

Abstract
The Gubbio Study is a prospective epidemiological study on the population residing in the city of Gubbio, Italy. Original objectives of the study were the control of hypertension and the role of cellular electrolyte handling in hypertension. Other objectives were added during the 30-year activity of the study. The original target cohort consists of individuals aged ≥ 5 years residing within the medieval walls of the city. To complete family genealogies, individuals residing outside the city were also included. Three active screenings (exams) were conducted. A total of 5376 individuals (response rate 92%) participated in Exam 1 which was performed in 1983–86. Follow-up exams were completed between 1989–92 and 2001–2007. Data categories included demographics, personal and family medical history, lifestyle habits, education, type of work, anthropometry, blood pressure, pulse rate, blood biochemistry, urine biochemistry and special investigations on cellular electrolyte handling. Electrocardiogram, echocardiogram, 24-h ambulatory blood pressure and uroflowmetry were performed in selected subgroups defined by age and/or sex. Data about hospitalizations, mortality and causes of death were collected starting from completion of Exam 1. The study shared the data with other studies.
Why was the Gubbio cohort set up?
The Gubbio Study is a prospective investigation ongoing since 1983 in the city of Gubbio, a medieval hill town in the northern central part of Italy (Figure 1). The study was designed to conduct cross-sectional and longitudinal epidemiological investigations in a sample of the general population. At the time of its design, hypertension and hypertension-related vascular disease were highly prevalent in Italy.1,2 Thus, the main objectives of the study were: (i) to support and to improve the detection and the control of hypertension in the population; and (ii) to investigate the role of the cellular handling of sodium and other electrolytes in the pathogenesis of hypertension.
Figure 1.

Map with location of the city of Gubbio
Our understanding of kidney dysfunction as a disorder often associated with hypertension and as a predictor of cardiovascular disease has grown during the 30-year activity of the study.3 Therefore, indices of kidney dysfunction were added to the list of the objectives of the study with main focus on urinary albumin excretion and on estimates of glomerular filtration rate derived from serum creatinine. The study also collected information on the genealogy of families thus allowing to investigate the familial aggregation of hypertension and other variables.
Who is in the Gubbio cohort?
An invitation to participate in the study was extended to the entire population aged 5 years and over residing within the medieval walls of the city of Gubbio. Names and addresses were provided by the municipal authority through the municipal census lists. Following an invitation letter signed by the town's mayor explaining the nature of the study, an employee visited each family to illustrate the study's aims and procedures and make an appointment for all family members willing to participate. In order to gather data in families, the same procedure was extended to first-degree relatives (parents, siblings and offspring) residing outside the medieval city. Baseline examination (Exam 1) was performed between 1983 and 1986.4 A total of 5376 individuals participated in Exam 1: 3537 residents within the city and 1839 residents outside the city (response rate 92%). The group of residents within the city and the group of residents outside had similar distribution of sex (female: 55% and 52%, respectively); ages 5–17 years (15% and 15%), ages 18–65 years (67% and 71%), and ages >65 years (18% and 14%). Figure 2 shows the distribution of age by sex in the whole Exam 1 cohort with city residents and non-residents combined together.
Figure 2.
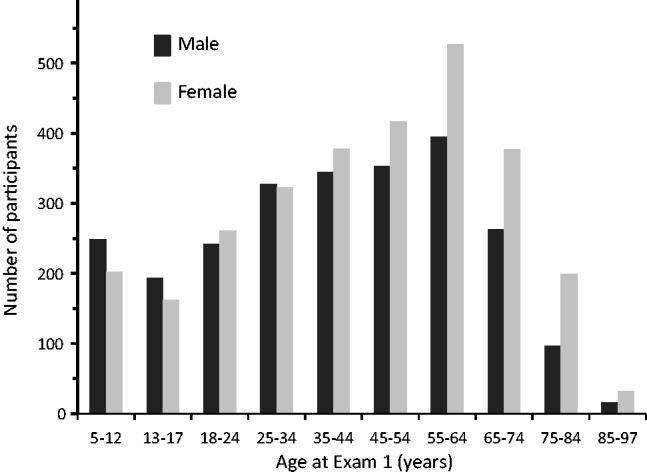
Number of participants in Exam 1 by sex and age
How often have they been followed-up?
