

Abstract
Objectives:
To conduct a prospective randomized study comparing the efficiency of 5 different ligation systems (ELL; elastomeric ligature, SSL; stainless steel ligature, LL; leone slide ligature, PSL; passive self-ligation and ASL; active self-ligation) over the duration of mandibular crowding alleviation.
Materials and Methods:
Fifty consecutive patients (54.2% male, 45.8% female; mean age: 16.69 years) satisfying the inclusion criteria were randomly allocated to 5 ligation groups with an equal sample size of 10 per group. The 5 groups received treatment with 0.022-inch MBT pre-adjusted edge-wise technique (ELL: Gemini 3M Unitek, SSL: Gemini 3M Unitek, LL: Gemini 3M Unitek, PSL: SmartClip 3M Unitek and ASL: In-Ovation R Euro GAC International). The models and cephalograms were evaluated for anterior arch alignment, extraction space closure, and lower incisal inclinations at pre-treatment T1 and at the end of initial alignment T2. Analysis of variance (ANOVA) and Post-hoc tests were used for data analysis.
Results:
Forty-eight participants completed the study, and SL systems showed a significant difference over CL groups in time to alignment, passive space closure, and incisal inclination. Multiple regression showed a reduction of 5.28 days in time to alignment by changing the ligation group in the order of ELL to ASL group and 1 mm increase in initial irregularity index increases time to alignment by 11.68 days.
Conclusion:
Self-ligation brackets were more efficient than conventional ligation brackets during initial leveling and alignment.
Keywords: Conventional, crowding, friction, leone ligatures, ligation, self-ligation
INTRODUCTION
Important factors determining the rate of tooth alignment include the bracket slot dimension, the associated inter bracket span, the choice of arch wire,[1,2,3,4] and frictional forces generated between bracket and arch wire. Friction has been defined as the resistance to motion that occurs when two objects move tangentially to each other.[5]
Friction, which impedes sliding movements, is determined by multiplying the coefficient of friction of the materials in contact by the normal force, which is the force of ligation in orthodontic appliance. Therefore, friction is directly proportional to the force of ligation.[6] An ideal ligation system for alleviation of crowding in orthodontic treatment primarily should ensure full bracket engagement of the arch wire and should exhibit low friction between brackets and arch wire.[7] Currently, two main types of brackets are available for practicing orthodontists-conventional (CL) and self-ligating (SL) brackets. In a conventional tie wing bracket, wire ligatures and elastomeric ligatures have been documented with higher frictional forces, which reach undesirable levels relative to those that are ideal for tooth movement.[8] SL brackets are considered a ligature-less bracket system with an inbuilt metal labial face, which provides the combination of low friction and full arch wire engagement. Two types of SL brackets have been developed: Active and Passive.[9,10]
The claimed advantages of both types of SL bracket systems include increased patient comfort due to the absence of ligatures, improved oral hygiene, less chair time, and shorter overall treatment time.[5] However, there are also certain disadvantages, including difficulty with the full expression of torque, frequent failure of the clips, and brackets that are bulkier and more expensive than conventional brackets.
To address some deficiencies of SL brackets, novel ligatures such as the Leone slide ligature (LL) have recently been developed. Leone slide ligatures (LL) have been developed with a polyurethane fourth wall, which allows the arch wire to slide freely in the slot while transmitting its full force to the tooth.
Several retrospective[11,12,13] and prospective[14,15,16,17,18,19,20,21,22,23] in-vivo studies have compared the efficiency of SL and CL brackets during various stages of treatment, reporting no significant differences during initial alignment. Miles et al.[19] and Miles et al.[21] did not find any significant differences when they prospectively compared Damon SL, Smart Clip (3M Unitek) SL with Victory Series CL brackets during initial alignment. Pandis et al.[14] also found no difference when comparing time to alignment in the mandibular arch between Damon 2 (Ormco) SL and Microarch (GAC international) CL brackets. A retrospective study by Hamilton[11] comparing In-Ovation (GAC) SL brackets and Victory Series CL brackets found no measurable difference in initial alignment time.
The above-said studies were based on non-extraction treatment plan and lack the evidence about the benefits of SL brackets for extraction patients during initial alignment. Scott et al.[22] conducted a randomized controlled trial of patients having mandibular first premolar extractions and concluded Damon 3MX SL brackets were no more efficient than Synthesis (Ormco) CL brackets during mandibular alignment. Ong et al.[24] compared efficiency of Damon 3MX SL brackets and Victory Series (3M Unitek) CL brackets for anterior arch alignment and passive space closure and found no significant difference between SL and CL groups. Early retrospective studies[11,12,13] include the possibility of outcome bias and subsequent prospective[14,15,16,17,18,19,20,21,22,23] clinical trials had the effect of confounding factors, such as various malocclusions treated with many modalities and methods,[14,15,16,17,18] lack of testing for the equivalence pre-treatment characteristics of the sample,[14,15,16,17,18] ill-defined selection criteria and variability with respect to arch wire sequences,[14,16] and bracket types[11,14,16,18,22] among the groups.
To date, there is little robust clinical evidence in the form of a well-designed prospective randomized clinical trial with adequate control over clinical variables: (bracket composition, dimension, arch wire type and sequence, inter-appointment interval and treatment plan), comparing the efficacy of the 5 available modes of ligation over treatment time to alignment, passive space closure, and changes in mandibular incisal inclination at the end of first phase of fixed appliance therapy.
