

In US Infant Mortality and the President’s Party,1 we analysed US infant mortality data from 1965 through 2010, and found that once one ‘filters’ out a smooth trend from the series, a persistent pattern emerges, with infant mortality rates being above trend during Republican Administrations and below trend during Democratic ones. As we noted in the article and detailed in its online appendix, this pattern is robust to whether we ‘filtered’ the trend using cubic splines, linear polynomials or fractional polynomials. The deviations from trend are visually evident and are easily detectable in the second stage regressions we estimated. Any claims about causality would be substantially stronger were we to understand mechanisms; yet, we believe the pattern we have uncovered merits reporting because it is striking and robust.
As our commentators also highlight, the identification of causal mechanisms in this research agenda is in its infancy, and so remains even in longstanding research endeavours across disciplines, not only epidemiology. Yet, there is a big difference between arguing that a causal mechanism between two variables ‘does not exist’ and acknowledging we ‘do not know’ if a causal mechanism exists or what it might be. The first statement leads to scientific paralysis; the second one is the engine of scientific endeavour.
Dorling and Catalano have very different reactions to our paper. In his commentary, Dorling2 accepts our central finding and invites readers to situate it among other related findings in the literature and join him in considering its range of possible implications. Catalano3 likens our article to bad dog food that should be recalled from supermarket shelves, pretty unappetizing stuff.
Putting aside Catalano’s ad hominem attacks, we welcome the opportunity to address his substantive points and, then, to discuss his scepticism about the enterprise of political epidemiology itself.
Catalano raises questions about the measure of infant mortality rate we use and, most importantly, disagrees with our choice of statistical procedure to ‘filter’ the data. Regarding the former, the ‘period’ measure we use is standard in the literature; it comes from the National Center for Health Statistics and divides infant deaths in each calendar year by live births in the same year, both values derived from vital statistics data. Conceptually, one might prefer true ‘birth cohort’ measures—where one would measure all infant deaths occurring among a calendar year’s births, including those that spill over into the next calendar year. However, given that the vast majority of US infant mortality occurs within the first month after birth—much during the first week—the magnitude of any misalignment is likely to be small. Importantly, we see no particular reason why the magnitude of the misalignment would be correlated with the president’s party. We experimented with approaches meant to approximate actual birth cohort infant mortality, including using data from the site Catalano used—the Human Mortality Database—and found the correlations between the period series we used in our paper and alternative series were very high (above 0.999).
On statistical approach, we disagree with Catalano’s indictment of our methods. We wonder whether he misunderstands our cubic spline procedure to de-trend the infant mortality series or the rationale for using it. Cubic splines represent linear combinations of cubic functions linked at ‘knots’. The cubic functions are constrained in such a way that the resulting curve and its first and second derivatives are continuous at the knots. As a result, as can be seen in Figure 1 in our paper, cubic splines do not have hinges (discontinuous first derivatives) at the knots.
Figure 1.
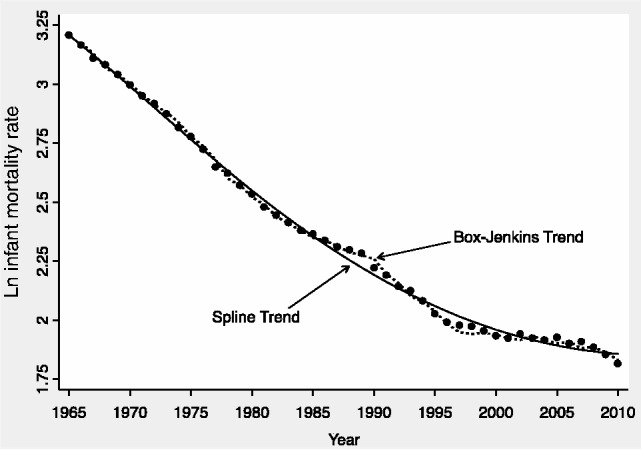
Box-Jenkins and cubic spline trends of logged US infant mortality. Dots • represent the natural log (Ln) of actual infant mortality rates; the dotted line represents a trend line derived from an estimated ARIMA (2/1/2) process; the solid line represents a trend derived from estimating a cubic spline with four equidistant knots
There are alternative procedures one might use for de-trending. One common approach is to fit third-, fourth-, fifth- or higher-order linear polynomials. These polynomials use integer power transformations of time as covariates. This method is just a special case of fractional polynomial regression, which offers more flexibility than do linear polynomials. Cubic splines represent an alternative, semi-parametric means for removing non-linear trends in time series data. As we report in the online appendix, regardless of whether we use linear polynomials, fractional polynomials or cubic splines to de-trend the infant mortality series, we obtain very similar results.
Catalano suggests Box-Jenkins methods as the best approach to filtering. These methods would fit an autoregressive integrated moving average (ARIMA) process to the infant mortality series. For many purposes, Box-Jenkins filters would be entirely appropriate; however, we do not believe this is true in the current case. As one can see very clearly from the Fourier series decompositions presented in the online appendix, time series variation in infant mortality is dominated by low-frequency variation (the non-linear time trend). There is also medium frequency variation (periods of roughly 16 years). Without overfitting the series, de-trending using either polynomials or cubic splines removes low-frequency variation (trends) from the data, but leaves the medium-frequency variation. Box-Jenkins methodology removes both the low- and medium-frequency variation. We make this point graphically in Figure 1, where we compare trends obtained using cubic splines with those obtained using best fitting ARIMA models.
We believe that illuminating the medium-frequency variation is important toward understanding sources of excess US infant mortality. Over the past half-century, the party of the president has turned over roughly every 8 years. The figure shows that there is middle-frequency variation in the infant mortality series that mirrors the political party affiliation of the president. Thus, using Box-Jenkins methods one could not distinguish between a slow-moving autonomous ARIMA process with a 16-year period that coincided with the presidential party shifts, and an actual presidential party effect.
