410.2010.01362.x. [DOI] [PubMed] [Google Scholar]
- 112.Gotanda Y, Iwata A, Ohnuma H, et al. Ongoing subclinical infection of hepatitis E virus among blood donors with an elevated alanine aminotransferase level in Japan. J Med Virol. 2007;79(6):734–742. doi: 10.1002/jmv.20834. [DOI] [PubMed] [Google Scholar]
- 113.Boxall E, Herborn A, Kochethu G, et al. Transfusion-transmitted hepatitis E in a ‘nonhyperendemic’ country. Transfus Med. 2006;16(2):79–83. doi: 10.1111/j.1365-3148.2006.00652.x. [DOI] [PubMed] [Google Scholar]
- 114.Vollmer T, Diekmann J, Johne R, Eberhardt M, Knabbe C, Dreier J. Novel approach for detection of hepatitis E virus infection in German blood donors. J Clin Microbiol. 2012;50(8):2708–2713. doi: 10.1128/JCM.01119-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Nelson KE. Transmission of hepatitis E virus by transfusion: what is the risk? Transfusion. 2014;54(1):8–10. doi: 10.1111/trf.12504. [DOI] [PubMed] [Google Scholar]
- 116.Bendall R, Ellis V, Ijaz S, Ali R, Dalton H. A comparison of two commercially available anti-HEV IgG kits and a re-evaluation of anti-HEV IgG seroprevalence data in developed countries. J Med Virol. 2010;82(5):799–805. doi: 10.1002/jmv.21656. [DOI] [PubMed] [Google Scholar]
- 117.Rossi-Tamisier M, Moal V, Gerolami R, Colson P. Discrepancy between anti-hepatitis E virus immunoglobulin G prevalence assessed by two assays in kidney and liver transplant recipients. J Clin Virol. 2013;56(1):62–64. doi: 10.1016/j.jcv.2012.09.010. [DOI] [PubMed] [Google Scholar]
- 118.Wu WC, Su CW, Yang JY, Lin SF, Chen JY, Wu JC. Application of serologic assays for diagnosing acute hepatitis E in national surveillance of a nonendemic area. J Med Virol. 2014;86(4):720–728. doi: 10.1002/jmv.23785. [DOI] [PubMed] [Google Scholar]
- 119.Favorov MO, Fields HA, Purdy MA, et al. Serologic identification of hepatitis E virus infections in epidemic and endemic settings. J Med Virol. 1992;36(4):246–250. doi: 10.1002/jmv.1890360403. [DOI] [PubMed] [Google Scholar]
- 120.Dawson GJ, Mushahwar IK, Chau KH, Gitnick GL. Detection of long-lasting antibody to hepatitis E virus in a US traveller to Pakistan. Lancet. 1992;340(8816):426–427. doi: 10.1016/0140-6736(92)91507-5. [DOI] [PubMed] [Google Scholar]
- 121.Slot E, Hogema BM, Riezebos-Brilman A, Kok TM, Molier M, Zaaijer HL. Silent hepatitis E virus infection in Dutch blood donors, 2011 to 2012. Euro Surveill. 2013;18(31):20550. doi: 10.2807/1560-7917.es2013.18.31.20550. [DOI] [PubMed] [Google Scholar]
- 122.Legrand-Abravanel F, Thevenet I, Mansuy JM, et al. Good performance of immunoglobulin M assays in diagnosing genotype 3 hepatitis E virus infections. Clin Vaccine Immunol. 2009;16(5):772–774. doi: 10.1128/CVI.00438-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Drobeniuc J, Meng J, Reuter G, et al. Serologic assays specific to immunoglobulin M antibodies against hepatitis E virus: pangenotypic evaluation of performances. Clin Infect Dis. 2010;51(3):e24–e27. doi: 10.1086/654801. [DOI] [PubMed] [Google Scholar]
- 124.Herremans M, Bakker J, Duizer E, Vennema H, Koopmans MP. Use of serological assays for diagnosis of hepatitis E virus genotype 1 and 3 infections in a setting of low endemicity. Clin Vaccine Immunol. 2007;14(5):562–568. doi: 10.1128/CVI.00231-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Zhou YH, Purcell RH, Emerson SU. An ELISA for putative neutralizing antibodies to hepatitis E virus detects antibodies to genotypes 1, 2, 3, and 4. Vaccine. 2004;22(20):2578–2585. doi: 10.1016/j.vaccine.2003.12.017. [DOI] [PubMed] [Google Scholar]