Hence, the purpose of this prospective randomized clinical trial was to compare the efficacy of 5 ligation modes, Elastomeric ligation (EL), Stainless steel ligation (SSL), Leone slide Ligation (LL), Passive self-ligation (PSL), and Active self-ligation (ASL). The primary outcome measure was rapidity of tooth alignment, and secondary outcome measures were passive space closure and changes in the mandibular incisal inclination.
MATERIALS AND METHODS
Ethical approval for the study was obtained from the Institutional Ethical committee (No. 22/94/11). The participants and their parents or guardians were informed of the study, its implications, and written consent was received from all. A randomized prospective clinical trial design was opted. The subjects were recruited from consecutive patients attending the Orthodontic Department between January 2011 and February 2012 and satisfied the inclusion criteria.
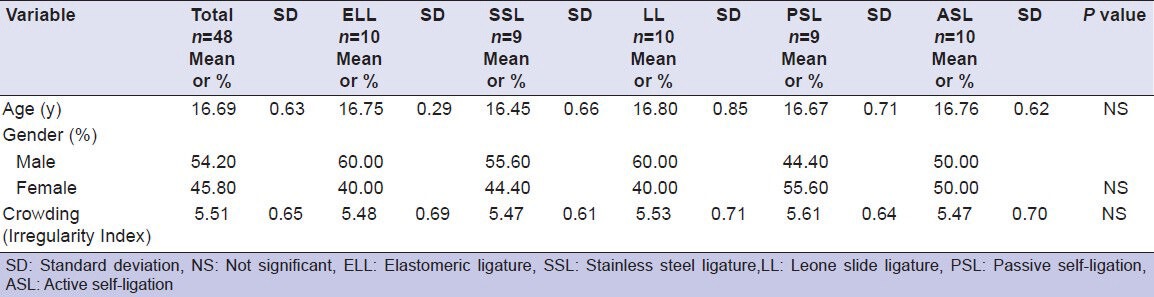
Fifty patients (23 males, 27 females) fulfilled the inclusion criteria. Their demographics are shown in Table 1. The subjects were randomly allocated for treatment with Elastomeric ligation (ELL), Stainless steel Ligation (SSL), Leone slide Ligatures (LL), Passive self-ligation (PSL), and Active self-ligation (ASL) brackets using unstratified subject allocation sequence made using a computer-generated randomization program done by a statistician independent from the study (http://www.randomization.com). Numbered opaque sealed envelopes containing the treatment allocation card were prepared by the statistician before the trial commencement. After the satisfaction of inclusion criteria and consent obtained from the subjects, the successive subjects were handed over the sealed envelopes by the secretary of the department, in order to conceal the assignments from the clinician until the appointment at which the appliance was to be placed.
Table 1.
Demographic and clinical characteristics of sample
A Post-Hoc sample size calculation with α = 0.05 and power = 80% reveals, a sample of 10 subjects per ligation group could be justified as a median sample size.
The bracket systems used were 0.022 slot MBT (Gemini series, 3M Unitek) for EL, SSL, LL and 0.022 slot MBT (Smart clip, 3M Unitek) for PSL, and 0.022 slot MBT (In-Ovation Euro, Dentsply GAC, USA) for ASL. Two operators treated the patients in all the 5 groups, and the bonding method was standardized between the groups using conventional etching and Transbond (3M Unitek) bracket adhesive.
The archwire sequence for the 5 groups was 0.014-inch, 0.016-inch and 0.016 × 0.022-inch copper-Ni-Ti (Cu-Ni-Ti) 35°C and 0.016 × 0.022-inch Stainless steel (Ormco; True-arch form) working wire in place for 1 month. The patients were reviewed every 6 weeks, and the first arch wire was left in place until the teeth were passively engaged in all the bracket slots before proceeding to the second arch wire. In bracket systems ligated with elastomeric modules, the arch wires were occasionally ligated with elastomeric in figure ‘8’configuration to permit bracket engagement in areas of marked irregularity.
Anchorage augmentation procedures like TPA in the upper arch and lower lingual arch were placed in all the patients at the initial appointment of appliance placement and were carried on to the retraction phase of mechanotherapy. Passive lace backs were placed in both the quadrants from the power arm of first molar to the canines in a figure ‘8’ fashion in all the groups. The distal ends of all the wires were cinched distal to the first molar tube. Active tie backs were placed when necessary.[25]
Pre-treatment characteristics were recorded including patient age, gender, sex, lower incisal irregularity index, lower first premolar extraction space, and lower incisal inclination. Pre-treatment study models were evaluated by using Little's irregularity index[26] to quantify the alignment of 6 mandibular anterior teeth. Mandibular dental casts and lateral cephalograms were taken at appliance placement (T1) and on the alignment date (T2) when the patient was considered complete after 1 month of working 0.016 × 0.022 stainless steel archwires and upon visual inspection of the correction of proximal contacts.
The time to alignment (T2 - T1) was calculated for each patient in days. Extraction space (T1) was measured from the closest points on the adjacent teeth before extraction. The mesiodistal widths of the teeth to be extracted were not used because they were often displaced from the arch form; this decreased the extraction space to be closed. Similarly, extraction spaces at (T2) were measured from the closest points on the crowns of the teeth on either side of the extraction space.
