

Abstract
Objective:
To investigate the repair potential of CAD/CAM (computer-aided design/computer-aided manufacturing) ceramic and composite blocks using a silane-containing bonding agent with different repair protocols.
Materials and Methods:
Twenty-four discs were constructed from CAD/CAM ceramic and composite blocks. The discs were divided into six groups according to surface pre-treatment employed; GI: Diamond stone roughening (SR), GII: SR+ silanization (SR+S), GIII: Hydrofluoric acid etching (HF), GIV: HF+ silanization (HF+S), GV: Silica coating (SC), GVI: SC+ silanization (SC+S). Silane-containing bonding agent (Single Bond Universal adhesive, 3M ESPE) was applied to the pre-treated discs. Prior to light curing, irises were cut from tygon tubes (internal diameter = 0.8 mm and height = 0.5 mm) and mounted on each treated surface. Nanofilled resin composite (Filtek Z350XT, 3M ESPE) was packed into the cylinder lumen and light-cured (n = 10). The specimens were subjected to microshear bond strength testing (μ-SBS) using universal testing machine. Failure modes of the fractured specimens were analyzed using field emission scanning electron microscope (FESEM). Eight representative discs were prepared to analyze the effect of surface treatments on surface topography using FESEM. μ-SBS results were analyzed using ANOVA and Tukeys post-hoc test.
Results:
Three-way ANOVA results showed that the materials, surface pre-treatment protocols, and silanization step had a statistically significant effect on the mean μ-SBS values at P ≤ 0.001. For ceramic discs, the groups were ranked; GIV (24.45 ± 7.35)> GVI ((20.18 ± 2.84)> GV (7.14 ± 14)= GII (6.72 ± 1.91)=GI (6.34 ± 2.21)=GIII (5.72 ± 2.18). For composite discs, groups were ranked; GI (24.98 ± 7.69)=GVI (24.84 ± 7.00) >GII (15.85 ± 5.29) =GV (14.65 ± 4.5)= GIV (14.24 ± 2.95)≥ GIII ((9.37 ± 2.78).
Conclusion:
The additional silanization step cannot be omitted if the repair protocol comprises of either hydrofluoric acid etching or silica coating for both CAD/CAM esthetic restorative materials. However, this step can be suppressed by using silane-containing adhesive with diamond stone roughened repair protocol.
Keywords: Computer-aided design/computer-aided manufacturing esthetic blocks, microshear bond strength, repair, scanning electron microscopy, silane
INTRODUCTION
Advances in CAD/CAM technology offers the dentist the opportunity to prepare, design, and fabricate esthetic indirect restorations in a single appointment, without the need for making impressions, provisional restorations, or dental laboratory support.[1] Milled restorations with CAD/CAM approach were found to be more accurate in terms of anatomic form, marginal fit and occlusal/interproximal contacts.[2,3,4,5]
Among the tooth-colored restorative materials applied to CAD/CAM technology are ceramics and resin composites. They are used for the construction of inlays, onlays and laminate veneers on occasion, however, under clinical condition, failure of esthetic restorations may occur. The most frequent causes for replacement are secondary caries, fracture, and chipping.[6,7] Total replacement scarifies sound tooth structure and results in increased preparation and restoration size.[8] Advances in adhesive dentistry make an intraoral repair using a resin bonded composite technique an attractive, functional, and esthetically pleasing alternative to restoration replacement.[9,10]
Various repair protocols were proposed by several authors.[11,12,13,14,15,16] These protocols aimed to modify the surface of the repaired substrate to promote its adhesive bonding capacity to the repaired resin composite. Different repair protocols comprised of mechanical, chemical, or physico-mechanical alteration methods. Mechanical alteration is accomplished via roughening by burs or airborne particle abrasion with alumina oxide particles.[11,12,13] While chemical alteration is done by either etching with orthophosphoric or hydrofluoric acid (HF).[12,14] Meanwhile, physico-mechanical modifying of the substrate could be done via tribosilica coating technique.[15]
Following modifying the surface texture of the repaired substrate, several authors addressed the importance of use of silane coupling agent in the chair side repair of chipped indirect esthetic restorations with composite.[17,18] Silane coupling agents are adhesion promoters able to provide chemical bonding with organic surfaces such as resin materials and inorganic surfaces, such as indirect glass ceramic restorations.[19]
Although modification of the surface texture of the repaired substrate and the application of the silane coupling agents are crucial steps in the repair process of indirect restorations, the application of bonding agent as intermediate agent is also advisable.[20,21,22] It is claimed that the bonding resin enhances the substrate wettability.[20,21,22,23] Furthermore, they seep into and level off the microrelief produced by various surface texture altering methods.[20]
For further simplicity, minimizing chair time as well as user friendly, a universal bonding agent containing silane was launched to the market. This raised a question whether the addition of silane to the bonding agent would omit the need of a separate silanization step. Thus, this study was carried out to elaborate: 1-If the operator could rely solely on the saline containing bonding agent with various repair protocols for indirect machinable restorations or still the additional silanization step is mandatory. 2- The impact of different surface pre-treatment protocols on the repair potential of machinable esthetic blocks. 3-Whether there is difference in repair bond strength between composite and ceramic blocks. The null hypotheses tested; First: Omitting the additional silanization step does not affect the μ-SBS of repaired indirect ceramic and resin composite CAD/CAM blocks with different repair protocols. Second: Different surface pre-treatment protocols have no influence on the μ-SBS of repaired tested machinable blocks. Third: There is no difference in the repair potential between indirect restorative materials evaluated.
