

Abstract
The purpose of the present study was to develop a Korean version of the trauma symptom checklist for children (TSCC) and to examine its reliability and validity for screening posttraumatic stress symptoms. A normative group of 405 children and adolescents aged 8 to 16 yr participated in the study. A test-retest procedure was conducted with 76 participants from the normative group after 4 weeks. In the traumatized group, 73 children and adolescents of the same age from the Child Sexual Abuse Treatment Center were included. Good internal consistency (Cronbach's alpha) for the total scale (0.95, ranging 0.79-0.85 on the clinical scales) and test-retest reliability for the total scale (r=0.91, ranging 0.71-0.87 on the clinical scales) were found. Confirmatory 6-factor analysis explained 51.1% of the variance. Other measures such as concurrent or discriminative validity were also shown to be satisfactory. In conclusion, the Korean version of TSCC has been shown to be a screening instrument with satisfactory psychometric qualities that is capable of identifying trauma symptoms among children and adolescents who have self-reported experiencing trauma or for whom clinicians have identified traumatic experiences.
Keywords: Trauma Symptom Checklist for Children, Post-Traumatic Stress, Self-Assessment, Children, Adolescents, Child Sexual Abuse, Screening
INTRODUCTION
Trauma is defined by the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) as exposure to an extreme traumatic stressor involving a direct personal experience of an event that involves actual or threatened death or serious injury or other threat to one's physical integrity; or witnessing an event that involves death, injury, or threat to the physical integrity of another person (1). Today much is known about the potential consequences of traumatic experiences, and there is an extensive literature that provides evidence that failure to resolve moderate to severe traumatic reactions may result in both short-term and long-term adverse consequences (2). However, not everyone who experiences a potentially traumatic event is affected by it, and it is difficult to predict individual consequences (3).
Childhood traumatic events, such as child abuse, peer assaults, natural disasters, childhood traumatic grief and medically-related trauma, are associated with a variety of negative mental health outcomes. These include anxiety, depression, posttraumatic stress, dissociation, oppositional behavior, suicidal and self-injurious behavior, anger and aggression, and sexual symptoms and age-inappropriate sexual behavior (4, 5, 6, 7, 8, 9). The potentially disastrous effects on each individual child resulting from different traumatic experiences, including sexual abuse, and the costs to the family and to society can be so substantial that it is essential to have sound assessment instruments for identifying these symptoms.
Before 1980, the assessment of childhood traumatic responses relied mostly on clinical case assessments (2), but after the Post Traumatic Stress Disorder (PTSD) diagnosis was introduced in the third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III), several instruments for the assessment of PTSD have been developed. Research has shown the need for trauma-specific instruments in order to identify these symptoms and has also shown that standard assessments or generic measurements of distress are not adequate to identify the symptoms of trauma. This is particularly true for children and adolescents who have been sexually abused (2, 8, 11, 12, 13, 14). Most measures that have been developed for use with traumatized children and adolescents have focused on specific types of trauma or specific areas of trauma-related distress, such as sexual trauma and sexual problems, for example, the Children's Impact of Traumatic Events Scale (CITES-R) (15, 16), the Child Sexual Behavior Inventory (CBSI) (17) and the Sexual Abuse Fear Evaluation (SAFE) (18), or for dissociation, for example, the Child Dissociative Checklist (CDC) (19) and the Adolescent Dissociative Experience Scale (A-DES) (14). The Trauma Symptom Checklist for Children (TSCC) (20) and the Trauma Symptom Checklist for Younger Children (TSCYC) (21) represent broad-based, multi-trait, self-report questionnaires with both abuse-specific (e.g., sexual concerns, dissociation, and posttraumatic stress) and generic (e.g., anger, anxiety, and depression) subscales.
The TSCC (20) is the only scale measuring trauma symptoms that includes scales to identify over- and under-reporting of traumatic symptoms, and it has been standardized in both non-clinical and clinical populations. The TSCC has been used in several studies as a measure of trauma symptoms (22, 23, 24, 25, 26) and in treatment outcome studies (27, 28, 29). A recent survey of traumatic stress professionals (Members of the International Society for Traumatic Stress Studies) has shown that the TSCC is the most widely used self-report scale for the measurement of trauma symptoms among children and adolescents (30), is considered quick and easy (2, 31), and is also well suited to be a screening instrument in clinical practice.
Among the various types of childhood trauma, child sexual abuse has been at the center of remarkable public and academic attention in Korea. The Yonsei University Health System was charged by the Korean Ministry of Gender Equality and Family with organizing child sexual abuse response teams named "Sunflower Centers," starting in 2004. Eight Sunflower Centers have been founded throughout Korea since and over a thousand sexually abused children have been evaluated and treated medically and psychologically in those centers each year. The Korean National Statistical Office reported 2,054 child sexual abuse cases among children and adolescents in 2011 and it was 2.4 times more than in 2007. For this reason, it became necessary to introduce measurements for the children's trauma symptom in Korea (http://police.go.kr/infodata/pds_crimes.jsp).
The need to evaluate child victims of sexual abuse has been growing and the relative lack of assessment resources such as a Korean version of the trauma scales has been problematic. The purpose of the present study was to develop a Korean version of the TSCC and to evaluate its reliability and factorial validity in non-clinical and clinical samples of Korean children and adolescents.
MATERIALS AND METHODS
Participants
Normative group
Our intent was to include children and adolescents, 8 to 16 yr of age, from different socioeconomic areas in Daegu, for which Jung-gu and Seo-gu were selected. They are areas within the city of Daegu with 76,545 and 223,279 inhabitants, respectively, and are representative of the city in terms of family socioeconomic status (32). In Korea, compulsory school for children and adolescents consists of nine grades, which include 6 grades of elementary school, 3 grades of middle school, and most children starting at age 7 finish by age 15 or 16. By applying a sampling procedure designed to ensure a good representation of students from different socioeconomic areas, schools were chosen according to official information about housing conditions. A proportional number of schools were then randomly chosen from each area. In total, 2 schools and 18 classes were chosen from among all schools in the compulsory school system, from the first grade of elementary school through the third grade of middle school. No school or class that was invited to participate refused, and 407 children and adolescents were available for this study. A total of 405 children and adolescents from these groups answered the TSCC. Cases with incomplete questionnaires were excluded (n=2, omitted enough questions to be invalid according to the TSCC manual). This resulted in a participation rate of 99.5%. There were 181 boys and 224 girls in the study (Table 1). The mean age and standard deviation was 12.0±2.1 yr for boys and 11.61±2.4 yr for girls. To assess test-retest reliability, 76 students (mean age=11.0 yr, SD=2.31), representing 16 classes randomly selected from the 18 classes from the first grade in elementary school through the third grade in middle school, completed the questionnaire a second time four weeks after completing the initial questionnaire. Four weeks between the two test occasions was considered to be a reasonable amount of time to obtain a degree of stability for answers and at the same time ensure that the answers were unduly influenced by the individual's recollection of the answers given during the first test (30).
