

Abstract
Objective:
The objective of the study is to assess the prevalence of malocclusion and orthodontic treatment needs among 12-15 years old school children of Udaipur, India.
Materials and Methods:
A cross-sectional descriptive survey was conducted among 887 subjects aged 12-15 years. The prevalence of malocclusion and orthodontic treatment needs was assessed using dental aesthetic index (World Health Organization, 1997). General information on demographic data was also recorded. Chi-square test, analysis of variance and Scheffe's test were employed for statistical analysis.
Results:
Malocclusion and orthodontic treatment need was reported among 33.3% of the study subjects. A significant age and gender difference depicting preponderance among younger age group and a male proclivity was experiential. A significant improvement in anterior crowding and largest anterior maxillary irregularity with age was documented. Males had a significantly higher prevalence of anterior crowding, midline diastema and largest anterior maxillary irregularity than females.
Conclusions:
The prevalence of malocclusion and orthodontic treatment needs among school children of Udaipur city, Rajasthan, India was found to be 33.3%. A significant age and gender difference was observed in prevalence of malocclusion, crowding and largest anterior maxillary irregularity. Midline diastema showed a significant gender difference. The baseline information outlined in the present study can be appropriately utilized for the future planning to meet the orthodontic treatment need among the population.
Keywords: Child, India, malocclusion, prevalence
INTRODUCTION
Malocclusion is defined as an irregularity of the teeth or a malrelationship of the dental arches beyond the range of what is accepted as normal.[1] Although malocclusion is not life-threatening,[2] it can be considered as a public health problem due to its high prevalence and prevention and treatment possibilities.[3] Malocclusions feature the third highest prevalence among oral pathologies, second only to tooth decay and periodontal disease and therefore rank third among world-wide dental public health priorities.[4]
Malocclusions are the result of orofacial adaptability to various etiological factors,[4] which result in various implications such as psychosocial problems related to impaired dentofacial aesthetics, disturbances of oral function, such as mastication, swallowing and speech and greater susceptibility to trauma and periodontal disease.[1] A number of studies have demonstrated its impact on quality-of-life.[5,6] Since the public equates good dental appearance with success in many pursuits and societal forces define the norms for acceptable, normal and attractive physical appearance, an individual with malocclusion might develop a feeling of shame about their dental appearance and may feel shy in social situations or lose career opportunities. There are several methods that may be used to evaluate, describe and classify occlusion. Since its development in 1986, the dental aesthetic index (DAI) has proven to be simple and rapidly applied.[7] A previous report has demonstrated the high reliability and validity of this index, which also compares favorably with other indices.[8,9] It is a cross-cultural index that links clinical and esthetic components mathematically to produce a single score. This index can be used for different communities and populations without requiring any modification.[10]
According to World Health Organization (WHO), the main oral diseases should be subjected to periodic epidemiological surveys. The epidemiological data on orthodontic treatment need is of interest for dental public health programs, clinical treatment, screening for treatment priority, resource planning and third party funding.[4] Appraisal of distribution of malocclusion in childhood can facilitate efforts to prevent such a disorder and its consequences and make it possible to reduce the complexity of costly orthodontic treatment. Furthermore, this knowledge might help to minimize or eliminate future treatment need.
Owing to the abovementioned issues and a dearth of information regarding malocclusion prevalence in this part of India, this study was taken up to assess the prevalence of malocclusion and orthodontic treatment needs in 12-15 years old school children of Udaipur, India.
MATERIALS AND METHODS
Study design and study population
A cross-sectional descriptive survey was conducted from September 2010 to February 2011 among 12-15 years old school children of Udaipur, India. Children with mixed dentition, craniofacial anomalies (clefts and syndromes) and who were undergoing or had a history of orthodontic treatment were excluded.
Official permission, ethical clearance and informed consent
The study protocol was reviewed by the Institutional Review Board and was granted ethical clearance. An official permission was obtained from the District Education Officer, District Education Office (Primary and middle; Secondary), Udaipur. A written informed consent was obtained from the parents of all the children who fulfilled the eligibility criteria and were willing to participate in the survey.
Training and calibration (reliability of the index used)
Before the commencement of the study, training and intra-examiner calibration was carried out on 20 school children in the Department of Public Health Dentistry, Pacific Dental College and Hospital. The intra-examiner reliability for DAI was assessed using kappa statistics, which was found to be 90%.
Validity of the index used
The gold standard of orthodontic treatment need was determined by three professors who are experts in the area of orthodontics with at least 10 years of clinical experience. They examined the 20 school children separately. Each child was coded as “no need for orthodontic treatment,” “elective orthodontic treatment” or “orthodontic treatment required” based on the clinical evaluation of each one. Where there was disagreement in the assessment by the professors, there was a discussion to reach a consensus.
The DAI scores and degrees of treatment need as determined by the examiner on the same 20 school children were regrouped in a dichotomous manner as follows: “without treatment needs” and “in need of treatment.” The DAI scores were dichotomized as “no need for treatment” (DAI < 25) and “in need of treatment” (DAI > 25). In the same way, the gold standard evaluation was dichotomized as follows: “without treatment needs” and “in need of treatment.” The latter category included “elective orthodontic treatment” and “orthodontic treatment required.”