- 126.Takahashi M, Kusakai S, Mizuo H, et al. Simultaneous detection of immunoglobulin A (IgA) and IgM antibodies against hepatitis E virus (HEV) Is highly specific for diagnosis of acute HEV infection. J Clin Microbiol. 2005;43(1):49–56. doi: 10.1128/JCM.43.1.49-56.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Zhang S, Tian D, Zhang Z, et al. Clinical significance of anti-HEV IgA in diagnosis of acute genotype 4 hepatitis E virus infection negative for anti-HEV IgM. Dig Dis Sci. 2009;54(11):2512–2518. doi: 10.1007/s10620-008-0657-4. [DOI] [PubMed] [Google Scholar]
- 128.Li S, Tang X, Seetharaman J, et al. Dimerization of hepatitis E virus capsid protein E2s domain is essential for virus-host interaction. PLoS Pathog. 2009;5(8):e1000537. doi: 10.1371/journal.ppat.1000537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Fogeda M, de Ory F, Avellón A, Echevarría JM. Differential diagnosis of hepatitis E virus, cytomegalovirus and Epstein-Barr virus infection in patients with suspected hepatitis E. J Clin Virol. 2009;45(3):259–261. doi: 10.1016/j.jcv.2009.05.022. [DOI] [PubMed] [Google Scholar]
- 130.Hyams C, Mabayoje DA, Copping R, et al. Serological cross reactivity to CMV and EBV causes problems in the diagnosis of acute hepatitis E virus infection. J Med Virol. 2014;86(3):478–483. doi: 10.1002/jmv.23827. [DOI] [PubMed] [Google Scholar]
- 131.Abravanel F, Chapuy-Regaud S, Lhomme S, et al. Performance of anti-HEV assays for diagnosing acute hepatitis E in immunocompromised patients. J Clin Virol. 2013;58(4):624–628. doi: 10.1016/j.jcv.2013.10.003. [DOI] [PubMed] [Google Scholar]
- 132.Sarin SK, Kumar M, Hepatitis E. In: Zakim and Boyer’s Hepatology: A Textbook of Liver Disease. 5th ed. Boyer T, Manns M, Wright TL, editors. Philadelphia, PA: Saunders; 2006. pp. 693–724. [Google Scholar]
- 133.Huang S, Zhang X, Jiang H, et al. Profile of acute infectious markers in sporadic hepatitis E. PLoS One. 2010;5(10):e13560. doi: 10.1371/journal.pone.0013560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Lan X, Yang B, Li BY, Yin XP, Li XR, Liu JX. Reverse transcription-loop-mediated isothermal amplification assay for rapid detection of hepatitis E virus. J Clin Microbiol. 2009;47(7):2304–2306. doi: 10.1128/JCM.00498-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Jothikumar N, Cromeans TL, Robertson BH, Meng XJ, Hill VR. A broadly reactive one-step real-time RT-PCR assay for rapid and sensitive detection of hepatitis E virus. J Virol Methods. 2006;131(1):65–71. doi: 10.1016/j.jviromet.2005.07.004. [DOI] [PubMed] [Google Scholar]
- 136.Gyarmati P, Mohammed N, Norder H, Blomberg J, Belák S, Widén F. Universal detection of hepatitis E virus by two real-time PCR assays: TaqMan and Primer-Probe Energy Transfer. J Virol Methods. 2007;146(1–2):226–235. doi: 10.1016/j.jviromet.2007.07.014. [DOI] [PubMed] [Google Scholar]
- 137.Baylis SA, Hanschmann KM, Blümel J, Nübling CM, HEV Collaborative Study Group Standardization of hepatitis E virus (HEV) nucleic acid amplification technique-based assays: an initial study to evaluate a panel of HEV strains and investigate laboratory performance. J Clin Microbiol. 2011;49(4):1234–1239. doi: 10.1128/JCM.02578-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Baylis SA, Blümel J, Mizusawa S, et al. HEV Collaborative Study Group World Health Organization International Standard to harmonize assays for detection of hepatitis E virus RNA. Emerg Infect Dis. 2013;19(5):729–735. doi: 10.3201/eid1905.121845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Abravanel F, Chapuy-Regaud S, Lhomme S, et al. Performance of two commercial assays for detecting hepatitis E virus RNA in acute or chronic infections. J Clin Microbiol. 2013;51(6):1913–1916. doi: 10.1128/JCM.00661-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Gerolami R, Borentain P, Raissouni F, Motte A, Solas C, Colson P. Treatment of severe acute hepatitis E by ribavirin. J Clin Virol. 2011;52(1):60–62. doi: 10.1016/j.jcv.2011.06.004. [DOI] [PubMed] [Google Scholar]