Table 1.
Demographic information for the normative sample (n = 405)
The same divisions of age groups were used as Briere (20) and, consequently, the samples consisted of two groups: children aged 8 to 12 yr (preadolescence) and children aged 13 to 16 yr (adolescence).
Traumatized group
In the traumatized group, there were 73 patients, consecutively chosen, who were selected from the Sunflower Center for the treatment of sexually abused children in Daegu. Parents or other guardians gave informed consent for participation. All cases had been sexually abused (corroborated by police reports and medical charts), but some had also been subjected to physical abuse. There were 49 girls and 24 boys in this group and the age varied between 8 and 17 yr (boys, mean age 10.1 yr, SD=1.3; girls, mean age 10.3 yr, SD=2.6). The TSCC was completed before the start of treatment, and no psychiatric diagnoses were made at that time.
Questionnaires
Trauma symptom checklist for children
The TSCC (Briere, 1996) is a self-report instrument designed to identify a broad range of symptoms of traumatic experiences in children and adolescents aged 8 to 17 yr (19). This 54-item questionnaire takes approximately 15-20 min to administer. Each item is rated on a 4-point Likert scale: 0 "never," 1 "sometimes," 2 "lots of times," and 3 "almost all of the time." The measure has six clinical scales with 9 to 10 items in each: Anxiety (Anx), Depression (Dep), Posttraumatic Stress (Pts), Sexual Concerns (Sc), Dissociation (Dis), and Anger (Ang). Three questions, items 10, 11, and 25, belong to two scales (Table 2). In addition, there are two subscales in the sexual concerns scale: sexual preoccupation (Sc-p) and sexual distress (Sc-d), and two in the dissociation scale: fantasy (Dis-F) and overt dissociation (Dis-O). There are also two validity scales: underresponse (Und) and hyperresponse (Hyp), in which underresponse describes a child's tendency to deny symptomatology and hyperresponse shows the tendency to overrespond to symptom items.
Table 2.
Confirmatory factor analysis restricted to six factors and the clinical scales in the original TSCC version*
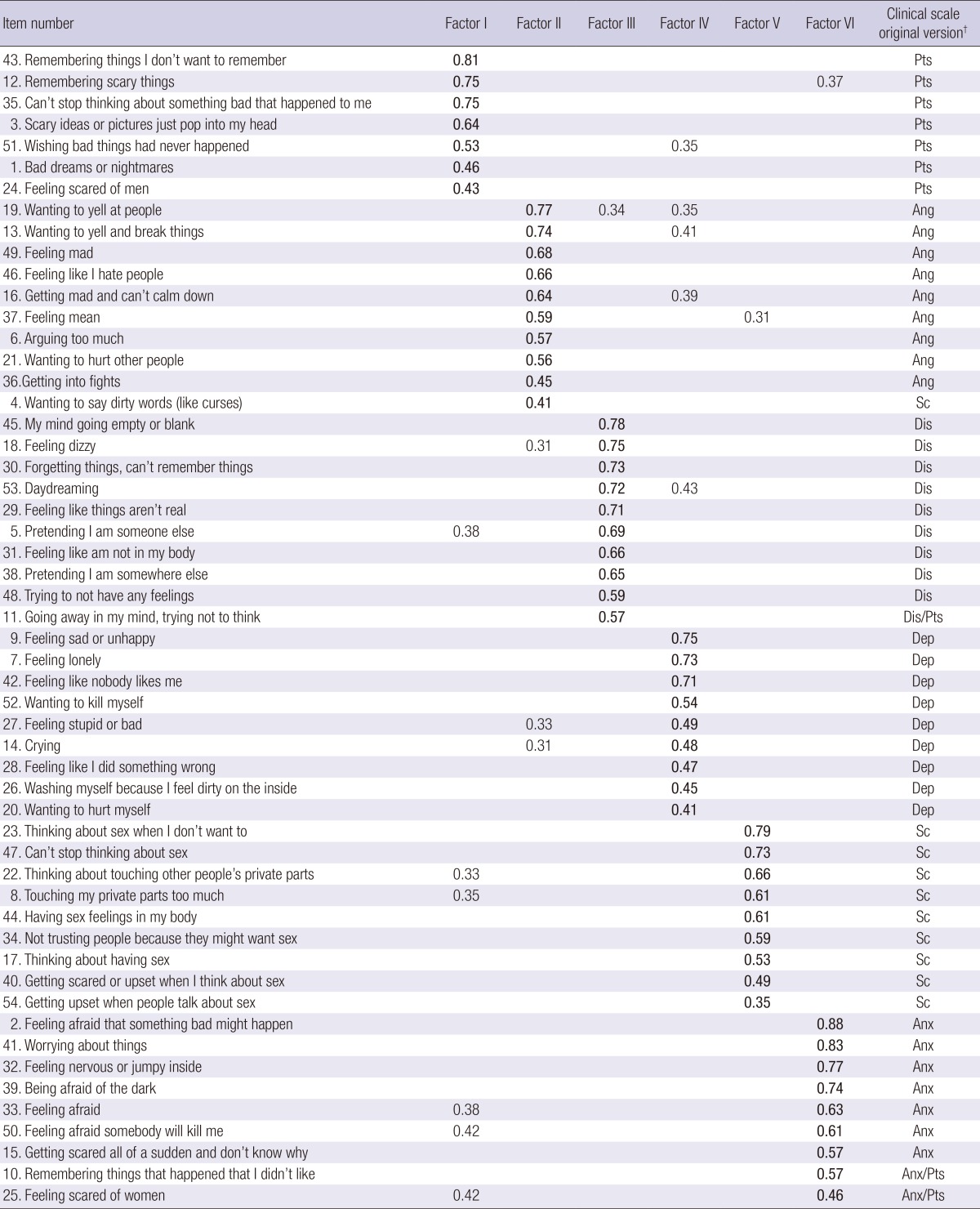
Only factor loadings>0.30 are displayed (interesting-important according to Hair, Andersen, Tatham, & Black, 1995), highest loading in bold-face type. *The extraction method used was the principal component analysis and rotation method: varimax rotation with Kaiser normalization (eigenvalues>1); †Pts (Post traumatic stress), Ang (Anger), Dis (Dissociation), Dep (Depression), Sc (Sexual Concern), Anx (Anxiety). TSCC, Trauma Symptom Checklist for Children.