Coded lateral cephalograms were traced, and mandibular incisal inclination was assessed for all patients at T1 and T2 using the angular measurement: Mandibular incisor to mandibular plane. Each patient model was numbered for identification. Wax was applied to cover the bracket on each model before measurement. Therefore, the researcher was blinded to patient's name, the ligation type during data collection to minimize systematic error. The study models were measured with digital calipers (Digimatic NTD 12-6”C, Mitutoyo Corp, Tokyo, Japan). All model and cephalometric measurements were measured by the researcher.
To assess the intra-examiner reliability, 15 plaster models and 15 cephalometric radiographs were randomly selected from the records. The cephalometric radiographs were retraced, and the measurements of the cephalometric variables were repeated. In the dental casts, the extraction spaces were re-measured. The reproducibility of the measurements was investigated with Intra-class Correlation Coefficient (ICC). The analysis showed no significant difference between the first and second measurements (ICC = 0.96).
Statistical analysis
Demographic and clinical characteristics were investigated with conventional descriptive statistics. Before performing the test of significance, normality assumptions were tested by Kolmogorov-Smirnov and Shapiro-Wilk test. ANOVA was performed for normally distributed variables, and non-parametric tests (Chi-square and Kruskal-Wallis) were used for non-normally distributed variables. Comparison between 5 ligation groups with respect to the treatment duration, passive space closure, and change in the mandibular incisal inclination was investigated by ANOVA followed by Post-Hoc Bonferroni analysis. Correlations as well as partial correlations for time to alignment as the dependent variable and other independent variables were calculated followed by a stepwise regression analysis. The statistical analyses were performed with SPSS software (release, 11.0, SPSS for windows, SPSS Chicago, III).
RESULTS
Figure 1 is the consort flow chart. Fifty subjects were recruited for the study and of them, 48 subjects completed the study and those who failed to complete the treatment were omitted from the statistical analysis (Per-Protocol Analysis). Baseline demographic and clinical characteristics for the 5 groups showed no discrimination with respect to age, gender, irregularity index, thus validating the random assignment of ligation methods to the 5 groups [Table 1].
Figure 1.
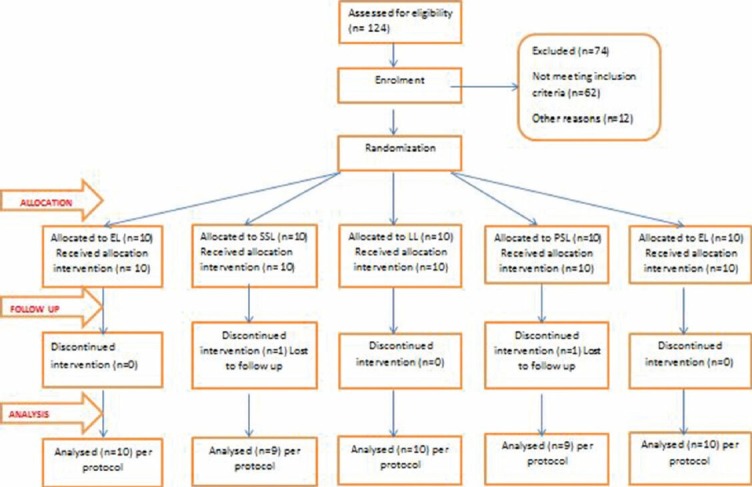
Consort flow chart
The mean duration of treatment time to alignment was 161.19 days overall: 176.30 days in the ELL group, 175.56 days in the SSL group, 159.10 days in the LL group, 152.67 days in the PSL group, and 142.90 days in the ASL group [Table 2]. ANOVA was used to compare the mean treatment time to alignment between 5 ligation systems followed by Post-hoc analysis. A statistically significant difference was found between all the groups, except for ELL vs.. SSL, LL vs.. PSL, and PSL vs.. ASL [Table 3]. Table 4 shows the mean passive space closure in each ligation group with 2.90 mm overall: 2.00 mm in ELL, 2.09 mm in SSL, 3.06 mm in LL, 3.50 mm in PSL, and 3.85 mm in ASL. Inferential statistical investigation showed a significant difference between all the groups, except for ELL vs.. SSL, LL vs.. PSL, and PSL vs.. ASL [Table 5].
Table 2.
Mean treatment time to alignment by ligation group
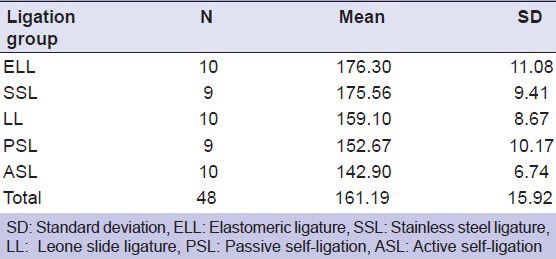
Table 3.
Comparison of mean treatment time to alignment between ligation systems
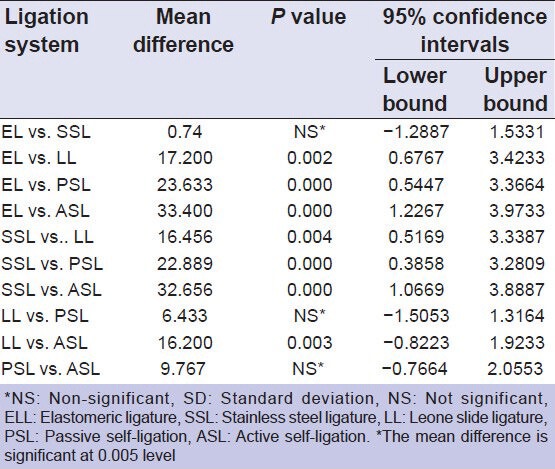
Table 4.