The first follow-up examination (Exam 2) was performed from 1989 to 1992. The invitation to participate in Exam 2 was sent to all individuals in the Exam 1 cohort, both those residing within and outside the city. Of the 5376 individuals in the Exam 1 cohort, 418 died before Exam 2; 3727 individuals participated in Exam 2 (response rate 75%).
The response rate in Exam 2 was similar in men and women (75% and 76%, respectively) and slightly higher for ages 18–65 years compared with ages 5–17 years and ages >65 years (77%, 70% and 73%, respectively). Table 1 shows socio-demographic data in non-responders and responders. The response rate in Exam 2 was higher for non-residents than in those residing within the city (81% and 72%, respectively). This difference was consistent in separate analyses for females (82% and 72%), males (82% and 70%), ages 5–17 years (79% and 66%), ages 18–65 years (83% and 73%) and ages >65 years (78% and 70%), respectively. Median of follow-up duration between Exam 1 and Exam 2 was 6 years in both sexes and in all age groups for both residents and non-residents.
Table 1.
Socio-demographic data by sex and age for individuals from Exam 1 who did not participate in Exam 2 and individuals who participated in Exam 2 (non-responders and responders, respectively)
| Women |
Men |
|||
|---|---|---|---|---|
| Non-responders | Responders | Non-responders | Responders | |
| Aged 5–17 years, n | 108 | 256 | 130 | 311 |
| Education, years | 5.3 | 5.0 | 4.9 | 5.0 |
| Student, % | 80.6% | 84.8% | 88.5% | 87.1% |
| Aged 18–65 years, n | 416 | 1488 | 403 | 1214 |
| Education, years | 8.7 | 7.2 | 9.7 | 8.2 |
| Homemaker,% | 34.6% | 48.7% | 0.0% | 0.1% |
| Farmer or blue-collar worker, % | 6.7% | 5.1% | 22.6% | 34.2% |
| White-collar worker, % | 39.9% | 32.3% | 47.6% | 41.7% |
| Professional or manager, % | 2.2% | 0.5% | 6.7% | 3.9% |
| Aged >65 years, n | 132 | 274 | 42 | 184 |
| Education, years | 4.9 | 4.2 | 4.9 | 5.3 |
| Homemaker,% | 43.2% | 46.4% | 0.0% | 0.0% |
| Retired, % | 52.3% | 44.9% | 85.7% | 84.8% |
In addition to the 3727 individuals who previously participated in Exam 1, an additional cohort of 1455 residents outside the city volunteered for Exam 2. This volunteer cohort, compared with the Exam 1 cohort, was similar for distribution of sex (female: 53% and 54%), ages 5–17 years (15% and 15%), ages 18–65 years (70% and 68%) and ages >65 years (15% and 17%), respectively. Likewise in the Exam 1 cohort, the most prevalent occupation in this volunteer cohort was as follows: student for males and females aged 5–17 years (90% and 90%, respectively); homemaker for women aged 18–65 years and >65 years (40% and 53%, respectively); white-collar worker for men aged 18–65 years (46%); retirement for men aged >65 years (84%). Thus, the Exam 1 cohort and this volunteer cohort were combined in analyses.
The second follow-up examination (Exam 3) was performed from 2001 to 2007. The invitation to participate in Exam 3 was extended only to two age-strata: the 2415 individuals aged 35–64 years in Exam 1 (residing either within or outside the city); and the 1641 individuals aged 45–64 years at Exam 2 (residing either within or outside the city). These two target groups partially overlapped because 1247 individuals fell into both age-strata. Thus, the overall target cohort of Exam 3 consisted of 2887 individuals as follows: 1247 individuals aged 35–64 years at Exam 1 and aged 45–64 years at Exam 2; 1168 individuals aged 35–64 years at Exam 1 but aged other than 45–64 years at Exam 2; and 472 individuals aged 45–64 years at Exam 2 but aged other than 35–64 years at Exam 1. The diagram in Figure 3 summarizes data about participants in the three exams. Of the 2887 individuals of the target cohort, 580 died before Exam 3 so that 1765 individuals participated in Exam 3. The response rate was 76% in both sexes. The non-responder group and the responder group differed for mean age at Exam 1 (51.8 and 48.3 years, respectively) and at Exam 2 (58.4 and 54.4 years, respectively) but were similar for education (6.6 and 6.7 years of education, respectively). Findings about age and education were similar in separate analyses for men and women (not shown). Distribution of data about occupation reported at Exam 2 was similar between non-responders and responders, the most prevalent occupation being homemaker among women of both groups and white-collar worker among men of both groups.
