

Abstract
Only seven cases of osteoma arising in the middle turbinate have been reported to date. We report the eighth case, involving osteoma in the middle turbinate of a child. This young boy was initially examined at the age of nine for the main complaint of nasal obstruction. Although a large osteoma with a maximum diameter of 30 mm was observed on computed tomography (CT), the patient was only observed because of the wishes of the family. At 13 years, he was again examined, as a result of worsening of the nasal obstruction. CT revealed that the osteoma had enlarged to a maximum diameter of 41 mm. Endoscopic surgery was attempted, but because of difficulties, the osteoma instead had to be removed under direct vision via a gingival incision. The final pathological diagnosis was osteoid osteoma. The nasal obstruction disappeared following surgery, with no recurrence after more than 12 months postoperatively.
Keywords: middle turbinate, osteoma, gingival incision, child
Introduction
Osteoma and fibrous dysplasia of bone are types of bone-derived benign tumors occurring in the paranasal and nasal cavities. Many osteomas originate in the paranasal cavity. However, these lesions rarely occur in the nasal cavity, and only seven cases of osteoma originating in the middle turbinate have been reported previously (Table 1).1–7 Nasal osteomas occur with highest incidence from the second to fourth decade of life.8 We report the eighth case of middle turbinate osteoma, which occurred in a pediatric patient. This report is the first case of middle turbinate osteoma removed by gingival incision. And we have been obtained written informed consent about reproducing information and photographs appearing in this manuscript.
Table 1.
Reported cases of osteomas of the middle turbinate.
| AUTHOR | PUBLISHED YEAR | AGE | GENDER | TUMOR SIZE | OPERATIVE APPROACH |
|---|---|---|---|---|---|
| 1. Whittet HB and Quiney RE1 | 1988 | 31 | female | Not written | Lateral rhinotomy |
| 2. Lin CJ, et al2 | 2003 | 73 | male | Not written | Modified Lynch incision |
| 3. Viswanatha B3 | 2008 | 14 | female | Not written | Modified Lynch incision |
| 4. Kutluan A, et al4 | 2009 | 31 | male | Not written | Craniofacial resection by combining bifrontal craniotomy with endonasal approach |
| 5. Migirov L, et al5 | 2009 | 65 | female | Not written | Patient refused the operation |
| 6. Daneshi A, et al6 | 2010 | 41 | female | 30 mm | Endoscopic surgery |
| 7. Yadav SP, et al7 | 2013 | 30 | male | 36 mm | Lateral rhinotomy |
| 8. Endo M, et al (present case) | 2014 | 13 | male | 41 mm | Gingival incision |
Case Report
The patient was a young boy who was examined at nine years for the main complaint of nasal obstruction, which had started four months earlier. A swelling in the middle turbinate was observed on initial examination. Computed tomography (CT) revealed a large, clearly defined mass in the left nasal cavity with a maximum diameter of 30 mm and similar radiolucency to bone (Fig. 1A). The mass was exerting outward pressure on the medial wall of the left orbit and the nasal septum was displaced to the right (Fig. 1B). No sinusitis was evident. The mass was considered to represent osteoma, and in accordance with the wishes of his parents, the patient was followed up by a local doctor. By 13 years, the nasal obstruction had worsened and the boy was again examined in our department. The mass in the left middle turbinate had increased in size compared to that at nine years. CT showed the mass had expanded to a maximum diameter of 41 mm (Fig. 2A). The interior of the left nostril was entirely occupied by the mass, which was pressing against the nasal septum (Fig. 2B). Sinusitis sphenoidalis was observed. In accordance with the wishes of the patient and his parents, surgery was performed. The procedure was attempted by endoscopy, but this had to be abandoned because the great size of the osteoma made it difficult to insert forceps and hemorrhage prevented a sufficient field of view under endoscopy. The procedure was changed to open surgery through a gingival incision and removal of the osteoma under direct vision. The lesion had a hard surface and a brittle interior. As en bloc resection could not be easily achieved, removal was done in a piecemeal fashion. Histopathological examination of the resected specimen with hematoxylin and eosin staining revealed osteoblasts together with fibrous bone formation and peripheral calcification. In the stroma, hyperplasia was observed, with spindle-shaped cells showing spindle-shaped to elliptical nuclei (Fig. 3). In view of these findings, osteoid osteoma was diagnosed. Component analysis showed 64% protein, 24% calcium carbonate, and 12% calcium phosphate. Nasal obstruction was completely resolved following surgery, and no recurrence has been encountered as of more than 12 months postoperatively (Fig. 4).
Figure 1.
