

Abstract
This study was done to develop a Korean version of the Quality of Sexual Function (QSF-K) and evaluate the validity and reliability of the QSF-K. The participants were 220 women who visited the Center for Uterine Cancer at the National Cancer Center in Korea. Participants completed the scale once and then again at a two to four week interval. The QSF-K, Female Sexual Function Index (FSFI) and European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC-QLQ-C30) were used in this study. Receiver operating characteristics (ROC) curve, area under the ROC curve (AUC), intraclass correlation coefficients (ICC), and Cronbach's alpha were analyzed. In the analysis of the reliability, Cronbach's alpha was 0.83 and the ICC was 0.70. The validity measured with the AUC of the QSF-K comparing the FSFI and Global Health/QOL of the EORTC-QLQ-C30 was 0.717 and 0.728, respectively. Specifically, the AUC of the sexual activity level of the QSF-K was 0.838 in the FSFI comparison. The AUC of the psycho-somatic QOL of the QSF-K was 0.758 in the Global Health/QOL of the EORTC-QLQ-C30 comparison. Approximately half of the women (51.8%) had mild complaints/problems. The Korean version of the QSF was developed and validated.
Graphical Abstract
Keywords: Sexuality, Questionnaires, Validation
INTRODUCTION
Sexuality and quality of life are important issues not only for healthy people but also for cancer survivors (1, 2, 3). Overall quality of life is strongly influenced by sexuality (4). Several scales have been developed to measure the sexuality or the quality of life, but usually the focus is on sexuality or the quality of life, not both (5, 6, 7). Some questionnaires assessing the quality of life include a few items related to sexuality; however, the contents and the number of these are quite varied across questionnaires (8, 9, 10). Therefore, the quality of life and sexuality cannot be compared between populations with different characteristics or between men and women. The Quality of Sexual Function (QSF) was developed to overcome such limitations (11). It measures the sexuality and quality of life at the same time, takes a short time to complete, and is easily understood (11). The QSF can be used for women and men. In summary, the merits of QSF are to compare the quality of sexual function for both gender and easy to answer and evaluate.
Sexual problems are quite common for Korean women (12). However, the expression and discussion of sexuality is usually very conservative in Korea, as in other Asian countries (13). Adults in Korea regard sexuality as an important part of life, but only 2% of men and women have discussed sexual dysfunction with a medical doctor (14). Therefore, unintimidating and simple screening tools to detect sexual dysfunction in couples are required for clinical and research activities.
The development and validation of a questionnaire with a specific language reflecting cultural differences and the underlying meanings of words in a specific language are important (15, 16, 17). The QSF has not yet been developed or validated in Korea. Therefore, our aim was to develop and validate the Korean version of the QSF (QSF-K).
MATERIALS AND METHODS
The QSF-K was developed using forward translation, back translation, harmonization, and a pilot test, leading to finalizing the scale. Three bilingual researchers translated the scale from English to Korean, considering the definition and origin of words, the Korean culture, and underlying meanings. Seven expert gynecologic oncologists and researchers identified awkward and inadequate use of words in forward translation and suggested substitutes. After the expert panel review, the questionnaire was translated back to English by a bilingual translator. The original version of the QSF and back translation were compared and confirmed by a Korean language scholar. The pilot version of the QSF-K was pretested using a target population. Opinions about the ease of understanding and acceptability towards this version of the QSF-K were solicited from the pilot study participants. The final version of the QSF-K was completed through this well-established process.
From February to July 2013, women who visited the outpatient Center for Uterine Cancer at the National Cancer Center in Korea were enrolled in the study. The inclusion criteria were 1) not diagnosed with cancer, 2) older than 18 yr of age, 3) able to speak and understand Korean, and 4) had sexual activity within 3 months before the completion of the questionnaire. The only exclusion criterion was refusing to participate in the survey. The QSF-K was completed by 220 women at the outpatient clinic. A re-test was completed by 199 women (90.5%) via telephone within 3±1 week of the first survey.
Korean version of the Quality of Sexual Function
The QSF is self-report questionnaire developed by Heinemann et al. in 2005 and composed of 40 items including 32 items specific to 4 domains and 8 general questions (11). The four domains are psycho-somatic quality of life (QOL), 13 items; sexual activity (ACT), 7 items; sexual (dys)function-self-reflection (SDFS), 7 items; and sexual (dys)function-partner's view (SDFP), 5 items. The QSF mainly uses a five-point scale (1-5); some items in sexual activity, sexual (dys)function-self-reflection, and sexual (dys)function-partner's view domains use a six-point scale (0-5) with the values. The final score is calculated by adding the score of all items. The severity of complaints/problems rises as the total score increases.