One of the unique features of our analysis is that it was entirely within country, over time. In his earlier methodological writing4 and in his commentary, Catalano advocates using comparison populations. But as he observes, each approach has attendant strengths and weaknesses and he suggests a combination approach. In his commentary, Catalano mentions that he conducted an analysis comparing Canada with the USA.
Although he does not present his results in detail, he interprets them as at odds with our findings. We applied his approach ourselves. Similar to what Catalano did, in our first step we regressed the natural log of US infant mortality rates, 1965–2010, on the same-year natural log of infant mortality rates in Canada. We de-trended the residuals from this regression using a cubic spline, and after recovering the residuals from the cubic spline, we regressed them on the presidential party indicator. Using this comparative approach, the estimated coefficient on the Republican Party indicator was 0.028 [95% confidence interval (CI) ± 0.018], a precise estimate very similar to the estimates we report in our paper. Because we used a cubic spline rather than the Box-Jenkins methods he uses to filter out any residual trend, finding such a high similarity in our results confirms that any discrepancies between our results and Catalano’s would be due to differences in the filtering procedures, not from using a comparative vs single-country approach.
Catalano’s methodological critique is part of his meta-argument where he disparages our use of the term ‘political epidemiology’ and suggests we invoked it to cloak our, in his view partisan and poorly designed, work in some positive aura associated with the field of epidemiology. We used this terminology because we thought it appropriate to situate our work within the context of a growing body of research—much of it published in this journal—that examines the association between political factors and health outcomes.
Is political epidemiology a worthy scientific enterprise or is it a misuse of statistics to score political points?
To the extent that human-made public, social and health policies and programmes are powerful determinants of health, epidemiology is a social, and inherently political, science. The emerging research agenda in ‘political epidemiology’ has noted numerous, credible causal venues linking politics to epidemiological outcomes, even beyond the realm of policy.6–8 The scientific acknowledgement of such plausible mechanisms is not the product of ‘political imagination’. At a minimum, dismissing it as such, naively discounts the huge powers of government to affect the distribution of the social, physical environmental, and life-course determinants of health that ultimately affect the social distribution of infant mortality, among many other health outcomes as Dorling reminds us.
The USA has an increasingly polarized yet very stable two-party system. Today, this two-party system is clearly defined by between-party heterogeneity and within-party homogeneity, an elite-level political sorting that did not happen independently of the racial agenda encrypted in the Southern Strategy employed by Republicans to win votes of disaffected Democrats subsequent to the Civil Rights Movement—a process termed by academics as the US ‘political realignment’. Political candidates running for office and the parties that support them ask for votes based on implicit and explicit claims that their general approach and specific policies will benefit the population’s well-being, whereas that of the candidate of the opposition party will be harmful. In such a polarized climate, Americans are primed to interpret election outcomes as either validating or delegitimizing, a psychosocial response that itself may have health effects, as Dorling also suggests. For both reasons, it would thus be surprising if electoral outcomes were without social, including health, consequences. And it would be scientifically negligent to consider their study off-limits and not empirically describe what they are.
The US political polarization, itself, suggests it may not be unusual to find the empirical evidence being more consistent with one party’s claims than the other party’s. We cannot infer that such findings automatically reveal the investigator’s partisan bias. If we did, where would the cynicism end? Wouldn’t such standards require that we also write off as partisan any opposing commentary? Instead, we hope that the way we have presented the data on infant mortality rates is sufficiently transparent for readers to understand the nature of the inferences we drew and to evaluate our claims on their merits.
As social scientists hoping to contribute to moving beyond the impasse to understanding entrenched social and racial disparities in infant mortality or other poor health outcomes, we think that empirically analysing whether political variables have health impacts is well within the purview of epidemiologists. Robust descriptive findings such as those we report are a first step. Empirically elaborating whether associations found have causal content and the related mechanisms is another step that we are beginning to take. Through reporting our striking and consistent findings, we hope other epidemiologists and social scientists will engage in such research, too.
Funding
This research was supported in part by the Eunice Kennedy Shriver National Institute of Child Health and Human Development [Grant # T32 HD007339] and also by a grant from the Russell Sage Foundation.
References
- 1.Rodriguez JM, Bound J, Geronimus AT. US infant mortality and the president's party. Int J Epidemiol 2014;43:818–26 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dorling D. All the president's children. Int J Epidemiol 2014;43:827–29 [DOI] [PubMed] [Google Scholar]
- 3.Catalano R. Political epidemiology, Republican presidents and dog food. Int J Epidemiol 2014;43:829–31 [DOI] [PubMed] [Google Scholar]
- 4.Catalano R, Ahern J, Bruckner T. Estimating the health effects of macrosocial shocks: a collaborative approach. In: Macrosocial Determinants of Population Health. New York: Springer, 2007 [Google Scholar]
- 5.Vogelsang TJ. Heteroskedasticity, autocorrelation, and spatial correlation robust inference in linear panel models with fixed-effects. J Econometrics 2012;166:303–19 [Google Scholar]
- 6.Bambra C, Fox D, Scott-Samuel A. Towards a politics of health. Health Promot Int 2005;20: 187–93 [DOI] [PubMed] [Google Scholar]
- 7.Beckfield J, Krieger N. Epi+ demos+ cracy: linking political systems and priorities to the magnitude of health inequities—evidence, gaps, and a research agenda. Epidemiol Rev 2009;31: 152–77 [DOI] [PubMed] [Google Scholar]
- 8.Muntaner C, Borrell C, Ng E, et al. Locating politics in social epidemiology. In: Rethinking Social Epidemiology. New York: Springer, 2012 [Google Scholar]