

Abstract
Fungal arthritis is an uncommon yet serious disorder in the newborn. Delay in diagnosis and management can lead to significant morbidity. We report our experience with management of two such cases. Two preterm neonates with multifocal arthritis caused by Candida were studied. Diagnosis was made by clinical examination, laboratory investigations, radiological investigations and culture. Both were treated by aspiration, arthrotomy and antifungal therapy. One patient recovered fully from the infection while the other had growth disturbances resulting in limb length inequality at recent followup. Prompt and expeditious evacuation of pus from joints and antifungal therapy is imperative for treatment. Associated osteomyelitis leads to further difficulty in treatment.
Keywords: Arthritis, candidiasis, neonates
INTRODUCTION
Septic arthritis in neonates and infants has increased in prevalence and severity over time and has important functional and social handicap.1,2 It is caused by a variety of microorganisms, most common being gram-positive, followed by gram-negative bacteria and fungi.3,4 However, there is a report of an important etiologic shift, with gram-negative organisms constituting 33%, gram-positive 20%, and fungal organisms 7%.5 Septic arthritis caused by Candida albicans is not seen widely and the actual incidence is not known.2 However, there are reports of increasing prevalence, from a few reported cases to almost 11 fold increase in the last 15 years.6 In almost all studies C. albicans is the most common fungal pathogen (53%),4,7,8 though other agents such as Candida tropicalis, Candida parapsilosis, Candida glabrata, Candida guilliermondii, and Candida krusei have also been implicated.1,2,7 This is mostly seen in premature infants with incidence of 10-25% in low birth weights infants,6,7 with neonatal septicemia having a long history of hospitalization. This predisposes the child to frequent colonization with microorganisms hence there is increased prevalence of neonatal septicemia. Other associated risk factors are prolonged hyperalimentation, gastrointestinal defects, prolonged intravenous (IV) catheters (up to 67%, and increase survival rates if removed under 3 days), long term steroid and antibiotic therapy and immunosuppression. Complications of disseminated neonatal candidiasis include arthritis, endocarditis, meningitis, endophthalmitis and respiratory disorders.1,2,3,4,5,6,7
Nearly, 85% pediatric fungal arthritis occurs in infants.8 In general, two forms of arthritis are seen primary as a result of acute candidiasis seen in hospitalized, preterm, septicemic infants with indwelling catheters and secondary presenting later following disseminated candidiasis.9
It mostly occurs as mono or oligoarthritis with knee joint most commonly involved. It can also lead to osteomyelitis in 70-80% of cases, which can be a simultaneous occurrence or late manifestation of hematogenously disseminated Candidiasis.8 Though the incidence of osteomyelitis has reduced over time, this condition requires prompt diagnosis and aggressive treatment to prevent and overcome the potential crippling sequel associated with it.9
CASE REPORTS
Case 1
A 25-day-old preterm neonate with a birth weight of 2.7 kg admitted since birth for neonatal septicemia elsewhere presented with pain and swelling of the left hip with the loss of spontaneous movements of the left lower extremity from 2 weeks. On clinical examination, there was swelling, pain on passive movements and instability on examination of the left hip (Barlow's positive). There was pain on passive movements of right shoulder as well.
X-ray pelvis with both hips anteroposterior (AP) view showed subluxation of the left hip while the right hip was lateralized. There were changes of early osteomyelitis in the upper end of the left femur [Figure 1a]. While the X-ray of right shoulder AP and axial views showed no abnormality Ultrasound of both hips revealed left sided intra-capsular collection with synovitis. Laboratory findings showed total leucocyte count (TLC) as 13,000/cu mm, C-reactive protein (CRP) as 4.42 mg/dl, erythrocyte sedimentation rate (ESR) as 90 mm/1st h. Blood culture was positive for C. albicans.
Figure 1.

(Case 1) - X-ray pelvis both hip joints anteroposterior view showing (a) left hip subluxation, osteomyelitis upper end femur left side (b) followup at 2 years and 8 months. There is appearance of capital femoral epiphysis on both sides and coxa magna left side
The child was taken up for aspiration and arthrotomy of the left hip. Purulent material and inflamed synovium obtained from the hip joint was sent for culture which was positive for Candida, while the histopathological examination of the inflamed synovium revealed synovitis. Right shoulder was also aspirated and was negative for any growth. Patient was treated with amphotericin B and fluconazole for 6 weeks. Hip was protected in Pavlik harness for 3 months.
Repeat laboratory investigations after 4 weeks showed improvement with TLC-4600/cu mm, CRP-2.2 mg/dl, ESR-15 mm/h. Pain and swelling in the left hip reduced progressively. The hip was stabilized in the Pavlik harness within 1 week and he regained spontaneous movements 2 months following arthrotomy. Hip was protected in a hip abduction brace for 3 months after discontinuing the Pavlik harness.