Korean version of the Female Sexual Function Index (FSFI-K)
The FSFI-K has 19 items in six domains of sexual functioning: sexual desire, arousal, lubrication, orgasm, satisfaction, and pain. The final score is calculated using the scoring guidelines of the FSFI (6, 18).
Korean version of European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC-QLQ-C30)
The EORTC QLQ C30 has 30 items in five functional scales (physical, role, cognitive, emotional, and social), three symptom scales (fatigue, pain, and nausea and vomiting), a global health and QOL scale, and single items for the assessment of additional symptoms (19). Only the global health and QOL scale was used for comparing the AUC with the QOL in the QSF-K. The global health and QOL domain of the EORTC QLQ C30 includes two items rated on a seven-point Likert scale. The final score is calculated using the scoring manual (20, 21).
Statistical analysis
Statistical analysis was completed to test the validity and reliability of the QSF-K. Validity was tested using item internal consistency (IIC), item-discriminant validity (IDV), the receiver operating characteristics (ROC) curve, and area under the ROC curve (AUC). Reliability was evaluated by internal consistency (Cronbach's alpha) and intraclass correlation coefficients (ICC). Statistics were analyzed using the R 2.12.1 statistical software.
Ethics statement
This study was approved by the institutional review board (NCCNCS-12-685). After agreeing the purpose of this study and signing the written informed consent form, all women participated in the study.
RESULTS
Of the 220 participants, 199 (90.5%) completed the second survey. Demographic characteristics are in Table 1. The mean age of the participants was 48.1 yr, 53.2% of participants completed college or above, 47.7% of participants were menopausal, 91.8% of participants were married, 90.9% of participants had a sexual partner, and 87.7% of participants had sexual contacts during past month.
Table 1.
Demographic and medical characteristics of healthy Korean women
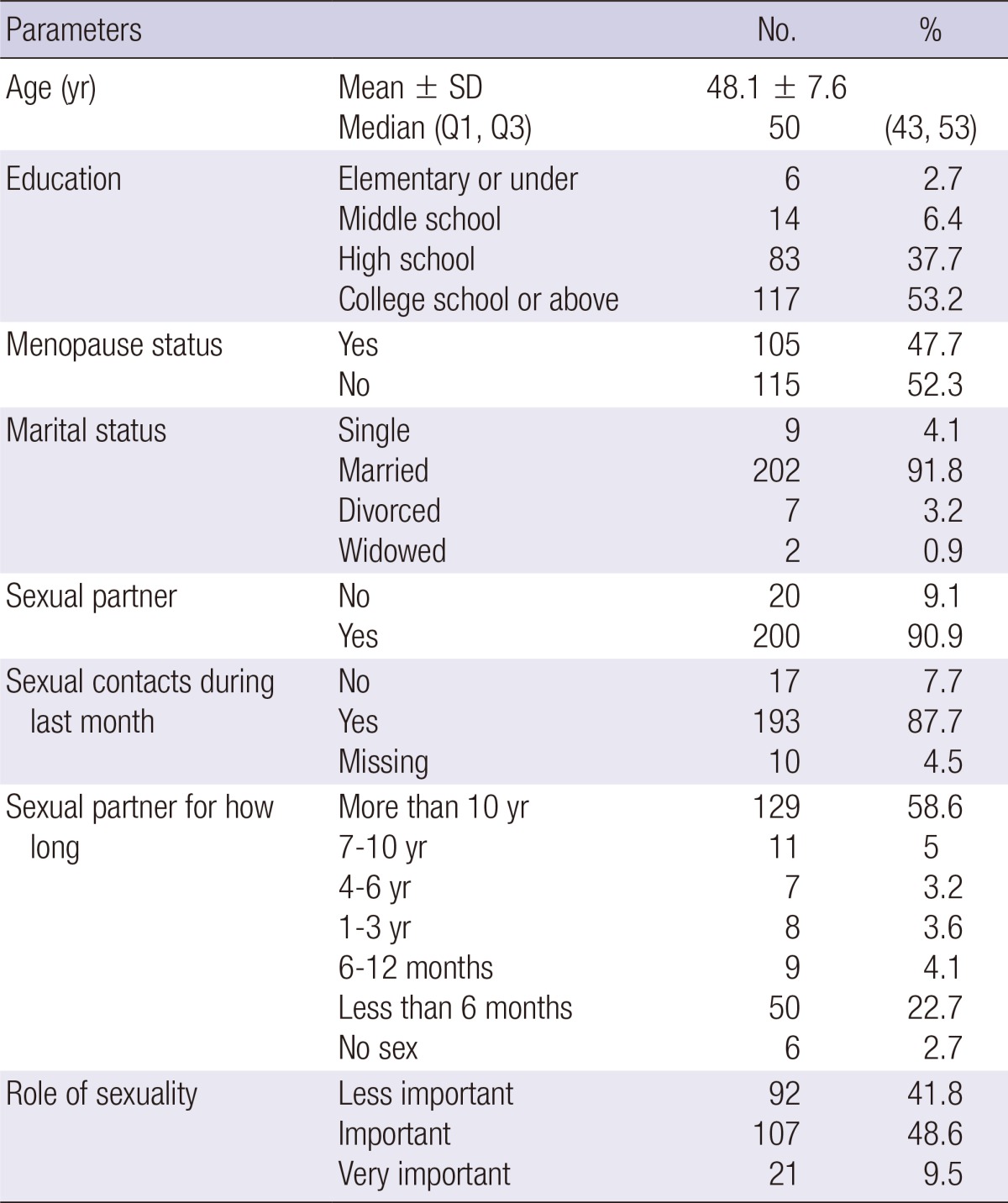
No, number; SD, standard deviation; Q, quartile.