The standardization of the TSCC was based on 3,008 normative school children from different parts of the USA and in the manual for the TSCC, Cronbach's alpha coefficients ranged from 0.77 to 0.89 for the clinical scales and 0.84 for the total scale (20). Its validity has been tested and established in various ways, such as convergent and discriminant validity, construct validity, and subscale intercorrelations (20, 34, 35).
The questionnaire was translated into Korean by two child and adolescent psychiatrists independently of each other. After a consensus procedure, the translated questionnaire was sent to a bilinguist for back-translation. The back-translation was then compared with the original and a final version with minor differences was sent to and accepted by the designer of the original scale.
Children's Depression Inventory (CDI)
The CDI, was used for the purpose of testing concurrent validity (correlation between the Korean version of the CDI and the depression subscale of the Korean version of the TSCC). The CDI was introduced by Maria Kovacs in 1981 and first published in 1992 (36, 37). The CDI is a symptom-oriented self-report instrument for assessing depression in children between the ages of 7 and 17 yr. The CDI contains 27 items, each of which consists of three statements. For each item, the individual is asked to select the statement that best describes his or her feelings for the past two weeks. The assessment is designed for a variety of situations, including schools, child guidance clinics, pediatric clinics, and child psychiatric settings. The Korean version of the CDI was developed in 1990 (38).
State-Trait Anxiety Inventory for Children (STAI-C)
The STAI-C was first introduced by Spieberger in 1970 (38). The instrument is designed to be used with upper elementary or junior high school-aged children and consists of two 20-item scales. The STAI-C State Anxiety (S-Anxiety) scale consists of 20 statements that ask children how they feel at a particular moment in time. The STAI-C Trait Anxiety (T-Anxiety) scale also contains 20 items, but subjects respond to these items by indicating how they feel at a particular moment in time.
The S-Anxiety scale is designed to measure transitory anxiety states, that is, subjective, consciously perceived feelings of apprehension, tension, and worry that vary in intensity and fluctuate over time. The T-Anxiety scale measures relatively stable individual differences in anxiety proneness, that is, differences between children in their tendency to experience anxiety states. Children with high T-Anxiety scores are more prone to respond to situations perceived as threatening with elevations in S-Anxiety intensity than children with low T-Anxiety scores. The Korean version of the STAI-C was developed in 1989. The Korean version of the Anxiety Questionnaire, the STAI-C, was also used for the purpose of testing concurrent validity (correlation between the Korean version of the STAI-C and the anxiety subscale of the Korean version of the TSCC).
Procedure
The headmaster of each school was first contacted by letter and then by telephone. When the headmaster had made a list of teachers and classes, written information was given to students and parents and informed consent was obtained. The students were also given information about where they could get counseling if participation had caused feelings of distress.
All questionnaires were answered anonymously. In the sixteen classes where the test-retest procedure had been involved, the teachers had coded the questionnaires to make certain that all were kept anonymous to the researchers.
Statistical procedures
To test the construct validity of the TSCC in the Korean sample, we performed factor analysis (CFA) using principal component analysis and varimax rotation with Kaiser normalization as the extraction method.
To evaluate the internal reliability of the TSCC in the Korean sample, we calculated Cronbach α coefficients for the total score and for each clinical scale. Test-retest reliability was evaluated using Pearson's r. The relationship between the total score and the clinical scales were also examined using Pearson's r.
Comparisons of the TSCC total score and subscale scores between the normal group and the traumatized group were examined using analysis of covariance (ANCOVA), controlling for the effects of age and gender. Statistical analysis was performed with SPSS/Windows (Version 16.0).
Ethics statement
The institutional review board of Kyungpook National University Hospital reviewed and permitted the study (2011-05-012). Informed consent of parents of the subjected school children was obtained before the study.
RESULTS
Reliability
The internal consistency for the total scale was 0.95 for the normative group and 0.98 for the traumatized group. The Cronbach's alpha for the clinical scales varied between 0.85 (Ang) and 0.79 (Sc) in the normative group, and between 0.92 (Anx) and 0.90 (Dep) in the traumatized group (Table 3). Lower Cronbach's alphas were seen in the Dis-f (0.51) and Sc-D (0.66) subscales in the normative group.
Table 3.
