

Abstract
Background
Pain can significantly influence an individual's health status and can have serious negative consequences: poor nutrition, decreased appetite, abnormal sleep patterns, fatigue, and impairment of daily living activities. Pain can cause psychological impairment and decrease healing and recovery from injuries and illness. A hallmark of many chronic conditions, pain affects more patients' lives than diabetes mellitus, heart disease, and cancer combined. However, many chronic sufferers do not have access to effective pain management for a variety of reasons, including limited access, restrictions, and personal and cultural biases.
Methods
This review summarizes issues of access, distribution, and cultural bias with regard to opioid agents and seeks to clarify the challenges related to opioid delivery. The considerable negative physical and mental consequences of chronic pain are discussed for the general and palliative care population.
Results
Opioids are an effective treatment for various intractable painful conditions, but problems in global opioid access for safe and rational use in pain management contribute to unnecessary suffering. These problems persist despite increased understanding in recent years of the pathophysiology of pain.
Conclusions
Comprehensive guidelines for goal-directed and patient-friendly chronic opiate therapy will potentially enhance the outlook for future chronic pain management. The improvement of pain education in undergraduate and postgraduate training will benefit patients and clinicians. The promise of new medications, along with the utilization of multimodal approaches, has the potential to provide effective pain relief to future generations of sufferers.
Keywords: Analgesics–opioid, chronic pain, healthcare disparities, health services accessibility, human rights, medical indigency, pain management, palliative care
INTRODUCTION
Albert Schweitzer said, “We must all die. But that I can save him from days of torture, that is what I feel as my great and ever new privilege. Pain is a more terrible lord of mankind than even death itself.”1 The International Association for the Study of Pain defines pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.”2 Melzack describes prolonged pain as a condition that destroys one's quality of life and can erode one's will to live, even causing individuals to end their lives.3
Pain, often called the fifth vital sign, can significantly influence an individual's health status and can have serious negative consequences, including morbidity and mortality.2,4,5 Chronic and high-intensity persistent pain can lead to poor nutrition, decreased appetite, abnormal sleep patterns, fatigue, and impairment of daily living activities. Pain can cause psychological impairment and decrease healing and recovery from injuries and illness.3,6 A hallmark of many chronic conditions, pain affects more patients' lives than diabetes mellitus, heart disease, and cancer combined.5
Pain is one of the most common symptoms associated with cancer. Portenoy and Lesage assert that 30%-50% of patients receiving treatment for solid tumors experience pain, and 70%-90% of patients with advanced cancer disease experience pain.7 Eighty-eight percent of cancer patients in the last year of their life are reported to be in pain. Forty-seven percent of patients whose treatment for cancer pain is controlled by their primary physicians feel that their treatment only partially controls the pain. Certain types of cancer pain, including neuropathic and cancer-induced bone pain, can be particularly challenging to treat.6,8
According to Brennan et al, a large gap exists between the increasingly sophisticated understanding of the pathophysiology of pain and the widespread inadequacy of its treatments.4 Providing effective pain control is a challenge for a variety of reasons: accessibility and cost of opioids; barriers related to physician training and perceptions, healthcare system restrictions, and patient perceptions; and cultural bias.
GLOBAL OPIOID CONSUMPTION AND AVAILABILITY
The morphine consumption rate in most regions does not reflect actual morphine needs for pain management. According to World Health Organization (WHO) data from 2003, 6 developed countries accounted for 79% of global morphine consumption, while developing countries only accounted for 6% of global opioid consumption despite improved access to pain treatment over the past 2 decades.1,2,9,10 A 2010 report by the International Narcotics Control Board (INCB) confirmed similar global trends of opioid availability.11 Opioid consumption levels for pain treatment have risen in European countries, Canada, and the United States (US), especially for cancer pain. In contrast, consumption levels in Asian, African, and Middle Eastern countries have stagnated or decreased despite international efforts to change political views on opioid use for pain management.11,12-14 Western European and North American countries consume the majority of the morphine produced in the world even though the combined population of these areas is less than one-fifth (17.2%) of the world's population (Table and Figure 1).15 However, even in the world's 6 richest countries, only 24% of patients' pain needs are adequately managed.15
Table.