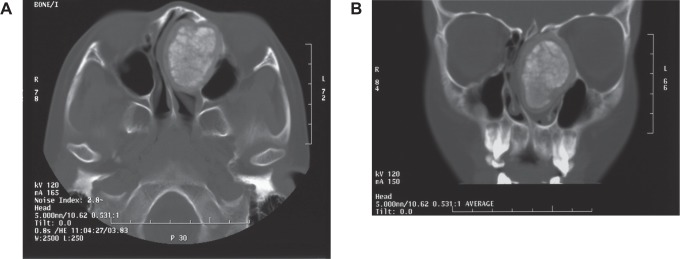
CT findings at nine years old (A: horizontal section; B: coronal section). CT reveals a clearly defined mass in the left nasal cavity with a maximum diameter of 30 mm and similar radiolucency to bone. The mass is exerting pressure on the lamina papyracea and nasal septum.
Figure 2.

CT findings at 13 years old (A: horizontal section; B: coronal section). The mass has increased in size, reaching a maximum diameter of 41 mm. The interior of the left nostril was entirely occupied by the mass, which was pressing against the nasal septum.
Figure 3.
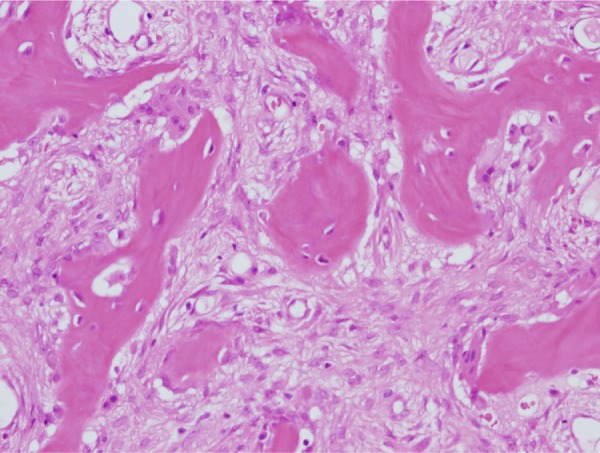
Pathological findings (hematoxylin and eosin staining). Trabeculae show mainly spindle-shaped cells and no adipose tissue.
Figure 4.
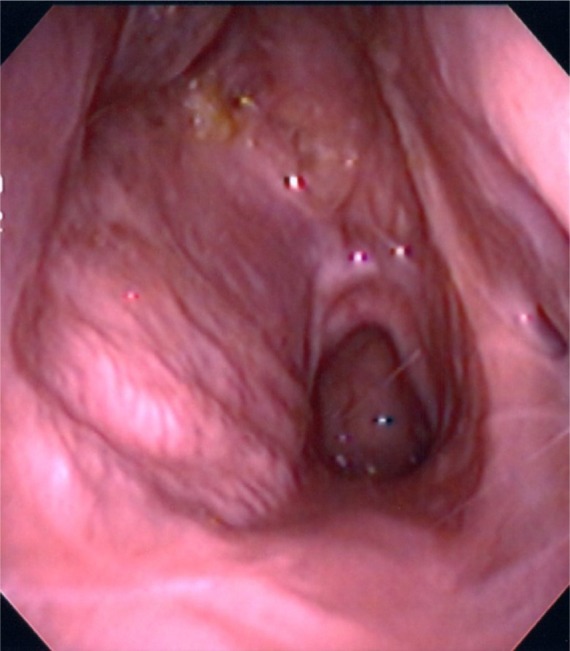
Post-operative nasal finding. Nasal obstruction was improved.
Discussion
Osteomas are benign tumors that slowly increase in size. For the majority of patients, no subjective symptoms arise in the initial phase. Osteoma produces symptoms according to a “mass effect.” When osteoma occurs in the paranasal cavity, an increase in the size of the mass may cause headache or chronic sinusitis. When they arise within the nose, the most common major complaint is nasal obstruction.6 The pressure exerted by the lesion may also give rise to symptoms such as diplopia, vision impairment, ophthalmalgia, and exophthalmos. Middle turbinate osteoma has been reported to cause pneumocephalus after extending into the anterior cranial fossa.4
The main complaint of the present patient was also nasal obstruction. At the time of surgery when the patient was 13 years old, he could hardly breathe through his nose at all. No other symptoms such as headache, diplopia, or exophthalmos were reported.
Osteoma is relatively easily diagnosed from plain X-rays and CT, and asymptomatic lesions are most often discovered incidentally during radiological examinations for other conditions. However, obtaining detailed information from plain X-rays is difficult. CT is useful for assessing relationships with neighboring structures such as the anterior cranial fossa, cribriform plate, and orbit, to consider surgical procedures.4,6 In the present case, CT clearly revealed that the osteoma was pressing on the lamina papyracea and nasal septum.