Figure 3.
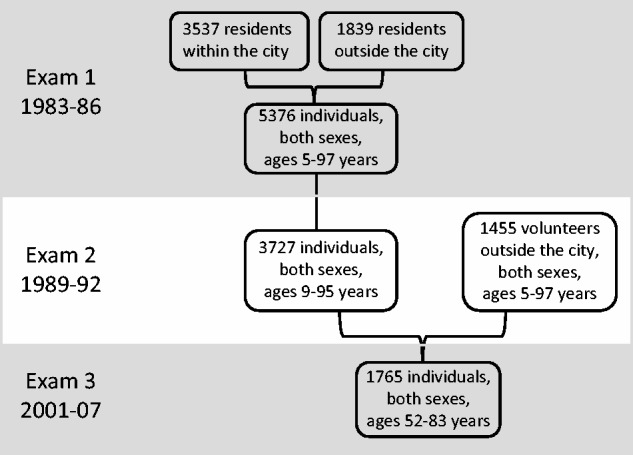
Diagram of design of and participants in the Gubbio Study
The feasibility of a fourth exam is currently under evaluation.
What has been measured?
The Gubbio Study adheres to the principles of the Declaration of Helsinki and Title 45 of the US Code of Federal Regulation. The study included the approval of the local authorities and informed consent from participants. Table 2 summarizes the list of variables measured in the three exams. The protocol of the exams is summarized below.
Table 2.
Summary of variables measured in each of the Study Exams
| Variable | Exam number |
||
|---|---|---|---|
| 1 | 2 | 3 | |
| Gender/age | Yes | Yes | Yes |
| Anthropometry | |||
| Weight/height | Yes | Yes | Yes |
| Waist/hip/plicometry | No | Yes | Yes |
| Education/occupation | Yes | Yes | Yes |
| Physical activity | No | Yes | Yes |
| Smoking habits | |||
| Smoker/ex-smoker | Yes | Yes | Yes |
| Reported number of cigarettes | Yes | Yes | Yes |
| Carbon monoxide in breath | Yes | No | No |
| Reported intake of | |||
| Alcohol | Yes | Yes | Yes |
| Caffeine-containing beverages | No | Yes | No |
| Milk/yogurt | No | Yes | No |
| Medical history | |||
| Personal history | Yes | Yes | Yes |
| Family history | Yes | Yes | Yes |
| Blood pressure/pulse rate | Yes | Yes | Yes |
| Electrocardiogram for persons aged ≥35 years | No | Yes | Yes |
| Echocardiogram for persons aged 45–54 years | No | Yes | No |
| 24-h ambulatory blood pressure for persons aged 45–54 years | No | Yes | No |
| Uroflowmetry for men aged ≥45 years | No | Yes | Yes |
| Duration of fasting before blood sampling | >2 hour | Overnight | Overnight |
| Blood biochemistry | |||
| Glucose, total cholesterol/HDL cholesterol | Yes | Yes | Yes |
| Triglycerides | No | Yes | Yes |
| Creatinine, uric acid | Yes | Yes | Yes |
| Blood count | Yes | Yes | Yes |
| Urea, sodium, potassium | Yes | Yes | No |
| Calcium, phosphorus, total protein | No | Yes | No |
| Alkaline phosphatase | No | Yes | No |
| Gamma-glutamyl-transferase | No | Yes | Yes |
| Biochemistry in first void urine | |||
| creatinine, sodium, and potassium | Yes | No | No |
| Biochemistry in overnight urine (fed conditions) | |||
| Creatinine, sodium, potassium, calcium, urea | No | Yes | No |
| Albuminuria for persons aged 45–64 years | No | Yes | No |
| Biochemistry in morning urine (fast conditions) | |||
| Creatinine, sodium, potassium, calcium, phosphorus, urate | No | Yes | No |
| Red blood cell electrolyte transport | Yes | Yes | No |
| Post-exam follow-up of events | |||
| Mortality data | Yes | Yes | No |
| Lethal/non-lethal cardiovascular disease for persons aged ≥35 years | Yes | Yes | No |
Exam 1 included the collection of an untimed spot sample of the first morning void urine for the assessment of dietary markers; the withdrawal of a venous blood sample after a fast of at least 2 h for routine biochemistry, blood count and special studies of electrolyte transport in red blood cells; and a brief medical visit for the administration of standardized questionnaires and for measurements of anthropometry, blood pressure and pulse. Participants were asked to refrain from eating or drinking for at least 2 h before the visit and from smoking or physical activity for at least one half-hour before the visit. Trained physicians measured blood pressure according to the WHO protocol with the use of mercury sphygmomanometers and cuffs of appropriate size. Blood pressure was measured on the right arm after participants had been seated quietly for 5 min. Three recordings were made, one minute apart.