MATERIALS AND METHODS
Specimen preparation
Thirty-two discs were constructed from indirect esthetic restorative blocks, which are designed for Cerec CAD/CAM system. Sixteen discs were constructed from leucite-reinforced glass ceramic blocks, shade A2, size 114 (Paradigm™ C; 3M ESPE), and the remaining half were constructed from nanohybrid resin composite blocks, shade A2, size 14 (Paradigm™ MZ100; 3M ESPE). Materials composition, manufacturer, and lot number are presented in Table 1.
Table 1.
Materials, composition, manufacturer, and lot number
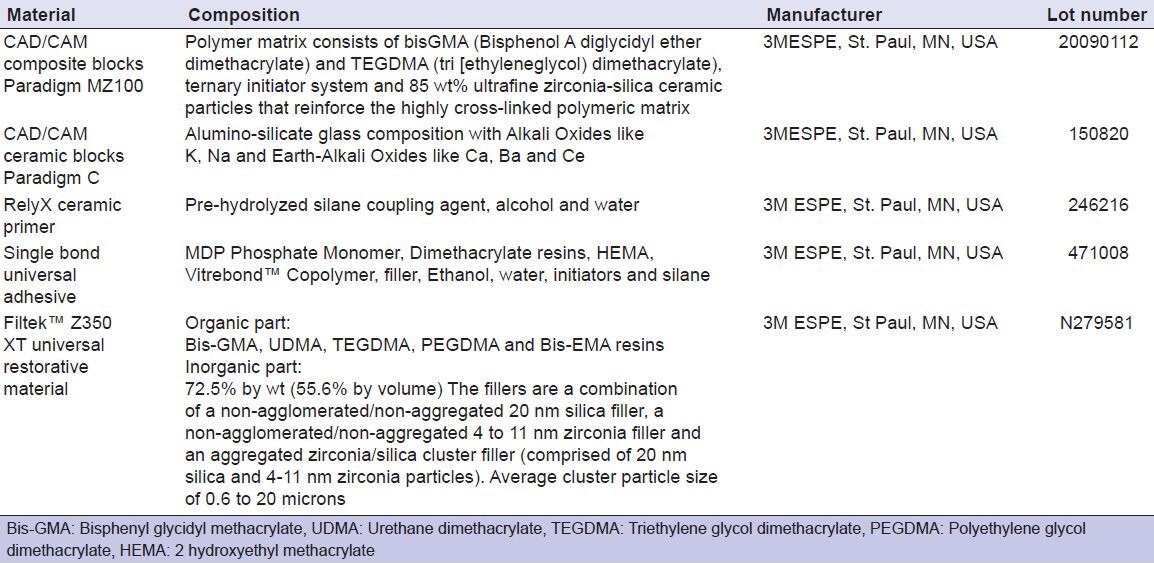
Discs of 3 mm thickness were obtained by sectioning the blocks using a low speed isomet saw (Isomet 1000, Buehler Ltd., Lake Bluff, IL, USA). The repaired surfaces were ground finished with 1200-grit silicon carbide abrasive papers (3M ESPE, St. Paul, MN, USA) under water cooling for surface standardization.[13] They were then ultrasonically cleaned (Vitasonic II, Vita, Bad Säckingen, Germany) in deionized water for 10 min to remove loose particles. The discs were embedded in acrylic resin blocks using plastic moulds with the surfaces to be repaired facing upwards. The discs were artificially aged by storing them in distilled water for 60 days. The water was changed every week to prevent bacterial growth.[21]
Twelve discs from each material were used for μ-SBS testing, and four discs were used to evaluate the effect of surface treatment on the surface topography using FESEM. The discs from each material were divided into six groups according the surface pre-treatment employed.
Group I (SR): Diamond stone roughening using a medium grit diamond stone (no. 848, Brassler, Savannah, Georgia, US). The stone was used in 5 strokes with minimum pressure using water cooled high speed hand-piece (450000 rpm). A new diamond bur was used for each four discs to ensure adequate sharpness and efficiency. This procedure was followed with 30% phosphoric acid etching (Scotchbond, 3M ESPE, St. Paul MN, USA) for 30 seconds.
GroupII (SR + S): Similar to group I followed by application of silane coupling agent.
GroupIII (HF): 3% hydrofluoric acid etching for 90 seconds (DenMat, Santa Maria, CA, USA), rinsed for 15 s and air-dried for 5 s.
Group IV (HF + S): Similar to group III followed by application of the silane coupling agent.
Group V (SC): Silica coating was done using an intraoral air-abrasion device (CoJet; 3M ESPE, Seefeld, Germany) filled with 30 μm alumina particles coated with silica (CoJet-Sand, 3 M ESPE AG, Seefeld, Germany) from a distance of approximately 10mm at a pressure of 2.5 bars for 10 s. Following surface conditioning, loose particles were gently air-blown.
GroupVI (SC + S): Similar to subgroup V followed by application of the silane coupling agent.
In the groups in which the silane coupling agent was applied, RelyX Ceramic Primer (3M ESPE, St Paul, MN, USA) was applied with a brush, left undisturbed for 1 min, and then air-dried.
Following the six different surface treatments, all groups received two consecutive coats of a silane containing bonding agent (Single Bond Universal adhesive, 3M ESPE), which was applied for 15 seconds with gentle agitation using a fully saturated applicator and gently air thinned for 5 seconds to evaporate solvent. Prior to light curing, irises were cut from tygon tubes (Norton Performance Plastic Co. Cleveland of USA) with an internal diameter of 0.8 mm and a height of 0.5 mm. Five irises were mounted on the treated surfaces to restrict the bonding area (n = 10). Light curing of the bonding resin was attempted for 10 seconds using Bluephase C5 (IvoclarVivadent AG, Schaan, Liechtenstein) light-emitting diode curing unit for 10 seconds at a light intensity of 500 mW/cm2. The light intensity was periodically checked with the light meter integrated in the hand piece holder of the curing unit. Nanofilled resin composite (Filtek Z350XT, 3M ESPE), shade A2, was packed into the cylinder Lumen, and a plastic matrix strip was placed over the resin composite and gently pressed flat and light-cured for 20 seconds using the same light curing unit according to manufacturer instructions.