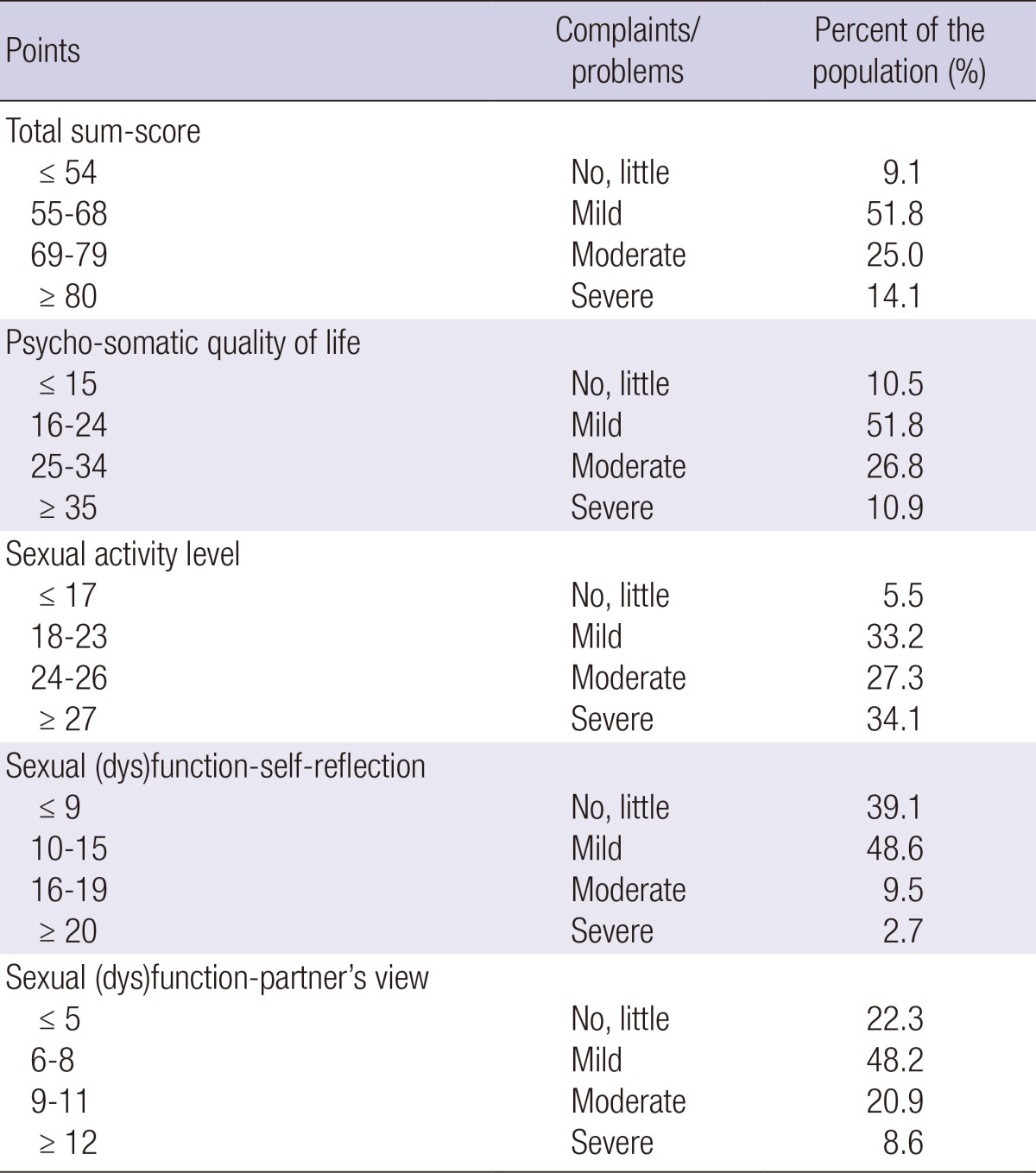
The score marked in the QSF scale was simply added up to each domains according to scoring points. Sum of scores were classified into four categories of complaints/problems; "no/little," "mild," "moderate," and "severe." Table 2 shows that how diverse the range of scores were in each categories. As a result of converting scores, the greatest proportion of participants were in the "mild" category: total score (51.8%), psycho-somatic quality of life (51.8%), sexual activity (33.2%), sexual (dys)function-self-reflection (48.6%), and sexual (dys)function-partner's view (48.2%).
