

Abstract
We analyzed national data collected by the Health Insurance Review and Assessment Service in Korea from 2007 to 2011; 1) to document procedural numbers and procedural rate of bipolar hemiarthroplasty (BH), primary and revision total hip arthroplasties (THAs), 2) to stratify the prevalence of each procedure by age, gender, and hospital type, and quantified, 3) to estimate the revision burden and evaluate whether the burden is changed over time. Our final study population included 60,230 BHs, 40,760 primary THAs, and 10,341 revision THAs. From 2007 to 2011, both the number and the rate of BHs, primary THAs increased steadily, whereas there was no significant change in revision THAs. Over the 5 yr, the rate of BHs and primary THAs per 100,000 persons significantly increased by 33.2% and 21.4%, respectively. The number of revision THAs was consistent over time. The overall annual revision burden for THA decreased from 22.1% in 2007 to 18.9% in 2011. In contrast to western data, there were no changes in the number and rate of revision THAs, and the rates of primary and revision THAs were higher for men than those for women. Although 5 yr is a short time to determine a change in the revision burden, there have been significant decreases in some age groups.
Graphical Abstract
Keywords: Epidemiology, Hip, Arthroplasty, Prevalence
INTRODUCTION
Total hip arthroplasty (THA) has promising outcomes in the treatment of end stage hip disease, which had led to its increased popularity in most western countries over the past decade (1, 2, 3, 4, 5, 6, 7, 8). Some previous studies also showed a steady increase in the annual incidence of revision THA, despite continual development in implant design, bearing couples, and surgical technique (1, 2, 4, 8). Conversely, results from the Norwegian Arthroplasty Register reported a decreased THA revision risk (9). These population-based epidemiological studies can provide important information about national trends of hip replacements as well as public health costs, which are needed to establish healthcare policies.
Western epidemiological data cannot be directly applied to Asian countries. Some studies have shown disparities in the rate of THA based on ethnicity (10, 11). There are two previous epidemiological studies from Asian countries (12, 13). One performed in Korea reported a relatively low rate of THA compared to western countries and increased annual incidence of THA from 2002 to 2006 (13). However, the study was limited to primary THA for patients with osteoarthritis and did not determine the prevalence and trends of revision THA. The other study performed in Taiwan reported on the use of partial hip replacement, primary, and revision THAs; different epidemiology of hip disease was evident between Han Chinese and Caucasians (12). This study was based on a national health insurance research database over the 9-yr period; however, trends by age and gender as well as revision burden were not documented.
The purpose of this study was to analyze national data collected by the Health Insurance Review and Assessment Service (HIRA) in South Korea from 2007 to 2011 and to document procedural numbers and the procedural rate of primary and revision THA stratified by age, gender, and hospital type. We also quantified the revision burden and evaluated whether the burden changed over time. Data of bipolar hemiarthropalsty (BH) use was also analyzed by same methods because the utilization of BH has recently increased to treat the increased number of patients with hip fractures in Korea (14, 15), and some portion of revision THA may be attributed to failed BHs. We therefore determined 1) whether the use of hip replacements (BH, primary, and revision THAs) and revision burden stratified by gender and age have increased over time, and 2) whether the epidemiological findings in Korea are different from data in western countries. We also determined 3) whether an increasing proportion of procedures had been performed with time by higher volume hospitals, such as tertiary and general hospitals.
MATERIALS AND METHODS
Data sources
The Korean HIRA database includes medical claims for all Korean citizens. In Korea, 97% of the population is legally obliged to enroll in the Korea National Health Insurance Program (KNHIP). Patients pay on average 30% of total medical costs to clinics or hospitals. All clinics and hospitals then submit claims data for inpatient and outpatient care including diagnoses (coded according to the International Classification of Disease, Tenth Revision, Clinical Modification [ICD-10-CM]), procedures, prescription records, demographic information, and direct medical costs to HIRA to obtain 70% reimbursement of the total medical costs from the government. The remaining 3% of the population not insured by a KNHIP are covered by a Medical Aid program. Claims data covered by Medical Aid program are also reviewed by HIRA. Thus, almost all information about patients and their medical records is available from the HIRA database. Hip replacements were identified by their principal procedure codes in the HIRA database. Surgical procedures in Korea are translated from the Electronic Data Interchange code of the KNHIP. Records with the procedure codes of BH (N0715), primary THA (N0711), and revision THA (N1711 and N1721) were selected. Femoral and acetabular component revision THAs (N1715 and N1725) were also included as revision THA. Primary ICD-10-CM diagnostic codes were analyzed to determine the most common underlying diagnoses for hip replacements. The average length of hospital stay and total inpatient hospitalization cost were also determined for each procedure.