Proforma details
A survey proforma designed with the help of WHO Oral Health Assessment form[11] consisted of two sections:
General information: Demographic data including name, age, gender and name and address of the school
Clinical parameter: DAI.[11]
Pilot survey
A pilot study was carried out among 70 children, 12-15 years old children from two schools to determine the feasibility of the study. Depending upon the prevalence of malocclusion obtained (31%), 95% confidence level and 10% allowable error, the sample size was determined to be 855 which was rounded off to 900.
Sampling design
Prior to instigation of the study, list of middle and high schools (Government and private) in Udaipur was obtained from District Education Office. Study sample was recruited by a multistage stratified sampling procedure. In the first stage, probability sampling was employed to select 30 schools in proportion to the total number of public (122) and private schools (180). Twelve public and 18 private schools were randomly selected. In the second stage, eligible school children were stratified according to age and gender and randomly selected in proportion to the total number of 12-15 years old students enrolled in each school. The number of children selected in each stratum (age and gender) was in proportion to students enrolled in each stratum in each school to reach the sample of around 900. The proportion of children chosen varied in all the schools accordingly.
Methodology
Data was collected by a single examiner. The examiner visited the schools on predetermined dates according to schedule. Eligible children were identified as per above specified sampling design and given informed consent forms to get them signed from their parents/guardians who were also notified by the school teachers on request of the investigator. A total of 887 subjects aged 12-15 years whose parents/guardians had given a written informed consent were examined among which 55.9% were males and 44.1% were females. The general information and the clinical examination findings were recorded. The examination for malocclusion was made according to DAI as described in WHO Oral Health Survey Basic Methods, 1997.[11] To reduce the examiner's bias (diagnostic criteria maintenance), duplicate examination was conducted on 5% (n = 45) of the population during the course of study. There were three differences in the DAI where the error was 1 mm in all of them, resulting in error rate of 0.7462%, which was disregarded (error smaller than 1.00%).
Statistical analysis
The recorded data was compiled and entered in a spreadsheet computer program (Microsoft Excel 2007) and then exported to data editor page of Statistical Package for the Social Sciences (SPSS) version 11.5 (SPSS Inc., Chicago, Illinois, USA).
The results of intra-examiner reliability were tested using Wilcoxon signed rank test. The validation of the index was performed by calculating sensitivity, specificity, positive predictive value and negative predictive value.
Descriptive statistics included computation of percentages, means and standard deviations. The Chi-square test (χ2) was used for comparisons of malocclusion prevalence between different age and gender groups. Analysis of variance along with Scheffe's test was used for comparison of mean DAI scores between the various age groups and changes in DAI scores. t-test was used for comparing the mean DAI scores between gender groups. For all tests, confidence interval and P value were set at 95% and ≤ 0.05 respectively.
RESULTS
Reliability and validity of index
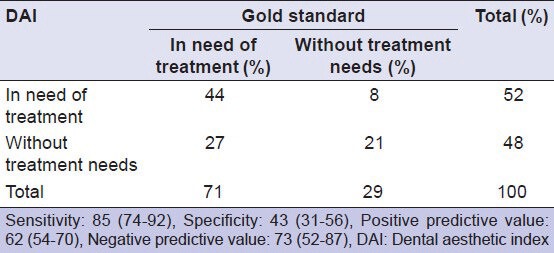
There was no statistically significant difference between the measurements for reliability (P = 0.41). The index had great sensitivity and low specificity, indicating a good ability to identify orthodontic treatment need [Table 1].
Table 1.
Frequency of orthodontic treatment need comparing diagnosis performed by panel opinion (gold standard) and DAI
Distribution of study subjects
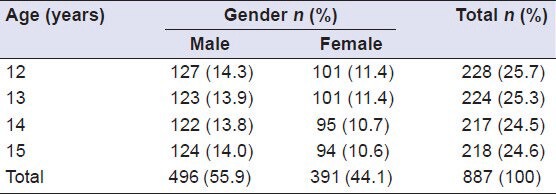
A total of 887 children (males: 496 [55.9%] and females 391 [44.1%]) participated in the survey [Table 2].
Table 2.
