

Abstract
The ability to extract different bio-medical parameters from one single wristwatch device can be very applicable. The wearable device that is presented in this paper is based on two optical approaches. The first is the extraction and separation of remote vibration sources and the second is the rotation of linearly polarized light by certain materials exposed to magnetic fields. The technique is based on tracking of temporal changes of reflected secondary speckles produced in the wrist when being illuminated by a laser beam. Change in skin’s temporal vibration profile together with change in the magnetic medium that is generated by time varied glucose concentration caused these temporal changes. In this paper we present experimental tests which are the first step towards an in vivo noncontact device for detection of glucose concentration in blood. The paper also shows very preliminary results for qualitative capability for indication of dehydration.
OCIS codes: (030.6140) Speckle, (280.0280) Remote sensing and sensors, (170.0170) Medical optics and biotechnology, (260.2110) Electromagnetic optics, (260.5430) Polarization
1. Introduction
Glucose plays a central role in metabolism: it is the principal metabolic pathway for transporting carbohydrates and is an important fuel for spurring metabolic energy in all human cells. Glucose plays a main role in many of the biochemical reactions that modulate the metabolic profile both physiologically and in pathologically.
Diabetes mellitus is a group of metabolic diseases in which a person has high level of glucose concentration in blood, which is caused because the pancreas does not produce enough insulin (diabetes type 1), or because the cells do not respond to the insulin that is produced (diabetes type 2). Type I diabetes is referred to as “insulin-dependent diabetes mellitus” (IDDM) or “juvenile diabetes”. Type II diabetes, which is related to the modern life style, is referred to as non insulin-dependent diabetes mellitus (NIDDM) or “adult-onset diabetes”. The latter form of diabetes constitutes >95% of all diabetic patients and affects 25.8 million people of all ages in the U.S (8.3 percent of the U.S population) [1] and 347 million people worldwide suffer from diabetes [2].
The development of a noninvasive method to measure glucose concentration is one of the most important goals of medicine. Since diabetic patients have to continuously monitor their blood glucose level. Currently, the most common way to measure glucose is by pricking a finger and applying the blood droplet to a strip that is inserted into a glucometer. The flux of the glucose reaction generates an electrical signal and the glucometer corresponds to the strength of the electrical current.
Despite the impressive advances in glucose biosensors, there are still many challenges related to the achievement of reliable glycemic monitoring. Desirable features of a biosensor system are accuracy, reliability, ultra-sensitivity, fast response, and low cost per test. In order for the procedure to be more comfortable and simple, a few optical non-invasive methods have been developed.
One method is photo-acoustic spectroscopy, which is based on the conversion of optical energy into acoustic energy through a multi-stage energy conversion process that uses a piezoelectric detector. A change in the photoacoustic pulse was found when the glucose concentration in the blood was altered [3]. Another example is optical coherence tomography (OCT). By using an interferometer with a light that is aimed at the subject, the light that backscatters from structures within the tissue interferes with the light from the reference arm. This method is based on a phenomenon in which the increase of glucose concentration in the blood decreases the scattering coefficient [4]. Another method is scattering where the result of increasing extracellular glucose concentration makes the refractive index increase, causing a decrease in the overall tissue scattering coefficient [5].
The referenced methods are not more widespread due to some disadvantages: (1) Photo-acoustic noninvasive glucose testing techniques demand a selection of a specific wavelength per subject which makes it hard for the development of the operational product. (2) In noninvasive monitoring of glucose concentration with OCT, the experiments were conducted in vitro with specific conditions (e.g. size of cell diameter), while other mechanisms of changes of OCT slope with glucose concentration are excluded from the experiments. (3) In polarization-based diffuse reflectance the experiments were not conducted on human subjects, while other substances present in skin and surrounding tissues could confound measurements of this type.
Other efforts to develop a noninvasive method to measure glucose concentration were not too successful. Recently, CNoga Medical Ltd. developed a Combo Glucometer. The device’s technology is based on four light emitting diodes (LEDs). The range of the illuminating wavelengths is 600 nm to 1150 nm (visual light to near infrared light). Due to the absorption, when the light passes the fingertip, the spectrum that is detected also changes. The processor analyzes the signal and extracts the bio parameters from the signal [6]. Another company that developed a non-invasive method to measure glucose level through the eye is Oculir which uses an infra-red laser aimed at the sclera (the white structure of the eye). The laser beam is reflected from membranes and vessels inside the eye ball back to the detector. Glucose has a high absorption rate of mid infrared radiation. As a result of this strong absorption – the light reflected back to the device is proportional to the glucose concentration in the blood [7]. Another company that developed a device that monitors glucose is Integrity Applications Ltd. The technology is a combination of three real-time technologies: ultrasonic, electromagnetic, and thermal. Each technology measures different bio-parameters that change according to the change in glucose concentration [8].
