

Abstract
Objectives:
Various coronally repositioned flap (CRF) techniques have been proposed for coverage of gingival recession defects. Although CRF has several modifications all of them needs vertical or oblique external releasing incisions for treatment of localized gingival recession defects. The aim of present article was to evaluate the effectiveness of a modification of the new CRF procedure without any releasing incision for treatment of shallow localized gingival recession defects.
Conclusion:
Shallow localized gingival recession defects can be treated with modified coronally repositioned flap technique successfully.
Keywords: Coronally repositioned flap, gingival recession, mucogingival surgery
INTRODUCTION
Gingival recession is the exposure of the root surface resulting from migration of the gingival margin apical to the cementoenamel junction. This causes root sensitivity, aesthetic complaints and root surface carious lesions.[1] The treatment of recession defects aims to reduce or eliminate these problems. A lot of surgical techniques, such as laterally positioned flap, coronally repositioned flap, free gingival grafts, have been proposed to obtain root coverage on exposed root surfaces.[2] Among these the coronally repositioned flap (CRF) procedure is a very common approach for root coverage, which is based on the coronal shift of the soft tissues on the exposed root surface.
Miller Class I recession does not extend to the mucogingival junction and there is some keratinized gingiva at the apical of the exposed root. In order to treat Miller Class I recession defects CRF is used as an effective technique and good clinical results have been reported.[3]
Although CRF has several modifications, all of them need vertical or oblique external releasing incisions for treatment of localized gingival recession.[4,5,6] This case series presents the results of a modified CRF technique without any external releasing incision.
MATERIALS AND METHODS
Study population
Seven systemically and periodontally healthy patients (three women and four men) aged between 31 to 46 (mean age 38,8 ± 5,8) with localize buccal recession defects (4 mandibular premolar and three maxillary premolar) were included. The subjects were from the group of patients referred for periodontal treatment to Department of Periodontology, Faculty of Dentistry and Ankara University. Patient selection criteria included: (1) Miller's Class I buccal gingival recession ≥ 1 mm; (2) presence of keratinize gingiva ≥ 1 mm apical to recession; (3) probing depth ≤ 3 mm; (4) no loss of hard and soft tissue in interdental area and (5) tooth vitality and absence of irregularities, caries or restorations in the area to be treated. Written consent form was signed by all patients. The study protocol was approved by the Ethical Committee of Faculty of Dentistry, Ankara University.
Clinical measurements
An individual acrylic stent was prepared for each patient in order to standardize and all clinical measurements were performed by one examiner. The following clinical parameters were measured at baseline (before surgery) and 3rd and 6th m post-surgery: (1) Recession Depth (RD): from cemento-enamel junction (CEJ) to gingival margin (GM) (2) Recession Width (RW): the horizontal dimension of the GM at the level of CEJ; (3) Probing Depth (PD): from GM to apical end of the sulcus; (4) Keratinized Tissue Height (KTH): from GM to muco-gingival junction (MGJ).
RD and RW measurements were taken by Boley gauge (measured accurately to ± 0,1mm). PD and KTH measurements were taken by using periodontal probe (Nordent DURALite ColorRings, USA). Location of MGJ was assessed visually after staining the MGJ with 10% iodine solution (Batticon, Adeka, Ankara, Turkey). All patients were received prophylaxis session including oral hygiene instruction and scaling and professional tooth cleaning with the use of a rubber cup and low abrasive polishing paste.
Surgical procedure
All surgical procedures were performed by one operator. Following local anesthesia (Articain with 1:100,000 epinephrine) an ultrasulculer (intrasulcular) incision was made at the buccal side of the involved tooth and extended to include one tooth on each side of the tooth to facilitate the coronally repositioning of the flap tissue. The intrasulculer incision consist of two oblique submarginal incisions in the interdental areas [Figure 1a and b]. A trapezoidal dissection was made towards apical end of the mucugingival junction and a split thicknes flap was raised without vertical releasing incisions [Figure 1c].
Figure 1.