Distribution of study subjects by age and gender
Distribution of DAI components by age and gender
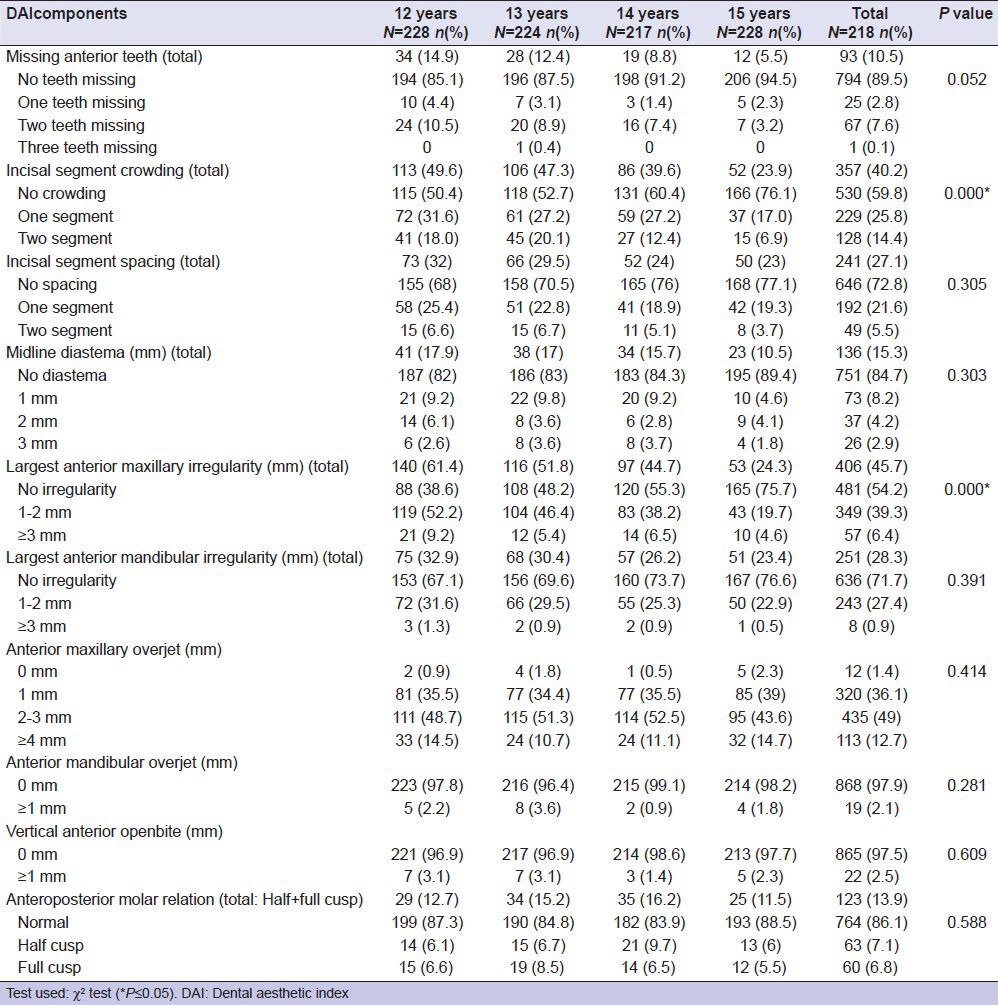
The proportion of children with crowding was significantly highest among 12 years age group (P = 0.00). A significant association (P = 0.00) of incisal segment crowding with gender was revealed with males portraying a greater prevalence of one segment (31.7%) and two segments crowding (18.5%) than females (One segment crowding: [18.4%], Two segments crowding: [9.2%]). Statistically significant gender difference evidenced a greater proportion of males ostentatious by 1 mm (12.3%), 2 mm (6.9%) and 3 mm (4.2%) diastema than females who embodied (3.1%), (0.8%) and (1.3%) children with 1 mm, 2 mm and 3 mm diastema respectively (P = 0.00). More than half of children (54.2%) showed no maxillary irregularity. Only (6.4%) had largest anterior maxillary irregularity of ≥3 mm. Statistically significant differences among the age groups (P = 0.00) showed a declining pattern of irregularity from 12 years toward 15 years. A significantly higher proportion of males revealed a largest anterior maxillary irregularity with the distribution of 45.4% and 7.9% children among 1-2 mm and ≥ 3 mm irregularity groups respectively (P = 0.00). Females exhibited 31.7% and 4.6% children with 1-2 mm and ≥ 3 mm irregularity respectively. A little more than one-fourth of the study population exhibited mandibular irregularity with 27.4% and 0.9% children falling in groups of 1-2 mm and ≥ 3 mm largest anterior mandibular irregularity respectively. Out of total 887 study subjects, majority (49%) possessed anterior maxillary overjet between 2 and 3 mm. Anterior mandibular overjet was evident in only 2.1% of the total children examined. Open bite was ostensible in 2.5% of the total children. Among all, 86.1% had normal molar relation, 7.1% had half cusp deviation and 6.8% had full cusp deviation [Tables 3 and 4].
Table 3.