In this paper the performance of a device that monitors the glucose concentration in the blood is described by using a new patented approach [9–13]. The described configuration includes observation of the secondary speckle pattern that is created by illuminating the human skin near blood artery with a laser beam and a magnetic field that is created by a magnet attached to the apparatus. Speckles are self-interfered random patterns generated due to optical interference of the wavefronts [14]. By using this technology, the skin’s temporal movement can be tracked. Various bio-parameters can be monitored from the blood flux pulsation. The magnetic field is necessary in order to create the Faraday effect which is the rotation of the plane of vibration of linearly polarized light when passing through a medium [15,16]. Changing the polarization state of the wavefront results in a change to the detected speckle field [16].
In the experiment the blood with the varying glucose concentration was interacting with the electromagnetic medium in which the Faraday effect interaction occurs. Changing the glucose concentration results in a change to the polarization state of a wavefront. The magnet in the suggested device is incorporated into a bracelet in which the optical detector is placed. This magnet produces a magnetic field which results in greater sensitivity and accuracy in the readings of the glucose measurements.
As glucose, dehydration is a vital biomedical parameter that needs continuous monitoring. The ability to monitor dehydration level by remote optical measurement can be useful in the physical activity of athletes and in the military as described in scientific literature [17–19]. Furthermore, dehydration can be a cause for delirium as well as a contributing factor to dementia in the elderly and in the very ill [20, 21]. A severe level of dehydration is considered a risk factor for heat exhaustion and heat stroke. Thus, remote optical measurement can be advantageous for multiple areas of study and practical to those engaged in extensive physical efforts and/or exposed to environmental heat stress.
Water is the main constituent of our body. There are more water molecules than any other molecule in the human body (about 60% of the body weight is water). At ambient comfort conditions (18–20 Cº) and low metabolic rate (rest to light exercise), water levels in the body are well regulated [22]. When there is negative balance between fluid loss and fluid consumption dehydration ensue. It is customary to refer to dehydration in three levels: mild, moderate, and severe. The signs and symptoms exacerbate from dry and sticky mouth, sleepiness or tiredness, to oliguria and anuria, delirium and unconsciousness. Severe cases of dehydration (>10%) can be fatal [22].
There are a few methods to determinate hydration status. One method is by measuring blood concentration (plasma osmolality) and another method is by urinalysis (analysis of urine) and urine specific gravity (SG) [23]. However, both methods cannot monitor dehydration during activity without taking a blood or urine sample.
Recently, another method to measure dehydration level was proposed [24] where the dehydration level is measured by the impedance or opposition to the flow of an electric current through the body fluids using an electrical model of cells and the principle of bioelectrical impedance.
In this paper we show how the same wearable device that is used to monitor the glucose concentration in the blood stream is also used to measure the indication of dehydration level. As with glucose, preliminary clinical trials are done to validate proposed operation principle for dehydration. Note that the approach presented here is only the first step towards the development of such a wearable module and further development is needed such as motion cancellation mechanism in order to make it more robust.
The novelties presented in this paper are as follows: (1) a more accurate and modified technique with respect to what we have presented before in [25] which is demonstrated by adding a magnet to the speckle based monitoring device. The work reported in [25] was based only on one effect: tracking of temporal changes of reflected secondary speckle pattern produced in the wrist for glucose concentration in the blood stream. The improved accuracy is obtained due to the fact that there is a second Faraday based effect that is also changing the speckle distribution with time. (2) for the first time a dehydration device was constructed and its operation principle was clinically demonstrated (for qualitative and quantitative estimation of dehydration), (3) an integrated and wearable module was constructed and used for the measurements of both biomedical parameters: glucose and level of dehydration.
2. Remote optical measurement of glucose in blood stream
2.1. Theoretical explanation
The device used to measure the glucose concentration or the dehydration level is a simple bracelet with a CMOS camera and a green laser (at 532 nm). To demonstrate the use of Faraday effect, we added a magnet to the bracelet as shown in Fig. 1 . The polarization rotation angle for light beam propagating through magneto-optic materials is [16]:
| (1) |
Where ϑis Verdet constant, B the magnetic field and L is the interaction length, λ0 is the optical wavelength and is the difference in index of refraction between two circularly polarized states leading to the rotation. As proven before [16], the minimal magnetic field Bmin needed to de-correlate the speckle field is proportional to:
| (2) |
R is the radius of the illuminating beam and L is the interaction length. Equation (2) defines the sensitivity of the proposed approach.
Fig. 1.

Schematic diagram of the system.
The temporal movement of the reflecting surface causes changes in the random speckle pattern over time. First a set of images as a function of time is measured. These sequential images are correlated in the second step. By calculating the correlation the relative movement of patterns can be extracted. This relative movement is obtained by allocating the time varying position of the correlation peak. The temporal movement of the human skin that is caused by the blood pulse stream is proportional to the relative shift of the speckle pattern [14]:
| (3) |
β is the change in the speckle pattern, α is the tilting angle of the illuminated surface (in our case, the human skin) and λ is the wavelength (in our case, 532 nm).