The specimens were stored at room temperature for one hour prior to removing the tygon tubes using a blade. In this manner, very small cylinders of resin, approximately 0.8 mm in diameter and 0.5 mm in height, were bonded to the treated surfaces.
Microshear bond strength testing
After storage in distilled water for 24 hours, their μ-SBS were measured using a universal testing machine (Llyod instruments Ltd, fareham UK). A wire of 0.2 mm diameter was looped around the resin composite cylinder, making contact through half its circumference, and was gently held flush against the direct resin composite-repaired disc interface. The resin-repaired disc interface, the wire loop, and the center of the load cell were aligned as straight as possible to ensure the correct application of the shear force. Shear force was applied to each specimen at a cross-head speed of 0.5 mm/min until failure occurred.
Bond strength was calculated according to the formula R = F/A, where “R” is the strength (MPa), “F” the load required for rupture of the specimen, and “A” is the interface area of the specimen (mm2), A= πr2, r is the radius of the specimen, which was checked with a digital caliper before the test.
Fractographic analysis
Fracture sites of debonded surfaces were gold sputtered under vacuum and examined using FESEM (FEI Quanata 200 ESEM, France) at 30 kV accelerating voltage. Observations were performed under X400 magnification.
The fracture modes were classified into one of three types:
Type A : Adhesive failure along the direct resin composite/repaired ceramic or composite discs.
Type B : Cohesive failure within bonding agent, direct resin composite, or both.
Type C : Mixed failure of A and B.
Statistical analysis
Statistical analysis was performed with IBM® SPSS® (SPSS Inc., IBM Corporation, NY, USA) Statistics Version 21 for Windows. The significance level was set at P ≤0.05. Three way-ANOVA was used to study the effect of different restorative materials used, repair protocol, and silanization on mean μ-SBS (MPa). One-Way ANOVA has been used to study the effect of different repair protocols within each restorative material tested. Tukey's post-hoc test was used for pair-wise comparison between the means when ANOVA test is significant. Independent t-test was used to compare between the two tested materials with different repair protocols. Mode of failure was presented as percentages.
Ultra-morphological characterization of the surface topography
Four representative discs were prepared from each machinable esthetic block. The first; left as control, the second; diamond stone-roughened, the third; hydrofluoric acid-treated, and the forth; silica-coated. The parameters of the treatments applied were similar to that of bond strength testing. Specimens were gold-sputtered under vacuum and examined using FESEM at X1500 magnification.
RESULTS
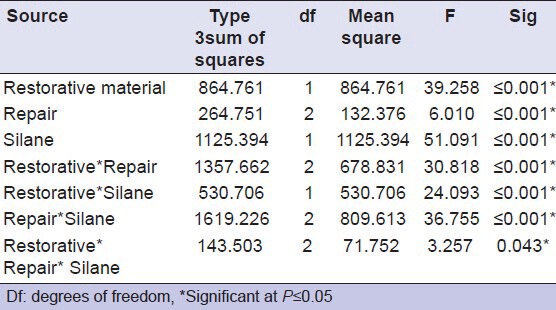
The results of three-way ANOVA presented in Table 2 showed that the additional silanization step, different surface pre-treatment protocols, and restorative materials exhibited significant influence on the mean μ-SBS values (P ≤ 0.001). Also, the interaction term between the three variables significantly affected the μ-SBS (P = 0.043).
Table 2.
Results of three-way ANOVA
Means and standard deviations (SD) of μ-SBS values in MPa of all tested groups are displayed in Table 3. A bar chart representing the μ-SBS mean values of all tested groups is presented in Figure 1. For ceramic discs, additional silanization step resulted in significant increase in the μ-SBS mean values in HF and SC-treated groups, while insignificant increase was found for SR group. For composite discs, additional silanization step significantly increased the μ-SBS of SC-treated group and significantly decreased μ-SBS for SR group. Meanwhile, it did not affect HF group.
Table 3.
Means and standard deviations of μ-SBS values (MPa) of all tested groups
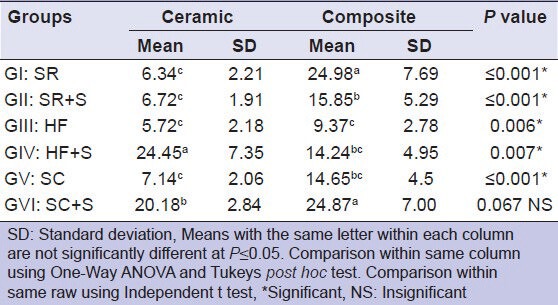
Figure 1.