Mean change in the passive space closure by ligation group in millimeters
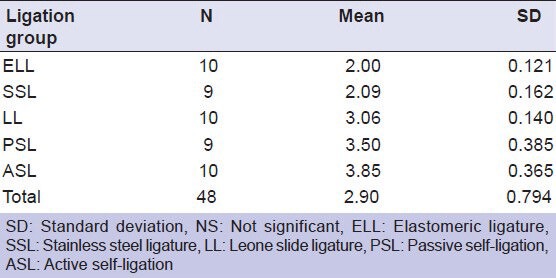
Table 5.
Comparison of the passive space closure between ligation groups
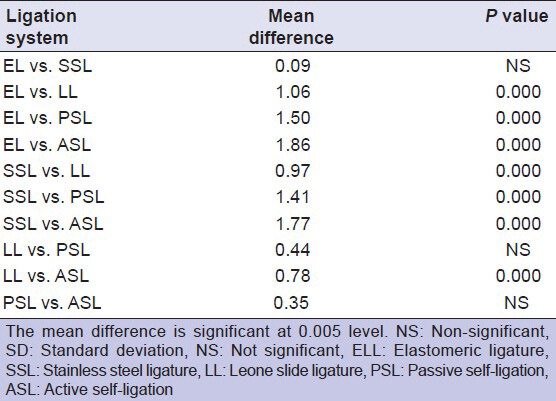
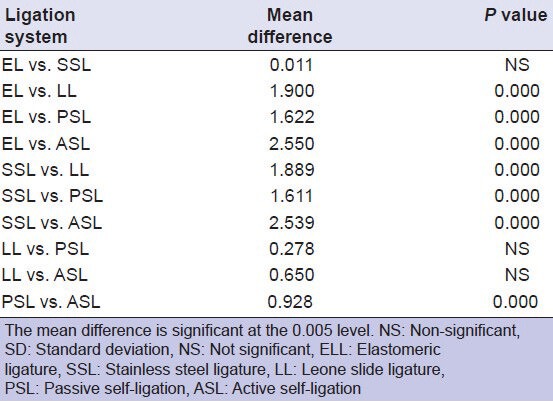
Table 6 shows the mean change in mandibular incisal inclination in each ligation group with 3.17° overall: 4.40° in ELL, 4.39° in SSL, 2.50° in LL, 2.78° in PSL, and 1.85° in ASL. Inferential statistical investigation showed a significant difference between all the groups, except for ELL vs.. SSL and LL vs.. PSL [Table 7].
Table 6.
Mean change in the mandibular incisal inclination by ligation group in degrees
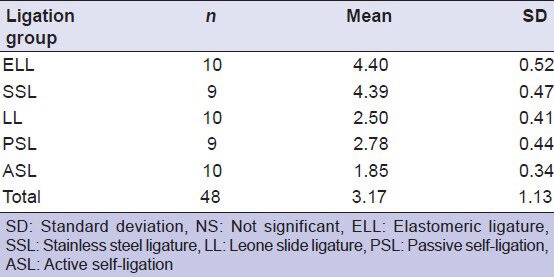
Table 7.
Comparison of change in the mandibular incisal inclination between ligation groups
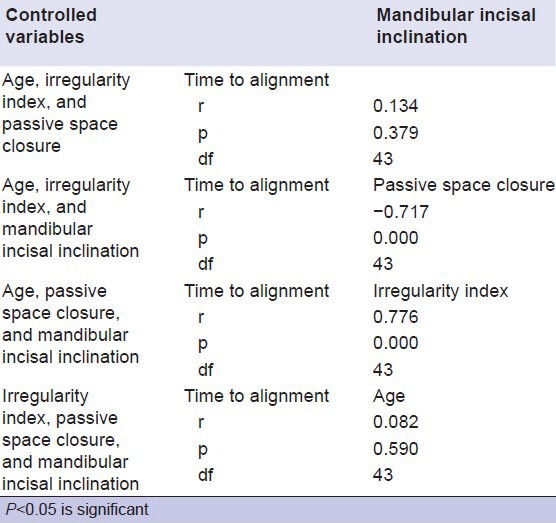
Pearson correlation coefficient for time to alignment, change in mandibular incisal inclination, passive space closure and irregularity index are 0.72, -0.839, and 0.457, respectively. All these correlation coefficients are significant (P < 0.01) [Table 8]. Correlation matrix indicates that the time to alignment is positively correlated with change in mandibular incisal inclination and irregularity index, while passive space closure and time to alignment are negatively correlated. However, these simple correlations are not controlled for the other directly related variables. Hence, partial correlations were calculated. Partial correlation of time to alignment with change in mandibular incisal inclination, passive space closure is significant (P < 0.05), and the partial correlation of time to alignment with age and change in mandibular incisal inclination is not significant [Table 9].
Table 8.
Pearson correlation coefficients
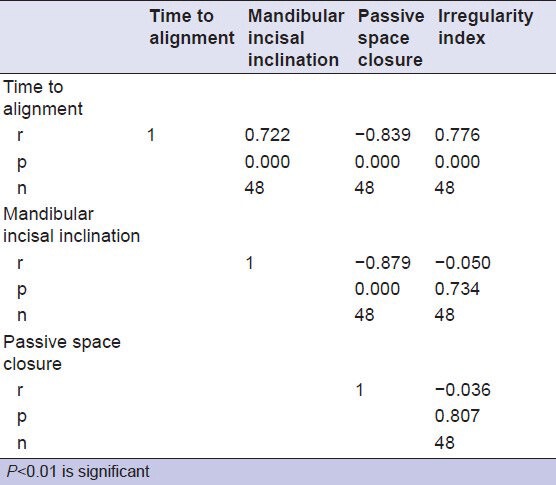
Table 9.