Exam 2 included a timed overnight urine collection under fed conditions for assessment of creatinuria, dietary markers and albuminuria; the withdrawal of an early morning venous blood sample after an overnight fast for measurements of routine biochemistry, blood count and special studies of electrolyte transport in red blood cells; a morning urine collection under fasting conditions for assessment of renal tubular function; a brief medical visit for the administration of standardized questionnaires and measurements of anthropometry, blood pressure and pulse. Blood pressure and pulse were measured as in Exam 1. Additionally, for specific subgroups Exam 2 included also a 12-lead resting electrocardiogram, a standard echocardiogram, the recording of 24-h ambulatory blood pressure and standard uroflowmetry.
Exam 3 included the withdrawal of an early morning venous blood sample after an overnight fast for measurements of routine biochemistry and blood count; a brief medical visit for the administration of standardized questionnaires, measurements of anthropometry, blood pressure and pulse, a 12-lead resting electrocardiogram, and standard uroflowmetry in men. Measurements of anthropometry, blood pressure, pulse, and uroflowmetry were performed with the use of the same procedures for Exam 2.
Laboratory procedures for all exams were carried out based on standardized protocols which included pre-study training, pre-study testing and ongoing quality controls (both internal and external) on at least 10% of blind duplicate samples. Electrocardiograms of Exams 2 and 3 were analysed using the Minnesota Code. Echocardiograms of Exam 2 were performed and read by the same trained operator with assessment of intra-reader variability in 20% of randomized tracings.
Reported information about hospitalizations and data about lethal events from the national registry were continuously collected up to the time of Exam 3. An independent observer (A.M.) reviewed and coded data about the incidence of non-fatal cardiovascular disease and causes of deaths according to the International Classification of Diseases, Ninth Revision.
What has been found? Key findings and publications
Control of hypertension
With a cut-off of 140 mmHg for systolic pressure and 90 mmHg for diastolic pressure, data of Exam 2 indicated that the prevalence of controlled hypertension had doubled from 12% to 24% after 6-year follow-up in approximately 2600 men and women who were aged 30–79 years at Exam 1.5 Moreover, the average systolic and diastolic blood pressures declined from Exam 1 to Exam 2 by at least 2 mmHg, against an expected rise. These changes were associated with more common and more intensive anti-hypertensive drug treatment and with a decline in alcohol consumption.5 Additionally, data of Exam 3 indicated a further increase in hypertension control up to 40% and a decline by 50% in deaths due to cardiovascular disease.6 Altogether, the data suggest that the observational epidemiological study contributed to improve the control of hypertension and of its complications in the population of Gubbio.
Cellular electrolyte handling in hypertension
The Gubbio Study published several papers with the main focus on the role of the red blood cell sodium/lithium counter-transport (Na/Li-CT).7–15 Data of Exam 1 indicated that a higher activity of red blood cell Na/Li-CT was cross-sectionally associated with a higher prevalence of hypertension independently of several possible confounders. In particular, a difference of one SD in the Na/Li-CT activity—approximately 150 µmol/l of cells/h—was associated with a 40% difference in the prevalence of hypertension among men and women aged 25–74 years.7 Longitudinal data of Exam 2 indicated that the same difference was independently associated with accelerated blood pressure increase over time12 and with a 25% increased risk of incident hypertension among originally non-hypertensive men and women.13 Moreover, Na/Li-CT data consistently indicated that overweight and high alcohol intake were associated with higher baseline activity of Na/Li-CT9 and with its further increase over time.14 Altogether, the data represented the first population-based evidence that an alteration in cellular sodium handling could have a primary role in the pathogenesis of hypertension possibly through interactions with an unfavourable metabolic profile. The view that metabolic disorders might be important in these interactions was further supported by the evidence that one SD higher Na/Li-CT was associated with a 35% higher risk of incident diabetes also.15
Kidney dysfunction