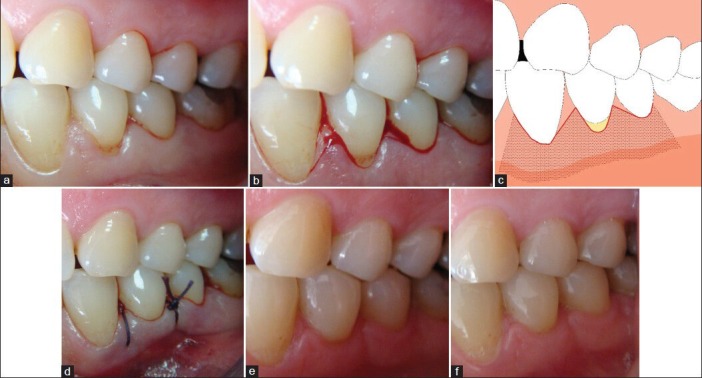
Surgical technique. (a) Preoperative view of left mandibular first premolar, (b) The incision technique, (c) Schematic drawing of the flap, (d) Coronal mobilization and suturing of the flap, (e) Postoperative view at 3rd m, (f) Postoperative view at 6th m
Following this, the papillae adjacent to the involved tooth were de-epithelized. The root surfaces were mechanically treated with the use of currettes. After instrumantation, the rooth surfaces were washed with saline solution. A sling suture, passed from mesial and distal angels of envelope flap, was performed. The suture was tied after the flap was coronally placed and covered the CEJ completely [Figure 1d].
Patients were instructed not to brush their teeth for 14 days in the treated area but to rinse their mouths with chlorhexidine solution (0, 12%). Post-operative pain and edema were controlled with flurbiprophen. Patients received a 100mg tablet for 3 days after operation. Sutures were removed after 14 days and patients were instructed to resume tooth brushing in the operated area. All patients were called for control appointment 3 and 6 month after surgery and the necessary measurements were made [Figure 1e and f] [Figure 2 and 3].
Figure 2.
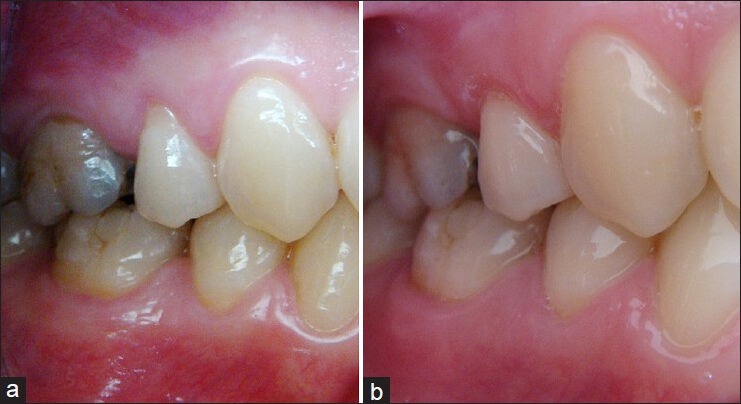
Case 2. (a) Preoperative view of right maxillar first premolar, (b) Postoperative view at 6th m
Figure 3.
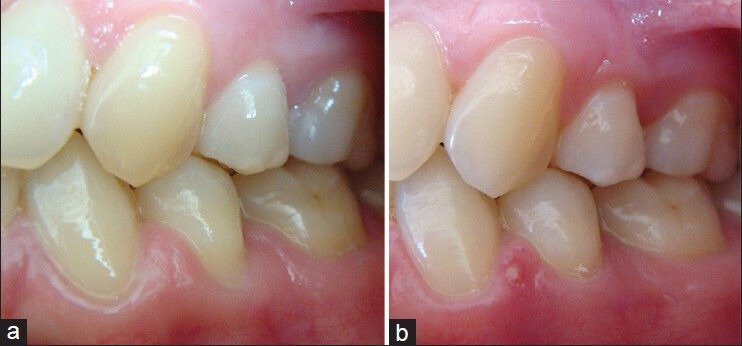
Case 3. (a) Preoperative view of left mandibular first premolar, (b) Postoperative view at 6th m
RESULTS
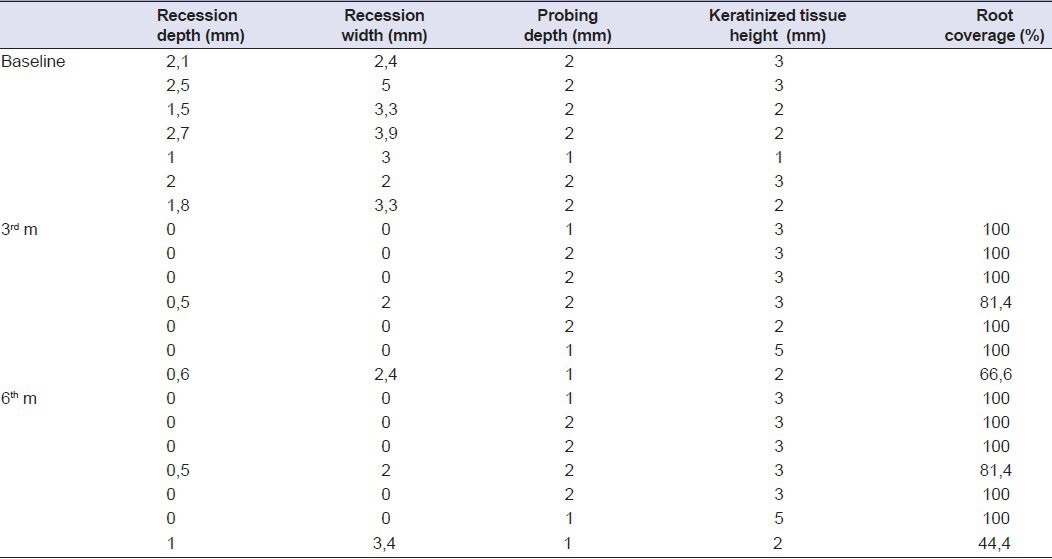
The Table 1 gives the baseline of 3rd and 6th m for the clinical parameters assessed. At baseline the average of the recession depths, recession widths, probing depts and keratinized gingiva heights was 1,94 ± 0,57 mm; 3,27 ± 0,98 mm; 1,85 ± 0,37 mm and 2,28 ± 0,75 mm respectively. The baseline mean of RD 1,94 ± 0,57 mm was reduced to 0,15 ± 0,26 mm at 3rd m and 0,21 ± 0,39 mm at 6th m. The baseline mean of RW 3,27 ± 0,98 mm was reduced to 0,62 ± 1,07 mm at 3rd m and 0,77 ± 1,37 mm at 6th m. Also the baseline mean of PD 1,85 ± 0,37mm was reduced to 1,57 ± 0,33 mm at 3rd m and 1,57 ± 0,53 mm at 6th m. However, the baseline mean of KTH 2,28 ± 0,75 was increased to 3 ± 1 mm at 3rd m and 3,14 ± 0,89 mm at 6th m. Mean root coverage was 92% at 3rd m and 89% at 6th m. Complete root coverage was observed in five patients. Clinical parameters at baseline, 3rd m and 6th m follow-up per patients showed in Table 2.
Table 1.
Comparision of clinical parameters (mean±SD) at different time points

Table 2.
Clinical parameters at baseline, 3rd m and 6th m follow-up
DISCUSSION
Increased aesthetic demands target periodontal plastic surgery to develop new techniques or perform modification of the current techniques. Several surgical procedures have been proposed in the last few years to obtain root coverage on the exposed root surface including coronally positioned flaps, connective tissue grafts, free gingival grafts.[3,7,8] In patients with a residual amount of keratinized tissue apical to the recession defect, the coronally repositioned flap technique may be recommended. Because CRF technique offers many advantages e.g.; optimum root coverage, good color blending.[9,10]