Partial correlation coefficients
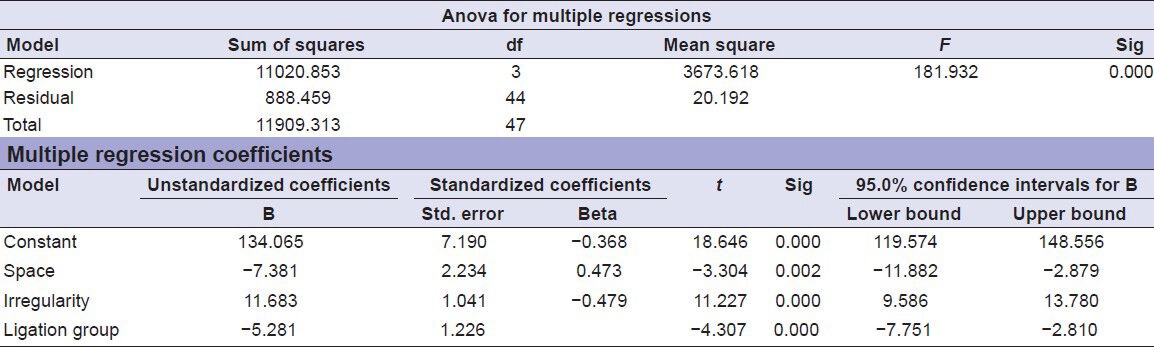
Multiple regression analysis was done to alignment as dependent variable, age, irregularity index, change in mandibular incisal inclination, and passive space closure as independent variables. The stepwise regression analysis gave an ‘R’ square value of 0.925, indicating that this linear model explained 93% of variability in time to alignment as influenced by the independent variables. The ANOVA indicated that the dependent and independent variables are having a linear relation and the linearity is significant. The final linear model included passive space closure, irregularity index, and mode of ligation as significantly contributing variables in deciding the time taken for alignment while age and change in mandibular incisal inclination were identified as non-significant variables, hence were excluded from the regression model. The final regression equation is:
Time to alignment = 134.07 - (7.38 × passive space closure) + (11.68 × Irregularity index) - (5.28 × ligation group).
The model shows that 1 mm of passive space closure contributes to 7.38 days reduction in time to alignment when irregularity index and ligation group are fixed variables, 1 mm increase in the irregularity index increases the time to alignment by 11.67 days by keeping the passive space and ligation groups as fixed variables. There will be a reduction of 5.28 days in time to alignment if the ligation groups are changed in the order from ELL to ASL per each group when passive space closure and irregularity are held constant [Table 10].
Table 10.
Multiple regression analysis
DISCUSSION
Our study is the first to simultaneously quantify, relate, and compare time to alignment, passive space closure, and change in the mandibular incisal inclination between 5 different ligation systems.
The results of this study suggest that SL groups (PSL, ASL) were more efficient than CL groups (EL, SSL) in terms of treatment time to alignment. The results of this study emphasize the clinical relevance of the in-vitro assessment of frictional protocols in many studies[27,28,29,30,31,32,33,34] during the past decade, which has often demonstrated a significant decrease in friction with SL systems compared with CL brackets designs, which is highly desirable during the initial alignment phase. This observation could be attributed to the substantial greater free play of the SL appliances in contrast to the conventional ligatures that act as obstacles because of the stress they exert on the arch wire adjacent to the bracket sides, precluding the free sliding of the wire into the slot walls, thus reducing the rate of tooth movement. Our findings have demonstrated ASL performing better than the PSL system with respect to the treatment time to alignment, but the difference was statistically insignificant. The possible explanation behind this observation could be due to the storage of some of the force in the active clip as well as in the wire with ASL brackets, which means a given wire will have its range of labiolingual action increased and, therefore, produce more alignment than would a passive slide with the same wire. In sufficiently lingually placed tooth with an active spring clip in relation to its neighboring teeth, a higher total force will usually be applied to the tooth in comparison to a passive clip. But, such force is unlikely to be detrimental with modern low modulus wires since several studies[7] have shown that only large deflections are likely to enable a superelastic wire to show a plateau of force for a range of deflection, which is unlikely to happen with passive self-ligation.
LL group was significantly more efficient from the CL group but was comparably inferior to the ASL group in terms of treatment time to alignment. The results are in accordance with an in-vitro study[35] in the past, which states that SL systems and Leone slide ligatures on conventional brackets produce significantly lower frictional forces compared with conventional ligatures.
Passive space closure, incisal proclination, and dental arch expansion have been considered as contributing factors for alleviation of crowding during orthodontic arch alignment.[36] However, studies have reported intentional development of the arch width, with appliance systems has been found to be highly unpredictable.[37,38] Hence, we, in our study, have abstained from evaluating the transverse arch dimensions.
The present study reflected a significant advantage of SL systems over CL systems with respect to passive space closure with less extraction space to close actively in SL category, which could eventually reduce the overall treatment time. The results demonstrate an identical performance between LL and PSL groups, PSL and ASL groups, while the ASL groups had significantly increased passive space closure in comparison to LL groups. The results concur with a previous study,[22] which suggested that SL brackets might encourage passive space closure during initial alignment. However, Ong et al.,[24] in their study found no difference in the amount of passive space closure during initial alignment between the bracket types.