Osteoma should be followed up in the absence of symptoms, but surgery is the only treatment option when symptoms are present. Surgical approaches are classified into external, endoscopic drill-out, and combined endoscopic and external procedures.9 Small osteomas can be removed using a transnasal approach without cosmetic problems. Lateral rhinotomy is an excellent procedure and suitable for osteomas involving the ethmoid region.8 External approach was used in the five, including 14-year-old girl, of seven reported cases originating in the middle turbinate. However, external approach has a cosmetic problem and leaves surgical scars on the face. Hence, it is not suitable especially for children. As the present patient was 13 years old, endoscopic surgery was initially attempted, but was abandoned in view of the difficulty of inserting forceps and the problems obtaining a sufficient field of view because of hemorrhage. Grabovac et al reported the inferior turbinate osteoma treated with sublabial approach through the upper mouth vestibule.10 The resection by gingival incision is useful because it does not have cosmetic problem, and the giant osteoma was removed under direct vision in the present case. Given the maximum diameter of 41 mm, the tumor was removed in a piecemeal fashion. This procedure proved successful in relieving the main complaint of nasal obstruction, and no cosmetic problems arose. However, long-term follow-up is considered necessary for this young patient, for early identification of any recurrence.
Footnotes
ACADEMIC EDITOR: Yasuo Ito, Editor in Chief
COMPETING INTERESTS: Authors disclose no potential conflicts of interest.
This paper was subject to independent, expert peer review by a minimum of two blind peer reviewers. All editorial decisions were made by the independent academic editor. All authors have provided signed confirmation of their compliance with ethical and legal obligations including (but not limited to) use of any copyrighted material, compliance with ICMJE authorship and competing interests disclosure guidelines and, where applicable, compliance with legal and ethical guidelines on human and animal research participants.
Author Contributions
Conceived and designed the experiments: KT. Analyzed the data: ME and RM. Wrote the first draft of the manuscript: ME. Contributed to the writing of the manuscript: KT and MS. Agree with manuscript results and conclusions: ME, KT, KN, RM and MS. Jointly developed the structure and arguments for the paper: KT, KN and MS. Made critical revisions and approved final version: KT, KN and MS. All authors reviewed and approved of the final manuscript.
FUNDING: Authors disclose no funding sources.
REFERENCES
- 1.Whittet HB, Quiney RE. Middle turbinate osteoma; an unusual case of nasal obstruction. J Laryngol Otol. 1988;102(4):359–361. doi: 10.1017/s0022215100104967. [DOI] [PubMed] [Google Scholar]
- 2.Lin CJ, Lin YS, Kang BH. Middle turbinate osteoma presenting with ipsilateral facial pain, epiphora, and nasal obstruction. Otolaryngol Head Neck Surg. 2003;128(2):282–283. doi: 10.1067/mhn.2003.29. [DOI] [PubMed] [Google Scholar]
- 3.Viswanatha B. Middle turbinate osteoma. Indian J Otolaryngol Head Neck Surg. 2008;60(3):266–268. doi: 10.1007/s12070-008-0090-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kutluhan A, Salviz M, Bozdemir K, Değer HM, Culha I, Ozveren MF. Middle turbinate osteoma extending into anterior cranial fossa. Auris Nasus Larynx. 2009;36(6):702–704. doi: 10.1016/j.anl.2009.02.003. [DOI] [PubMed] [Google Scholar]
- 5.Migirov L, Drendel M, Talmi YP. Osteoma in an aerated middle nasal turbinate. Isr Med Assoc J. 2009;11(2):120. [PubMed] [Google Scholar]
- 6.Daneshi A, Jalessi M, Heshmatzade-Behzadi A. Middle turbinate osteoma. Clin Exp Otorhinolaryngol. 2010;3(4):226–228. doi: 10.3342/ceo.2010.3.4.226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Yadav SP, Gulia JS, Hooda A, Khaowas AK. Giant osteoma of the middle turbinate: a case report. Ear Nose Throat J. 2013;92:4–5. E10–E12. [PubMed] [Google Scholar]
- 8.Atallah N, Jay MM. Osteomas of paranasal sinuses. J Laryngol Otol. 1981;95(3):291–304. doi: 10.1017/s0022215100090721. [DOI] [PubMed] [Google Scholar]
- 9.Strek P, Zagólski O, Składzień J, Kurzyński M, Dyduch G. Osteomas of the paranasal sinuses: surgical treatment options. Med Sci Monit. 2007;13(5):CR244–CR250. [PubMed] [Google Scholar]
- 10.Grabovac S, Hadzibegovic AD, Markesic J. Inferior turbinate osteoma as a cause of unilateral nose obstruction. Coll Antropol. 2012;36(suppl 2):189–191. [PubMed] [Google Scholar]