The Gubbio Study was one of the first population-based surveys to report on urinary albumin excretion and on estimates of glomerular filtration rate (eGFR).16–21 Data of Exam 2 indicated that the prevalence of microalbuminuria—i.e. of a moderate elevation in urinary albumin ranging between 30 and 199 µg/min—is approximately 5% in middle-aged adults and is at least 10-fold higher than the prevalence of more severe elevation in urinary albumin defined as macroalbuminuria.16 In non-diabetic persons, male sex, blood pressure, plasma total cholesterol and cigarette smoking were directly associated with the prevalence of microalbuminuria independently of each other and of other confounders.16 Data of the study are the first evidence that systolic hypertension is cross-sectionally associated with a 5-fold increase in the prevalence of microalbuminuria even in the absence of diastolic hypertension.17 Further analyses indicated that microalbuminuria is cross-sectionally associated more strongly with coronary heart disease than with low values of eGFR.18–20 Finally, longitudinal data of the study indicated that the hazard ratio of non-lethal and lethal cardiovascular disease was approximately 50% higher in persons with microalbuminuria or with low values of eGFR, independently of each other and of the classical cardiovascular risk factors.21)
Other objectives
The other publications from the study cover a wide spectrum of objectives with inclusion of clinical, laboratory or dietary correlates of hypertension,22–27 various cardiovascular risk factors,28–35 urinary stone diseases,22,36,37 phosphorus homeostasis38,39 and interactions between environmental and genetic factors.40,41
What are the main strengths and weaknesses?
The age range of the population, the number of exams, the duration of follow-up, the spectrum of variables under study and the availability of pedigree data represent a quite unique combination. Figure 2 shows that the population of the study included not only adults but also children and individuals aged ≥75 years. Thus, the study allows us to investigate cross-sectionally and longitudinally differences associated with age from childhood to adulthood, from adulthood to older age and during ageing, a possibility which is uncommon among other epidemiological studies. The availability of data from three different exams over a period of more than 20 years allows us to focus selectively on middle-term and/or long-term analyses. The available variables are listed in Table 2 and allow a number of investigations. Finally, the availability of the pedigrees for approximately 1000 families with two generations and for 200 families with three generations affords the option of analyses on the familial aggregation of given traits, as done with focus on the role of pleiotropy in blood pressure and overweight40 and on the heritability of 20-year blood pressure changes in 338 nuclear pedigrees.41
The main weakness of the study is the fact that data of some variables were not collected in the whole target cohort but only in sex- and age-specific subgroups. Other weaknesses are the limited information about dietary factors and about codifications for non-cardiovascular events.
Can I get hold of the data? Where can I find out more?
The Gubbio Study shared data at the individual level and at the cohort level with other studies in Italy and abroad. Data are not open access but there are no strict limitations to data sharing. The steering committee of the study evaluates the proposals of data sharing on a case-by-case basis. There is no specific form for applications about data sharing. Please contact mlaurenzi@comcast.net for information and/or proposals.
Funding
Economic support to the study was given in the past by: Merck, Sharp & Dohme, Italy (MSD); the U.S. National Heart, Lung, and Blood Institute (Grant R01HL-40397-02); the Ministero Italiano di Università e Ricerca (Grant # 068034, PRIN 2004).
Acknowledgements
The study was made possible thanks to the enthusiasm of the people of Gubbio and to the continued support of its municipal and health authorities and community leaders. From 1982 to the present, the City of Gubbio have made available the following: the premises of the Centre of Preventive Medicine (i.e. the outpatient clinic where the exams took place and where the data were collected and recorded); the census lists that were used to define and to contact the initial target sample; and the registry of deaths with inclusion of the causes of death. Routine laboratory procedures and echocardiograms were performed in the Civil Hospital of Gubbio. Measurements of IDMS-traceable serum creatinine and urinary albumin were performed in the Second University of Naples, Italy (SUN). The codification of electrocardiograms was performed with collaboration between the Division of Cardiology of the Civil Hospital of Gubbio and CardioRicerca (CRR), Rome, Italy. The codification of incident cardiovascular events was performed by CRR. Special studies of red blood cell electrolyte transport were performed in the Federico II University, Naples, Italy (FUN).
The study activities have been guided by a steering committee whose members have been P. Angeletti (MSD), M.M., A.M., J. Stamler, R. Stamler (Northwestern University, Chicago) and A.Z.
Conflict of interest: None declared.
KEY MESSAGES.
During 20 years of follow-up, control of hypertension among participants in the Gubbio Study increased from 12% to 40%, a rate which was the highest in Italy and among the highest in the world.