Regional Per Capita Use of Morphine in 2005
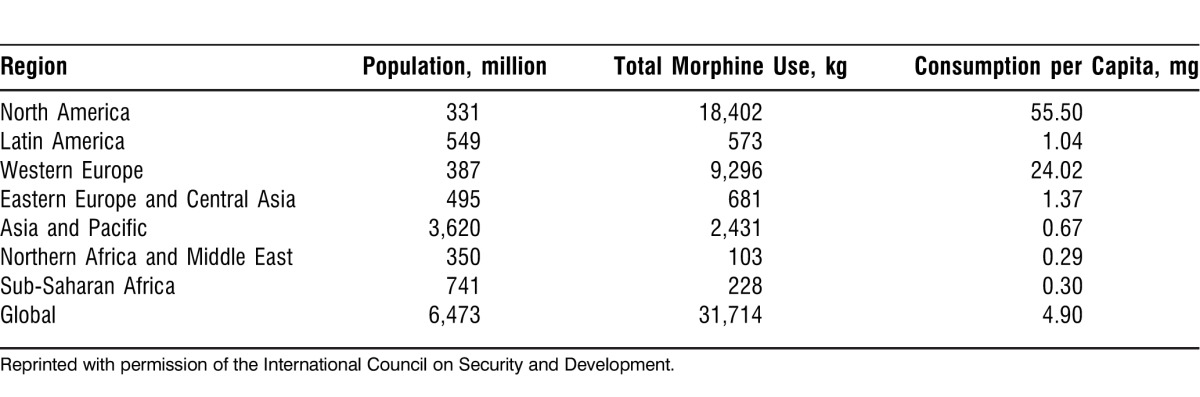
Figure 1.
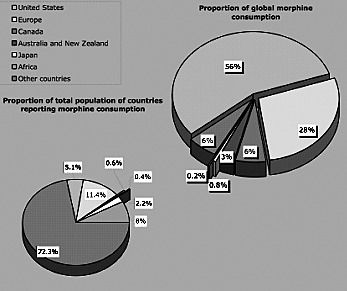
Worldwide distribution of morphine consumption in 2009. (Source: International Narcotics Control Board.7)
Opioid abuse affects availability. The United Nations Office on Drugs and Crime (UNODC) reported that an estimated 12-14 million heroin users consumed approximately 375 metric tons of heroin in 2009,16 yet 5.5 billion people (83% of the world's population) had no access to opioid treatment for pain, based on their Adequacy of Consumption Measure.17
In 2006, Afghanistan produced more than 6,100 metric tons of opium, yet that quantity was insufficient to meet the world's actual morphine needs, estimated to be approximately 6,152 metric tons.11,18 Also, a survey by UNODC showed a 36% decrease in the production of opium, from 5,800 tons in 2011 to 3,700 tons in 2012, resulting in higher opium pricing.19 Although the cost of opioid analgesics appears relatively low, studies have reported that opioid analgesic retail prices are much higher in developing countries than developed countries, making opioid-based analgesics unaffordable to patients who are in poverty.20 Solving these problems depends on international communities achieving a balance between ensuring availability of opioids for medical and scientific purposes and preventing their diversion for abuse, a well-known and significant problem. Therefore, the need for effective working partnerships and international collaborations is urgent to minimize suffering from unnecessary pain.12,13
PHYSICIAN, PATIENT, AND HEALTHCARE SYSTEM BARRIERS
The personal perceptions of physicians and patients, as well as restrictions within healthcare systems, contribute to the unnecessary suffering that results from nonexistent or inadequate pain management services.19,20
Physician Training and Perceptions
Physicians may have personal biases regarding gender, race, and ethnicity that affect their attitudes toward patients' pain. They may also lack adequate pain education and training, including pain assessment skills.
Patient Perceptions
Patients may fear that the presence of pain indicates a serious illness and interpret a prescription for opioids as a sign of impending death, or they may believe that the use of pain medication will lead to addiction and uncomfortable side effects. Patients may be unable to adequately articulate their level of pain to a physician.
Healthcare System Restrictions
The healthcare system may struggle with insufficient funds, leading to inadequate treatment for low-income patients, decreased access to specialized pain care, and an increase in outpatient care that may not be optimal for pain management. Poor reimbursement policies, multiple pain assessment tools with inconsistent results, and strict legal requirements for pain physicians and clinics are other healthcare system–related factors that lead to inadequate treatment of pain.
IMPACTS OF CULTURAL BIASES ON EFFECTIVE PAIN MANAGEMENT
United Kingdom
Approximately 320,500 people were diagnosed with cancer in the United Kingdom (UK) in 2009, equating to an incidence of approximately 519 per 100,000.21 Figure 2 shows the rate of diagnosed cases of cancer in the UK by sex for the years 2007-2009. According to the Office for National Statistics, in 2012 the mortality rate for females with cancer was 151 per 100,000, and the mortality rate for males with cancer was 209 per 100,000, with 74,000 female deaths and 81,600 male deaths from cancer.22
Figure 2.