Till today, all of CRF techniques used for the treatment of isolated recession defects except semilunar flap technique described by Tarnow[11] needs vertical releasing incisions. However, in Tarnow's technique, horizontal releasing incision and raising a split thickness flap enables the coronal displacement of the flap.
Raetzke[12] has described “envelope technique” for treatment of localized gingival recession defects. Although this technique does not include vertical releasing incisions, performed together with sub-epithelial connective tissue graft. In the tunnel technique,[13] though it does not include vertical releasing incisions, exposed root surfaces are covered by a sub-epithelial connective tissue graft combined with an envelope flap. This technique is also used for the treatment of multiple recession defects.
These vertical surgical incisions could impair blood supply and the coronal displacement of the flap and sutures could stretch the residual vessels.[14] Contrary to this, the absence of vertical releasing incisions may provide some advantages. Zucchelli and Sanctis[15] suggested a new surgical approach for treatment of multiple recession defects. In this technique, they have made only horizontal incision to design an envelope flap and elevated split-full-split thickness flap. At the end of this study they have reported some clinical and biologic advantages. Blood supply is not damaged, so stability of the surgical margin is achieved and healing is better. Furthermore vertical releasing incision often results in unaesthetic visible scars. Also, absence of these incisions means less suture and so less surgical time which are beneficial for wound healing and patients’ discomfort.
At the classic CRF technique flap is elevated as full thickness. Recently, some investigators have modified this technique. Sanctis and Zucchelli[4] have suggested split-full-split thickness flap elevation with vertical releasing incisions for treatment of isolated recession type defects. They reported that split thickness flap elevation facilitates the nutritional exchanges between surgical papillae and the underlying disepithelized anatomical papillae and improved the blending (in terms of color and thickness) of the surgically treated area with respect to adjacent soft tissues. Raetzke[12] reported minimal surgical trauma at recipient site where preparation consist of an undermining partial thickness incision only, instead of elevation and relocation of full thickness tissue.
In this case series we have suggested a modified coronally repositioned flap technique. In this technique, we have made only intrasulcular incision, continuing to the mesial and distal adjacent teeth, elevated trapezoidal split thickness flap and also used only one sling suture to stabilization of flap. Our technique allows coronally reposition of the flap without vertical releasing incisions at shallow localized gingival recession defect. Therefore, this modified CRF technique is less invasive than classic CRF technique described by Allen and Miller.