Distribution of DAI components among study subjects by gender
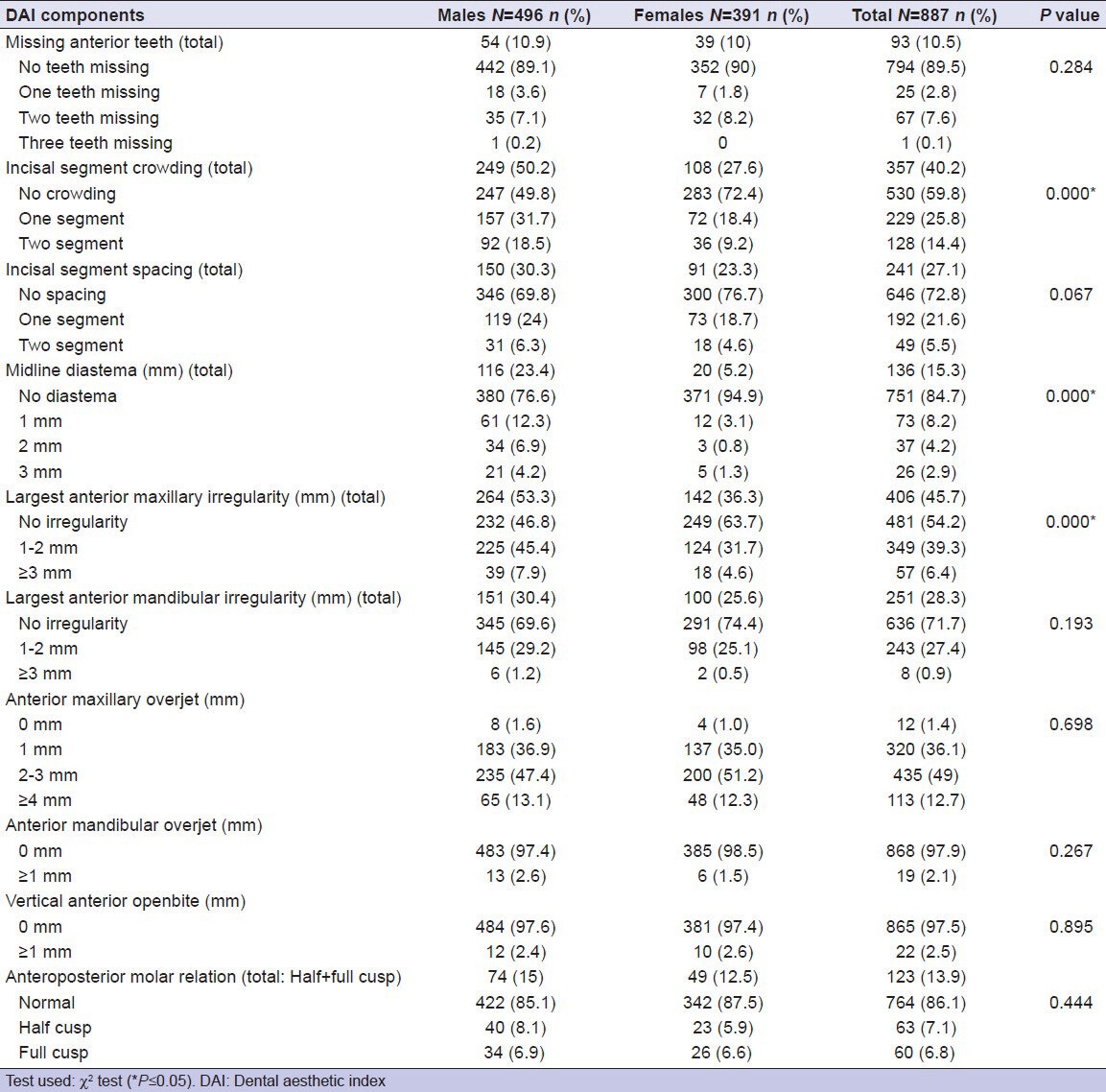
Table 4.
Distribution of DAI components among study subjects by age
Distribution of DAI scores by age and gender
The overall mean DAI score of the study population was 22.06 ± 5.623, which kept reducing significantly by age (P = 0.00) with a score of 23. 47 ± 5.624, 22.62 ± 5.669, 21.76 ± 5.511 and 20.32 ± 5.216 among 12, 13, 14, and 15 years age group respectively. Females portrayed a significantly lower mean DAI score (20.99 ± 5.355) than males (22.91 ± 5.689) with P = 0.00 [Table 5].
Table 5.