Reliability of the TSCC Scales in the normative group and the traumatized group in this study and Briere's study
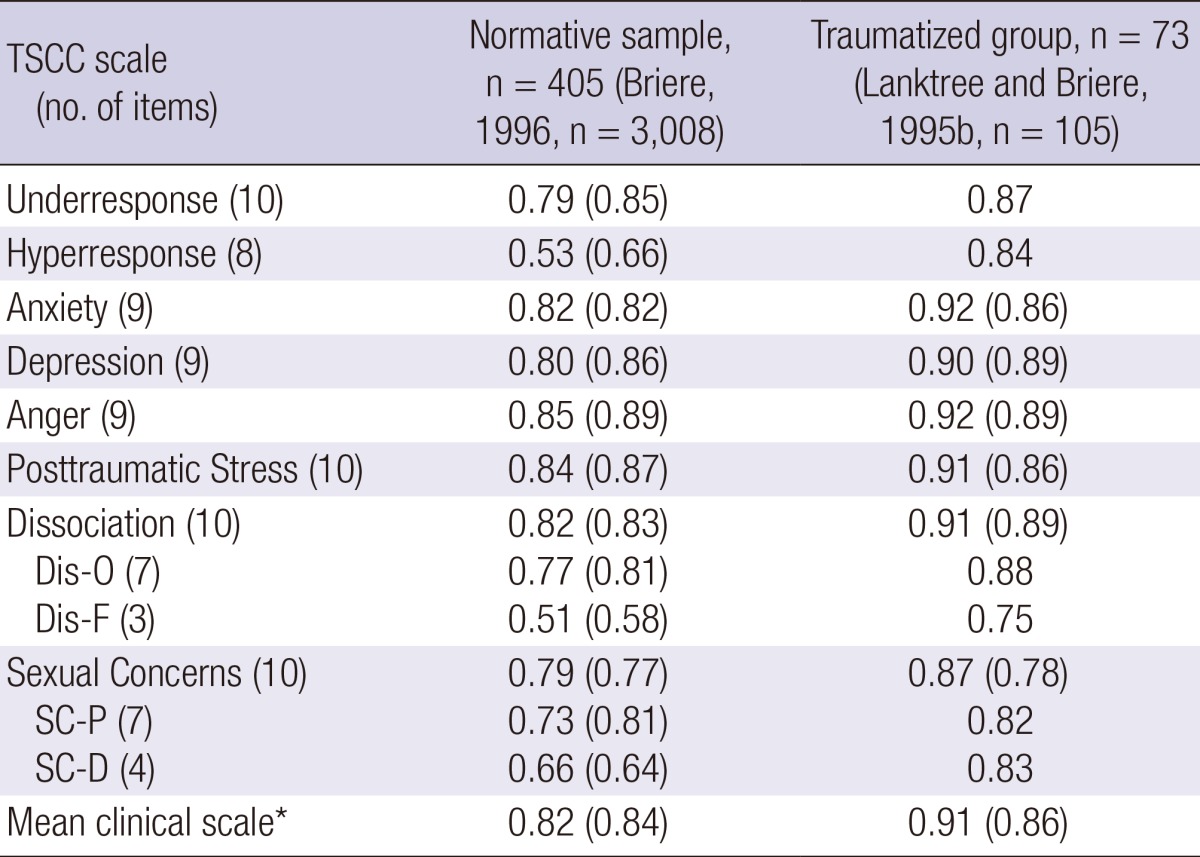
For the two validity scales (UND and HYP) and the four clinical subscales (DIS-O, DIS-F, SC-P, SC-D) for the child abuse center in Lanktree and Briere, 1995, reliability was not reported. *Mean a across six TSCC clinical scales (subscales not included). TSCC, Trauma Symptom Checklist for Children; DIS-O, Overt Dissociation; DIS-F, Fantasy; SC-P, Sexual Preoocupation; SC-D, Sexual Distress.
Test-retest reliability
When test-retest reliability (n=76, mean=11.0, SD=2.3) was examined, r was 0.91 for the total scale and r was 0.87 for the clinical Anxiety scale, 0.81 for the Depression scale, 0.82 for the Anger scale, 0.81 for the Posttraumatic stress scale, 0.89 for the Dissociation scale (Dissociation-overt, r=0.83; Dissociation-fantasy, r=0.72) and 0.75 for the Sexual Concerns scale (Sexual concerns-preoccupation, r=0.72; Sexual concerns-distress, r=0.71). Underresponse had an r of 0.71, and hyperresponse had an r of 0.70 (Table 4).
Table 4.
Test-retest reliability of the TSCC scales (n = 76, mean = 11.0, SD = 2.31)

Pearson correlation 2-tailed significance set at P<0.05 for all. Und, Underresponse; Hyp, Hyperresponse; Anx, Anxiety; Dep, Depression; Anx, Anger; Pts, Posttraumatic Stress; Dis, Dissociation; Dis-O, Overt Dissociation; Dis-F, Fantasy; Sc, Sexual Concerns; Sc-P, Sexual Preoccupation; Sc-D, Sexual Distress; TSCC, Trauma Symptom Checklist for Children.
Validity
Construct validity
Factor analysis
Exploratory and a confirmatory factor analyses of the total population, including the normative group and the traumatized group, were conducted to investigate the construct of the Korean version of the TSCC. The exploratory factor analysis yielded nine factors with an eigenvalue over 1, which explained 55.1% of the variance. Confirmatory factor analysis (six factors) explained 51.1% of the variance. The confirmatory factor analysis resulted in a structure similar to Briere's, 1996 (19) proposed six-factor structure (Table 2).
The first and strongest factor explained 10.6% of the variance. Seven items, all from the original Posttraumatic stress scale belonged to this factor. The second factor explained 10.2% of the variance. Nine items, all from the original Anger scale, belonged to this factor and one item originally belonging to the Sexual Concern subscale was also included in the second factor. The third factor explained 9.5% of the variance. In this factor, ten items were included and all items fit within the theoretical construct of Dissociation. All items had a factor loading above 0.30. The fourth factor explained 8.5% of the variance. All nine items from the theoretical factor Depression loaded highest on this factor. The fifth factor explained 7.4% of the variance. All nine items from the theoretical factor Sexual concern loaded highest in this factor and well above a factor loading of 0.30. The one other item loaded high in the Anger scale. Finally, the sixth factor explained 4.9% of the variance. All items from the theoretical factor Anxiety loaded highest on this factor and above 0.30.
Correlations between the subscales and the total scale
The correlations between the clinical scales and the total scale varied between 0.71 (Sc) and 0.90 (Dep). The correlations between all the subscales are presented in Table 5.
Table 5.