CONCLUSION
The results of the present case series demonstrated that the modified CRF technique was effective for treatment of shallow localized gingival recessions. However, long-term new studies are necessary to evaluate the clinical effectiveness of this technique.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared
REFERENCES
- 1.Lucchesi JA, Santos VR, Amaral CM, Peruzzo DC, Duarte PM. Coronally positioned flap for treatment of restored tooth surfaces: A 6-m clinical evaluation. J Periodontol. 2007;78:615–23. doi: 10.1902/jop.2007.060380. [DOI] [PubMed] [Google Scholar]
- 2.Kassab MM, Cohen RE. Treatment of gingival recession. J Am Dent Assoc. 2002;133:1499–506. doi: 10.14219/jada.archive.2002.0080. [DOI] [PubMed] [Google Scholar]
- 3.Allen EP, Miller PD. Coronal positioning of existing gingiva: Short term results in the treatment of shallow marginal tissue recession. J Periodontol. 1989;5:316–9. doi: 10.1902/jop.1989.60.6.316. [DOI] [PubMed] [Google Scholar]
- 4.De Sanctis M, Zucchelli G. Coronally advanced flap: A modified surgical approach for isolated recession type defects. Three-year results. J Clin Periodontol. 2007;34:262–8. doi: 10.1111/j.1600-051X.2006.01039.x. [DOI] [PubMed] [Google Scholar]
- 5.Amarante SE, Leknes KN, Skavland J, Lie T. Coronally positioned flap procedures with or without a bioabsorbable membran in the treatment of human gingival recession. J Periodontol. 2000;71:989–98. doi: 10.1902/jop.2000.71.6.989. [DOI] [PubMed] [Google Scholar]
- 6.Silva RC, Joly JC, Lima AF, Tatakis DN. Root coverage using the coronally positioned flap with or without a subepithelial connective tissue graft. J Periodontol. 2004;75:413–9. doi: 10.1902/jop.2004.75.3.413. [DOI] [PubMed] [Google Scholar]
- 7.Tatiana M, Deliberadora TM, Boscob AF, MArtinsc TM, NAgatab MJ. Treatment of gingival recessions associated to cervical abrasion lesions with subepithelial connective tissue graft: A case report. Eur J Dent. 2009;3:318–23. [PMC free article] [PubMed] [Google Scholar]
- 8.Ustun K, Sarı Z, Orucoglu H, Duran I, Hakkı SS. Severe gingival recession Ccaused by traumatic occlusion and mucogingival stress: A case report. Eur J Dent. 2002;2:127–33. [PMC free article] [PubMed] [Google Scholar]
- 9.Roccuzzo M, Bunino M, Needleman I, Sanz M. Periodontal plastic surgery for treatment of localized gingival recessions: A systematic review. J Clin Periodontol. 2002;29:178–94. doi: 10.1034/j.1600-051x.29.s3.11.x. [DOI] [PubMed] [Google Scholar]
- 10.Harrıs RJ, Harrıs AW. The coronally positioned pedicle graft with inlaid margins: A predictable method of obtaining root coverage of shallow defects. Int J Per Rest Dent. 1994;14:228–41. [PubMed] [Google Scholar]
- 11.Tarnow DP. Semilunar coronally repositioned flap. J Clin Periodontol. 1986;13:182–5. doi: 10.1111/j.1600-051x.1986.tb01456.x. [DOI] [PubMed] [Google Scholar]
- 12.Raetzke PB. Covering localized areas of root exposure employing the ‘envelope’ technique. J Periodontol. 1985;56:397–402. doi: 10.1902/jop.1985.56.7.397. [DOI] [PubMed] [Google Scholar]
- 13.Zabalegui I, Sicilia A, Cambra J, Gil J, Sanz M. Treatment of multiple adjacent gingival recessions with the tunnel subepithelial connective tissue graft: A clinical report. Int J Periodontics Restorative Dent. 1999;19:199–206. [PubMed] [Google Scholar]
- 14.Baldi C, Pini Prato G, Paqliaro U, Nieri M, Saletta D, Muzzi L, Cortellini P. Coronally advanced flap procedure for root coverage. Is flap thickness a relevant predictor to achieve root coverage?. A case series. J Periodontol. 1999;70:1077–84. doi: 10.1902/jop.1999.70.9.1077. [DOI] [PubMed] [Google Scholar]
- 15.Zucchelli G, Santics M. Treatment of multiple Recession type defects in patients with esthetic demands. J Periodontol. 2000;71:1506–14. doi: 10.1902/jop.2000.71.9.1506. [DOI] [PubMed] [Google Scholar]