Mandibular incisal inclination during initial alignment was significantly influenced by the bracket system with SL brackets resulting in significantly lesser incisal proclination. The results suggest that CL appliances resolve crowding more through an incisal proclination while SL brackets relieve crowding by facilitating more passive space closure. This phenomenon with SL brackets would help in preventing the torque loss during the initial alignment, prevent round tripping of the anterior teeth, thus minimizing root resorption and would greatly minimize the net effective anchorage loss during the overall treatment time of an individual.
To summarize, SL systems (PSL, ASL) had a significant measurable advantage over CL systems (ELL, SSL) with respect to the three variables: (a) reduction in treatment time to alignment, (b) increased passive space closure, and (c) decrease in incisal proclination. LL system was comparatively beneficial over CL systems but inferior to ASL systems and with an insignificant difference from PSL systems. The study showed an insignificant difference in the clinical performance between ELL, SSL in conventional, while ASL performed significantly superior to PSL system in SL groups.
The results of our study, however, differ with previous studies[14,15,19,21,22,24] in the rapidity of alignment, amount of passive space closure, and mandibular incisal inclination. The difference could be explained by the variability of bracket designs utilized in SL and CL appliances with their characteristic prescriptions, variability in arch form, arch wire sequence, and final working arch wires. Certain studies[14,16,19,22,24] have compared Damon2, Damon3 PSL brackets with a 0.019 × 0.025-inch working stainless steel arch wire to CL systems with MBT prescription (Victory Series, 3M Unitek). A thicker wire of 0.019 × 0.025-inch is likely to completely fill the slot contributing to an increase in friction as well as torque effectiveness, thereby increasing the time to alignment with SL systems when the arch wire sequence is carried on till the 0.019 × 0.025-inch stainless steel working arch wire. In studies[14] that had 0.014 × 0.025-inch copper-nickel-titanium Damon arch form wherein measurements are taken, the lack of significant difference could be attributed to the high torque version of Damon MX that increases the frictional resistance at the bracket slot arch wire interface. In addition, narrower bracket design of Damon 3MX can increase the contact angle and contribute to elastic binding and notching with wires of higher dimension and stiffness. In our study, we have standardized MBT prescription, arch forms, and arch sequence to all the 5 ligation groups with measurements taken at the end of a 0.016 × 0.022-inch stainless steel working arch wire. A 0.016 × 0.022-inch wire would create a slop of 0.005-inch, which reduces the frictional resistance in all the ligation groups and thereby could enhance the alignment efficiency of active spring clip and passive SL systems through a more passive space closure and lesser incisal inclination. For majority of bracket arch wire combinations, the friction values obtained were significantly higher than with only the terminal brackets ligated, confirming that ligation plays an important role in generating friction.[39,40]
The strength of the study was standardization of clinical variables such as bracket composition, dimension, prescription, arch wire type, arch wire sequence, inter-appointment intervals, category of dento-alveolar malocclusion and extraction pattern. Consecutive eligible patients were included to minimize confounding variables with method of ligation being the critical difference between treatment groups. Despite the strict inclusion, exclusion criteria, and standardization of the clinical variables, a major limitation with the study is the sampling bias with a low initial sample size recruited into the study although lost to follow up was minimal. The aim of a randomized clinical trial is to provide an unbiased assessment of the effects of a treatment intervention. A small sample size could eventually lead to a random error that can arise when the results of the clinical trial could be different from the truth. In small trials, the probability of reporting a clinically important effect due to chance is relatively higher and the effects of random error on the estimates decreases as the trial becomes larger. Hence, a similar study with a larger sample size is needed in future to minimize the random error that could be associated with the present study. The results of this RCT suggest that clinicians can appreciate the effectiveness of SL systems when used with undersized wires. This situation, however, could be negated as treatment progresses and wires of higher dimension and stiffness are engaged in the brackets. Treatment efficiency is the product of many mechanical and biological factors. Along with individual biological variation, bracket type can significantly influence the treatment efficiency and overall treatment span in orthodontic mechanotherapy.