The temporal change of glucose concentration Cv(t) is proportional to the temporal change of β(t) [17]:
| (4) |
According to the last equation (Eq. (4) the relative shift of the speckle pattern monitors the change of the temporal glucose concentration.
In the following scheme (Fig. 2 ) one can see the chart flow with the explanation of the contribution of the temporal movement of the skin and the Faraday effect to the speckle pattern change. The importance of the magnet is that it allows interaction only with glucose and not other materials because of the high Verdet constant of the glucose molecule in contrast to molecules of other materials in our blood stream.
Fig. 2.

A flowchart of the glucose concentration effects on the speckle pattern.
2.2. Experimental results
The setup is a device worn like a bracelet (Fig. 3 ). It consists of a green laser (at 532nm) and a camera attached to the bracelet. The camera is also connected to a computer. In order to obtain a magneto-optic effect, a magnet was attached to the device.
Fig. 3.

The optical configuration for remote measuring of glucose levels from the subject’s hand. The subject’s hand is under laser illumination. The magnet is connected to the side of the device.
The camera (PixelLink PL-E531) captures images of the secondary speckle pattern reflected from the subject’s hand at the rate of 545 frames per second (fps). The distance from the laser to the subject’s hand is approximately 5cm. The laser output power is approximately 5mW.
In order to achieve good temporal resolution we want to increase our sampling rate. For example, each pulse is about 0.2 sec, we want to sample at least 20 samples in this period. On the other hand, if the frame rate is too high, the measured temporal peaks will be too low (less energy per sample). In the experiment we choose the sampling rate to be 545 frames per second as a result of this tradeoff.
After extracting the speckle pattern in each frame, we calculate the correlation and obtain a change in the 2-D position of the correlation peak versus time [25]. Figure 4 shows the raw data of 2-D correlation images sequence which we denote ‘OCG’ (Optical CardioGram). Every pulse is shaped similarly to an ECG PQRST pulse. The average of five pulses is taken for further calculations. The graph in Fig. 5 is a flowchart showing the algorithm we use for the monitoring of the glucose concentration and the dehydration level. The algorithm is mainly based upon correlation between the images of the speckle patterns in temporally adjacent frames and checking the movement in the position of the obtained correlation peak.
Fig. 4.
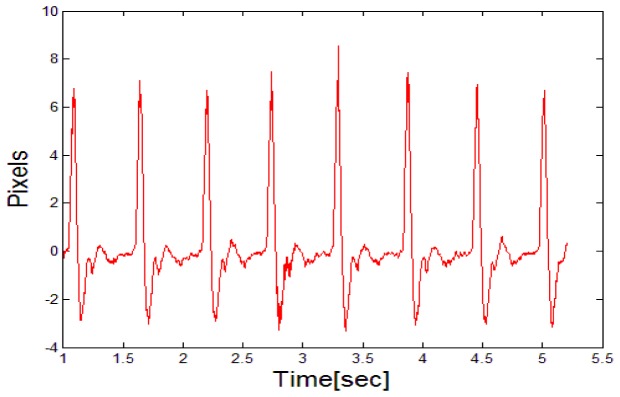
The OCG pulses that were measured by our bracelet setup.
Fig. 5.

Summary of the algorithm.
The observed parameters from the video files were analyzed by a specific MATLAB program that was written for this purpose. Each file contained approximately 5 seconds of video samples at a rate of 545 fps. From the OCG graph, the maximum pulse amplitude that refers to the highest amplitude during one heartbeat was analyzed. In each measurement 4 to 7 peaks were taken and then averaged. Our aim is to demonstrate that the average amplitude in each frame is correlated with the two bio-medical parameters measured in this paper as demonstrated in the following sections.
In all experiments the subjects were healthy people and their blood pressure was measured throughout the experiment in order to make sure that indeed there is no other effect on β (see Eq. (3)) other than the change in the glucose concentration.
2.2.1. Stability test
The stability of the averaged amplitude (the optical parameter) was checked to quantify the performance of the device and to ensure that the changes on the OCG graph were indeed the result of the glucose concentration. Glucose levels were taken after 12 hours of fasting and the subjects did not eat or drink during the test (except for the sweetened drinks). To compare the optical parameter to the glucose concentration we normalized the optical parameter to the actual glucose parameter. Glucose concentration levels are given as mg/dl and the units of the measured optical parameter are presented as pixels. A blood sample from a finger was taken to measure the glucose concentration with a glucometer (FreeStyle Lite Blood Glucose Monitoring System [26]). Immediately afterwards 4 optical measurements were taken (i.e. the average from four OCG graphs and the respective four peak amplitudes were considered).
The optical measurements were then compared to the glucometer values. During a period of 30 min. every five minutes four frames were analyzed and at the end of the 30 minutes period another glucometer reading was performed. The first glucometer value was 88[mg/dl] and the final value was 84[mg/dl]. In Fig. 6 one can see that the highest deviation from the first normalized value is not more than 8.8% during the 30 minute span of the tests.