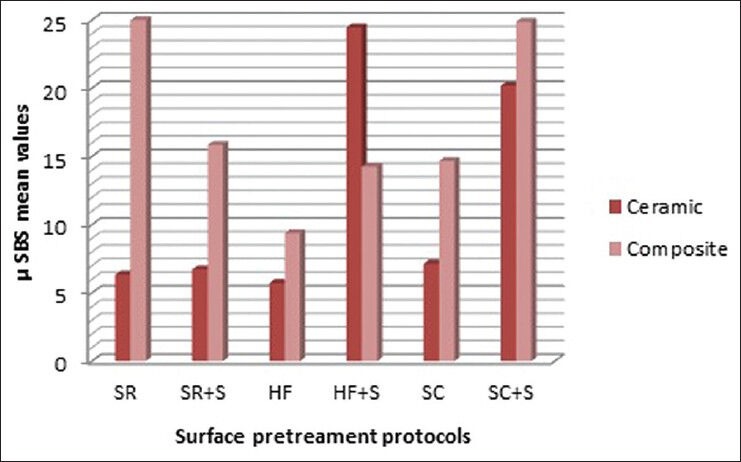
Bar chart representing the μ-SBS mean values of all tested groups
For ceramic repair, HF+S (24.45 ± 7.35) had statistically significant the highest μ-SBS followed by SC+S (20.18 ± 2.84), while SR showed the lowest mean values (6.34 ± 2.21). For composite repair, the highest μ-shear bond strength was obtained for SR (24.98 ± 7.69) with no significant difference with SC+S (24.87 ± 7.00), while HF showed the lowest bond strength values (9.37 ± 2.78) with no significant difference with HF+S (14.24 ± 4.95) and SC (14.65 ± 4.5).
The results of the independent t-test revealed that for similar treatments, significantly higher μ-SBS were obtained with composite discs than with ceramic discs, except for HF+S, SC+S treated groups.
Percentage of failure modes for all tested groups is presented in Table 4. For the ceramic discs, the predominant mode of failure for the discs pre-treated with SR, SR+S, and HF [Figure 2a] was adhesive failure at the interface. The highest percent of cohesive failure (50%) was evident in HF+S-treated group [Figure 2b]. In the same group, 40% of the specimens showed mixed mode of failure [Figure 2c]. In the SC+S groups, 50% of specimens showed mixed modes of failures [Figure 2d].
Table 4.
Percentage of failure modes of all tested groups
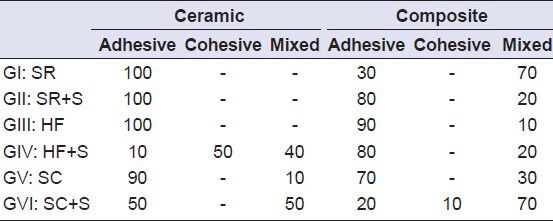
Figure 2.
SEM photos of representative specimens from ceramic. (a) adhesive failure in HF group, (b) cohesive failure in HF+S group, (c) mixed failure in HF+S group, (d) mixed failure in SC+S group
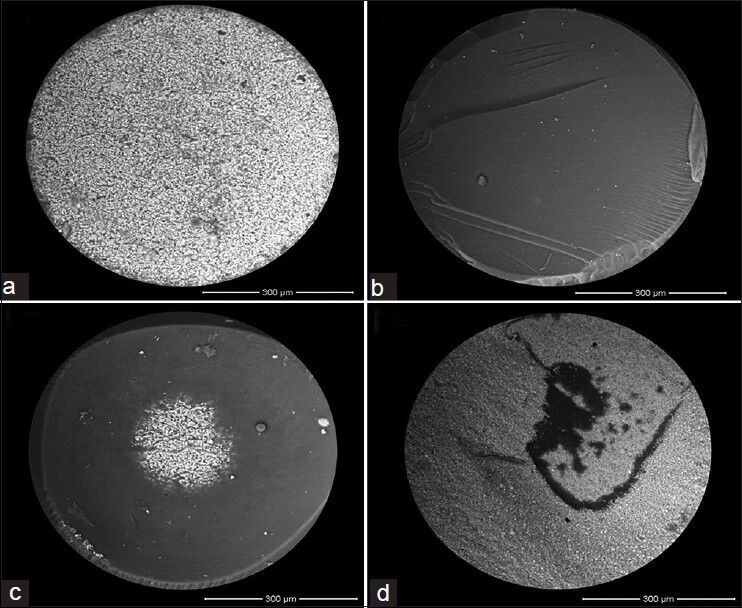
For the composite blocks, higher percentage of mixed modes of failures compared to the ceramic groups is evident. In HF group, 90% of the specimens showed adhesive failure [Figure 3a]. In both SR [Figure 3b] and SC+S groups [Figure 3c and 3d], 70% of the specimens showed mixed mode of failures. Figure 3b shows pieces of the new composite were found inside the grooves made by the diamond stone.
Figure 3.