One SD higher activity of red blood cell membrane sodium-lithium counter-transport is associated with 35% higher prevalence of hypertension and 25% higher incidence of hypertension.
The prevalence of moderate elevation in urinary albumin excretion defined as microalbuminuria is <2% in adults without hypertension, obesity, cigarette smoking or hypercholesterolaemia but increases up to 15% in adults with three or more of these risk factors.
Microalbuminuria and/or reduced glomerular filtration rate are associated with 50% higher risk of incident cardiovascular disease independently of hypertension, obesity, cigarette smoking, hypercholesterolaemia and diabetes.
References
- 1.Mariotti S, Capocaccia R, Farchi G, Menotti A, Verdecchia A, Keys A. Differences in the incidence rate of coronary heart disease between north and south European cohorts of the Seven Countries Study as partially explained by risk factors. Eur Heart J. 1982;3:481–87. doi: 10.1093/oxfordjournals.eurheartj.a061335. [DOI] [PubMed] [Google Scholar]
- 2.Keys A, Menotti A, Aravanis C, et al. The seven countries study: 2,289 deaths in 15 years. Prev Med. 1984;13:141–54. doi: 10.1016/0091-7435(84)90047-1. [DOI] [PubMed] [Google Scholar]
- 3.Sarnak MJ, Levey AS, Schoolwerth AC, et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation. 2003;108:2154–69. doi: 10.1161/01.CIR.0000095676.90936.80. [DOI] [PubMed] [Google Scholar]
- 4.Laurenzi M, Cirillo M, Angeletti M, et al. Gubbio Population Study: baseline findings. Nutr Metab Cardiovasc Dis. 1991;1:S1–S18. [Google Scholar]
- 5.Menotti A, Lanti M, Zanchetti A, et al. Impact of the Gubbio population study on community control of blood pressure and hypertension. J Hypertens. 2001;19:843–50. doi: 10.1097/00004872-200105000-00002. [DOI] [PubMed] [Google Scholar]
- 6.Menotti A, Lanti M, Angeletti M, et al. Twenty-year cardiovascular and all-cause mortality trends and changes in cardiovascular risk factors in Gubbio, Italy: the role of blood pressure changes. J Hypertens. 2009;27:266–74. doi: 10.1097/HJH.0b013e32831cbb0b. [DOI] [PubMed] [Google Scholar]
- 7.Laurenzi M, Trevisan M. Sodium-lithium countertransport and blood pressure: the Gubbio Population Study. Hypertension. 1989;13:408–15. doi: 10.1161/01.hyp.13.5.408. [DOI] [PubMed] [Google Scholar]
- 8.Cirillo M, Trevisan M, Laurenzi M. Calcium binding capacity of erythrocyte membrane in human hypertension. Hypertension. 1989;14:152–55. doi: 10.1161/01.hyp.14.2.152. [DOI] [PubMed] [Google Scholar]
- 9.Trevisan M, Laurenzi M. Correlates of sodium-lithium countertransport. Findings from the Gubbio Epidemiological Study. Circulation. 1991;84:2011–19. doi: 10.1161/01.cir.84.5.2011. [DOI] [PubMed] [Google Scholar]
- 10.Laurenzi M, Cirillo M, Trevisan M. The Gubbio data epidemiology and pathophysiology. Clin Exp Hypertens. 1992;14:261–69. doi: 10.3109/10641969209036187. [DOI] [PubMed] [Google Scholar]
- 11.Trevisan M, Krogh V, Cirillo M, Laurenzi M, Dyer A, Stamler J. Red blood cell sodium and potassium concentration and blood pressure. Ann Epidemiol. 1995;5:44–51. doi: 10.1016/1047-2797(94)00040-z. [DOI] [PubMed] [Google Scholar]
- 12.Cirillo M, Laurenzi M, Panarelli W, et al. Sodium-lithium countertransport and blood pressure change over time: the Gubbio Study. Hypertension. 1996;27:1305–11. doi: 10.1161/01.hyp.27.6.1305. [DOI] [PubMed] [Google Scholar]
- 13.Laurenzi M, Cirillo M, Panarelli W, et al. Baseline sodium-lithium countertransport and 6-year incidence of hypertension. Circulation. 1997;97:581–87. doi: 10.1161/01.cir.95.3.581. [DOI] [PubMed] [Google Scholar]