Table 2.
The quality of sexual function (QSF) scale norm values
Reliability
Thirty-two items of the total scale were consistent if each item were deleted. Table 3 shows the mean values of the total and domain scores of the QSF-K. Cronbach's alpha coefficient was 0.83, ranging from 0.61 to 0.90 (Table 4). The test-retest procedure revealed ICC values for the total QSF-K score were 0.70, with items ranging from 0.52 to 0.70.
Table 3.
Reliability of total scale mean and Cronbach's alpha if item deleted
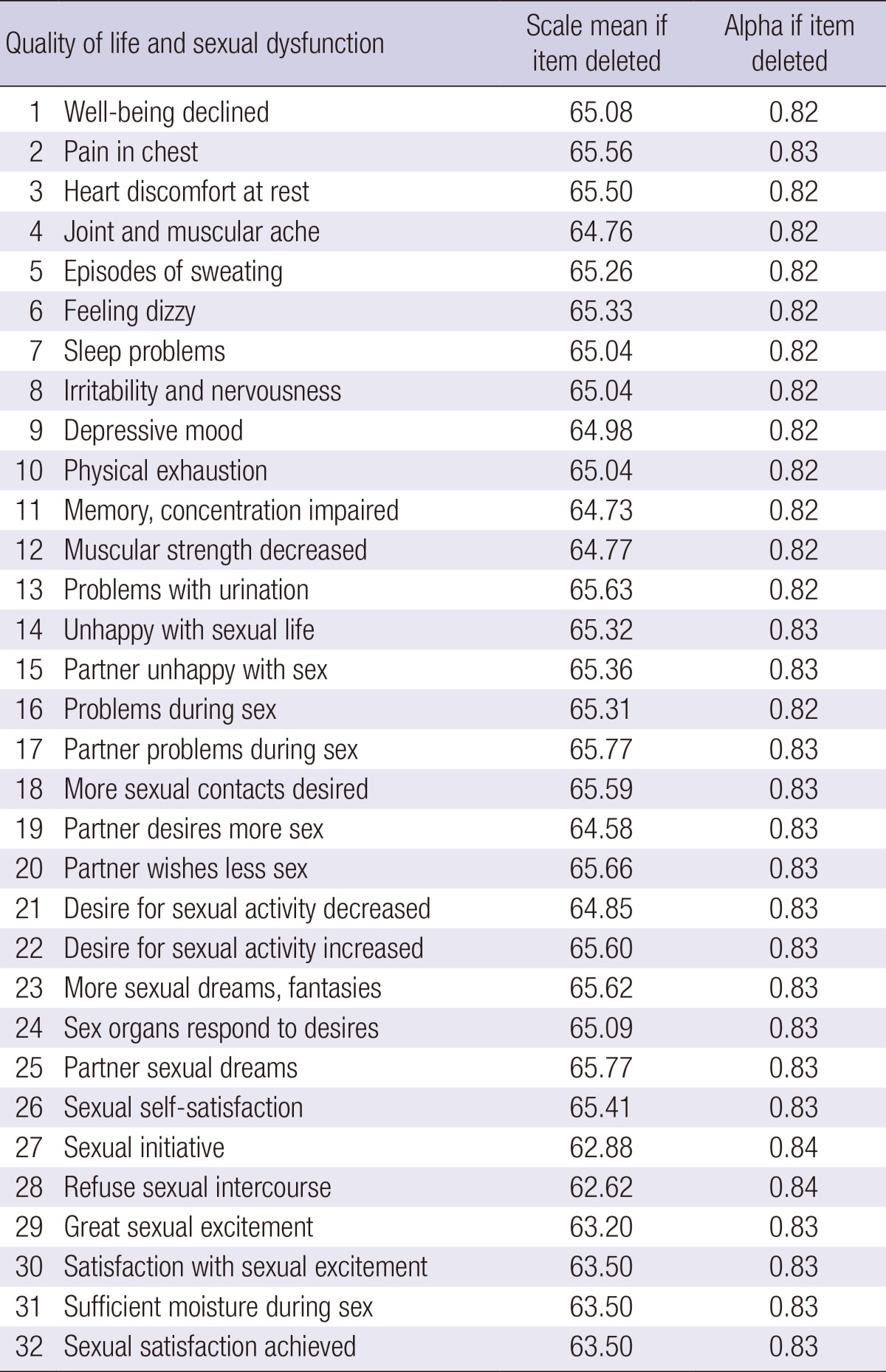
Table 4.