Correlation between the scales, subscales, and the total scale of the TSCC
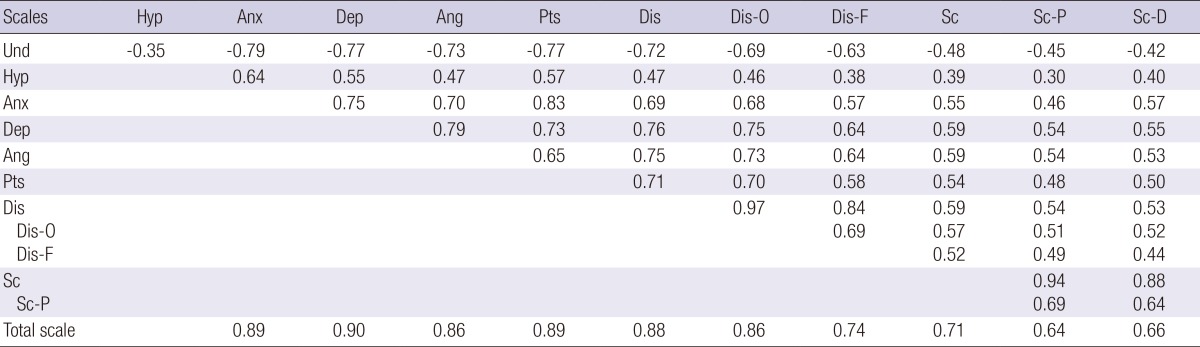
Pearson correlation 2-tailed significance set at P<0.05 for all. Und, Underresponse; Hyp, Hyperresponse; Anx, Anxiety; Dep, Depression; Ang, Anger; Pts, Posttraumatic stress; Dis, Dissociation; Dis-O subscale, Dissociation-overt; Dis-F subscale, Dissociation-fantasy; Sc, Sexual Concern; Sc-P subscale, Sexual-preoccupation; Sc-D subscale, Sexual-distress; Und, Underresponse; TSCC, Trauma Symptom Checklist for Children.
Concurrent validity
In the normative group, 405 students had also completed the CDI and STAI-C. In order to establish concurrent validity, their total scores on the CDI and TAIC were correlated with the Dep and Anx subscales on the TSCC. The correlation coefficients (Pearson's r) were found to be 0.55 and 0.74, respectively (Table 6).
Table 6.
TSCC clinical scale correlations with the CDI and the STAIC scores in a normative sample
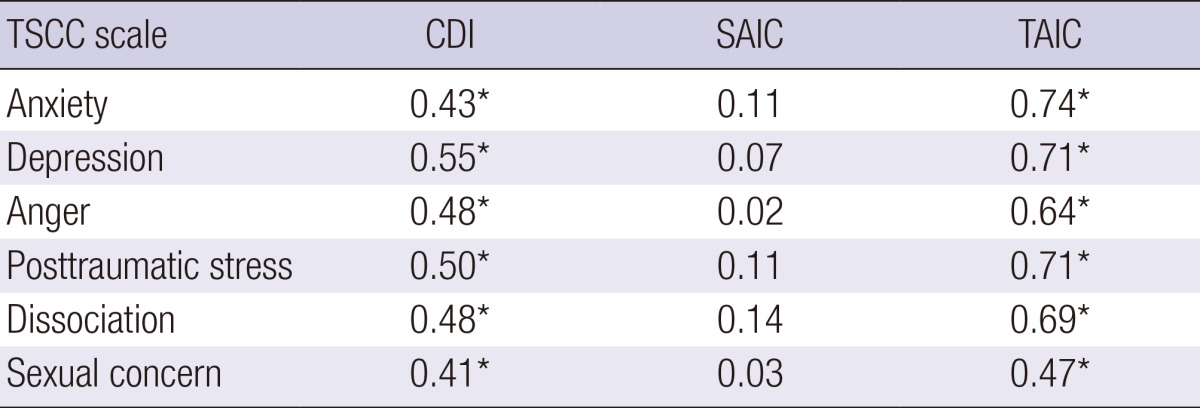
All correlations significant at P<0.05 except for SAIC. *P<0.05, n=405. TSCC, Trauma Symptom Checklist for Children; CDI, Children's Depression Inventory; SAIC, State Anxiety Inventory for Children; TAIC, Trait Anxiety Inventory for Children.
Means in the normative group
The means and standard deviations found in the normative group are shown in Table 7. There were no significant differences (ANOVA) between boys and girls in the normative group on any of the clinical scales. Considering two age groups, the means for Sexual concerns-preoccupation was higher in male (1.5±2.4) than in female (0.6±1.3) (P=0.002) and the means Underresponse validity scale was higher in male (6.8±3.0) than in female (6.0±2.5) (P=0.04) in adolescence group. The older boys scored higher on Sc (P<0.001) and Dis (P=0.02) than the younger boys, and the older girls scored higher on Anx (P=0.02), Dep (P=0.001), Ang (P=0.01), and Dis (P<0.001), except for Sc and Pts than the younger girls.
Table 7.
Differences in the means of subscales of the TSCC between the normative group and the traumatized group in our study and those in Briere's study in 1996
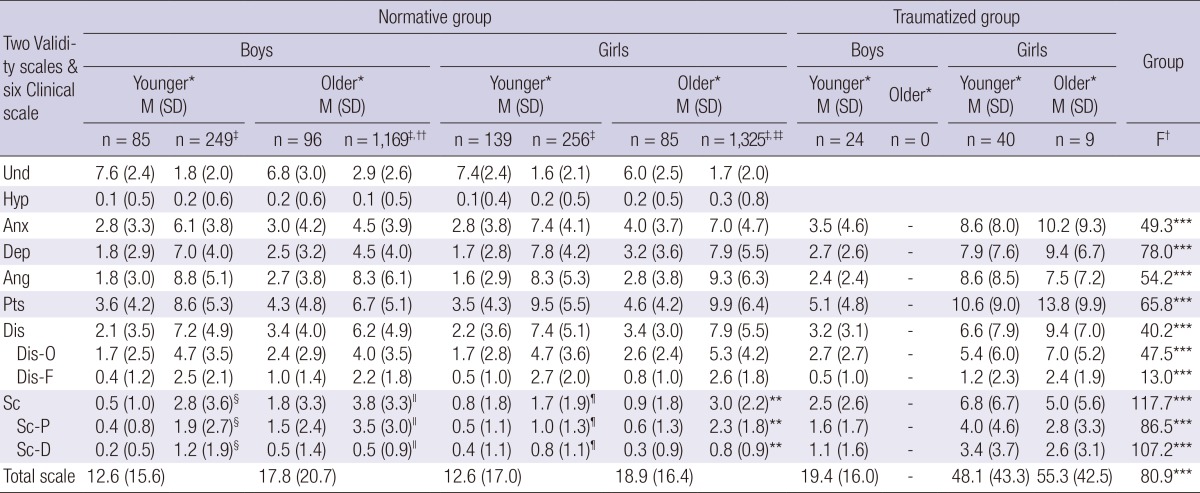
*Age in two groups, 8-12 (younger) and 13-16 (older) years of age; †Analysis of covariance (ANCOVA) with each clinical scale and subscales, as well as the total scale as a dependent variable, each group as an independent factor, and gender and age as covariances. Graded area: data from our study; ‡Data from Briere's study, 1996; §n=71; ∥n=39; ¶n=65; **n=46; ††n=ranged from 1139 to 1169; ‡‡n=ranged from 1289 to 1325. ***P<0.01. TSCC, Trauma Symptom Checklist for Children; Und, Underresponse; Hyp, Hyperresponse; Anx, Anxiety; Dep, Depression; Ang, Anger; Pts, Posttraumatic stress; Dis, Dissociation; Dis-O subscale, Dissociation-overt; Dis-F subscale, Dissociation-fantasy; Sc, Sexual Concerns; Sc-P subscale, Sexual-preoccupation; Sc-D subscale, Sexual-distress.