Data and statistical analyses
We calculated the number of hip replacement procedures according to age, gender, and hospital type. Age categories in yr are the same as were used previously (i.e., <45, 45-64, 65-74, 75-84, and ≥85) (1). In Korea, the hospital type is classified as clinics, hospital, general hospital, and tertiary hospital. Clinics mainly focus on outpatient care but are legally allowed to have up to 29 inpatients beds. Hospitals have a minimum of 30 inpatients beds and general hospitals are institutions that have a minimum of 100 inpatients beds and provide physician specialist services in major areas. Tertiary hospitals indicate general hospitals that are approved to provide most types of advanced medical care and treat severely ill patients with a minimum of 20 departments. The rate of hip replacements was calculated by dividing the number of surgical procedures by the corresponding year-specific Korean population based on a census database managed by the National Statistical Office and then adjusting to the rate per 100,000 persons. We also evaluated the change in the procedural rate from 2007 to 2011. A Poisson regression analysis was used to estimate the magnitude of the annual change in the procedural rate (rate ratio). Briefly, if there is no change in the procedural rate over time, the rate ratio will be 1.0. A rate ratio exceeding 1.0 suggests a procedural rate that is increasing over time. By examining the magnitude of this rate ratio and testing it against the null value of 1.0, we could evaluate whether there were significant changes in procedural rates over the 5 yr study period. The effects of age and gender on procedural rates of hip replacements were evaluated. In addition, the annual change rates of hip replacements were assessed using a simple linear regression, stratified by age and/or gender group. The annual revision burden was calculated by dividing the number of revision THAs by the total number of primary and revision THAs (16). The revision burden was stratified by both age and gender. Simple linear regression was used to evaluate the year-to-year change in the burden. Similarly, the change of procedural rates according to type of hospital was examined with the simple linear regression.
Ethics statement
This study protocol was exempted for review by the institutional review board of the Seoul National University Hospital (E-1401-049-547) in accordance with the exemption criteria, and approved by institutional reiew board of NECA (NECAIRB12-004).
RESULTS
Epidemiology of hip replacements and the revision burden
Our final study population included 60,230 BHs, 40,760 primary THAs, and 10,341 revision THAs. The demographic characteristics of patients undergoing hip replacements are summarized in Tables 1 and 2.
Table 1.
Number of hip replacements in Korea from 2007 to 2011
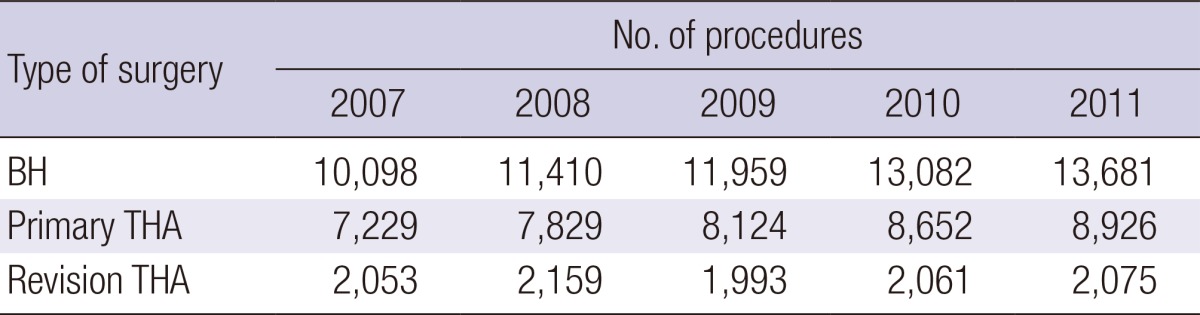
BH, bipolar hemiarthropalsty; THA, total hip arthroplasty.