Mean dental aesthetic index score among study subjects by age and gender
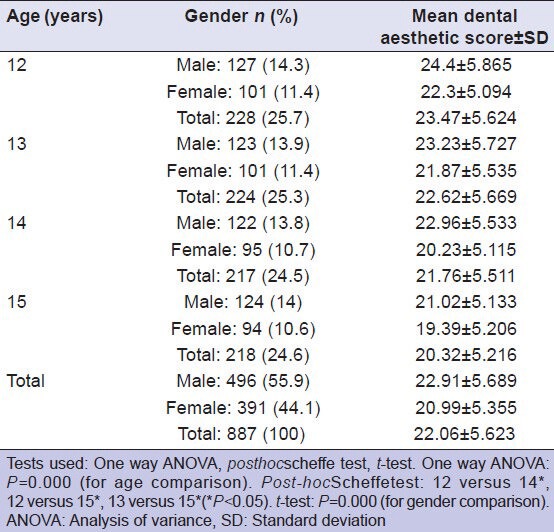
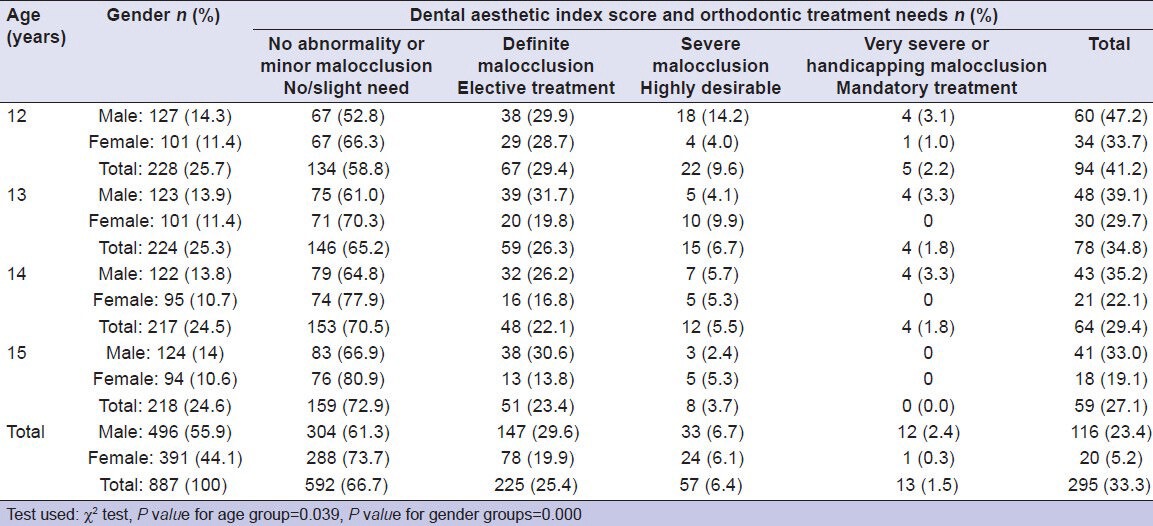
Table 6 explains a significant difference in the DAI score and orthodontic treatment needs among the study population by age (P = 0.03) and gender (P = 0.00). Of the whole population, 33.3% subjects had malocclusion and required orthodontic treatment. Agewise distribution showed a statistically significant decrease (P = 0.03) in the severity of DAI score from 12 to 15 years age group. Significant variance (P = 0.00) by gender was also ascertained with a higher percentage of male children unfolding definite malocclusion requiring elective treatment 29.6%, severe malocclusion requiring highly desirable treatment (6.7%) and very severe or handicapping malocclusion requiring mandatory orthodontic treatment than females. Elective treatment need: 19.9%, highly desirable treatment need: 6.1% and mandatory orthodontic treatment need: 0.3%.
Table 6.
Dental aesthetic index scores and orthodontic treatment needs among study subjects by age and gender
DISCUSSION
The present cross-sectional descriptive study was conducted to assess the prevalence of malocclusion and orthodontic treatment needs among 12-15 years old school going children of Udaipur, India using DAI. The execution of epidemiologic studies and dissemination of data such as that of the present study seek to advocate the need to include an orthodontic focus in the public dental services. In the studies of malocclusion prevalence, one should always choose a well-defined sample, subjects with no prior history of orthodontic treatment and objective data collection.[12] The present study fulfills such criteria.
In relation to dental anomalies, 10.5% of the study population had one or more missing anterior teeth either in maxilla and/or mandible. These results are comparable with otherstudies.[13,14,15] The missing anterior teeth observed could be either congenitally missing or due to lack of economic resources compelling people to elect the least expensive treatment (extraction) to solve their dental health problems. However, since no radiographs were used, further research is recommended to confirm this.
Furthermore, in the present study 40.2% of children had either one or two segment crowding. This prevalence is close to that reported for children living in Moshi (41.2%),[16] Belgaum (38.5%)[17] and Davangere (38.7%).[15] In harmony with the preceding surveys,[18,19] prevalence of crowding displayed a narrowing propensity with increasing age. Lower frequency of crowding in females than males narrated in studies by Danaei et al.[14] and Rwakatema et al.[16] was sustained in the present study. Like most communities,[7,15] the population studied in this research had more crowding than spacing.
On the whole, the anterior spacing affected 27.1% of the study population nearing with those expounded among Malaysians,[10] Bogotians[12] and among school children of Belgaum, India.[17]
The presence of crowding and spacing in the dental arches may be due to dentoalveolar discrepancies and tooth size and jaw size discrepancies.[15] The high prevalence of crowding may also partly be explained by the occurrence of caries and molar extraction, which causes the migration of the first permanent molar, inclinations and rotations.[4] An approximating frequency of midline diastema with the earlier studies[7,15] was observed in the present study sample. Gass et al.[18] while studying familial correlations and the hereditability of maxillary midline diastema, suggested a possible genetic basis for it. In our study, females exhibited a lower prevalence of diastema, approximately one-third, which is inconsistent with previous studies.[16,19]
In the present study, largest anterior maxillary irregularity was conferred in 45.7% of the study subjects, which is analogous to those obtained by Esa et al.[10] (40.6%) and Rwakatema et al.[16] (46%) in 2001 and 2007 respectively. Majority (39.3%) of the participants had largest anterior maxillary irregularity between 1 and 2 mm, which may be compared to the value obtained in Spain (38.5%).[7] Frequency of absence of maxillary irregularity showed a significant augmentation among the older children when weighed against the younger ones. Estioko et al.[20] also illustrated a similar improvement with age. Consistent with a survey among Iranians,[14] in the present study, males showed a significantly higher prevalence of maxillary irregularity than females.