The QSF-K dimension characteristics of healthy Korean women

ACT, sexual activity level; ICC, intraclass correlation coefficient; IIC, item internal consistency; IDV, item discriminant validity; QOL, psycho-somatic quality of life; SDFP, sexual (dys)function partner's; SDFS, sexual (dys)function self-reflection.
Validity
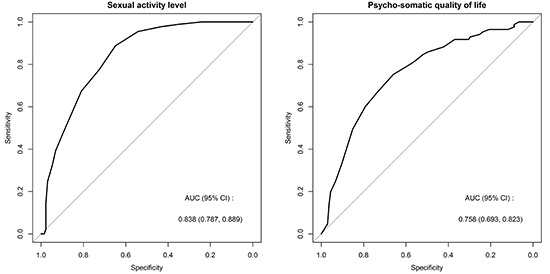
The QSF-K sub-dimension IIC was 0.11-0.76 and the IDV percentages were between 90% and 100% (Table 4). Table 5 shows sub-dimension scores and the total score of the QSF-K. The total sum score AUC of the QSF-K compared to the FSFI-K, which is relevant to the sexual activity domain, was 0.717 (95% confidence interval [CI], 0.647-0.787); the AUC of the sexual activity compared to the FSFI-K was 0.838, (95% CI, 0.787-0.889) and the rest of sub-dimensions (95% CI), psycho-somatic quality of life, sexual (dys)function-self-reflection, and sexual (dys)function-partner's view were 0.577 (0.499-0.654); 0.573,(0.495-0.650); and 0.539 (0.464-0.615), respectively (Fig. 1A).
Table 5.
The area under the ROC curve (95% CI) for the QSF-K using the FSFI-K and the Global Health/QOL domain of the EORTC-QLQ-C30

ACT, sexual activity level; CI, confidence interval; EORTC-QLQ-C30, European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; QOL, psycho-somatic quality of life; SDFP, sexual (dys)function partner's; SDFS, sexual (dys)function self-reflection.
Fig. 1.

ROC curve of Korean version of Quality of Sexual Function (QSF-K) compared to Korean version of Female Sexual Function Index (FSFI-K) and Global Health/QOL in EORTC-QLQ-C30 in healthy Korean women. (A) Sexual activity level in QSF-K compared to FSFI. (B) Psycho-somatic quality of life in QSF-K compared to Global health/QOL in EORTC-QLQ-C30.
The total sum score AUC of the QSF-K compared to the Global Health/QOL of the EORTC-QLQ-C30, which is related to the QOL domain, was 0.728 (95% CI, 0.661-0.796); the AUC of the psycho-somatic quality of life compared to the Global Health/QOL of the EORTC-QLQ-C30 was 0.758, (0.693-0.823) and the remains of sub-dimensions (95% CI), sexual activity, sexual (dys)function-self-reflection, and sexual (dys)function-partner's view were 0.573 (0.496-0.650); 0.545 (0.468-0.622); and 0.566 (0.488-0.644), respectively (Fig. 1B).