CONCLUSION
Self-ligating brackets were more efficient than conventional brackets in anterior alignment, passive space closure, and mandibular incisal inclination during initial phase of orthodontic treatment.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared
REFERENCES
- 1.Cobb NW, 3rd, Kula KS, Phillips C, Proffit WR. Efficiency of multi-strand steel, superelastic Ni-Ti and ion-implanted Ni-Ti archwires for initial alignment. Clin Orthod Res. 1998;1:12–9. doi: 10.1111/ocr.1998.1.1.12. [DOI] [PubMed] [Google Scholar]
- 2.Evans TJ, Jones ML, Newcombe RG. Clinical comparison and performance perspective of three aligning arch wires. Am J Orthod Dentofacial Orthop. 1998;114:32–9. doi: 10.1016/s0889-5406(98)70234-3. [DOI] [PubMed] [Google Scholar]
- 3.O’Brien K, Lewis D, Shaw W, Combe E. A clinical trial of aligning archwires. Eur J Orthod. 1990;12:380–4. doi: 10.1093/ejo/12.4.380. [DOI] [PubMed] [Google Scholar]
- 4.West AE, Jones ML, Newcombe RG. Multiflex versus superelastic: A randomized clinical trial of the tooth alignment ability of initial arch wires. Am J Orthod Dentofacial Orthop. 1995;108:464–71. doi: 10.1016/s0889-5406(95)70046-3. [DOI] [PubMed] [Google Scholar]
- 5.Tecco S, Festa F, Caputi S, Traini T, Di Iorio D, D’Attilio M. Friction of conventional and self-ligating brackets using a 10 bracket model. Angle Orthod. 2005;75:1041–5. doi: 10.1043/0003-3219(2005)75[1041:FOCASB]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 6.Rinchuse DJ, Miles PG. Self-ligating brackets: Present and future. Am J Orthod Dentofacial Orthop. 2007;132:216–22. doi: 10.1016/j.ajodo.2006.06.018. [DOI] [PubMed] [Google Scholar]
- 7.Harradine NW. Self-ligating brackets: Where are we now? J Orthod. 2003;30:262–73. doi: 10.1093/ortho/30.3.262. [DOI] [PubMed] [Google Scholar]
- 8.Shivapuja PK, Berger J. A comparative study of conventional ligation and self-ligation bracket systems. Am J Orthod Dentofacial Orthop. 1994;106:472–80. doi: 10.1016/S0889-5406(94)70069-9. [DOI] [PubMed] [Google Scholar]
- 9.Thomas S, Sherriff M, Birnie D. A comparative in vitro study of the frictional characteristics of two types of self-ligating brackets and two types of pre-adjusted edgewise brackets tied with elastomeric ligatures. Eur J Orthod. 1998;20:589–96. doi: 10.1093/ejo/20.5.589. [DOI] [PubMed] [Google Scholar]
- 10.Franchi L, Baccetti T, Camporesi M, Barbato E. Forces released during sliding mechanics with passive self-ligating brackets or nonconventional elastomeric ligatures. Am J Orthod Dentofacial Orthop. 2008;133:87–90. doi: 10.1016/j.ajodo.2007.08.011. [DOI] [PubMed] [Google Scholar]
- 11.Hamilton R, Goonewardene MS, Murray K. Comparision of active self-ligating brackets and conventional pre-adjusted brackets. Aust Orthod J. 2008;24:102–9. [PubMed] [Google Scholar]
- 12.Eberting JJ, Straja SR, Tuncay OC. Treatment time, outcome, and patient satisfaction comparisons of Damon and conventional brackets. Clin Orthod Res. 2001;4:228–34. doi: 10.1034/j.1600-0544.2001.40407.x. [DOI] [PubMed] [Google Scholar]
- 13.Harradine NW. Self-ligating brackets and treatment efficiency. Clin Orthod Res. 2001;4:220–7. doi: 10.1034/j.1600-0544.2001.40406.x. [DOI] [PubMed] [Google Scholar]
- 14.Pandis N, Polychronopoulou A, Eliades T. Self-ligating vs. conventional brackets in the treatment of mandibular crowding: A prospective clinical trial of treatment duration and dental effects. Am J Orthod Dentofacial Orthop. 2007;132:208–15. doi: 10.1016/j.ajodo.2006.01.030. [DOI] [PubMed] [Google Scholar]
- 15.Fleming PS, DiBiase AT, Sarri G, Lee RT. Efficiency of mandibular arch alignment with 2 preadjusted edgewise appliances. Am J Orthod Dentofacial Orthop. 2009;135:597–602. doi: 10.1016/j.ajodo.2007.06.014. [DOI] [PubMed] [Google Scholar]
- 16.Pandis N, Polychronopoulou A, Makou M, Eliades T. Mandibular dental arch changes associated with treatment of crowding using self-ligating and conventional brackets. Eur J Orthod. 2010;32:248–53. doi: 10.1093/ejo/cjp123. [DOI] [PubMed] [Google Scholar]
- 17.Fleming PS, DiBiase AT, Lee RT. Randomized clinical trial of orthodontic treatment efficiency with self-ligating and conventional fixed orthodontic appliances. Am J Orthod Dentofacial Orthop. 2010;137:738–42. doi: 10.1016/j.ajodo.2009.06.023. [DOI] [PubMed] [Google Scholar]
- 18.DiBiase AT, Nasr IH, Scott P, Cobourne MT. Duration of treatment and occlusal outcome using Damon3 self-ligated and conventional orthodontic bracket systems in extraction patients: A prospective randomized clinical trial. Am J Orthod Dentofacial Orthop. 2011;139:e111–6. doi: 10.1016/j.ajodo.2010.07.020. [DOI] [PubMed] [Google Scholar]
- 19.Miles PG, Weyant RJ, Rustveld L. A clinical trial of Damon 2 vs. conventional twin brackets during initial alignment. Angle Orthod. 2006;76:480–5. doi: 10.1043/0003-3219(2006)076[0480:ACTODV]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 20.Miles PG. Self-ligating vs. conventional twin brackets during en-masse space closure with sliding mechanics. Am J Orthod Dentofacial Orthop. 2007;132:223–5. doi: 10.1016/j.ajodo.2007.04.028. [DOI] [PubMed] [Google Scholar]