Fig. 6.

Stability test of the system: The normalized optical parameter during 30 minutes. The difference in values is displayed [in percents].
2.2.2. Main test
The main test was divided into 2 parts. Initially, experiments were done on the subject, on whom the stability test was performed (a non-diabetic 28 years old male; 73 kg), and repeated the same protocol several times.
The subject came to the lab after 12 hours fast. First both the optical parameter and a blood sample were taken for a calibration purpose. Immediately afterwards the subject drank 500 ml of grape soda. The ingredients of the soda are shown in Table 1 .
Table 1. Nutritional values of 500 ml grape soda.
| Quantity | Units | |
|---|---|---|
| Energy | 195 | cal |
| Carbohydrates | 50 | g |
| Protein | 0 | g |
| Fats | 0 | g |
| Sodium | 50 | mg |
| Vitamin C | 30 | mg |
After the subject drank the entire bottle of grape soda, samples of the optical and the glucometer devices were taken every five minutes during the period when the glucose level was increasing and between five and fifteen minutes during the drop in glucose concentration.. First, in order to prove the benefit of Faraday effect, we removed the magnet from the device. The experiment was done under the same conditions as the following experiments with the magnet. One can see in Fig. 7(a) and 7(b) that in comparison to the experiments with the magnet there is tracking of glucose concentration only during the first 20 minutes of the experiment while during the experiment with the magnet the tracking is continued through the entire experiment during the negative slope of the modified concentration.
Fig. 7.
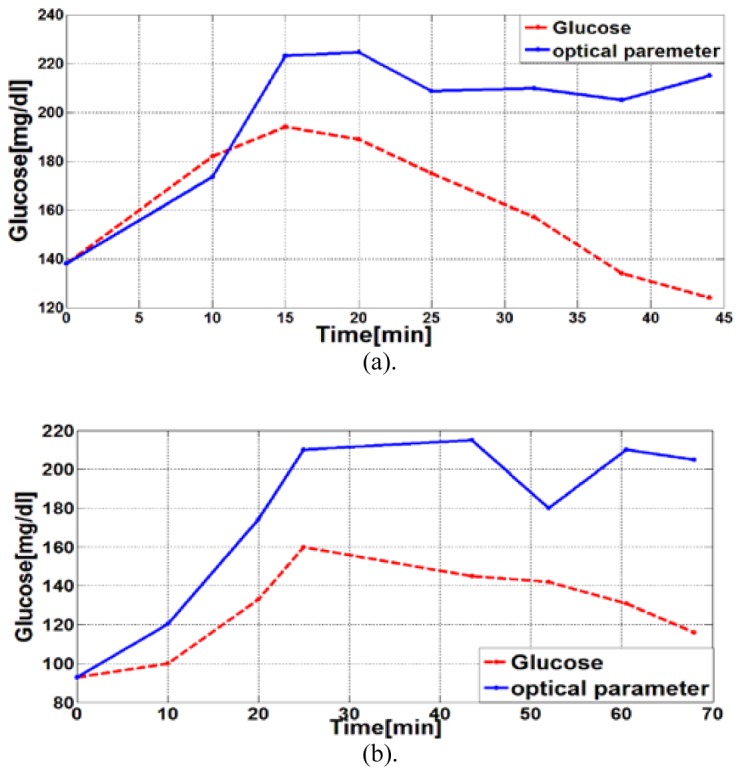
An experiment without the effect of the magnet. Glucose level is denoted with a red line (measured with glucometer device) and the optically measured parameter is denoted with a blue line. (a). First experiment completely without a magnet. (b). Second experiment completely without a magnet.
In the next step, the magnet was connected to our bracelet device. The duration of the experiments were between 45 to 85 minutes in order to track the increase and decrease in glucose level and in order to have time for the subject’s glucose level to return to its baseline level and remain stable. Some of the obtained results are presented in Fig. 8 .
Fig. 8.

Normalized Glucose level in blood and the normalized peak amplitude of the same subject. Glucose level is denoted with a red line and the optically measured parameter is denoted with a blue line.
The four different panels in Fig. 8 refer to the experiments taken with the same subject on different days. The glucose and the optical parameter values were normalized by the maximum value of the glucose concentration and the optical parameter measured in our experiment.
The standard deviation (STD) of each measurement samples (the error bars that are shown in Fig. 8 and Fig. 9 ) was calculated by the equation:
| (5) |
where and n is the number of elements in the sample. The optically measured parameter is tracking glucose level measured with a glucometer; the optical measurement fluctuates as the glucose level returns to baseline.
Fig. 9.

Normalized Glucose level in blood and the normalized peak amplitude of 4 different subjects. Glucose level is denoted with a red line and the optically measured parameter is denoted with a blue line.