DISCUSSION
In the current study, the QSF-K was developed using a precise procedure. First, forward translation, back translation, and a pilot test were conducted. Second, participants completed the questionnaire initially, and were retested within 3±1 week. Third, the reliability and validity were confirmed through statistical analysis. Cronbach's alpha was 0.83 and ICC test reliability ICCs were 0.70. The validity measured with the AUC of the QSF-K comparing the FSFI-K and Global Health/QOL of the EORTC-QLQ-C30 was 0.717 and 0.728, respectively. Particularly, the AUC of the sexual activity of the QSF-K was 0.838 to compare of FSFI-K. The AUC of the psycho-somatic quality of life of the QSF-K was 0.758 to compare of the Global Health/QOL of the EORTC-QLQ-C30.
Cronbach's alpha of 0.83 suggests that the QSF-K is a reliable in comparison with the original QSF Cronbach's alpha (0.8). Test-retest reliability was represented by the ICC. In this study, the ICC was in the acceptable range for two domains, the psycho-somatic quality of life (0.69) and sexual activity (0.62), but not for the sexual (dys)function-self-reflection (0.52) and sexual (dys)function-partner's view (0.52). The sexual (dys)function-self-reflection domain measures the perception of personal problems in sexual functions (11), and sexual (dys)function-partner's view domain measures sexual problems that participant believed her partner perceived (11). This might be due to real changes in sexual (dys)function-self-reflection and sexual (dys)function-partner's view over time. On the other hand, the difference between the face-to-face interview in the primary survey and telephone interview in the secondary survey might have influenced the results.
The IIC of 0.37-0.76 was observed for psycho-somatic quality of life among the participants. These high correlations are comparable to those reported by Heinemann (0.57-0.90) (11). Considering the moderate ICCs of the sexual (dys)function-self-reflection and sexual (dys)function-partner's view, we estimated the AUC comparison of the FSFI-K and EORTC-QLQ-C30. FSFI-K is focused on sexuality and EORTC-QLQ-C30 estimates quality of life, respectively. On the other hand, QSF-K measures sexuality with quality of life at once. In addition, FSFI-K is a method targeted at only female gender, whereas, QSF-K is applicable for male and female both gender. The AUC of 0.717 in overall FSFI-K is acceptable. However, the AUC of the psycho-somatic quality of life, sexual (dys)function-self-reflection, and sexual (dys)function-partner's view dimensions is not acceptable. This might be because the FSFI-K does not consider the quality of life and sexual function from the view of the partner. When the AUC of the QSF-K was compared with the Global Health/QOL of the EORTC-QLQ-C30, which is a standard quality of life questionnaire measure, the psycho-somatic quality of life domain score of the QSF-K was acceptable (AUC 0.758; 95% CI, 0.693-0.823).
Sexual complains/problems were divided into four categories-"no/little," "mild," "moderate," or "severe"-based on the total score and each domain score. In the QSF total sum score, 21.1% of German and 9.1% of Korean women responded "no/little" (11). "Moderate" or more for the severity of complaints/problems on the psycho-somatic quality of life in the QSF was similar for German and Korean women (38.6% and 37.7%) (11). On the other hand, 61.4% of Korean women answered that they have sexual activity complaints/problem of "moderate" or more. It is more than twice of the 25.6% reported by German women (11). Furthermore, points of sexual (dys)function-self-reflection and sexual (dys)function-partner's view-were rated lower by Korean women than by German women. Korean women responded sexual (dys)function-self-reflection 12.2% and sexual (dys)function-partner's view 29.5%, whereas German women only responded 17.4% and 35.8%. It is consistent with the previous results that sexual pleasure and interest was lower in Asian compared to European countries (lack of sexual interest, 34.8 vs 25.6; sex not pleasurable, 29.7% vs 17.1%) (22, 23). This might be influenced by differences in health status, attitudes toward sexuality, and sexual behaviors by culture or ethnicity (24, 25).
To date, Brazil was the only country outside of Europe that had validated the QSF, and they just showed the process of translation (26). Therefore, the current study results in Korea cannot be compared to Brazilian results (26). In the QSF-K, a few minor modifications were made to the original QSF during translation. First, the term "declined" in question 1 was translated as "getting worse" in Korean. Second, "pain in my chest has occurred" in question 2 was translated as "I have had experienced chest pain" in Korean. Third, "unhappy" in question 14 and 15 was translated as "dissatisfied" in Korean. Fourth, "sexual intercourse" in several questions was translated as "sex." Lastly, polite expressions and the Korean terms of respect in Korean are reflected in the QSF-K. These modifications in the QSF-K were confirmed to reflect the Korean culture and undertone of the Korean language for the best understanding and interchangeability with original QSF by the multidisciplinary team including gynecologists, sexual health specialists, nurse researchers, bilingual translators, and a Korean language scholar.