- 14.Cirillo M, Laurenzi M, Panarelli W, Trevisan M, Stamler J. Prospective analysis of traits related to 6-year change in sodium-lithium countertransport. Hypertension. 1999;33:887–93. doi: 10.1161/01.hyp.33.3.887. [DOI] [PubMed] [Google Scholar]
- 15.Vaccaro O, Cuomo V, Trevisan M, et al. Enhanced Na–Li countertransport: a marker of inherited susceptibility to type 2 diabetes. Int J Epidemiol. 2007;34:1123–28. doi: 10.1093/ije/dyi160. [DOI] [PubMed] [Google Scholar]
- 16.Cirillo M, Senigalliesi L, Laurenzi M, et al. Microalbuminuria in nondiabetic adults: relation of blood pressure, body mass index, plasma cholesterol levels, and smoking: the Gubbio Population Study. Arch Intern Med. 1998;158:1933–39. doi: 10.1001/archinte.158.17.1933. [DOI] [PubMed] [Google Scholar]
- 17.Cirillo M, Stellato D, Laurenzi M, Panarelli W, Zanchetti A, De Santo NG. Pulse pressure and isolated systolic hypertension: association with microalbuminuria. Kidney Int. 2000;58:1211–18. doi: 10.1046/j.1523-1755.2000.00276.x. [DOI] [PubMed] [Google Scholar]
- 18.Cirillo M, Laurenzi M, Panarelli P, Mancini M, Zanchetti A, De Santo NG. Relation of urinary albumin excretion to coronary heart disease and low renal function: role of blood pressure. Kidney Int. 2004;65:2290–97. doi: 10.1111/j.1523-1755.2004.00652.x. [DOI] [PubMed] [Google Scholar]
- 19.Cirillo M, Laurenzi M, Mancini M, Zanchetti A, De Santo NG. Low muscular mass and overestimation of microalbuminuria by urinary albumin/creatinine ratio. Hypertension. 2006;47:56–61. doi: 10.1161/01.HYP.0000197953.91461.95. [DOI] [PubMed] [Google Scholar]
- 20.Cirillo M, Laurenzi M, Mancini M, Zanchetti A, Lombardi C, De Santo NG. Low glomerular filtration in the population: prevalence, associated disorders, and awareness. Kidney Int. 2006;70:800–06. doi: 10.1038/sj.ki.5001641. [DOI] [PubMed] [Google Scholar]
- 21.Cirillo M, Lanti M, Menotti A, et al. Definition of kidney dysfunction as a cardiovascular risk factor: use of urinary albumin excretion and estimated glomerular filtration. Arch Inter Med. 2008;168:617–24. doi: 10.1001/archinte.168.6.617. [DOI] [PubMed] [Google Scholar]
- 22.Cirillo M, Laurenzi M. Elevated blood pressure and positive history of kidney stones: results from a population-based study. J Hypertens. 1988;6(Suppl 4):S485–86. doi: 10.1097/00004872-198812040-00153. [DOI] [PubMed] [Google Scholar]
- 23.Cirillo M, Laurenzi M. Erythrocyte and platelet volume in human hypertension. J Hypertens. 1989;7(Suppl):S168–69. doi: 10.1097/00004872-198900076-00080. [DOI] [PubMed] [Google Scholar]
- 24.Cirillo M, Laurenzi M, Stamler J. Factors related to blood pressure in a sample of Italian children age 5 to 14. Semin Nephrol. 1989;9:267–71. [PubMed] [Google Scholar]
- 25.Cirillo M, Laurenzi M, Trevisan M, Stamler J. Hematocrit, blood pressure, and hypertension. The Gubbio Population Study. Hypertension. 1992;20:319–26. doi: 10.1161/01.hyp.20.3.319. [DOI] [PubMed] [Google Scholar]
- 26.Cirillo M, Lombardi C, Laurenzi M, De Santo NG. Relation of urinary urea to blood pressure: interaction with urinary sodium. J Hum Hypertens. 2002;16:205–12. doi: 10.1038/sj.jhh.1001323. [DOI] [PubMed] [Google Scholar]
- 27.Ferrara LA, Vaccaro O, Cardoni O, Mancini M, Zanchetti A. Arterial hypertension increases left ventricular mass: role of tight blood pressure control. J Hum Hypertens. 2004;18:637–42. doi: 10.1038/sj.jhh.1001698. [DOI] [PubMed] [Google Scholar]