The largest anterior mandibular irregularity occurred with prevalence of 28.3% in the study population, which is lower than the irregularity found in the upper arch (45.7%). This finding is entrenched in some previous studies.[10,15] Prevalence of largest anterior mandibular irregularity is similar to the prevalence obtained in other studies.[21,10,17]
From the data offered in the literature,[21,22,1] the proportion of 12.7% of the subjects with increased overjet found in the current study is authenticated. Edge to edge bite was recorded in rare cases (1.4%), which are lower than that found by Onyeaso[13] among Nigerians (3.2%) and Gelgör et al.[23] among Anatolians (5.6%).
Esthetic considerations aside, there are two other reasons why protruding maxillary incisors require treatment. First, it has been established that children with increased overjets are more likely to suffer traumatic injuries to their teeth[24] and secondly, there would seem to be a correlation between increased plaque scores, gingival inflammation and protruding maxillary incisors.[25]
Anterior mandibular overjet or reverse overjet displayed a very rare prevalence of 2.1% among the study population coinciding with other studies.[10,21] Apart from the growth discrepancies, early loss of upper primary canines, leading to palatal tipping and/or distal migration of upper permanent anterior teeth may also be considered as a causative factor of mandibular overjet.[1] Anterior crossbite need early interceptive treatment to enhance favorable growth and development of not only the occlusion, but also the entire craniofacial complex.[25]
In the present study, 2.5% of children presented with vertical anterior open bite. Similar results were observed by Hill[26] among Glasgow children, Esa et al.[10] among Malaysians and Shivakumar et al.[15] among Davangere children. Onyeaso[27] verified that anterior open bite was recorded in subjects with digit sucking and/or tongue thrusting habits. Thilander et al.[12] pointed out that an anterior open bite is more frequently observed in black than in white American adolescents, indicating that its occurrence may be genetically determined.
The predominant anteroposterior relationship of dental arches was normal (86.1%) in the present study sample. Deviations from normal relation were observed in 13.9% of the subjects. Similar results were obtained by other studies.[12,15] Among all, 7.1% had half cusp deviation and 6.8% had full cusp deviation. Greater frequencies of children with deviations from normal molar relation were observed in some other surveys.[10,7] The ancestral background of the various populations may have an effect on the prevalence of deviated anteroposterior molar relation. It can also be accounted for by a premature loss or massive caries of deciduous teeth.
Orthodontic treatment need found (33.3%) was similar with the needs assessed by Estioko et al.[20] among 12-16 years old Victorians (36.6%), Rwakatema et al.[16] among 12-15 years old Tanzanians (35.3%) and Moura and Cavalcanti[28] (35.1%) and Garbin et al.[29] (34.7%) among 12 years old Brazilians. The present study population portrayed a greater treatment need than that observed among 12-18 years old Brazilians,[19] 12-15 years old Iranians,[14] 12-15 years[15] and 12-14 years[17] old South Indian populations. This may be due to the fact that orthodontic concern is still given low priority in oral health-care in this area and there is an absence of planning of orthodontic care program. Instead, orthodontic care is only provided on the basis of paid service by trained specialist orthodontists who make it expensive and unaffordable.
The mean DAI score was found to be 22.06 ± 5.623, which was similar to the scores obtained in other studies.[21,14] A decrease in mean DAI scores and orthodontic treatment need with increasing age has been demonstrated in the present investigation in accordance with study among Victorians.[20] According to Knutson, a plausible explanation to this could be that the temporary malocclusions are corrected with age because the child outgrows deforming habits and dental relationships are returned to normal.[20]
Males showed slightly higher mean DAI scores (22.91) than females (20.99), which concurs with the results among 12-13 years old Malaysians[10] and 12-14 years old sample of Iranian children.[14] This generates a higher demand for orthodontic treatment among males than females. The reason for this is not understood, but it might be related to the fact that male growth starts later and does not reach maximum at the age range of the study population.