- 21.Miles PG. SmartClip versus conventional twin brackets for initial alignment: Is there a difference. Aust Orthod J. 2005;21:123–7. [PubMed] [Google Scholar]
- 22.Scott P, DiBiase AT, Sherriff M, Cobourne M. Alignment efficiency of Damon3 self-ligating and conventional orthodontic bracket systems: A randomized clinical trial. Am J Orthod Dentofacial Orthop. 2008;134:470.e1–8. doi: 10.1016/j.ajodo.2008.04.018. [DOI] [PubMed] [Google Scholar]
- 23.Johansson K, Lundström F. Orthodontic treatment efficiency with self-ligating and conventional edgewise twin brackets. A prospective randomized clinical trial. Angle Orthod. 2012;82:929–34. doi: 10.2319/101911-653.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ong E, McCallum H, Griffin MP, Ho C. Efficiency of self-ligating vs. conventional ligated brackets during initial alignment. Am J Orthod Dentofacial Orthop. 2010;138:138.e1–7. doi: 10.1016/j.ajodo.2010.03.020. [DOI] [PubMed] [Google Scholar]
- 25.McLaughlin RP, Bennett JC, Trevisi HJ. Edinburgh: Mosby; 2001. Systemised Orthodontic Treatment Mechanics; pp. 101–2. [Google Scholar]
- 26.Little RM. The irregularity index: A quantitative score of mandibular anterior alignment. Am J Orthod. 1975;68:554–63. doi: 10.1016/0002-9416(75)90086-x. [DOI] [PubMed] [Google Scholar]
- 27.Berger JL. The influence of SPEED bracket's self-ligating design on force levels in tooth movement: A comparative in-vitro study. Am J Orthod Dentofacial Orthop. 1990;97:219–28. doi: 10.1016/S0889-5406(05)80055-1. [DOI] [PubMed] [Google Scholar]
- 28.Sims AP, Waters NE, Birnie DJ, Pethybridge RJ. A comparison of the forces required to produce tooth movement in-vitro using two self-ligating brackets and a pre-adjusted bracket employing two types of ligation. Eur J Orthod. 1993;15:377–85. doi: 10.1093/ejo/15.5.377. [DOI] [PubMed] [Google Scholar]
- 29.Sims AP, Waters NE, Birnie DJ. A comparison of the forces required to produce tooth movement exvivo through three types of pre-adjusted brackets when subjected to determined tip or torque values. Br J Orthod. 1994;21:367–73. doi: 10.1179/bjo.21.4.367. [DOI] [PubMed] [Google Scholar]
- 30.Read-Ward GE, Jones SP, Davies EH. A comparision of self-ligating and conventional orthodontic bracket systems. Br J Orthod. 1997;24:309–17. doi: 10.1093/ortho/24.4.309. [DOI] [PubMed] [Google Scholar]
- 31.Thomas S, Sheriff M, Birnie D. A comparative in-vitro study of the frictional characteristics of two types of self-ligating brackets and two types of pre-adjusted edgewise brackets tied with elastomeric ligatures. Eur J Orthod. 1998;20:589–96. doi: 10.1093/ejo/20.5.589. [DOI] [PubMed] [Google Scholar]
- 32.Thorstenson GA, Kusy RP. Resistance to sliding of self-ligating brackets versus conventional stainless steel twin brackets with second-order angulations in the dry and wet (saliva) states. Am J Orthod Dentofacial Orthop. 2001;120:361–70. doi: 10.1067/mod.2001.116090. [DOI] [PubMed] [Google Scholar]
- 33.Khambay B, Millett D, McHugh S. Evaluation of methods of archwire ligation on frictional resistance. Eur J Orthod. 2004;26:327–32. doi: 10.1093/ejo/26.3.327. [DOI] [PubMed] [Google Scholar]
- 34.Henao SP, Kusy RP. Frictional evaluation of dental typodont models using four self-ligating designs and a conventional design. Angle Orthod. 2005;75:75–85. doi: 10.1043/0003-3219(2005)075<0075:FEODTM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 35.Gandini P, Orsi L, Bertoncini C, Massironi S, Franchi L. In vitro frictional forces generated by three different ligation methods. Angle Orthod. 2008;78:917–21. doi: 10.2319/090607-420.1. [DOI] [PubMed] [Google Scholar]
- 36.AlQabandi AK, Sadowsky C, Begole EA. A comparison of the effects of rectangular and round arch wires in leveling the curve of Spee. Am J Orthod Dentofacial Orthop. 1999;116:522–9. doi: 10.1016/s0889-5406(99)70183-6. [DOI] [PubMed] [Google Scholar]
- 37.Sandstrom RA, Klapper L, Papaconstantinou S. Expansion of the lower arch concurrent with rapid maxillary expansion. Am J Orthod Dentofacial Orthop. 1998;94:296–302. doi: 10.1016/0889-5406(88)90054-6. [DOI] [PubMed] [Google Scholar]
- 38.Menendez M, Alarcon JA, Travesi A, Palma JC. Paris, Chicago: Quintessence; 2005. Evaluation of dental arch width and form changes after orthodontic treatment with the Damon system. Proceedings of the International Orthodontic Conference 2005; p. 445. [Google Scholar]
- 39.Sims AP, Waters NE, Birnie DJ, Pethybridge RJ. A comparision of the forces required to produce tooth movement in vitro using two self-ligating brackets and pre-adjusted bracket employing two types of ligation. Eur J Orthod. 1993;15:377–85. doi: 10.1093/ejo/15.5.377. [DOI] [PubMed] [Google Scholar]
- 40.Thomas S, Sherriff M, Birnie D. A comparative in vitro study of the frictional characteristics of two types of self-ligating brackets and two types of pre-adjusted edgewise brackets tied with elastomeric ligatures. Eur J Orthod. 1998;20:589–96. doi: 10.1093/ejo/20.5.589. [DOI] [PubMed] [Google Scholar]