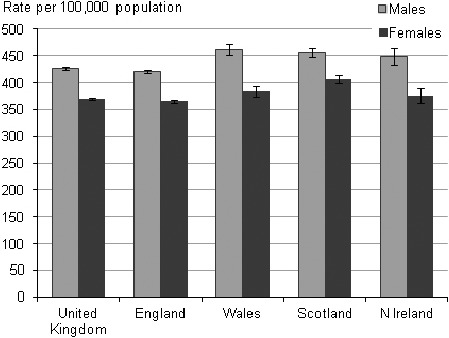
Diagnosed cases of cancer by sex in the United Kingdom, 2007-2009. (Source: UK Office for National Statistics.21)
Reports suggest that underutilization of a multidisciplinary care approach between palliative care and pain medicine may contribute to inadequate pain management among patients in the UK.23-25 Recent surveys show that more than 30% of patients, representing approximately 46,020 individuals, receive poor pain control during their illness, and 10% of those fail to receive effective pain relief recommended by WHO.23 The British Pain Society (BPS) published a 2010 guide on cancer pain management for health professionals with emphasis on the importance of a multimodal approach. The WHO 3-step analgesic ladder model has provided a cost-effective pain treatment approach for many cancer sufferers; however, different models of analgesia treatment must be developed to address the increasing complexity of cancer and its treatments.26 Additionally, in the 3-step analgesic ladder, the use of morphine for cancer pain management has not been the gold standard approach although opioids continue to be the mainstay of pain treatment, morphine is relatively cheap, and morphine is the most widely available opioid analgesic.14,27
Opioid use for chronic noncancer pain remains controversial; the safety and efficacy of long-term opioid use is described as uncertain.28 Persistent or chronic pain affects more than 5 million patients in the UK.28 Opioid use is effective for treating a number of pain states for noncancer conditions but can cause serious problems with long-term use, including tolerance, dependence, and the potential for addiction.28 Recent studies show that patients with a current or past history of substance misuse or with a diagnosis of psychiatric illness are more likely to develop problems with opioid use.11,25,29
United States
The American Cancer Society estimated that 1,638,910 new cancer cases would be diagnosed in the US in 2012.30 The number of individuals older than 85 years is predicted to reach 10 million by year 2030, with an associated dramatic increase in the number of cancer cases.31,32 To maintain these patients' quality of life, expert and advanced pain management care is needed, and various disciplines within the healthcare system are emerging to improve pain management and expand palliative care to more patients.33 Palliative care medicine is an evolving field in which new treatment modalities are continuously under development and existing modalities are increasingly applied to ease the suffering of patients. In a review of current pain management in US palliative care, Green et al found that disparities existed among different racial and ethnic groups with regard to pain perception, assessment, and treatment.30 These disparities were present in various clinical settings, including the emergency room and postoperative recovery, and in various types of pain, including acute, cancer, chronic nonmalignant, and experimental pain.
The expansion and improvement of palliative care have been achieved by increasing education and research of cancer in several medical disciplines, changing institutional attitudes, and developing national guidelines for the improved assessment of cancer care at the national level.34 One important initiative was to establish palliative care programs across the US. Data from the 2008 American Hospital Association Annual Survey of US Hospitals showed that 1,299 hospitals (31%) have palliative care programs.34,35 Palliative support ranges from small consultation clinics to extensive multidisciplinary palliative care in large institutions. The level of palliative care support has increased in more than 632 hospitals since 2010 when these hospitals reported that they had palliative care programs. The intention of the initiative is to improve the quality of life for patients with cancer through effective pain control.36
Malaysia
Malaysia has a highly accessible public healthcare system, yet palliative medicine is still not an established discipline.37 Malaysian government surveys have reported that opioid consumption in Malaysia is dramatically lower than the global average, which may indicate inadequate pain provisions for patients who are terminally ill. Reports indicate that only 24% of patients who suffer from cancer pain receive regular opioid analgesia.38 The primary barriers to effective pain management in Malaysia stem from physicians' and patients' perceptions regarding the use of opioids. In one survey of physicians in Malaysia, 46% responded that they lacked medical knowledge to manage patients with severe cancer pain, and 64% were concerned about unwanted side effects to opioid use, such as respiratory depression and dependency. Fear of addiction is among patients' most common concerns, as there is some confusion regarding the legality of opioid use in Malaysia. Additional barriers include the lack of formal medical education in palliative care and the lack of adequate facilities in smaller clinics to prepare or stock cheap oral morphine.39 A number of initiatives aim to improve current misconceptions regarding opioid use by establishing palliative care wards in hospitals and implementing postgraduate training programs in palliative care. Recent campaigns to raise public awareness of opioid use for cancer pain have been carried out to support the provision of good palliative care.37,38
India
The annual occurrence of cancer in India is estimated to be about 90 cases per 100,000 people, but because cancer is not required to be reported, this figure could be an underestimate.38-40 Approximately 500,000 new cases of cancer are estimated to occur in India each year, with approximately 1.5 million persons diagnosed with cancer. In 2020, the annual incidence of cancer is projected to be 1,150,000 and the total number of cases is projected to be 6 million, based on 2010 rates.41,42