SEM photos of representative specimens from indirect resin composite. (a) adhesive failure in HF group, (b) mixed failure in SR group, (c and d) mixed failure in SC+S group
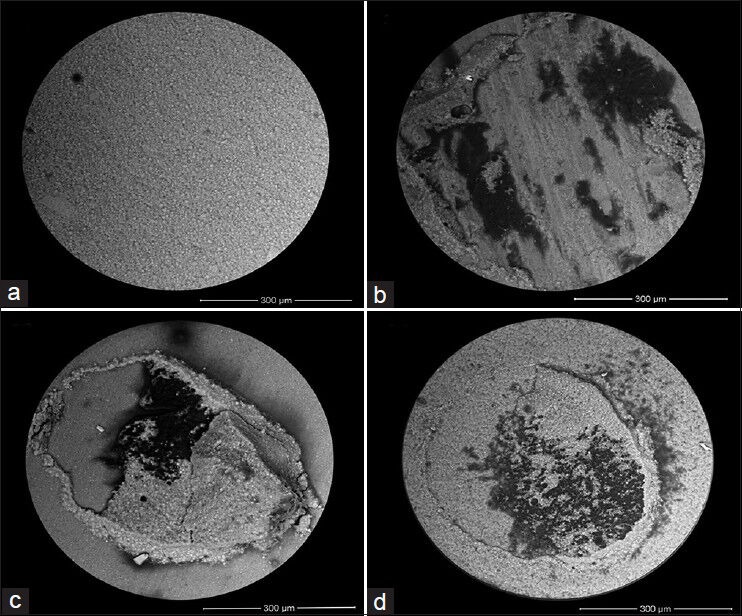
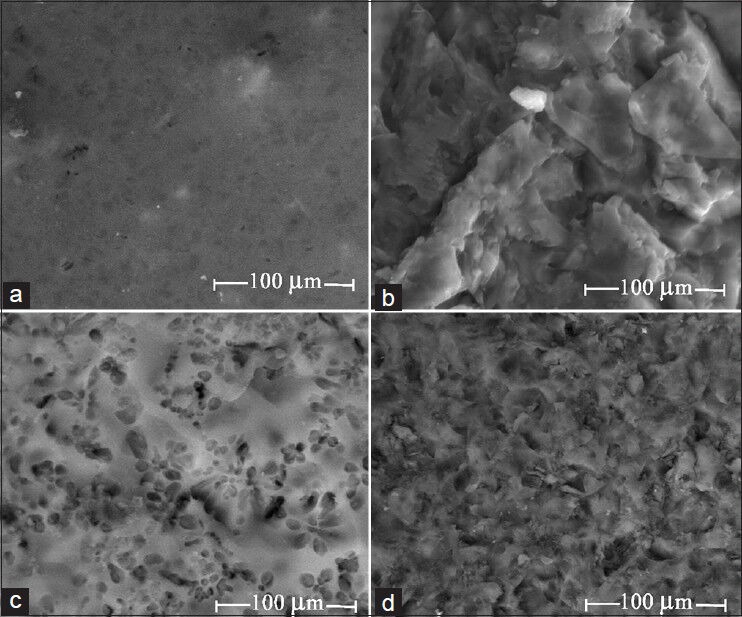
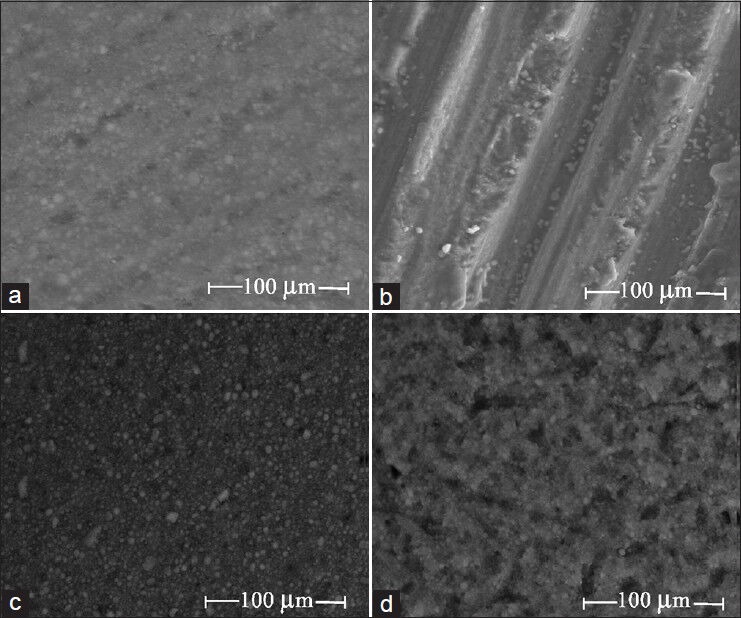
SEM analysis showed different surfaces topographies on both ceramic [Figure 4] and composite [Figure 5] surfaces; A: Control and following different pre-treatment protocols, B: SR, C: HF etching, and D: SC. SR revealed uneven surfaces with pits and porosities on both ceramic [Figure 4b] and indirect resin composite [Figure 5b] surfaces. However, the existence of the grinding marks was more evident on the composite surfaces compared to the ceramic alternative. HF etching of the ceramic surface revealed micro-involutions and recess areas created by etching the glass ceramic [Figure 4c]. On contrary, HF treatment of the indirect resin composite surfaces [Figure 5c] was associated with partial degradation of the resin matrix and little evidence of microprosities and undercuts. In SC group, micromechanical retentive features were evident on both the ceramic (4D) and indirect resin composite (5D) surfaces. The presence of attached silica/alumina particles was also noted.
Figure 4.
SEM photos representing the surface topography of ceramic blocks (a) Control, (b) Diamond stone roughening, (c) Hydrofluoric acid etching, (d) Silica Coating. SR revealed uneven surfaces with pits and porosities [Figure 4b]. HF etching revealed micro-involutions and recess areas created by etching the glass ceramic [Figure 4c]. In SC group, micromechanical retentive features were evident (4D) with the presence of attached silica/alumina particles
Figure 5.
SEM photos representing the surface topography of composite blocks. (a) Control, (b) Diamond stone roughening, (c) Hydrofluoric acid etching, (d) Silica Coating. SR revealed uneven surfaces with pits and porosities with the existence of the grinding marks from diamond stone [Figure 5b]. HF etching was associated with partial degradation of the resin matrix and little evidence of microprosities and undercuts [Figure 5c]. In SC group, micromechanical retentive features were evident with the presence of attached silica/alumina particles [Figure 5d]
DISCUSSION
Adhesive dentistry brought into perspective the possibility of the repair of pre-existing restorations rather than their complete replacement.[24] In the present study, the repair potential of the machinable CAD/CAM esthetic blocks was assessed using μ-SBS test. This test is considered a relatively simple test that permits efficient screening of adhesive systems, regional and depth profiling of a variety of substrates.[25] The microshear data was coupled with microscopic analysis of the fractured surfaces to provide a more consistent and complete description of the fracture process and modes of failure. Emphasis can then be placed on strengthening the weakest component in the chain until failure shifts to another part of the adhesive complex.[19] Shifting the mode of failure away from the ceramic/composite-repair resin interface might infer better bonding performance. In addition, evaluation of the effect of different surface pre-treatments on the surface topography of the tested materials using FESEM is a complementary tool, that gives clues about actual mechanism of adhesive bonding and helps to understand how every surface pre-treatment alters the substrate surface microscopically.