In the second part of the study the glucose level of four other subjects was measured, whose characteristics are summarized in Table 2 .
Table 2. Summary of subject information.
| # | Gender | Age[Years] | Weight[kg] |
|---|---|---|---|
| 1 | Male | 22 | 95 |
| 2 | Male | 28 | 75 |
| 3 | Male | 47 | 84 |
| 4 | Male | 37 | 88 |
The protocol according to which those subjects were tested is exactly as described above. The duration of the experiment was between 45 and 55 minutes until the glucose readings returned to baseline levels and remained stable. Some of the results are presented in Fig. 9.
It is evident from Fig. 9 that the patterns of changes in the optical and glucometer values are similar to the preliminary results that were described above.
In order to examine the performance of our device in the last experiments (Figs. 8, 9) we checked every sample out of the 70 optical measurements we had all together (all trials over all subjects). The maximal error we had was around 30%.
Although it was obtained due to lack of accuracy in our device itself, one also needs to remember that the readout of the glucometer to which our measurement was compared also had in average of 20% error (thus the error between our measurement and the true glucose concentration in the blood stream could have been only 10% in this case). We also saw that 95.71% out of our optical measurements were with less than 15% deviation from the readout made by the reference glucometer measurement. It is also important to note that one major factor of our errors is related to the fact that our sensor was moving in respect to the wrist during the measurement itself. This problematic movement will be compensated with motion compensator that will be added to our watch in the near future. The reduction of the error will also be done via a more general calibration process.
There are 3 main ways to diagnose diabetes: (1) Fasting Plasma Glucose (FPG): the blood glucose concentration after fasting 8 hours is greater than 126 mg/dl. (2) Oral Glucose Tolerance Test (OGTT): two-hour test that monitors the subject’s glucose blood levels before and 2 hours after the subject drank a sweet liquid. Diabetes is diagnosed in this test as greater than or equal to 200 mg/dl. (3) Casual Plasma Glucose Test: blood check any time of the day in a case of severe diabetic symptoms. Diabetes is diagnosed in this test as greater than or equal to 200 mg/dl. If we consider that 95.7% of our optical measurements are within the error range, there might be a big usefulness of our technique in the medical practice due to the fact that we present a very simple device that might be applied for diabetic diagnostics. Also please note that our device does not have to be used for medical diagnostics but rather for the field of wellness in which the people that use the device are healthy (e.g. people that monitor their diet or sportsmen) and the device is aimed to provide only the trend of the glucose concentration in their blood stream.
3. Experimental results for remote optical monitoring of dehydration
In this section, we show that the same optical principle used to monitor glucose concentration can also be applied for monitoring dehydration level. Essentially, we report on the use of a similar device than the one included in Fig. 1 and 3 but without the magnet attached to it. The reference for the dehydration level is the relative change in body weight.
The experiments were conducted in collaboration with a medical physician from Tel-Ha-Shomer hospital in Israel. It was done as part of the ongoing Helsinki approved medical research on dehydration that is being conducted in Heller Institute of Medical Research.
In these experiments the water loss was estimated by weighing the subject before and after the experiment. The dehydration protocol consisted of sitting in a chamber with an inside temperature of 50 °C. Every few minutes, the chamber was ventilated in order to prevent excessive heat absorbance and hyperthermia. During the heat exposure three OCG measurements were taken, with the bracelet device described above. The measurements were taken at three time points: 0 minutes, 40 minutes, and 70 minutes of exposure. Three healthy individuals, whose characteristics are outlined in Table 3 , were studied.
Table 3. Summary of subject’s information.
| # | Gender | Age[Years] | Weight[kg] |
|---|---|---|---|
| 1 | Male | 22 | 95 |
| 2 | Male | 28 | 75 |
| 3 | Male | 47 | 84 |
3.1 Standard deviation of background fluctuations
The fluctuations of the segment that is shown in Fig. 10 were examined. The region is marked and zoomed in at time 0 (the beginning of the exposure) and after 70 minutes (the end of the exposure).
Fig. 10.

(a). The OCG pulses that were measured at the beginning of the experiment in order to calibrate the system. The ellipse marks the region of the fluctuations. (b). Close-up of the fluctuations at the beginning of the experiment (time 0) that corresponds to the ellipse markup in Fig. 6(a). (c). The OCG pulses that were measured at the end of the experiment (after 70 minutes). The ellipse marks the region of the fluctuations. (d). Close-up of the fluctuations at the end of the experiment (after 70 minutes).
STD analysis of 4 sequential segments were selected (i.e. 4 test regions before the positive slope of 4 consecutive pulses). The segment was chosen to be 0.2 sec just before the high stroke in pulse profile. The results are shown in Table 4 .