Sexuality and quality of life has been evaluated in women with gynecologic cancer (ClinicalTrials.gov identifier: NCT01809405) by our research team (27). Studies to evaluate the sexuality and quality of life in women with cervical, ovarian, and endometrial cancer are ongoing. The sexuality of gynecologic cancer survivors compared to healthy women and the relationship between sexuality and quality of life according to the type of cancer will be identified in the near future.
In conclusion, we successfully developed the QSF-K and the reliability and validity was confirmed in a sample of Korean women. To the best of our knowledge, the QSF is only valid and reliable tool to measure sexuality and quality of life at the same time for both women and men. We believe that the QSF-K will be useful in clinical and research settings.
Footnotes
This work was supported by grants from the Korean National Cancer Center (1340930-1).
The authors have no conflicts of interest to disclose.
References
- 1.Ligibel JA, Denlinger CS. New NCCN guidelines for survivorship care. J Natl Compr Canc Netw. 2013;11:640–644. doi: 10.6004/jnccn.2013.0191. [DOI] [PubMed] [Google Scholar]
- 2.Yoo SH, Yun YH, Park S, Kim YA, Park SY, Bae DS, Nam JH, Park CT, Cho CH, Lee JM. The correlates of unemployment and its association with quality of life in cervical cancer survivors. J Gynecol Oncol. 2013;24:367–375. doi: 10.3802/jgo.2013.24.4.367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lee SS, Chung HY, Yu W. Quality of life of long-term survivors after a distal subtotal gastrectomy. Cancer Res Treat. 2010;42:130–134. doi: 10.4143/crt.2010.42.3.130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Robinson JG, Molzahn AE. Sexuality and quality of life. J Gerontol Nurs. 2007;33:19–27. doi: 10.3928/00989134-20070301-05. [DOI] [PubMed] [Google Scholar]
- 5.Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A. The international index of erectile function (IIEF): a multidimensional scale for assessment of erectile dysfunction. Urology. 1997;49:822–830. doi: 10.1016/s0090-4295(97)00238-0. [DOI] [PubMed] [Google Scholar]
- 6.Rosen R, Brown C, Heiman J, Leiblum S, Meston C, Shabsigh R, Ferguson D, D'Agostino R., Jr The Female Sexual Function Index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26:191–208. doi: 10.1080/009262300278597. [DOI] [PubMed] [Google Scholar]
- 7.King MT. The interpretation of scores from the EORTC quality of life questionnaire QLQ-C30. Qual Life Res. 1996;5:555–567. doi: 10.1007/BF00439229. [DOI] [PubMed] [Google Scholar]
- 8.Sprangers MA, Groenvold M, Arraras JI, Franklin J, te Velde A, Muller M, Franzini L, Williams A, de Haes HC, Hopwood P, et al. The European Organization for Research and Treatment of Cancer breast cancer-specific quality-of-life questionnaire module: first results from a three-country field study. J Clin Oncol. 1996;14:2756–2768. doi: 10.1200/JCO.1996.14.10.2756. [DOI] [PubMed] [Google Scholar]
- 9.Greimel E, Bottomley A, Cull A, Waldenstrom AC, Arraras J, Chauvenet L, Holzner B, Kuljanic K, Lebrec J, D'haese S. An international field study of the reliability and validity of a disease-specific questionnaire module (the QLQ-OV28) in assessing the quality of life of patients with ovarian cancer. Eur J Cancer. 2003;39:1402–1408. doi: 10.1016/s0959-8049(03)00307-1. [DOI] [PubMed] [Google Scholar]
- 10.Van Andel G, Bottomley A, Fosså SD, Efficace F, Coens C, Guerif S, Kynaston H, Gontero P, Thalmann G, Akdas A, et al. An international field study of the EORTC QLQ-PR25: a questionnaire for assessing the health-related quality of life of patients with prostate cancer. Eur J Cancer. 2008;44:2418–2424. doi: 10.1016/j.ejca.2008.07.030. [DOI] [PubMed] [Google Scholar]
- 11.Heinemann LA, Potthoff P, Heinemann K, Pauls A, Ahlers CJ, Saad F. Scale for Quality of Sexual Function (QSF) as an outcome measure for both genders? J Sex Med. 2005;2:82–95. doi: 10.1111/j.1743-6109.2005.20108.x. [DOI] [PubMed] [Google Scholar]