Table 2.
Demographic characteristics of patients who had hip replacements
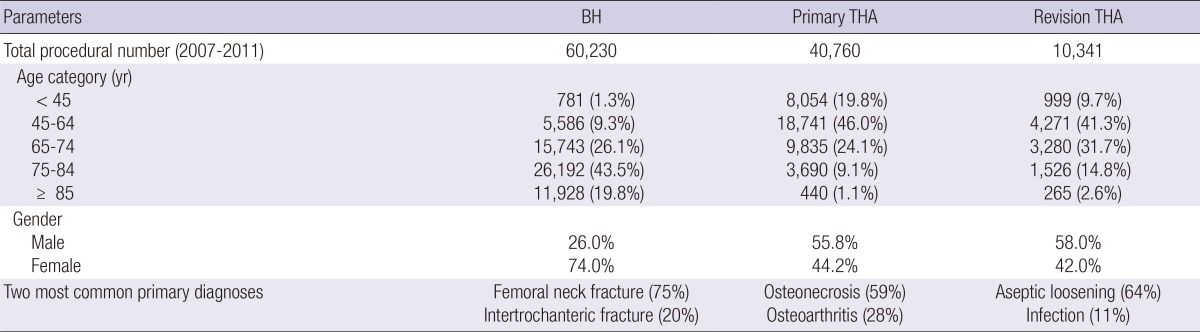
BH, bipolar hemiarthropalsty; THA, total hip arthroplasty.
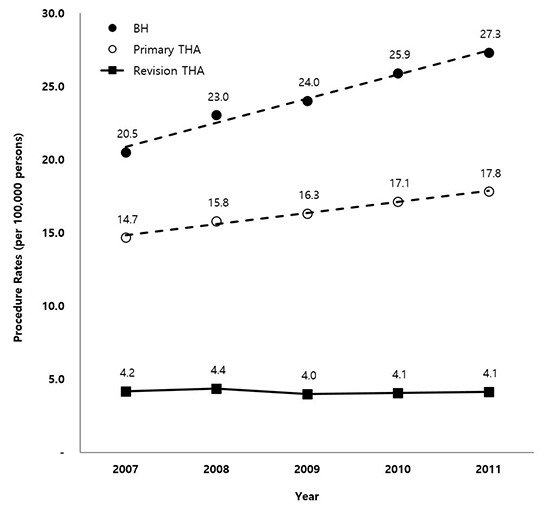
Between 2007 and 2011, both the number and the rate of BHs and primary THAs increased substantially, whereas there was no significant change in the number and rate of revision THAs. Over the 5 yr, the rates of both BHs and primary THAs significantly increased by 33.2% (20.5 per 100,000 in 2007 to 27.3 per 100,000 in 2011) and 21.4% (14.7 per 100,000 in 2007 to 17.8 per 100,000 in 2011), respectively (P<0.001). However, the rate of revision THAs remained at an average of 4.2 per 100,000 (range, 4.0 to 4.4 per 100,000). The rate of BH and primary THA increased by 1.7 and 0.8 procedures per 100,000 persons per year, respectively (Fig. 1).
Fig. 1.

Procedural rates of bipolar hemiarthroplasty, primary, and revision total hip arthroplasties in Korea from 2007 to 2011.
Overall, 63% of patients treated with BH were ≥75 yr of age, while 66% and 51% of patients treated with primary and revision THAs were <65 yr of age, respectively (Table 2). The rate of BHs significantly increased in those ≥65 yr of age (P<0.001) (Fig. 2), with females displaying a consistent 2.9-times higher rate throughout the 5-yr period. The rate of primary THAs significantly increased in all age groups (P<0.01), except those ≥85 yr of age (Fig. 3), and a consistent 1.3-times higher male prevalence was evident. Although the overall rate of revision THAs remained constant over time, a significant decrease in the rate was found in those <65 yr of age (P<0.003), and males displayed a consistent 1.4-times higher revision THA rate (Fig. 4).