The present epidemiological survey assessed the orthodontic treatment priorities among children of Udaipur city at a young age. A systematic orthodontic examination carried out at a young age permits not only the planning and timing of treatment of malocclusion, but also facilitates the use of preventive and interceptive measures to minimize the severity of lesion and these measures requires an emphasis to meet the needs related to gross functional impairments. Notwithstanding its advantages, the study has some limitations. The DAI can be useful in both epidemiological surveys to identify unmet need for orthodontic treatment and as a screening device to prioritize subsidized orthodontic treatment in public programs where resources are insufficient to meet the demands. However, it does not record features like dental midline discrepancy, traumatic deep overbite, buccal cross-bite and posterior open bite, which are major occlusal problems that could strongly influence the treatment need. Another factor that limits this index is the fact that it was developed for the permanent dentition, therefore inadequate for deciduous and mixed dentition, being unable to identify malocclusion cases in its early stages. In addition, this index is applicable to persons with normal skeleton without abnormalities such as cleft lip, cleft palate, disproportion of maxilla and mandible, which have been excluded from the study.[14] According to Estioko et al.,[20] a malocclusion index must measure malocclusion in terms of the basic orthodontic defect, the degree of which either remains the same or increases over time. The decrease in DAI scores with age is contrary to this requirement. This may indicate that DAI does not consider developmental changes that coincide with chronologic age and it should be tested further in a longitudinal study. The cross-sectional nature of the present study limits the determination of a true age difference in the malocclusion traits and DAI scores as the cross-sectional design confounds maturation with cohort. Therefore, it can only be used descriptively. Differences in age groups or cohort can be described, but the differences cannot be definitively explained. This necessitates a longitudinal study. As well, a more extensive survey involving a larger sample from the rural and urban areas of the districts of Rajasthan would provide a better baseline for planning purpose. Specific aspects such as distribution of dental professionals and adaptation of available human and material resources will require further studies.
CONCLUSION
The prevalence of malocclusion and orthodontic treatment needs among school children of Udaipur city, Rajasthan, India was found to be 33.3%. The prevalence was greater among older than younger children and also among males than females. Further longitudinal studies are required to clarify the findings and to provide accurate estimates of the orthodontic treatment need. Age and gender distribution of crowding and largest anterior maxillary irregularity revealed a significant difference with greater prevalence among younger age groups than older ones and among males than females. Midline diastema was also significantly higher among males than females.
The present study provides baseline information to underpin the implementation of school-based oral health promotion programs. To meet the orthodontic treatment needs, the Public Health Dentistry and Orthodontic Departments of dental colleges should undertake imperative steps in the initiation and implementation of a comprehensive agenda. There is also a need to inculcate the orthodontic services in the current public health policies to fill the lacunae. A sustained effort of the public private collaboration resulting in a creative synergy capitalizing on the talent and resources of each partner can have a beneficial role.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared
REFERENCES
- 1.Mtaya M, Brudvik P, Astrøm AN. Prevalence of malocclusion and its relationship with socio-demographic factors, dental caries, and oral hygiene in 12- to 14-year-old Tanzanian school children. Eur J Orthod. 2009;31:467–76. doi: 10.1093/ejo/cjn125. [DOI] [PubMed] [Google Scholar]
- 2.Karaiskos N, Wiltshire WA, Odlum O, Brothwell D, Hassard TH. Preventive and interceptive orthodontic treatment needs of an inner-city group of 6- and 9-year-old Canadian children. J Can Dent Assoc. 2005;71:649. [PubMed] [Google Scholar]
- 3.Marques LS, Pordeus IA, Ramos-Jorge ML, Filogônio CA, Filogônio CB, Pereira LJ, et al. Factors associated with the desire for orthodontic treatment among Brazilian adolescents and their parents. BMC Oral Health. 2009;9:34. doi: 10.1186/1472-6831-9-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Brito DI, Dias PF, Gleiser R. Prevalence of malocclusion in children aged 9-12 years old in the city of Nova Friburgo, Rio de Janeiro state, Brazil. Rev Dent Press Ortod Ortop Facial. 2009;14:118–24. [Google Scholar]
- 5.Marques LS, Ramos-Jorge ML, Paiva SM, Pordeus IA. Malocclusion: Esthetic impact and quality of life among Brazilian school children. Am J Orthod Dentofacial Orthop. 2006;129:424–7. doi: 10.1016/j.ajodo.2005.11.003. [DOI] [PubMed] [Google Scholar]