India accounted for the consumption of 103 kg of morphine in 1992, a decrease from 411 kg in 1984.43 The consumption of morphine for medicinal use in India in 1990 was 150 kg; this rate is comparable to the consumption rate for Denmark that has 895 million fewer inhabitants than India. Access to morphine for cancer pain in India appears to be limited, with most morphine given via the parenteral route.44
In recent years, cancer facilities such as cancer detection and prevention clinics and hospitals routinely have dispensed oral morphine for cancer pain management as a result of improved medical education. However, patients with cancer still receive inadequate opioid therapy for their pain. They are often too ill to travel to cancer facilities and possess limited financial capacity for opioid treatment.45,46
Latin America
Statistics by the Pain & Policy Studies Group at the University of Wisconsin and INCB show that Latin America accounts for less than 1% of the world's opioid consumption, indicating inadequate availability of opioid analgesics in that region.47 One reason for the limited availability is that many countries in Latin America have overly restrictive laws governing opioid use. For example, some national laws prohibit or restrict opioid use throughout the duration of therapy, limiting dosages and concentrations regardless of clinical conditions and medical needs. The cost of opioid therapy is also prohibitively expensive for the majority of the population. In Argentina and Mexico, the monthly cost of opioid therapy for cancer pain relief can be more than 200% of the average monthly income.48 Factors that contribute to the high price of opioids are the cost of import and licensing taxes, the cost of distribution, legal restrictions on the storage and sale of opioids, and decreased demand caused by those legal restrictions.12
Strategies for promoting opioid utilization for pain control have been ongoing since the WHO Palliative Care Program projects were implemented in Latin America.48 A set of widely used guidelines enabling health professionals and regulators to identify barriers to opioid use was initially distributed in various WHO-sponsored workshops. The Andean region (Bolivia, Chile, Colombia, Ecuador, Peru, and Venezuela) and Southern Cone countries (Argentina, Brazil, Paraguay, and Uruguay) have been involved in these projects. Positive outcomes have been seen in various countries, such as the creation of a national pain relief program in Colombia and a national palliative care program in Uruguay, as well as the newly founded Latin American Palliative Care Association that aims to improve pain control strategies.49
Africa
Approximately 826 million people in Africa are affected by the human immunodeficiency virus (HIV) and acquired immune deficiency syndrome (AIDS) pandemic, resulting in a high prevalence of HIV/AIDS and resultant mortality.50 WHO has promoted several initiatives and palliative care projects for patients with cancer and HIV/AIDS in Botswana, Ethiopia, Tanzania, Uganda, and Zimbabwe; however, the development of modern palliative care practices in Africa remains scattered and poor.51 From 2000 to 2002, 29 African countries, including Sudan, Chad, Mali, and Nigeria, reported no morphine utilization, and these countries had no known palliative care activity during this time period.52 Low levels of opioid utilization across the continent and limited statistical data for medical opioid use indicate that cultural and social barriers exist with regard to opioid use in pain relief.53
In 2010, global mean consumption of morphine in milligrams per capita was 5.99; the majority of African countries consumed less than 1 mg per capita with the exception of South Africa where the average morphine consumption was 10.93 mg per capita.52 In South Africa, palliative care services are firmly established in hospital settings.52,53
In recent years, WHO has drawn global attention to the urgent need for better pain management in patients with cancer and AIDS, explaining, “The majority of those suffering unrelieved pain are in low and middle income countries, where there is an increasing burden of chronic diseases, such as cancer and AIDS.”1,54
Some significant movements to improve morphine availability have been made in various African countries in recent years. For example, in Uganda, free morphine therapy for patients with cancer and HIV/AIDS has allowed healthcare professionals to prescribe morphine within their clinical practices.55 However, opioid distribution remains a challenge in many of the developing countries, such as Zimbabwe, because of barriers with regard to drug availability, policymaking, and education.
CHRONIC OPIOID THERAPY FOR NONCANCER PAIN
Much of the opioid use in developed countries is associated with chronic noncancer pain, with the risk of potential addiction and dependence. Evidence-based guidelines by BPS, the American Pain Society (APS), and WHO aim to develop a multidisciplinary approach to the use of chronic opioid therapy for adults with noncancer pain, with the goal of reducing a diversion to abuse.23,25,28
The key recommendations for initiating chronic opioid therapy include (1) an accurate physical assessment and examination, including a psychiatric history by clinicians; (2) a short trial of chronic opioid therapy as an option for patients with moderate or severe noncancer pain that has an adverse impact on function or quality of life; (3) stringent monitoring of patients with a history of drug abuse, psychiatric issues, and behavioral problems; (4) frequent evaluation of patients using chronic opioid therapy, with drug therapy discontinued when necessary; and (5) assistance for patients in meeting therapeutic goals and gradually decreasing dosage to manage intolerable adverse effects, such as aberrant drug-related behavior.