Clinically, aging is a result of exposure of esthetic materials to the oral environment. This aging process alters the physical, chemical, and mechanical properties of the restorative material, which will have a direct impact on its repair potential. In this study, aging was done storing them in distilled water for 60 days.[21]
The results of the present study clarified that the additional silanization step, different surface pre-treatment protocols, and the esthetic restorative materials have a direct influence on the repair bond strength. Thus, the three tested null hypotheses are rejected.
Silanes are adhesion promoters that contain two different reactive functional groups that can react and couple with various inorganic and organic materials. They are used to increase the union of dissimilar materials. The hydrolysable functional groups react to the surface hydroxyl groups of inorganic substrates creating a siloxane bond (Si-O-Si). The organic non-hydrolysable functional group with a carbon-carbon double bond can polymerize with resin composite monomers containing double bonds.[17,18] It could be assumed that there should be equilibrium between the amount of the hydroxyl groups of inorganic substrates exposed and the hydrolysable functional groups present in the silane. Thus, the quality of the siloxane bond formed is determined by the concentration of the silane solution[17] and the surface pre-treatment protocol that determine the amount of hydroxyl groups exposed.
For the ceramic blocks, HF etching generated a micromechanically retentive surface texture as depicted in Figure 4c, via preferential dissolution of the glassy phase from ceramic matrix. It also promoted hydroxyl group formation on the ceramic surface.[17] It could be assumed that the concentration of the silane in the bonding agent was not compatible with hydroxyl groups formed on the ceramic surfaces, which might in turn impaired the surface wettability and resin impregnation into the microretentive recess areas. The additional silanization step enhanced the chemical bonding to the exposed hydroxyl groups and surface wettability with resin impregnation. This was corroborated with amelioration of the repaired bond strength and shifting the mode of failures from 100% adhesive failures to 50% cohesive failures.
The same scenario could be predicted with the resin composite blocks as the additional silanization step enhanced the repair bond strength although of no statistical significance owing to the relatively lower silica content present compared to its ceramic alternative. However, HF etching was not the best repair protocol with such material compared to SR and SC+S subgroups. This could be attributed to the aggressive etching effect of HF that partially eroded the resinous matrix as depicted in Figure 5c. This ultra-morphological observation is similar to those of El Zohairy et al.[23] This result is in agreement with several authors[12,20,24] whom found that HF negates the repair potential of resinous composite restorations.
In the tribochemical silica-coating repair protocol, the substrate surfaces were blasted with the air-borne particles that are silica-coated alumina particles, accelerated by compressed air. The particles hit the surface and create locally high temperatures caused by the transfer of kinetic energy of the particles. The fresh SiO2 layer penetrates and was embedded onto the substrate surface.[17] Thus, creating retentive surface textures along with an increase in the percentage Si exposed at the surface as depicted in Figures 4d and 5d. This made the additional silanization step typically required. An intermediate silane application forms covalent bonding between the silica-coated layer and repaired resin composite.[17,26]
For ceramic blocks, SC+S pre-treatment was ranked the second most appropriate repair protocol following HF+S. This finding corroborates with those of Ozcan et al.[13] and contradicts those of Jedynakiewicz et al.,[27] whom found that the bond strength to machinable glass ceramics can be enhanced by silicoating in place of etching.
For resin composite blocks, the SC+S was considered the best repair protocol with no significant difference from SR group with the existence of 70% mode of failures in both tested groups. This result is in agreement with several authors,[28,29,30] whom found that silica coating and silanization showed significantly higher bond strength results than that of HF+S.
In contrary, Rathke et al.[31] found that the use of silica coating technique had no advantage over common bonding systems when used in the repair of microhybrid composite (Spectrum TPH). This contradiction could be attributed to difference in the chemical composition between both resin composites examined.
The additional silanization step following diamond stone grinding did not affect the repair bond strength for the ceramic, while it negated that of the indirect resin composite. The diamond stone grinding protocol induced macromechanical retentive features, together with microretention, as depicted in Figures 4b and 5b. This process might have associated with exposure of filler particles of the resin composite disc.[20] It is worth mentioning that in this study, phosphoric acid etching was done after diamond stone grinding to eliminate the formed smear layer and produce a clean surface.[22]
The negative effect of the additional silanization step with indirect resin composite could be attributed to the relative low amount of hydroxyl groups exposed, even though that some filler particles were exposed, they were in equilibrium with amount of silane present in the bonding agent. The additional silane step led to the existence of unreacted hydrolysable function groups with existence of week siloxane bond. The increase in the thickness of silane layer might have compromised the repaired bond strength.[17] Similar findings were reported by Bonstein et al.,[32] and Brosh et al.[33]
Diamond stone roughening protocol with ceramics is considered the worse protocol in the present study; this was in conjunction with appearance of 100% adhesive failures. This would be attributed to the relative brittleness of the ceramic making the retentive grinding grooves less evident, thus little contribution to macro mechanical retention compared to composite. The results are in agreement with Özcan et al.,[13] whom found the bur grinding with diamond stone followed by phosphoric acid showed significantly lower μSBS values compared to hydrofluoric acid etching and silica coating groups.