- 6.Bernabé E, Flores-Mir C, Sheiham A. Prevalence, intensity and extent of oral impacts on daily performances associated with self-perceived malocclusion in 11-12-year-old children. BMC Oral Health. 2007;7:6. doi: 10.1186/1472-6831-7-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Baca-Garcia A, Bravo M, Baca P, Baca A, Junco P. Malocclusions and orthodontic treatment needs in a group of Spanish adolescents using the dental aesthetic index. Int Dent J. 2004;54:138–42. doi: 10.1111/j.1875-595x.2004.tb00269.x. [DOI] [PubMed] [Google Scholar]
- 8.Marques CR, Couto GB, Orestes Cardoso S. Assessment of orthodontic treatment needs in Brazilian school children according to the dental aesthetic index (DAI) Community Dent Health. 2007;24:145–8. [PubMed] [Google Scholar]
- 9.Camilleri S, Mulligan K. The prevalence of malocclusion in Maltese school children as measured by the index of orthodontic treatment need. Malta Med J. 2007;19:19–23. [Google Scholar]
- 10.Esa R, Razak IA, Allister JH. Epidemiology of malocclusion and orthodontic treatment need of 12-13-year-old Malaysian school children. Community Dent Health. 2001;18:31–6. [PubMed] [Google Scholar]
- 11.4th ed. Geneva: WHO; 1997. World Health Organization. Oral Health Surveys: Basic Methods. [Google Scholar]
- 12.Thilander B, Pena L, Infante C, Parada SS, de Mayorga C. Prevalence of malocclusion and orthodontic treatment need in children and adolescents in Bogota, Colombia. An epidemiological study related to different stages of dental development. Eur J Orthod. 2001;23:153–67. doi: 10.1093/ejo/23.2.153. [DOI] [PubMed] [Google Scholar]
- 13.Onyeaso CO. Orthodontic treatment need of Nigerian outpatients assessed with the dental aesthetic index. AustOrthod J. 2004;20:19–23. [PubMed] [Google Scholar]
- 14.Danaei SM, Amirrad F, Salehi P. Orthodontic treatment needs of 12-15-year-old students in Shiraz, Islamic republic of Iran. East Mediterr Health J. 2007;13:326–34. [PubMed] [Google Scholar]
- 15.Shivakumar K, Chandu G, Shafiulla M. Severity of malocclusion and orthodontic treatment needs among 12- to 15-Year-Old school children of Davangere district, Karnataka, India. Eur J Dent. 2010;4:298–307. [PMC free article] [PubMed] [Google Scholar]
- 16.Rwakatema DS, Ng’ang’a PM, Kemoli AM. Orthodontic treatment needs among 12-15 year-olds in Moshi, Tanzania. East Afr Med J. 2007;84:226–32. doi: 10.4314/eamj.v84i5.9530. [DOI] [PubMed] [Google Scholar]
- 17.Pankaj S. Prevalence of malocclusion and orthodontic treatment needs among 12-15 years school children using dental aesthetic index (DAI) J Indian Assoc Public Health Dent. 2010;15:81–4. [Google Scholar]
- 18.Gass JR, Valiathan M, Tiwari HK, Hans MG, Elston RC. Familial correlations and heritability of maxillary midline diastema. Am J Orthod Dentofacial Orthop. 2003;123:35–9. doi: 10.1067/mod.2003.56. [DOI] [PubMed] [Google Scholar]
- 19.Cavalcanti AL, Sarmento DJ, Santos JA, Moura C, Granville-Garcia AF. Prevalence of malocclusion and orthodontic treatment need in Brazilian adolescents. Hell Orthod Rev. 2008;11:91–9. [Google Scholar]
- 20.Estioko LJ, Wright FA, Morgan MV. Orthodontic treatment need of secondary school children in Heidelberg, Victoria: An epidemiologic study using the dental aesthetic index. Community Dent Health. 1994;11:147–51. [PubMed] [Google Scholar]
- 21.Otuyemi OD, Ogunyinka A, Dosumu O, Cons NC, Jenny J. Malocclusion and orthodontic treatment need of secondary school students in Nigeria according to the dental aesthetic index (DAI) Int Dent J. 1999;49:203–10. doi: 10.1111/j.1875-595x.1999.tb00523.x. [DOI] [PubMed] [Google Scholar]
- 22.Onyeaso CO. Prevalence of malocclusion among adolescents in Ibadan, Nigeria. Am J Orthod Dentofacial Orthop. 2004;126:604–7. doi: 10.1016/j.ajodo.2003.07.012. [DOI] [PubMed] [Google Scholar]
- 23.Gelgör IE, Karaman AI, Ercan E. Prevalence of malocclusion among adolescents in central Anatolia. Eur J Dent. 2007;1:125–31. [PMC free article] [PubMed] [Google Scholar]
- 24.Ravishankar TL, Kumar MA, Ramesh N, Chaitra TR. Prevalence of traumatic dental injuries to permanent incisors among 12-year-old school children in Davangere, South India. Chin J Dent Res. 2010;13:57–60. [PubMed] [Google Scholar]
- 25.Davies TM, Shaw WC, Addy M, Dummer PM. The relationship of anterior overjet to plaque and gingivitis in children. Am J Orthod Dentofacial Orthop. 1988;93:303–9. doi: 10.1016/0889-5406(88)90160-6. [DOI] [PubMed] [Google Scholar]
- 26.Hill PA. The prevalence and severity of malocclusion and the need for orthodontic treatment in 9-, 12-, and 15-year-old Glasgow school children. Br J Orthod. 1992;19:87–96. doi: 10.1179/bjo.19.2.87. [DOI] [PubMed] [Google Scholar]
- 27.Onyeaso CO, Oneyeaso AO. Occlusal/dental anomalies found in a random sample of Nigerian school children. Oral Health Prev Dent. 2006;4:181–6. [PubMed] [Google Scholar]
- 28.Moura C, LeiteCavalcanti A. Severity of occlusal pathologies and associated factors in 12-year-old school children. Acta Odontol Latinoam. 2008;21:115–9. [PubMed] [Google Scholar]
- 29.Garbin AJ, Perin PC, Garbin CA, Lolli LF. Malocclusion prevalence and comparison between the angle classification and the dental aesthetic index in scholars in the interior of Sao Paulo state-Brazil. Dent Press J Orthod. 2010;15:94–102. [Google Scholar]