FUTURE DIRECTIONS
Drug Delivery
Advances in the delivery of medication have improved their pharmacokinetic profiles and minimized unwanted side effects. These advances have been particularly important in expanding the utility of existing medications to better serve a variety of patients. Extended-release formulations of medications, including opioid agents, allow for simpler dosing regimens, improved patient satisfaction, and improved patient compliance. In addition, they provide more stable blood concentrations of therapeutic agents and may avoid the peaks and troughs of immediate-release drugs, resulting in fewer adverse effects that occur at peak concentrations and fewer periods of inadequate treatment caused by low drug concentrations at trough points.
Parenteral Formulations
Transdermal and transmucosal delivery systems are attractive options for palliative care patients for whom enteral delivery may be limited by nausea, malabsorption, or dysphagia; these delivery systems are also a good option for drugs with poor oral bioavailability. Many opiate medications have poor oral bioavailability, and their utility has been greatly enhanced by the development of transmucosal preparations (eg, Actiq, Fentora) and transdermal formulations (eg, Duragesic). Transmucosal agents allow for rapid treatment of breakthrough pain, while Duragesic patches deliver a basal rate of fentanyl to treat chronic pain. Ionsys is an iontophoretic transdermal fentanyl delivery system under development that would allow patient-controlled analgesia (PCA) through the active delivery of transdermal fentanyl on patient demand with the added safety of timing lockouts.
New transmucosal formulations of the opioid sufentanil may be able to provide rapid and enduring pain control through a sublingual PCA system, known as Zalviso. Sufentanil is an analog of fentanyl that is approximately 10 times more potent than fentanyl and 1,000 times more potent than morphine; it provides superior analgesia with lower rates of respiratory depression than fentanyl or morphine after intravenous (IV) administration. However, sufentanil is extremely lipophilic, resulting in a short duration of action caused by rapid redistribution into lipid-rich tissues in the body.56,57 Zalviso delivers a 3 mm tablet on demand under the patient's tongue with programmed timing lockouts. The advantage of this technology is that it does not require the placement of an IV line or classic PCA equipment. Clinical data have been positive.58 In addition to opioids, transdermal delivery systems of nonsteroidal antiinflammatory drugs such as diclofenac and transdermal lidocaine (Lidoderm) are prescribed to treat localized pain and inflammation. Delivery systems such as the Flector Patch and Voltaren Gel allow targeted application of antiinflammatory agents with decreased systemic absorption, which may result in an improved safety profile and fewer side effects. In addition to these transdermal and sublingual delivery systems, intranasal delivery systems of morphine (Rylomine) and fentanyl are being investigated, as are intranasal, oral, and sublingual formulations of medications such as ketamine.59 The ever-expanding complement of new drug delivery systems promises to greatly improve the safety and utility of medications available for symptom management in palliative care.
CONCLUSION
The APS has called pain the fifth vital sign in an attempt to increase the awareness of pain among healthcare professionals. Untreated or undertreated pain significantly decreases a patient's quality of life by causing sleep disorders, depression, impaired activity, mood alterations, abnormal appetite, inability to focus, and poor hygiene. Opioids are a popular choice for the treatment of intractable painful conditions, but barriers to effective pain assessment and management exist in both developed and developing countries. Huge disparities exist in opiate production vs actual needs, as well as in the distribution of morphine in developed countries vs developing countries. Imbalances between opioid consumption and availability persist despite international efforts in recent years. Opioid distribution must be improved throughout the world.
Healthcare professionals and patients are often concerned about the side effects of opioid analgesics, particularly the potential for tolerance and addiction. Comprehensive guidelines for goal-directed and patient-friendly chronic opiate therapy potentially will enhance the outlook for future chronic pain management. The improvement of pain education in undergraduate and postgraduate training will benefit patients and clinicians. The promise of new medications, along with the utilization of multimodal approaches, has the potential to provide effective pain relief to future generations of sufferers.
Footnotes
The authors have no financial or proprietary interest in the subject matter of this article.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care, Medical Knowledge, and Practice-Based Learning and Improvement.