Differences between the normative group and the traumatized group
As shown in Table 7, there were significant differences between the normative and the traumatized groups on each of the clinical scales and subscales when adjusting for gender and age. There were only younger boys in sexually traumatized group.
DISCUSSION
This study showed that the Trauma Symptom Checklist for Children could be translated into Korean and used in the Korean culture outside of English-speaking society and still maintained its psychometric properties. This is the first study using the Trauma Symptom Checklist for Children in a Korean population of normal and traumatized children and adolescents.
Our experience is that the TSCC is easy to administer and is readily understood by the normal group and the traumatized group studied. This increases the usefulness of the TSCC as a screening instrument for clinicians in their planning for diagnostic procedures and treatment in their clinical and research work.
The psychometric properties of the Korean translation of the TSCC were good. The total scale and the clinical scales in our study had approximately the same internal consistency as Briere (20) reported from a normative sample and from a child abuse center in the Lanktree and Briere's sample (35) (Table 3). The lowest Cronbach's alpha coefficient was found in the Dis-F scale in both studies. Our sample size (n=405) was smaller than Briere's (n=3,008), which explains our slightly lower alpha coefficients for every scale except sexual concerns (SC). Although the sample size in our traumatized group (n=75) was the smallest and larger sample sizes tend to show higher alpha coefficients, all of the coefficients in our traumatized group were higher than those of the normative group (n=405) in our sample and also higher than those of Lanktree and Briere's sample (n=105) (35). This means that the Korean version of the TSCC is more reliable in a target population of children and adolescents with sexual trauma. The internal consistency of the Swedish sample (n=728, aged 10-17) was 0.94 for the total scale, and varied between 0.78 to 0.85 in the normative group and between 0.74 to 0.89 in the traumatized group for the clinical scales, which was similar to our results (35).
Conclusion from our study is that the internal consistency of the TSCC is high and satisfactory in both the normative and traumatized population, and is similar to other published studies. The test-retest reliability was found to be high (0.85), which had not been reported in the Briere's study (Table 4). The test-retest reliability in Swedish version was r=0.81 (n=79 of 728 aged 10 to 17) (35).
In order to study the construct validity, confirmatory factor analysis was performed, and our interpretation of the outcome was similar to Briere's (23) factors, excepting one item on the Sexual Concerns subscale. Item 4 was 'wanting to say dirty words.' was seen as being restricted to the 'Anger' subscale instead of being a part of the 'Sexual Concerns' subscale as it is in the original English version. One explanation for this could be cultural difference. In Confucian culture in Korea, 'dirty words' was extremely prohibited in public and might be considered as very aggressive attitude instead of 'Sexual Concerns'. Unlike Swedish version in which Anxiety subscale did not show up as expected, Korean version came close to all Briere's factors (35).
Concurrent validity was studied comparing the Depression subscale and the Anxiety subscale with the CDI and STAI-C. The Anxiety scale of the TSCC was correlated with the Trait anxiety subscale of the STAI-C. The anxiety scale of the TSCC is associated with trait anxiety, not state anxiety. Correlation coefficients for the CDI ranged from 0.43 to 0.55 in our sample and from 0.45 to 0.68 in Briere's report, with the exception of the Sexual Concerns scale (20). The coefficient for the Sexual Concerns was 0.41 in our study; there was no report of it in Briere's study. In Briere's study, the Revised Children's Manifest Anxiety Scale (RCMAS) was used to assess concurrent validity and the correlation coefficients ranged from 0.51 to 0.63. The correlation coefficients with the TAIC ranged from 0.64 to 0.74 in our study. The Sexual Concerns scale was not reported in Briere's study and had a correlation coefficient of 0.47 in our study. Therefore, concurrent validity of the Korean version of the TSCC was shown as above.
Significantly higher mean scores were found for the traumatized group in the total scale and all of the clinical scales compared to the normative group in our study, which demonstrated the discriminant validity of the Korean version of the TSCC. However, a comparison of the means of the TSCC in our sample with those in Briere's report (20) and Swedish sample (39) showed that the means in our study were substantially lower for all of the clinical scales for all ages and gender categories in the normative group. In our sample, there was a much higher score in the underresponse validity scale than in Briere's report. This result suggests a pattern of symptom underreporting in our study group, which was also reported in the development of the Korean version of the Adolescent Dissociative Experience Scale (39) and of the 20-Item Toronto Alexithymia Scale in Korean Adolescents (40). Culturally, Korea is the one of the countries showing a response bias toward giving the most socially desirable answer, and Korean adolescents perceived their health risk likelihood and rated the chances of most health problems happening to them as significantly lower than a group of Austrians in a previous study (41). This cultural context should be considered when determining culturally-specific norms (scores). Another explanation for the difference in means between the studies was the sampling procedure. Briere (20) combined a school and a medical waiting room sample rather than using a classroom school sample as in our study. This medical waiting-room sample of children could have included a more problematic population than a classroom sample.