On the other hand, this protocol was considered a superior repair protocol with indirect resin composite. SEM photos revealed that 70% of the failure modes were mixed. In most cases, pieces of the new composite were found inside the grooves made by a diamond stone, held back by the bonding agent. Several studies reported the positive effect of bur grinding.[20,32,33] On contrary, Loomens et al.[34] found no differences between diamond stone grinding, HF etching, and silica coating.
The current study shows that the repair bond strength values with CAD/CAM composite blocks were higher than that with CAD/CAM ceramic blocks with all repair protocols, except for HF+S group. This could be attributed to the differences in the elastic modules between the two materials. As the resilience of composite polymer material can withstand stresses more than ceramic material (brittle in nature), which tends to fracture at the adhesive interface at lower values.[23]
CONCLUSIONS
Under the parameters of the present study, the following conclusions can be drawn:
Depending on the silane content incorporated in the bonding agent used merely is not sufficient when the repair protocol comprises of chemical (HF acid etching) or physico-mechanical (tribochemical silica coating) alteration for both CAD/CAM esthetic restorative materials tested. On contrary, with macromechanical alteration (diamond stone roughening), the additional silanization step did not influence the repair bond strength of the ceramic material, while it negatively affected the repair bond strength of indirect resin composite material.
SC+S is the most acceptable repair protocol that can be used equally with both indirect esthetic restorations.
CAD/CAM composite material has superior repair bond strength more than ceramic material.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared
REFERENCES
- 1.Mörmann WH, Brandestini M, Lutz F. The Cerec system: Computer-assisted preparation of direct ceramic inlays in 1 setting. Quintessenz. 1987;38:457–70. [PubMed] [Google Scholar]
- 2.Akbar JH, Petrie CS, Walker MP, Williams K, Eick JD. Marginal adaptation of Cerec 3 CAD/CAM composite crowns using two different finish line preparation designs. J Prosthodont. 2006;15:155–63. doi: 10.1111/j.1532-849X.2006.00095.x. [DOI] [PubMed] [Google Scholar]
- 3.Reiss B. Occlusal surface design with Cerec 3D. Int J Comput Dent. 2003;6:333–42. [PubMed] [Google Scholar]
- 4.Sato K, Matsumura H, Atsuta M. Relation between cavity design and marginal adaptation in a machine-milled ceramic restorative system. J Oral Rehabil. 2002;29:24–7. doi: 10.1046/j.1365-2842.2002.00798.x. [DOI] [PubMed] [Google Scholar]
- 5.Peumans M, Hikita K, De Munck J, Van Landuyt K, Poitevin A, Lambrechts P, et al. Effects of ceramic surface treatments on the bond strength of an adhesive luting agent to CAD-CAM ceramic. J Dent. 2007;35:282–8. doi: 10.1016/j.jdent.2006.09.006. [DOI] [PubMed] [Google Scholar]
- 6.Frankenberger R, Petschelt A, Krämer N. Leucite-reinforced glass ceramic inlays and onlays after six years: Clinical behavior. Oper Dent. 2000;25:459–65. [PubMed] [Google Scholar]
- 7.Forss H, Widström E. Reasons for restorative therapy and the longevity of restorations in adults. Acta Odontol Scand. 2004;62:82–6. doi: 10.1080/00016350310008733. [DOI] [PubMed] [Google Scholar]
- 8.Gordan VV, Mondragon E, Shen C. Replacement of resin-based composite: Evaluation of cavity design, cavity depth, and shade matching. Quintessence Int. 2002;33:273–8. [PubMed] [Google Scholar]
- 9.Turkaslan S, Tezvergil-Mutluay A. Intraoral repair of all ceramic fixed partial denture utilizing preimpregnated fiber reinforced composite. Eur J Dent. 2008;2:63–8. [PMC free article] [PubMed] [Google Scholar]
- 10.Blum IR, Jagger DC, Wilson NH. Defective dental restorations: To repair or not to repair. Part 2: All-ceramics and porcelain fused to metal systems? Dent Update. 2011;38:150–2. doi: 10.12968/denu.2011.38.3.150. [DOI] [PubMed] [Google Scholar]
- 11.Blum IR, Nikolinakos N, Lynch CD, Wilson NH, Millar BJ, Jagger DC. An in vitro comparison of four intra-oral ceramic repair systems. J Dent. 2012;40:906–12. doi: 10.1016/j.jdent.2012.07.008. [DOI] [PubMed] [Google Scholar]
- 12.Lucena-Martín C, González-López S, Navajas-Rodríguez de Mondelo JM. The effect of various surface treatments and bonding agents on the repaired strength of heat-treated composites. J Prosthet Dent. 2001;86:481–8. doi: 10.1067/mpr.2001.116775. [DOI] [PubMed] [Google Scholar]
- 13.Ozcan M, Valandro LF, Amaral R, Leite F, Bottino MA. Bond strength durability of a resin composite on a reinforced ceramic using various repair systems. Dent Mater. 2009;25:1477–83. doi: 10.1016/j.dental.2009.06.020. [DOI] [PubMed] [Google Scholar]
- 14.Brentel AS, Ozcan M, Valandro LF, Alarça LG, Amaral R, Bottino MA. Microtensile bond strength of a resin cement to feldpathic ceramic after different etching and silanization regimens in dry and aged conditions. Dent Mater. 2007;23:1323–31. doi: 10.1016/j.dental.2006.11.011. [DOI] [PubMed] [Google Scholar]