REFERENCES
- 1.International Association for the Study of Pain. Pain: Clinical updates. 2004 Sep;12(5):1–4. http://iasp.files.cms-plus.com/Content/ContentFolders/Publications2/PainClinicalUpdates/Archives/PCU04-5_1390264543538_30.pdf. Accessed March 19, 2014. [Google Scholar]
- 2.International Association for the Study of Pain. Classification of Chronic Pain. Washington, DC: International Association for the Study of Pain;; 2011. [Google Scholar]
- 3.Melzack R. The tragedy of needless pain. Sci Am. 1990 Feb;262(2):27–33. doi: 10.1038/scientificamerican0290-27. [DOI] [PubMed] [Google Scholar]
- 4.Brennan F, Carr DB, Cousins M. Pain management: a fundamental human right. Anesth Analg. 2007 Jul;105(1):205–221. doi: 10.1213/01.ane.0000268145.52345.55. [DOI] [PubMed] [Google Scholar]
- 5.Human Rights Watch. New York, NY: Human Rights Watch; 2009. Access to pain treatment as a human right. Executive summary. http://www.hrw.org/en/reports/2009/03/02/please-do-not-make-us-suffer-any-more-0. Accessed March 19, 2014. [Google Scholar]
- 6.Merskey H, Bogduk N. Classification of Chronic Pain. 2nd ed. Seattle, WA: International Association for the Study of Pain Press;; 1994. eds. [Google Scholar]
- 7.Portenoy RK, Lesage P. Management of cancer pain. Lancet. 1999 May 15;353(9165):1695–1700. doi: 10.1016/S0140-6736(99)01310-0. [DOI] [PubMed] [Google Scholar]
- 8.United Nations Office on Drugs and Crime. World Drug Report. Vienna, Austria: New York, NY: United Nations; 2007. http://www.unodc.org/pdf/research/wdr07/WDR_2007.pdf. Accessed March 19, 2014. [Google Scholar]
- 9.Milani B, Sholten W. The World Medicines Situation: Access to Controlled Medicines. 3rd ed. Geneva, Switzerland: World Health Organization;; 2011. [Google Scholar]
- 10.World Health Organization. World Health Organization; Jun, 2010. Medicine: access to controlled medicines (narcotic and psychotropic substances) http://www.who.int/mediacentre/factsheets/fs336/en/. Accessed March 19, 2014. [Google Scholar]
- 11.International Narcotics Control Board. Report of the International Narcotics Control Board on the Availability of Internationally Controlled Drugs: Ensuring Adequate Access for Medical and Scientific Purpose. New York, NY: International Narcotics Control Board;; 2011. [Google Scholar]
- 12.De Lima L. Opioid availability in Latin America as a global problem: a new strategy with regional and national effects. J Palliat Med. 2004 Feb;7(1):97–103. doi: 10.1089/109662104322737368. [DOI] [PubMed] [Google Scholar]
- 13.Silbermann M. Current trends in opioid consumption globally and in Middle Eastern countries. J Pediatr Hematol Oncol. 2011 Apr;33(Suppl 1):S1–S5. doi: 10.1097/MPH.0b013e3182121872. [DOI] [PubMed] [Google Scholar]
- 14.Pain & Policy Studies Group, World Health Organization Collaborating Center for Policy and Communications in Cancer Care, University of Wisconsin Comprehensive Cancer Center. Madison, WI: University of Wisconsin Pain & Policy Studies Group; 2002. Availability of Opioid Analgesics in Asia: Consumption Trends, Resources, Recommendations. http://s3.amazonaws.com/zanran_storage/www.painpolicy.wisc.edu/ContentPages/890535482.pdf. Accessed March 19, 2014. [Google Scholar]
- 15.International Narcotics Control Board. Report of the International Narcotics Control Board for 2007. New York, NY: United Nations;; 2008. [Google Scholar]
- 16.United Nations Office on Drugs and Crimes. World Drug Report. The Opium/Heroin Market. New York, NY: United Nations; 2011. http://www.unodc.org/documents/data-and-analysis/WDR2011/The_opium-heroin_market.pdf. Accessed March 19, 2014. [Google Scholar]
- 17.Seya MJ, Gelders SF, Achara OU, Milani B, Scholten WK. A first comparison between the consumption of and the need for opioid analgesics at country, regional, and global levels. J Pain Palliat Care Pharmacother. 2011;25(1):6–18. doi: 10.3109/15360288.2010.536307. [DOI] [PubMed] [Google Scholar]
- 18.United Nations Office on Drugs and Crime. Single Convention on Narcotic Drugs, 1961. As Amended by the 1971 Protocol Amending the Single Convention on Narcotic Drugs, 1961. New York, NY: United Nations; 1972. https://www.unodc.org/unodc/en/treaties/single-convention.html. Accessed March 19, 2014. [Google Scholar]
- 19.United Nations Office on Drugs and Crime. Afghanistan: Opium Survey 2012. New York, NY: United Nations;; 2012. [Google Scholar]