In previous studies, there were significantly higher means in girls than in boys in the normative group except SC where adolescent boys normally scored significantly higher. In our study, there was no such gender difference but still higher SC-preoccupation score in adolescent boys in normative group. The girls tended to score higher as they grew older except SC in Swedish sample and in traumatized group in our study (39). In traumatized group, there was significant gender difference (P<0.001) and age difference in girls (P<0.01). Why there was no difference between gender in normative group was not fully understood but a pattern of under reporting symptoms could be one explanation.
The study has two limitations. First, the sample is not a representative national sample, since other large cities in Korea were not included in this study. To establish national norms for the Korean version of the TSCC, a larger sample would be needed. A second limitation is that only sexually traumatized children and adolescents were included in our traumatized sample. The need for Korean screening tools for posttraumatic stress symptoms has been in high demand and urgently needed, especially for sexually abused children. The Korean version of the TSCC has been shown to be a proper screening tool for this purpose.
In conclusion, this initial validation study shows the Korean version of the TSCC to be a promising measure of posttraumatic stress symptoms in Korean children and adolescents. It has been shown to be psychometrically appropriate and will be a useful self-reporting instrument for Korean clinicians. The TSCC is useful in identifying traumatic symptoms in children and adolescents who have been traumatized, and specifically for children and adolescents who have been sexually abused. It is valuable to have a screening tool for clinical practice in order to provide proper therapeutic help for children and adolescents.
ACKNOWLEDGMENT
Thank you for two Clinical Psychologists, Min-A Kang and Hae-Jung Kim, other precious colleague and child sexual abuse victims treated in Sunflower Child Center, Daegu Gyeongbuk Child Sexual Abuse Response Center, in Daegu, Korea.
Footnotes
The author has no conflicts of interest to disclose.
This work was supported by Biomedical Research Institute grant, Kyungpook National University Hospital (2007).
References
- 1.American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. Washington, D.C.: American Psychiatric Association; 1994. [Google Scholar]
- 2.Nader KO. Assessing traumatic experiences in children. In: Wilson JP, Keane TM, editors. Assessing psychological trauma and PTSD. New York: Guilford Press; 1997. pp. 291–348. [Google Scholar]
- 3.National Center for Post Traumatic Stress Disorder. Fact sheet and child measures. [accessed on 6 August 2006]. Available at http://www.ncptsd.vagov/fact/specific/fschildren.html.
- 4.Fergusson DM, Horwood LJ, Lynskey MT. Childhood sexual abuse and psychiatric disorder in young adulthood: II. psychiatric outcomes of childhood sexual abuse. J Am Acad Child Adolesc Psychiatry. 1996;35:1365–1374. doi: 10.1097/00004583-199610000-00024. [DOI] [PubMed] [Google Scholar]
- 5.Flannery DJ, Singer MI, Wester K. Violence exposure, psychological trauma, and suicide risk in a community sample of dangerously violent adolescents. J Am Acad Child Adolesc Psychiatry. 2001;40:435–442. doi: 10.1097/00004583-200104000-00012. [DOI] [PubMed] [Google Scholar]
- 6.Ford JD. Traumatic victimization in childhood and persistent problems with oppositional-defiance. J Aggress Maltreat Trauma. 2002;6:25–58. [Google Scholar]
- 7.Guterman NB, Cameron M, Hahm HC. Community violence exposure and associated behavior problems among children and adolescents in residential treatment. J Aggress Maltreat Trauma. 2003;6:111–136. [Google Scholar]
- 8.Johnson JG, Cohen P, Gould MS, Kasen S, Brown J, Brook JS. Childhood adversities, interpersonal difficulties, and risk for suicide attempts during late adolescence and early adulthood. Arch Gen Psychiatry. 2002;59:741–749. doi: 10.1001/archpsyc.59.8.741. [DOI] [PubMed] [Google Scholar]
- 9.Maida CA, Gordon NS, Strauss G. Child and parent reactions to the Los Angeles Area Whittier Narrows Earthquake. J Soc Behav Pers. 1993;8:421–436. [Google Scholar]
- 10.Saltzman WR, Pynoos RS, Layne CM, Steinberg AM, Aisenberg E. Trauma-and grief-focused intervention for adolescents exposed to community violence: results of a school-based screening and group treatment protocol. Group Dyn. 2001;5:291–303. [Google Scholar]
- 11.Fricker AE, Smith DW. Trauma specific versus generic measurement of distress and the validity of self-reported symptoms in sexually abused children. J Child Sex Abus. 2001;10:51–66. [PubMed] [Google Scholar]
- 12.McLeer SV, Deblinger E, Atkins MS, Foa EB, Ralphe DL. Post traumatic stress disorder in sexually abused children. J Am Acad Child Adolesc Psychiatry. 1988;27:650–654. doi: 10.1097/00004583-198809000-00024. [DOI] [PubMed] [Google Scholar]
- 13.Wolfe DA, Sas L, Wekerle C. Factors associated with the development of posttraumatic stress disorder among child victims of sexual abuse. Child Abuse Negl. 1994;18:37–50. doi: 10.1016/0145-2134(94)90094-9. [DOI] [PubMed] [Google Scholar]
- 14.Armstrong JG, Putnam FW, Carlson EB, Libero DZ, Smith SR. Development and validation of a measure of adolescent dissociation: the Adolescent Dissociative Experiences Scale. J Nerv Ment Dis. 1997;185:491–497. doi: 10.1097/00005053-199708000-00003. [DOI] [PubMed] [Google Scholar]
- 15.Wolfe VV. Measuring post-traumatic stress disorder: the Children's Impact of Traumatic Events Scale - revised. APSAC Advis. 1996;9:25–26. [Google Scholar]