At followup, the child started waking at 14 months of age. At the last followup at 2 years 8 months of age, the child was ambulatory without a limp. Hips were stable to examination and had full and symmetric range of movements. He could squat and sit cross legged. X-ray pelvis with both hips showed ossified capital epiphysis on both sides. There was mild coxa magna on the left side [Figure 1b]. Right shoulder had full and painless movements.
Case 2
A 1 month 20 days old infant presented with multiple joint swellings involving bilateral shoulders, elbows, knees, ankles and loss of spontaneous movements and painful movements of the left hip for 1 month. He was a preterm child with a birth weight of 2.4 kg and was diagnosed as a case of neonatal septicemia and kept in a neonatal intensive care unit for 28 days before being referred to our hospital. Prior to being referred his left knee was aspirated which was positive for Candida on culture. The child was irritable and had pain on passive movements of both hip joints and instability on the left side. The left knee was also painful on passive movements and had effusion. There was no pain on movements of the right knee. The upper limbs had mild swelling around the elbows and shoulders but the child had spontaneous movements of both upper limbs.
X-ray pelvis with both hips AP view revealed the hip was lateralized on both sides with early changes of osteomyelitis in the upper ends of femur bilaterally and osteomyelitis of the lower end of femur on the right side and upper end of the tibia on the left side [Figure 2a]. Ultrasound of the left hip revealed a collection with synovitis.
Figure 2.
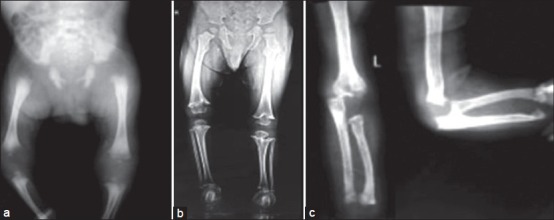
(Case 2) - (a) Preoperative radiograph of both lower limbs anteroposterior view showing osteomyelitis of lower end of femur on right side and upper end of tibia on the left side. Hip was lateralized on both sides (b) Standing orthogram at 2 years age showing coxa valga left femur, growth arrest proximal tibia left and distal femur right (c) X-ray left elbow (anteroposterior and later views) showing destruction of lower end of humerus
Laboratory investigations showed CRP 15.6 mg/dl, white blood cells (WBC) 11920/cu mm.
The child was taken up for aspiration and drainage of the left hip and repeat aspiration of left knee. Purulent fluid was obtained on aspiration of the knee and on arthrotomy of the hip joint. The pus as well as the synovial tissue was sent for culture. Pus culture and tissue culture from the hip was negative for any growth as was the aspirate from the knee.
Clinical examination and laboratory investigations of leucocytosis and raised CRP were suggestive of some infection. Fungal etiology was based on the previous culture from the left knee. The patient was started on antifungal therapy Amphotericin B which was continued for 5 weeks.
Repeat laboratory investigations after 10 days showed improvement with CRP 2.35 mg/dl, WBC 9450/cu mm. The hip joint was stabilized in the Pavlik harness within a week and the pain and swelling reduced progressively with time. The child regained spontaneous movements of hip within 4 weeks following arthrotomy. The hip was protected in Pavlik harness for a total of 2 months. A hip abduction brace was used for another 3 months for protection of the hips.
Followup examination revealed that the child had started walking without support at 16 months of age. At the most current followup at 2 years of age, the patient was ambulatory without support and walked without a limp. Both hips were stable to examination and had full range of motion. The patient could squat, but had difficulty in sitting cross legged. Galeazzi sign was positive, with shortening of right femur. There was overall minimal limb length inequality.
X-ray showed well formed capital femoral epiphysis, with coxa valga on the left, growth arrest of the distal femur on the right and at the proximal tibia on the left [Figure 2b]. There was no angular deformity present in either lower limb. Left elbow had a cubitus varus deformity, with deformation of the lower end of the humerus [Figure 2c]. The elbow however had full and painless range of movement.
DISCUSSION
The examination findings confirmed the multifocal involvement of Candida arthritis, especially in premature infants.4 In lab investigations, CRP is a better indicator then ESR because it increases immediately following infection and decreases as the infection subsides. Timely diagnosis and intervention by aspiration, arthrotomy and antifungal therapy goes a long way in salvaging a joint.5 In the above cases, the joint could be salvaged despite presenting after 2 weeks. IV amphotericin B remains the standard treatment for Candida sepsis.10 IV or oral fluconazole is an alternative to amphotericin B.11,12 While antibiotic resistance to fluconazole has been found to be from 18% to 24% no resistance was found against amphotericin B.11,12
Though Candida if present can grow on routine bacteriological media,13 it is advisable to screen “at-risk” neonates with both bacterial and fungal cultures.