- 20.Taylor AL, Gostin LO, Pagonis KA. Ensuring effective pain treatment: a national and global perspective. JAMA. 2008 Jan 2;299(1):89–91. doi: 10.1001/jama.2007.25. [DOI] [PubMed] [Google Scholar]
- 21.Cherny NI, Catane R, Kosmidis PA. Problems of opioid availability and accessibility across Europe: ESMO tackles the regulatory causes of intolerable and needless suffering. Ann Oncol. 2006 Jun;17(6):885–887. doi: 10.1093/annonc/mdl073. Epub 2006 Apr 20. [DOI] [PubMed] [Google Scholar]
- 22.Office for National Statistics. Cancer Incidence and Mortality in the UK, 2007-2009. London, England: Office for National Statistics;; 2012. [Google Scholar]
- 23.British Pain Society. Cancer Pain Management. London, England: British Pain Society;; 2010. [Google Scholar]
- 24.Hill CS., Jr The barriers to adequate pain management with opioid analgesics. Semin Oncol. 1993 Apr;20((2 Suppl 1)):1–5. [PubMed] [Google Scholar]
- 25.British Pain Society. The Use of Drugs Beyond Licence in Palliative Care and Pain Management. London, England: The Association for Palliative Medicine and the British Pain Society;; 2005. [Google Scholar]
- 26.Fotedar KK. WHO ladder—relevance in today's world. Int J of Perioperative Ultrasound and Appl Technol. May-August. 2013;2(2):49–53. [Google Scholar]
- 27.World Health Organization. Cancer Pain Relief. 2nd ed. Geneva, Switzerland: World Health Organization;; 1996. [Google Scholar]
- 28.British Pain Society. Opioids for Persistent Pain: Good Practice. London, England: British Pain Society;; 2010. [Google Scholar]
- 29.British Pain Society. Pain and Problem Drug Use: Information for Patients. London, England: British Pain Society; 2007. http://www.britishpainsociety.org/book_misuse_patients.pdf. Accessed March 19, 2014. [Google Scholar]
- 30.Green CR, Anderson KO, Baker TA, et al. The unequal burden of pain: confronting racial and ethnic disparities in pain. Pain Med. 2003 Sep;4(3):277–294. doi: 10.1046/j.1526-4637.2003.03034.x. Erratum in: Pain Med. 2005 Jan-Feb;6(1):99. [DOI] [PubMed] [Google Scholar]
- 31.Bair MJ, Matthias MS, Nyland KA, et al. Barriers and facilitators to chronic pain self-management: a qualitative study of primary care patients with comorbid musculoskeletal pain and depression. Pain Med. 2009 Oct;10(7):1280–1290. doi: 10.1111/j.1526-4637.2009.00707.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.US Census Bureau. Number of older americans. AgingStats.gov. 2008 http://www.agingstats.gov/Agingstatsdotnet/Main_Site/Data/2008_Documents/Population.aspx. Accessed March 19, 2014. [Google Scholar]
- 33.Gordon DB, Dahl JL, Miaskowski C, et al. American pain society recommendations for improving the quality of acute and cancer pain management: American Pain Society Quality of Care Task Force. Arch Intern Med. 2005 Jul 25;165(14):1574–1580. doi: 10.1001/archinte.165.14.1574. [DOI] [PubMed] [Google Scholar]
- 34.Meier DE. Palliative care in hospitals. J Hosp Med. 2006 Jan;1(1):21–28. doi: 10.1002/jhm.3. [DOI] [PubMed] [Google Scholar]
- 35.Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin. 2009 Jul-Aug;59(4):225–249. doi: 10.3322/caac.20006. Epub 2009 May 27. [DOI] [PubMed] [Google Scholar]
- 36.Deandrea S, Montanari M, Moja L, Apolone G. Prevalence of undertreatment in cancer pain. A review of published literature. Ann Oncol. 2008 Dec;19(12):1985–1991. doi: 10.1093/annonc/mdn419. Epub 2008 Jul 15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.MacDonald N, Ayoub J, Farley J, Foucault C, Lesage P, Mayo N. A. Quebec survey of issues in cancer pain management. J Pain Symptom Manage. 2002 Jan;23(1):39–47. doi: 10.1016/s0885-3924(01)00374-8. [DOI] [PubMed] [Google Scholar]
- 38.Ministry of Health Malaysia. Management of Cancer Pain. Putrajaya, Malaysia: Ministry of Health Malaysia; 2010. http://www.acadmed.org.my/index.cfm?&menuid=67. Accessed March 19, 2014. [Google Scholar]
- 39.Devi BC, Tang TS, Corbex M. Setting up home-based palliative care in countries with limited resources: a model from Sarawak, Malaysia. Ann Oncol. 2008 Dec;19(12):2061–2066. doi: 10.1093/annonc/mdn422. Epub 2008 Jul 17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Murthy NS, Chaudhry K, Rath GK. Burden of cancer and projections for 2016, Indian scenario: gaps in the availability of radiotherapy treatment facilities. Asian Pac J Cancer Prev. 2008 Oct-Dec;9(4):671–677. [PubMed] [Google Scholar]