- 12.Song SH, Jeon H, Kim SW, Paick JS, Son H. The prevalence and risk factors of female sexual dysfunction in young Korean women: an internet-based survey. J Sex Med. 2008;5:1694–1701. doi: 10.1111/j.1743-6109.2008.00840.x. [DOI] [PubMed] [Google Scholar]
- 13.Lee ZN. Korean culture and sense of shame. Transcult Psychiatry. 1999;36:181–194. [Google Scholar]
- 14.Moreira ED, Jr, Kim SC, Glasser D, Gingell C. Sexual activity, prevalence of sexual problems, and associated help-seeking patterns in men and women aged 40-80 years in Korea: data from the Global Study of Sexual Attitudes and Behaviors (GSSAB) J Sex Med. 2006;3:201–211. doi: 10.1111/j.1743-6109.2006.00210.x. [DOI] [PubMed] [Google Scholar]
- 15.Ahn TY, Lee DS, Kang WC, Hong JH, Kim YS. Validation of an abridged Korean version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Korean J Urol. 2001;42:535–540. [Google Scholar]
- 16.Choi JH, Kim TJ, Shin K, Choi CB, Kim JH, Kim SH, Kim NI, Ahn MJ, Jung HJ, Lee KE, et al. The reliability and validity of a Korean translation of the ASAS health index and environmental factors in Korean patients with axial spondyloarthritis. J Korean Med Sci. 2014;29:334–337. doi: 10.3346/jkms.2014.29.3.334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Park HJ, Yang HK, Shin DW, Kim YY, Kim YA, Yun YH, Nam BH, Bhatia S, Park BK, Ghim TT, et al. Cross-cultural adaptation of the Korean version of the minneapolis-manchester quality of life instrument-adolescent form. J Korean Med Sci. 2013;28:1788–1795. doi: 10.3346/jkms.2013.28.12.1788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kim HY, So HS, Park KS, Jeong SJ, Lee JY, Ryu SB. Development of the Korean-version of female sexual function index (FSFI) Korean J Androl. 2002;20:50–56. [Google Scholar]
- 19.Yun YH, Park YS, Lee ES, Bang SM, Heo DS, Park SY, You CH, West K. Validation of the Korean version of the EORTC QLQ-C30. Qual Life Res. 2004;13:863–868. doi: 10.1023/B:QURE.0000021692.81214.70. [DOI] [PubMed] [Google Scholar]
- 20.Fayers PM, Aaronson NK, Bjordal K, Groenvold M, Curran D, Bottomley A. EORTC QLQ-C30 scoring manual. Brussels: European Organisation for Research and Treatment of Cancer; 2001. [Google Scholar]
- 21.Snyder CF, Blackford AL, Okuyama T, Akechi T, Yamashita H, Toyama T, Carducci MA, Wu AW. Using the EORTC-QLQ-C30 in clinical practice for patient management: identifying scores requiring a clinician's attention. Qual Life Res. 2013;22:2685–2691. doi: 10.1007/s11136-013-0387-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Nicolosi A, Glasser DB, Kim SC, Marumo K, Laumann EO GSSAB Investigators' Group. Sexual behaviour and dysfunction and help-seeking patterns in adults aged 40-80 years in the urban population of Asian countries. BJU Int. 2005;95:609–614. doi: 10.1111/j.1464-410X.2005.05348.x. [DOI] [PubMed] [Google Scholar]
- 23.Moreira ED, Jr, Brock G, Glasser DB, Nicolosi A, Laumann EO, Paik A, Wang T, Gingell C GSSAB Investigators' Group. Help-seeking behaviour for sexual problems: the global study of sexual attitudes and behaviors. Int J Clin Pract. 2005;59:6–16. doi: 10.1111/j.1742-1241.2005.00382.x. [DOI] [PubMed] [Google Scholar]
- 24.Nappi RE, Lachowsky M. Menopause and sexuality: prevalence of symptoms and impact on quality of life. Maturitas. 2009;63:138–141. doi: 10.1016/j.maturitas.2009.03.021. [DOI] [PubMed] [Google Scholar]
- 25.Parker R. Sexuality, culture and society: shifting paradigms in sexuality research. Cult Health Sex. 2009;11:251–266. doi: 10.1080/13691050701606941. [DOI] [PubMed] [Google Scholar]
- 26.Pereira VM, Silva ACdO, Nardi AE, Heinemann LA. Translation and cross-cultural adaptation into Brazilian Portuguese of the Scale for Quality of Sexual Function (QSF) Rev psiquiatr Rio Gd Sul. 2011;33:87–97. [Google Scholar]
- 27.Validation of sexual function scale in gynecologic cancer. [accessed on 20 April 2014]. Available at http://www.clinicaltrials.gov.