Table 4. The STD of background fluctuation at the beginning and end of the dehydration experiment.
| Time(min) | Std 1 | Std 2 | Std 3 | Std 4 | Average | Weight[Kg] | ∆Weight (%) | |
|---|---|---|---|---|---|---|---|---|
| Subject #1 | 0 | 0.0372 | 0.0321 | 0.0338 | 0.0406 | 0.0359 | 74.4 | 0.67 |
| 70 | 0.0767 | 0.1264 | 0.1363 | 0.0611 | 0.1 | 73.9 | ||
| Subject #2 | 0 | 0.0331 | 0.0402 | 0.0334 | 0.0314 | 0.0345 | 95.5 | 0.52 |
| 70 | 0.0678 | 0.0763 | 0.0725 | 0.0845 | 0.0752 | 95 | ||
| Subject #3 | 0 | 0.0502 | 0.0542 | 0.1032 | 0.084 | 0.0729 | 83.9 | 1.31 |
| 70 | 0.0672 | 0.0628 | 0.0743 | 0.093 | 0.0743 | 82.8 |
One of the main signs of mild to moderate dehydration is muscle weakness [22], this sign caused the change in the pulse shapes standard deviation. The STD for the segments at the end of the exposure is higher compared to those at the time 0. As shown in Table 5 , the subjects lost from 0.5% to 1.31% of their weight. With this parameter, one can see that even insignificant changes in the body’s water balance can be effectively monitored.
Table 5. Summary of measured values by subject.
| Time [Min] | Weight [Kg] |
Optical parameter
[normalized kg] |
Weight [%] | Optical parameter [%] | |
|---|---|---|---|---|---|
| Subject #1 | 0 | 74.4 | 74.2 | 100 | 100 |
| 40 | - | 63.14 | - | 85.09 | |
| 70 | 73.9 | 66.28 | 99.33 | 89.33 | |
| Subject #2 | 0 | 95.5 | 95.5 | 100 | 100 |
| 40 | - | 32.41 | - | 33.94 | |
| 70 | 95 | 32.01 | 99.47 | 33.52 | |
| Subject #3 | 0 | 83.9 | 83.9 | 100 | 100 |
| 20 | - | 48.25 | - | 57.51 | |
| 70 | 82.8 | 33.33 | 98.68 | 39.73 |
3.2 Maximum pulse amplitude
The comparison of the same bio-medical parameter that was examined in the glucose study (refers to the highest amplitude during one heartbeat) can be applied to evaluate changes in body weight due to dehydration. In this case the weight is linearly transformed to the estimated values according to the calibration at the first measurement (time = 0). The results for each of the participants are presented in Fig. 11(a) -11(c). The sensor was moving in respect to the wrist during the measurement itself. In order to prevent these movements it was decided to measure the weight at the end of the experiment (not to bother the subject with more movements). This problematic movement will be compensated with a motion compensator that will be added to our watch in the near future.
Fig. 11.

Weight of tested subjects compared to the maximum amplitude peak measured by the proposed optical device. The weight is denoted by a red line and red axes and the optically measured parameter is denoted by a black line and black axes. (a). First subject. (b). Second subject. (c). Third subject.
Table 5 shows the measured values for each subject.
The first subject’s weight was 74.4kg at the beginning of the experiment and 73.7kg at the end of exposure. The peaks' pulse amplitude and the weight were calibrated to be 100% and then the changes in weight to the changes in the optically measured parameter were compared. The big decrease in the optically measured parameter is an indication of the dehydration level in each subject. At time 0 average of 4.31 pixels were measured, at 40 minutes 3.5 pixels, and at time 70 min 3.6 pixels.
The reason for the minimal change between the last two measurements was regarded to the increase in the number of times the chamber's door was opened in the last 30 minutes compared to the first 40 minutes. The optically measured parameter of the second subject decreased even more sharply between the first and the second measurement. Between the second and the third measurement there was no change due to the increase in the number of times the chamber door was opened in the last 30 minutes. The measurements of the third subject also show a sharp decrease after 40 minutes. Furthermore, there is a decrease between the last two measurements. The results are compatible with what was expected due to the chamber door being opened the same number of times in the last 30 minutes as compared to the first 40 minutes. For this reason, the third subject lost the most weight compared to the others.
The temporal β signal is very informative and different biomedical related factors have different effect on its shape. Thus, it can be correlated also to dehydration estimation. In both experiment (glucose and dehydration) the measurement was very controlled and the blood pressure was measured in order to make sure that the changed caused by the dehydration is not related to the change in the blood pressure. All subjects that participated in the experiment were healthy people without blood pressure problems.
Although there should be a calibration made for every subject for conversion of the measured optical parameters into the proper medical units of the specific monitored biomedical factor, the calibration is done only once and it can hold for a long period of time of at least a few weeks (experimental evidence of this claim can be found in [14]. At the end of this reference, the author presents an experiment conducted during a year. The results of this experiment show that the OCG signature was maintained during this long period).
In the case of dehydration the idea is not to do a diagnostics but only to obtain a general indication of amount of water in the tissue. Therefore in the case of the dehydration measurement we do not claim for accuracy or reliability but just that our monitoring device has general estimation capability as it is aimed for the wellness market.