Neonatal septic arthritis has a potential for disastrous sequels with long term disability, especially with joint destruction, instability and growth disturbances.9 Other conditions affecting the neonatal joints such as multifocal osteomyelitis, chronic granulomatous disease, neonatal onset multisystem inflammatory disease, leukemia, eosinophilic granuloma, juvenile rheumatoid arthritis, Langerhans cell histiocytosis should also be kept in mind. Progress of infection, nonspecificity of laboratory data of culture negative septic arthritis (up to 18-48%),14 and failure to recognize Candida as a potential pathogen may also lead to delay in diagnosis and complications.15
Fungal arthritis should be kept in mind while treating a neonatal septic arthritis case especially in “at-risk” neonates who are preterm, low birth weight with a long history of hospitalization having multifocal involvement and have blood and pus samples, which are negative for bacterial culture. From our experience in these cases proper timely diagnosis and aggressive line of treatment with arthrotomy and long term duration of Amphotericin B and Fluconazole as an alternative should be used with a prolonged followup to monitor and treat the sequels of arthritis and osteomyelitis.
Footnotes
Source of Support: Nil.
Conflict of Interest: None.
REFERENCES
- 1.Noyes FR, McCabe JD, Fekety FR., Jr Acute Candida arthritis. Report of a case and use of amphotericin B. J Bone Joint Surg Am. 1973;55:169–76. [PubMed] [Google Scholar]
- 2.Cuéllar ML, Silveira LH, Espinoza LR. Fungal arthritis. Ann Rheum Dis. 1992;51:690–7. doi: 10.1136/ard.51.5.690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Svirsky-Fein S, Langer L, Milbauer B, Khermosh O, Rubinstein E. Neonatal osteomyelitis caused by Candida tropicalis. Report of two cases and review of the literature. J Bone Joint Surg Am. 1979;61:455–9. [PubMed] [Google Scholar]
- 4.Herring JA. Tachdijan's Paediatric Orthopaedics. In: Herring JA, editor. 3rd ed. Philadelphia: WB Saunders Co.; 2002. pp. 1841–77. [Google Scholar]
- 5.Deshpande SS, Taral N, Modi N, Singrakhia M. Changing epidemiology of neonatal septic arthritis. J Orthop Surg (Hong Kong) 2004;12:10–3. doi: 10.1177/230949900401200103. [DOI] [PubMed] [Google Scholar]
- 6.Toopey WH. UCSF Medical centre Manual. 8th ed. California: 2003. Candidiasis in the newborn. Intensive care Nursery House Staff Manual; pp. 128–9. [Google Scholar]
- 7.Stamos JK, Rowley AH. Candidemia in a pediatric population. Clin Infect Dis. 1995;20:571–5. doi: 10.1093/clinids/20.3.571. [DOI] [PubMed] [Google Scholar]
- 8.Lambertus M, Thordarson D, Goetz MB. Fungal prosthetic arthritis: Presentation of two cases and review of the literature. Rev Infect Dis. 1988;10:1038–43. doi: 10.1093/clinids/10.5.1038. [DOI] [PubMed] [Google Scholar]
- 9.Ciftdemir NA. Fungal septic arthritis in the newborn. Turk Arch Pediatr. 2011;46:92–93. [Google Scholar]
- 10.Stoll BJ, Gordon T, Korones SB, Shankaran S, Tyson JE, Bauer CR, et al. Late-onset sepsis in very low birth weight neonates: A report from the National Institute of Child Health and Human Development Neonatal Research Network. J Pediatr. 1996;129:63–71. doi: 10.1016/s0022-3476(96)70191-9. [DOI] [PubMed] [Google Scholar]
- 11.Hsieh WB, Leung C. Candidal arthritis after complete treatment of systemic candidiasis. J Chin Med Assoc. 2005;68:191–4. doi: 10.1016/S1726-4901(09)70248-5. [DOI] [PubMed] [Google Scholar]
- 12.Narain S. Neonatal systemic candidiasis in a tertiary care centre. Indian J Med Microbiol. 2003;21:56–8. [PubMed] [Google Scholar]
- 13.Fisher F, Cook NB. 1st ed. Philadelphia: WB Saunders Company; 1998. Fundamentals of Diagnostic Mycology; p. 200. [Google Scholar]
- 14.Lyon RM, Evanich JD. Culture-negative septic arthritis in children. J Pediatr Orthop. 1999;19:655–9. [PubMed] [Google Scholar]
- 15.Ho NK, Low YP, See HF. Septic arthritis in the newborn: A 17 years’ clinical experience. Singapore Med J. 1989;30:356–8. [PubMed] [Google Scholar]