- 16.Wolfe VV, Gentile C, Michienzi T, Sas L, Wolfe DA. The children's impact of traumatic events scale: a measure of post-sexual-abuse PTSD symptoms. Behav Assess. 1991;13:359–383. [Google Scholar]
- 17.Jin Y, Chung US, Jeong SH, Lee WK. The reliability and validity of the Korean version of the child sexual behavior inventory. Psychiatry Investig. 2013;10:336–345. doi: 10.4306/pi.2013.10.4.336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Putnam FW, Helmers K, Trickett PK. Development, reliability, and validity of a child dissociation scale. Child Abuse Negl. 1993;17:731–741. doi: 10.1016/s0145-2134(08)80004-x. [DOI] [PubMed] [Google Scholar]
- 19.Briere J. Trauma Symptom Checklist for Children (TSCC) professional manual. Odessa: Psychological Assessment Resources; 1996. [Google Scholar]
- 20.Briere J. Trauma Symptom Checklist for Young Children (TSCYC) professional manual. Odessa: Psychological Assessment Resources; 2005. [Google Scholar]
- 21.Bal S, Crombez G, Van Oost P, Debourdeaudhuij I. The role of social support in well-being and coping with self-reported stressful events in adolescents. Child Abuse Negl. 2003;27:1377–1395. doi: 10.1016/j.chiabu.2003.06.002. [DOI] [PubMed] [Google Scholar]
- 22.Bal S, Van Oost P, De Bourdeaudhuij I, Crombez G. Avoidant coping as a mediator between self-reported sexual abuse and stress-related symptoms in adolescents. Child Abuse Negl. 2003;27:883–897. doi: 10.1016/s0145-2134(03)00137-6. [DOI] [PubMed] [Google Scholar]
- 23.Brady KL, Caraway SJ. Home away from home: factors associated with current functioning in children living in a residential treatment setting. Child Abuse Negl. 2002;26:1149–1163. doi: 10.1016/s0145-2134(02)00389-7. [DOI] [PubMed] [Google Scholar]
- 24.Shaw JA, Lewis JE, Loeb A, Rosado J, Rodrigues RA. Child on child sexual abuse: psychological perspectives. Child Abuse Negl. 2000;24:1591–1600. doi: 10.1016/s0145-2134(00)00212-x. [DOI] [PubMed] [Google Scholar]
- 25.Shaw JA, Lewis JE, Loeb A, Rosado J, Rodrigues RA. A comparison of Hispanic and African-American sexually abused girls and their families. Child Abuse Negl. 2001;25:1363–1379. doi: 10.1016/s0145-2134(01)00272-1. [DOI] [PubMed] [Google Scholar]
- 26.Cohen JA, Mannarino AP, Knudsen K. Treating sexually abused children: 1 year follow-up of a randomized controlled trial. Child Abuse Negl. 2005;29:135–145. doi: 10.1016/j.chiabu.2004.12.005. [DOI] [PubMed] [Google Scholar]
- 27.Lanktree CB, Briere J. Outcome of therapy for sexually abused children: a repeated measures study. Child Abuse Negl. 1995;19:1145–1155. doi: 10.1016/0145-2134(95)00075-j. [DOI] [PubMed] [Google Scholar]
- 28.Nolan M, Carr A, Fitzpatrick C, O'Flaherty A, Keary K, Turner R, O'Shea D, Smyth P, Tobin G. A comparison of two programs for victims of child sexual abuse. Child Abuse Rev. 2002;11:103–123. [Google Scholar]
- 29.Elhai JD, Gray MJ, Kashdan TB, Franklin LC. Which instruments are most commonly used to assess traumatic event exposure and posttraumatic effects? a survey of traumatic stress professionals. J Trauma Stress. 2005;18:541–545. doi: 10.1002/jts.20062. [DOI] [PubMed] [Google Scholar]
- 30.Balaban V. Psychological assessment of children in disasters and emergencies. Disasters. 2006;30:178–198. doi: 10.1111/j.0361-3666.2006.00314.x. [DOI] [PubMed] [Google Scholar]
- 31.Daegu Statistical Information. Statistics. [accessed on 31 December 2008]. Available at http://www.Daegu.Daegu.go.kr/Administrative/Resident_Registration.aspx.
- 32.Crouch JL, Smith DW, Ezzell CE, Saunders BE. Measuring reactions to sexual trauma among children: comparing the children's impact of traumatic events scale and the trauma symptom checklist for children. Child Maltreat. 1999;4:255–263. [Google Scholar]
- 33.Sadowski CM, Friedrich WN. Psychometric properties of the Trauma Symptom Checklist for Children (TSCC) with psychiatrically hospitalized adolescents. Child Maltreat. 2000;5:364–372. doi: 10.1177/1077559500005004008. [DOI] [PubMed] [Google Scholar]
- 34.Lanktree CB, Briere J. Early data on the new Sexual Concerns and Dissociation subscales of the TSCC: unpublished manuscript, Department of Psychiatry, University of Southern California School of Medicine. In: Briere J, editor. Trauma Symptom Checklist for Children (TSCC) professional manual. Odessa: Psychological Assessment Resources; 1995. [Google Scholar]
- 35.Nilsson D, Wadsby M, Svedin CG. The psychometric properties of the Trauma Symptom Checklist For Children (TSCC) in a sample of Swedish children. Child Abuse Negl. 2008;32:627–636. doi: 10.1016/j.chiabu.2007.09.009. [DOI] [PubMed] [Google Scholar]
- 36.Kovacs M. Rating scales to assess depression in school-aged children. Acta Paedopsychiatr. 1981;46:305–315. [PubMed] [Google Scholar]
- 37.Kovacs M. Children's Depression Inventory (CDI) Ontario: Multi-Health Systems Inc.; 1992. [Google Scholar]
- 38.Spielberger CD, Gorsuch RL, Lushene RE. Manual for the State-Trait Anxiety Inventory. Palo Alto: Consulting Psychologists Press; 1970. [Google Scholar]
- 39.Shin JU, Jeong SH, Chung US. The Korean version of the adolescent dissociative experience scale: psychometric properties and the connection to trauma among Korean adolescents. Psychiatry Investig. 2009;6:163–172. doi: 10.4306/pi.2009.6.3.163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Seo SS, Chung US, Rim HD, Jeong SH. Reliability and validity of the 20-item toronto alexithymia scale in Korean adolescents. Psychiatry Investig. 2009;6:173–179. doi: 10.4306/pi.2009.6.3.173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Kim Y. Australian and Korean adolescents' perceived health risk. Psychol Rep. 2007;101:816–822. doi: 10.2466/pr0.101.3.816-822. [DOI] [PubMed] [Google Scholar]