- 41.Murthy NS, Juneja A, Sehgal A, Prabhakar AK, Luthra UK. Cancer projection by the turn of century-Indian science. Indian J Cancer. 1990 Jun;27(2):74–82. [PubMed] [Google Scholar]
- 42.Takiar R, Nadayil D, Nandakumar A. Projections of number of cancer cases in India (2010-2020) by cancer groups. Asian Pac J Cancer Prev. 2010;11(4):1045–1049. [PubMed] [Google Scholar]
- 43.Redmond K. Organizational barriers in opioid use. Support Care Cancer. 1997 Nov;5(6):451–456. doi: 10.1007/s005200050113. [DOI] [PubMed] [Google Scholar]
- 44.Rajagopal MR, Joranson DE, Gilson AM. Medical use, misuse, and diversion of opioids in India. Lancet. 2001 Jul 14;358(9276):139–143. doi: 10.1016/s0140-6736(01)05322-3. [DOI] [PubMed] [Google Scholar]
- 45.Grant M, Elk R, Ferrell B, Morrison RS, von Gunten CF. Current status of palliative care—clinical implementation, education, and research. CA Cancer J Clin. 2009 Sep-Oct;59(5):327–335. doi: 10.3322/caac.20032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Varghese C. Cancer Prevention and Control in India. New Delhi, India: National Cancer Control Programme; 2002. http://www.indg.in/india/sitemap-1/health/national_health_programmes/Cancer%20Prevention%20and%20Control%20in%20India.pdf. Accessed March 19, 2014. [Google Scholar]
- 47.Pain & Policy Studies Group. Availability of Opioid Analgesics in Latin America and the World. Guadalajara, Mexico: 2002. Prepared for: 1st Congress of the Latin American Association of Palliative Care, 7th Latin American course on medicine and palliative care; March 20-22. [Google Scholar]
- 48.De Lima L, Bruera E, Joranson DE, et al. Opioid availability in Latin America: the Santo Domingo report. Progress since the Declaration of Florianopolis. J Pain Symptom Manage. 1997;13(4):213–219. doi: 10.1016/s0885-3924(96)00325-9. [DOI] [PubMed] [Google Scholar]
- 49.De Lima L. Advances in palliative care in Latin America and the Caribbean: ongoing projects of the Pan American Health Organization (PAHO) J Palliat Med. 2001 Summer;4(2):228–231. [PubMed] [Google Scholar]
- 50.Joint United Nations Programme on HIV/AIDS (UNAIDS) Global report: UNAIDS report on the global AIDS epidemic. Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS (UNAIDS); 2013. http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiology/2013/gr2013/UNAIDS_Global_Report_2013_en.pdf. Accessed March 31, 2014. [Google Scholar]
- 51.Clark D, Wright M, Hunt J, Lynch T. Hospice and palliative care development in Africa: a multi-method review of services and experiences. J Pain Symptom Manage. 2007 Jun;33(6):698–710. doi: 10.1016/j.jpainsymman.2006.09.033. [DOI] [PubMed] [Google Scholar]
- 52.International Narcotics Control Board. Madison, WI: Pain & Policy Studies Group; 2011. Global Opioid Consumption. http://www.painpolicy.wisc.edu/global. Accessed March 19, 2014. [Google Scholar]
- 53.Cleary J, Powell RA, Munene G, et al. Formulary availability and regulatory barriers to accessibility of opioids for cancer pain in Africa: a report from the Global Opioid Policy Initiative (GOPI) Ann Oncol. doi: 10.1093/annonc/mdt499. 13 Dec; 24 Suppl 11:xi14-xi23. [DOI] [PubMed] [Google Scholar]
- 54.Joranson DE, Ryan KM. Ensuring opioid availability: methods and resources. J Pain Symptom Manage. 2007 May;33(5):527–532. doi: 10.1016/j.jpainsymman.2007.02.013. [DOI] [PubMed] [Google Scholar]
- 55.Jagwe JJ, Merriman AA. Uganda: delivering analgesia in rural Africa: opioid availability and nurse prescribing. J Pain Symptom Manage. 2007;33:547–551. doi: 10.1016/j.jpainsymman.2007.02.014. [DOI] [PubMed] [Google Scholar]
- 56.Waldman S. Pain Management. 2nd ed. Philadelphia, PA: Elsevier;; 2011. ed. [Google Scholar]
- 57.Deshpande CM, Mohite SN, Kamdi P. Sufentanil vs fentanyl for fast-track cardiac anaesthesia. Indian J Anaesth. 2009 Aug;53(4):455–462. [PMC free article] [PubMed] [Google Scholar]
- 58.Macintyre PE, Jarvis DA. A phase 2 multicenter, randomized, placebo-controlled study to evaluate the clinical efficacy, safety, and tolerability of sublingual Sufentanil NanoTab in patients following elective unilateral knee replacement surgery. Pain. 1995;64:357–364. [Google Scholar]
- 59.Buonsenso D, Barone G, Valentini P, Pierri F, Riccardi R, Chiaretti A. Utility of intranasal ketamine and midazolam to perform gastric aspirates in children: a double-blind, placebo controlled, randomized study. BMC Pediatr. 2014 Mar 5;14(1):67. doi: 10.1186/1471-2431-14-67. [DOI] [PMC free article] [PubMed] [Google Scholar]