- 15.Ozcan M. The use of chairside silica coating for different dental applications: A clinical report. J Prosthet Dent. 2002;87:469–72. doi: 10.1067/mpr.2002.124365. [DOI] [PubMed] [Google Scholar]
- 16.Kukiattrakoon B, Thammasitboon K. Optimal acidulated phosphate fluoride gel etching time for surface treatment of feldspathic porcelain: On shear bond strength to resin composite. Eur J Dent. 2012;6:63–9. [PMC free article] [PubMed] [Google Scholar]
- 17.Matinlinna JP, Vallittu PK. Bonding of resin composites to etchable ceramic surfaces-an insight review of the chemical aspects on surface conditioning. J Oral Rehabil. 2007;34:622–30. doi: 10.1111/j.1365-2842.2005.01569.x. [DOI] [PubMed] [Google Scholar]
- 18.Lung CY, Matinlinna JP. Aspects of silane coupling agents and surface conditioning in dentistry: An overview. Dent Mater. 2012;28:467–77. doi: 10.1016/j.dental.2012.02.009. [DOI] [PubMed] [Google Scholar]
- 19.Pollington S, Fabianelli A, van Noort R. Microtensile bond strength of a resin cement to a novel fluorcanasite glass-ceramic following different surface treatments. Dent Mater. 2010;26:864–72. doi: 10.1016/j.dental.2010.04.011. [DOI] [PubMed] [Google Scholar]
- 20.Yesilyurt C, Kusgoz A, Bayram M, Ulker M. Initial repair bond strength of a nano-filled hybrid resin: Effect of surface treatments and bonding agents. J Esthet Restor Dent. 2009;21:251–60. doi: 10.1111/j.1708-8240.2009.00271.x. [DOI] [PubMed] [Google Scholar]
- 21.Staxrud F, Dahl JE. Role of bonding agents in the repair of composite resin restorations. Eur J Oral Sci. 2011;119:316–22. doi: 10.1111/j.1600-0722.2011.00833.x. [DOI] [PubMed] [Google Scholar]
- 22.da Costa TR, Serrano AM, Atman AP, Loguercio AD, Reis A. Durability of composite repair using different surface treatments. J Dent. 2012;40:513–21. doi: 10.1016/j.jdent.2012.03.001. [DOI] [PubMed] [Google Scholar]
- 23.El Zohairy AA, De Gee AJ, Mohsen MM, Feilzer AJ. Microtensile bond strength testing of luting cements to prefabricated CAD/CAM ceramic and composite blocks. Dent Mater. 2003;19:575–83. doi: 10.1016/s0109-5641(02)00107-0. [DOI] [PubMed] [Google Scholar]
- 24.Rodrigues SA, Jr, Ferracane JL, Della Bona A. Influence of surface treatments on the bond strength of repaired resin composite restorative materials. Dent Mater. 2009;25:442–51. doi: 10.1016/j.dental.2008.09.009. [DOI] [PubMed] [Google Scholar]
- 25.Armstrong S, Geraldeli S, Maia R, Raposo LH, Soares CJ, Yamagawaa J. Adhesion to tooth structure: A critical review of “micro” bond strength test methods. Dent Mater. 2010;26:e50–62. doi: 10.1016/j.dental.2009.11.155. [DOI] [PubMed] [Google Scholar]
- 26.Ozcan M, Barbosa SH, Melo RM, Galhano GA, Bottino MA. Effect of surface conditioning methods on the microtensile bond strength of resin composite to composite after aging conditions. Dent Mater. 2007;23:1276–82. doi: 10.1016/j.dental.2006.11.007. [DOI] [PubMed] [Google Scholar]
- 27.Jedynakiewicz NM, Martin N. The effect of surface coating on the bond strength of machinable ceramics. Biomaterials. 2001;22:749–52. doi: 10.1016/s0142-9612(00)00294-5. [DOI] [PubMed] [Google Scholar]
- 28.Rinastiti M, Ozcan M, Siswomihardjo W, Busscher HJ. Immediate repair bond strengths of microhybrid, nanohybrid and nanofilled composites after different surface treatments. J Dent. 2010;38:29–38. doi: 10.1016/j.jdent.2009.08.009. [DOI] [PubMed] [Google Scholar]
- 29.Passos SP, Ozcan M, Vanderlei AD, Leite FP, Kimpara ET, Bottino MA. Bond strength durability of direct and indirect composite systems following surface conditioning for repair. J Adhes Dent. 2007;9:443–7. [PubMed] [Google Scholar]
- 30.Ozcan M, Alander P, Vallittu PK, Huysmans MC, Kalk W. Effect of three surface conditioning methods to improve bond strength of particulate filler resin composites. J Mater Sci Mater Med. 2005;16:21–7. doi: 10.1007/s10856-005-6442-4. [DOI] [PubMed] [Google Scholar]
- 31.Rathke A, Tymina Y, Haller B. Effect of different surface treatments on the composite-composite repair bond strength. Clin Oral Investig. 2009;13:317–23. doi: 10.1007/s00784-008-0228-2. [DOI] [PubMed] [Google Scholar]
- 32.Bonstein T, Garlapo D, Donarummo J, Jr, Bush PJ. Evaluation of varied repair protocols applied to aged composite resin. J Adhes Dent. 2005;7:41–9. [PubMed] [Google Scholar]
- 33.Brosh T, Pilo R, Bichacho N, Blutstein R. Effect of combinations of surface treatments and bonding agents on the bond strength of repaired composites. J Prosthet Dent. 1997;77:122–6. doi: 10.1016/s0022-3913(97)70224-5. [DOI] [PubMed] [Google Scholar]
- 34.Loomans BA, Cardoso MV, Roeters FJ, Opdam NJ, De Munck J, Huysmans MC, et al. Is there one optimal repair technique for all composites? Dent Mater. 2011;27:701–9. doi: 10.1016/j.dental.2011.03.013. [DOI] [PubMed] [Google Scholar]