Other chemicals in blood may also have similar effects on the measured parameter. However, one needs to note not only the effect but its amount as well. The amount of dehydration that we measured was very significant and presented as percentages out of the overall body weight. This is a very significant amount of liquids expressed in liters. Change in other chemicals in the body are never in such large quantities and thus it was relatively simple to distinguish between the two. The fact that dehydration measures only such large amount of liquids is sufficient in sense of precision as only large amounts really affect the body functionality and if commercial application is to be considered in the future, this is the exact range of precision that is required. Thus, although in the general case, various chemicals in the blood stream can affect the vibration profile and therefore to properly distinguish between them a more complicated signal processing algorithm is needed, in the dehydration case this problem is not evident.
4. Conclusions
In this paper the use of optical remote configuration for the estimation of glucose concentration in blood and dehydration level was presented. This is the first step towards developing a wearable in vivo module for measurement of glucose and for qualitative estimation of dehydration levels. “The testing of both parameters were optically monitored continuously via the same device and in the same conditions. Thus, the system can measure both biomedical parameters simultaneously and independently. Still several technological challenges are to be overcome in order to make the proposed sensor an applicable wearable device. The main challenge is to add a motion cancelation mechanism since at the moment the best results were obtained in the case when the sensor was more stable and more fixed with respect to the wrist of the subject. Further maturing of a more robust, generic and automatic calibration process that will translate the optical readout into the exact value of the estimated biomedical parameter is also required.
The glucose test showed high percentage of prediction in the sense that around 96% of our optical measurements were with less than 15% deviation from the readout made by the reference glucometer measurement. The estimated results in the dehydration test showed two independent parameters that can indicate a change in body water levels. The measurements in the case of dehydration were only qualitative and not quantitative. In this paper we presented the preliminary capability to correlate between the temporal changes in the vibration profile of the pulse wave measured from the wrist with our optical device to the change in glucose concentration in the blood and to the dehydration level. The magnet was added to the system in order to enhance the sensitivity of our measurement by using Faraday’s effect and in order to trace both the negative and the positive slope in the glucose concentration change, and it has proven to be more effective compared with to what we have presented before in Ref [25].
The suggested simple device was remote and used non-invasively. Unlike previous attempts based on detection of glucose which used relatively high power lasers, our device used only a very low power emitting laser (only a few mW), a camera, and a magnet that may simply be combined and assembled into a bracelet.
As both biomedical parameters (glucose and dehydration) are related to nutrition, further developments of this technology will allow the implementation of an autonomic and real-time monitoring device, which will be capable of analyzing changes in glucose concentration in the blood and dehydration level during activity while allowing free movement of the subject.
Acknowledgment
Part of this work has been funded by the Spanish Ministerio de Economía y Competitividad and the Fondo Europeo de Desarrollo Regional (FEDER) under the project FIS2010-16646.
References and links
- 1.National Diabetes Information Clearinghouse (NDIC) , http://diabetes.niddk.nih.gov/dm/pubs/statistics/
- 2.Danaei G., Finucane M. M., Lu Y., Singh G. M., Cowan M. J., Paciorek C. J., “National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980,” Lancet 378, 31–40 (2011). [DOI] [PubMed] [Google Scholar]
- 3.MacKenzie H. A., Ashton H. S., Spiers S., Shen Y., Freeborn S. S., Hannigan J., Lindberg J., Rae P., “Advances in photoacoustic noninvasive glucose testing,” Clin. Chem. 45(9), 1587–1595 (1999). [PubMed] [Google Scholar]
- 4.Esenaliev R. O., Larin K. V., Larina I. V., Motamedi M., “Noninvasive monitoring of glucose concentration with optical coherence tomography,” Opt. Lett. 26(13), 992–994 (2001). 10.1364/OL.26.000992 [DOI] [PubMed] [Google Scholar]
- 5.Cameron B. D., Li Y., “Polarization-based diffuse reflectance imaging for noninvasive measurement of glucose,” J. Diabetes Sci. Tech. 1(6), 873–878 (2007). 10.1177/193229680700100611 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.CNoga Medical Ltd , http://www.cnoga.com/
- 7.Oculir Inc , http://www.oculir.com/
- 8.Harman-Boehm I., Gal A., Raykhman A. M., Zahn J. D., Naidis E., Mayzel Y., “Noninvasive glucose monitoring: a novel approach,” J. Diabetes Sci. Tech. 3(2), 253–260 (2009). 10.1177/193229680900300205 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Z. Zalevsky, J. Garcia, V. Mico, M. Belkin, Y. Beiderman, I. Margalit and R. Barelly, “Method and system for non-invasively monitoring biological or biochemical parameters of individual,” PCT Application No. PCT/IL2013/050658.