- 28.Laurenzi M, Stamler R, Trevisan M, Dyer A, Stamler J. Is Italy losing the “Mediterranean advantage"? Report on the Gubbio population study: cardiovascular risk factors at baseline. Prev Med. 1989;18:35–44. doi: 10.1016/0091-7435(89)90052-2. [DOI] [PubMed] [Google Scholar]
- 29.Laurenzi M, Mancini M, Menotti A, et al. Multiple risk factors in hypertension: results from the Gubbio study. J Hypertens. 1990;8(Suppl):S7–12. doi: 10.1097/00004872-199003001-00003. [DOI] [PubMed] [Google Scholar]
- 30.Menotti A, Lanti M, Puddu PE, et al. First risk functions for prediction of coronary and cardiovascular disease incidence in the Gubbio Population Study. Ital Heart J. 2000;1:394–99. [PubMed] [Google Scholar]
- 31.Puddu PE, Lanti M, Menotti A, et al. Serum uric acid for short-term prediction of cardiovascular disease incidence in the Gubbio Population Study. Acta Cardiol. 2001;56:243–51. doi: 10.2143/AC.56.4.2005651. [DOI] [PubMed] [Google Scholar]
- 32.Puddu PE, Lanti M, Menotti A, et al. Red blood cell count in short-term prediction of cardiovascular disease incidence in the Gubbio population study. Acta Cardiologica. 2002;57:177–85. doi: 10.2143/AC.57.3.2005387. [DOI] [PubMed] [Google Scholar]
- 33.Menotti A, Lanti M, Zanchetti A, et al. The role of HDL cholesterol in metabolic syndrome predicting cardiovascular events. The Gubbio population study. Nutr Metab Cardiovasc Dis. 2011;21:315–22. doi: 10.1016/j.numecd.2009.11.001. [DOI] [PubMed] [Google Scholar]
- 34.Ferrara LA, Vaccaro O, Cardoni O, Laurenzi M, Mancini M, Zanchetti A. Indexation criteria of ventricular mass and predictive role of blood pressure and body composition. Am J Hypertens. 2005;18:1282–87. doi: 10.1016/j.amjhyper.2005.05.020. [DOI] [PubMed] [Google Scholar]
- 35.Ferrara LA, Cardoni O, Mancini M, Zanchetti A. Metabolic syndrome and left ventricular hypertrophy in a general population. Results from the Gubbio Study. J Hum Hypertens. 2007;21:795–801. doi: 10.1038/sj.jhh.1002232. [DOI] [PubMed] [Google Scholar]
- 36.Cirillo M, Laurenzi M, Panarelli W, Stamler J. Urinary sodium to potassium ratio and urinary stone disease. Kidney Int. 1994;46:1133–39. doi: 10.1038/ki.1994.376. [DOI] [PubMed] [Google Scholar]
- 37.Cirillo M, Stellato D, Panarelli P, Laurenzi M, De Santo NG. Cross-sectional and prospective data on urinary calcium and urinary stone disease. Kidney Int. 2003;63:2200–06. doi: 10.1046/j.1523-1755.2003.t01-2-00003.x. [DOI] [PubMed] [Google Scholar]
- 38.Cirillo M, Ciacci C, De Santo NG. Age, renal tubular phosphate resorption, and serum phosphate levels in adults. N Engl J Med. 2008;359:864–66. doi: 10.1056/NEJMc0800696. [DOI] [PubMed] [Google Scholar]
- 39.Cirillo M, Botta G, Chiricone D, De Santo NG. Glomerular filtration rate and serum phosphate: an inverse relation diluted by age. Nephrol Dial Transplant. 2009;24:2123–31. doi: 10.1093/ndt/gfp040. [DOI] [PubMed] [Google Scholar]
- 40.Schork NJ, Weder AB, Trevisan M, Laurenzi M. The contribution of pleiotropy to blood pressure and body-mass index variation: the Gubbio Study. Am J Hum Genet. 1994;54:361–73. [PMC free article] [PubMed] [Google Scholar]
- 41.Monti M, Bonati MT, Crocamo C, et al. Heritability of blood pressure at baseline and change over time in pedigrees from the Gubbio population study. 22nd European Meeting on Hypertension and Cardiovascular Protection. J Hypertens. 2012;30(e-Suppl A) Abstract e297 (PP.LB01.436). Available from: http://journals.lww.com/jhypertension/Documents/ESH_2012.pdf (14 January 2013, date last accessed) [Google Scholar]