- 141.Péron JM, Dalton H, Izopet J, Kamar N. Acute autochthonous hepatitis E in western patients with underlying chronic liver disease: a role for ribavirin? J Hepatol. 2011;54(6):1323–4. doi: 10.1016/j.jhep.2011.01.009. author reply 1324. [DOI] [PubMed] [Google Scholar]
- 142.Anty R, Ollier L, Péron JM, et al. First case report of an acute genotype 3 hepatitis E infected pregnant woman living in South-Eastern France. J Clin Virol. 2012;54(1):76–78. doi: 10.1016/j.jcv.2012.01.016. [DOI] [PubMed] [Google Scholar]
- 143.Kamar N, Garrouste C, Haagsma EB, et al. Factors associated with chronic hepatitis in patients with hepatitis E virus infection who have received solid organ transplants. Gastroenterology. 2011;140(5):1481–1489. doi: 10.1053/j.gastro.2011.02.050. [DOI] [PubMed] [Google Scholar]
- 144.Jagjit Singh GK, Ijaz S, Rockwood N, et al. Chronic Hepatitis E as a cause for cryptogenic cirrhosis in HIV. J Infect. 2013;66(1):103–106. doi: 10.1016/j.jinf.2011.11.027. [DOI] [PubMed] [Google Scholar]
- 145.Parvez MK. Chronic hepatitis E infection: risks and controls. Intervirology. 2013;56(4):213–216. doi: 10.1159/000349888. [DOI] [PubMed] [Google Scholar]
- 146.Chaillon A, Sirinelli A, De Muret A, Nicand E, d’Alteroche L, Goudeau A. Sustained virologic response with ribavirin in chronic hepatitis E virus infection in heart transplantation. J Heart Lung Transplant. 2011;30(7):841–843. doi: 10.1016/j.healun.2011.03.013. [DOI] [PubMed] [Google Scholar]
- 147.Mallet V, Louvet A, Chakvetadze C, et al. Ribavirin treatment forchronic hepatitis E: a case-series. Hepatology. 2010;52(Suppl 1):869A. [Google Scholar]
- 148.Schildgen O, Müller A, Simon A. Chronic hepatitis E and organ transplants. N Engl J Med. 2008;358(23):2521–2. doi: 10.1056/NEJMc080634. author reply 2522. [DOI] [PubMed] [Google Scholar]
- 149.Alric L, Bonnet D, Beynes-Rauzy O, Izopet J, Kamar N. Definitive clearance of a chronic hepatitis E virus infection with ribavirin treatment. Am J Gastroenterol. 2011;106(8):1562–1563. doi: 10.1038/ajg.2011.158. [DOI] [PubMed] [Google Scholar]
- 150.Tan HH, Leong HN, Tan BH, et al. Chronic hepatitis E infection resulting in graft failure in a liver transplant tourist. Case Rep Transplant. 2011;2011:654–792. doi: 10.1155/2011/654792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Fujiwara S, Yokokawa Y, Morino K, Hayasaka K, Kawabata M, Shimizu T. Chronic hepatitis E: a review of the literature. J Viral Hepat. 2014;21(2):78–89. doi: 10.1111/jvh.12156. [DOI] [PubMed] [Google Scholar]
- 152.Riezebos-Brilman A, Puchhammer-Stöckl E, van der Weide HY, et al. Chronic hepatitis E infection in lung transplant recipients. J Heart Lung Transplant. 2013;32(3):341–346. doi: 10.1016/j.healun.2012.11.027. [DOI] [PubMed] [Google Scholar]
- 153.Pischke S, Stiefel P, Franz B, et al. Chronic hepatitis e in heart transplant recipients. Am J Transplant. 2012;12(11):3128–3133. doi: 10.1111/j.1600-6143.2012.04200.x. [DOI] [PubMed] [Google Scholar]
- 154.Shrestha MP, Scott RM, Joshi DM, et al. Safety and efficacy of a recombinant hepatitis E vaccine. N Engl J Med. 2007;356(9):895–903. doi: 10.1056/NEJMoa061847. [DOI] [PubMed] [Google Scholar]
- 155.Kamar N, Legrand-Abravanel F, Izopet J, Rostaing L. Hepatitis E virus: what transplant physicians should know. Am J Transplant. 2012;12(9):2281–2287. doi: 10.1111/j.1600-6143.2012.04078.x. [DOI] [PubMed] [Google Scholar]