- 10.Shenhav A., Brodie Z., Beiderman Y., Garcia J., Mico V., Zalevsky Z., “Optical sensor for remote estimation of alcohol concentration in blood stream,” Opt. Commun. 289, 149–157 (2013). 10.1016/j.optcom.2012.09.079 [DOI] [Google Scholar]
- 11.Beiderman Y., Horovitz I., Burshtein N., Teicher M., Garcia J., Mico V., Zalevsky Z., “Remote estimation of blood pulse pressure via temporal tracking of reflected secondary speckles pattern,” J. Biomed. Opt. 15(6), 061707 (2010). [DOI] [PubMed] [Google Scholar]
- 12.Beiderman Y., Talyosef R., Yeori D., Garcia J., Mico V., Zalevsky Z., “Use of PC mouse components for continuous measuring of human heartbeat,” Appl. Opt. 51(16), 3323–3328 (2012). 10.1364/AO.51.003323 [DOI] [PubMed] [Google Scholar]
- 13.Beiderman Y., Teicher M., Garcia J., Mico V., Zalevsky Z., “Optical technique for classification, recognition and identification of obscured objects,” Opt. Commun. 283(21), 4274–4282 (2010). 10.1016/j.optcom.2010.06.059 [DOI] [Google Scholar]
- 14.Zalevsky Z., Beiderman Y., Margalit I., Gingold S., Teicher M., Mico V., Garcia J., “Simultaneous remote extraction of multiple speech sources and heart beats from secondary speckles pattern,” Opt. Express 17(24), 21566–21580 (2009). 10.1364/OE.17.021566 [DOI] [PubMed] [Google Scholar]
- 15.Frieser M. J., “A survey of magnetooptic effects,” Magnetics, IEEE Trans 4(2), 152–161 (1968). 10.1109/TMAG.1968.1066210 [DOI] [Google Scholar]
- 16.Anand A., Trivedi V., Mahajan S., Chhaniwal V. K., Zalevsky Z., Javidi B., “Speckle-based optical sensor for low field Faraday rotation measurement,” Sensors Journal, IEEE 13(2), 723–727 (2013). 10.1109/JSEN.2012.2227310 [DOI] [Google Scholar]
- 17.Maughan R. J., Shirreffs S. M., Watson P., “Exercise, heat, hydration and the brain,” J. Am. Coll. Nutr. 26(5), 604S–612S (2007). 10.1080/07315724.2007.10719666 [DOI] [PubMed] [Google Scholar]
- 18.Murray B., “Hydration and physical performance,” J. Am. Coll. Nutr. 26(5), 542S–548S (2007). 10.1080/07315724.2007.10719656 [DOI] [PubMed] [Google Scholar]
- 19.Sawka M. N., Noakes T. D., “Does dehydration impair exercise performance?” Med. Sci. Sports Exerc. 39(8), 1209–1217 (2007). 10.1249/mss.0b013e318124a664 [DOI] [PubMed] [Google Scholar]
- 20.Culp K. R., Wakefield B., Dyck M. J., Cacchione P. Z., DeCrane S., Decker S., “Bioelectrical impedance analysis and other hydration parameters as risk factors for delirium in rural nursing home residents,” J. Gerontol. A Biol. Sci. Med. Sci. 59(8), 813–817 (2004). 10.1093/gerona/59.8.M813 [DOI] [PubMed] [Google Scholar]
- 21.Voyer P., Richard S., Doucet L., Carmichael P. H., “Predisposing factors associated with delirium among demented long-term care residents,” Clin. Nurs. Res. 18(2), 153–171 (2009). 10.1177/1054773809333434 [DOI] [PubMed] [Google Scholar]
- 22.Jéquier E., Constant F., “Water as an essential nutrient: the physiological basis of hydration,” Eur. J. Clin. Nutr. 64(2), 115–123 (2010). 10.1038/ejcn.2009.111 [DOI] [PubMed] [Google Scholar]
- 23.Armstrong L. E., Maresh C. M., Castellani J. W., Bergeron M. F., Kenefick R. W., LaGasse K. E., Riebe D., “Urinary indices of hydration status,” Int. J. Sport Nutr. 4(3), 265–279 (1994). [DOI] [PubMed] [Google Scholar]
- 24.P. A. Uchagaonkar, S. A. Shinde, V. Patil, and R. K. Kamat, “embedded wearable system for hydration measurement,” Int J Phys Mathemat Sci 1,127–131 (2011). http://www.cibtech.org/jpms.htm
- 25.Beiderman Y., Blumenberg R., Rabani N., Teicher M., Garcia J., Mico V., Zalevsky Z., “Demonstration of remote optical measurement configuration that correlates to glucose concentration in blood,” Biomed. Opt. Express 2(4), 858–870 (2011). 10.1364/BOE.2.000858 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.FreeStyle Lite Blood Glucose Monitoring System , https://www.myfreestyle.com/products/freestyle-lite-overview.html?icid=in_footer-product-banner_product-home_freestyle-lite