Fig. 2.

Procedural rates of bipolar hemiarthroplasty stratified by age group.
Fig. 3.

Procedural rates of primary total hip arthroplasty stratified by age group.
Fig. 4.

Procedural rates of revision total hip arthroplasty stratified by age group.
The primary ICD-10-CM diagnostic codes were identified. The two most common reasons for BH were femoral neck fracture (ICD-10-CM: S720, 75%) and intertrochanteric fracture of the femur (ICD-10-CM: S721, 20%). For primary THA, osteonecrosis (ICD-10-CM: M87, 59%) was the most common diagnosis, followed by osteoarthritis (ICD-10-CM: M16, 28%). Revision THAs were most commonly performed due to aseptic loosening (ICD-10-CM: T840, T848, and T 895, 64%) and infection (ICD-10-CM: T814 and T845, 11%).
Over the 5-yr period, the revision burden for primary THA averaged 20.3% and steadily decreased from 22.1% in 2007 to 18.9% in 2011 (Fig. 5). The linear regression model of year-to-year change in revision burden showed that the revision burden for primary THA remained consistent for men. For women, there were significant annual decreases of 1.97% (95% confidence interval [CI], -3.43 to -0.51) in the less than those 45-yr-of-age and 1.14% (95% CI, -2.11 to -0.16) for those 65 to 74-yr-old (Table 3).
Fig. 5.

The revision burden for primary total hip arthroplasty in Korea from 2007 to 2011.
Table 3.
Annual change in the revision burden of total hip arthroplasty, by age and gender, in Korea from 2007 to 2011(%)
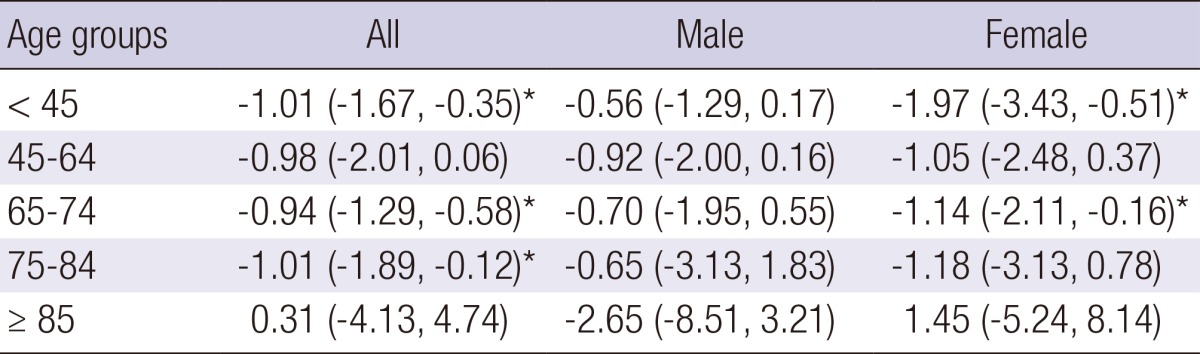
*P value<0.05. BH, bipolar hemiarthropalsty; THA, total hip arthroplasty.
Hospital characteristics
Between 2007 and 2011, BHs were most commonly performed at general hospitals (50.4%), followed by hospitals (30.3%), tertiary hospitals (17.4%), and clinics (1.9%). The number of primary THAs was the greatest in general hospitals (36.1%), followed by tertiary hospitals (33.6%), hospitals (28.8%), and clinics (1.5%). The proportion of primary THAs performed in hospitals increased significantly from 26.1% in 2007 to 30.9% in 2011, whereas the proportion of primary THAs performed in general hospitals significantly decreased from 39.2% in 2007 to 33.8% in 2011. The number of revision THAs was the highest in tertiary hospitals (39.3%), followed by general hospitals (38.1%), hospitals (21.7%), and clinics (0.9%) (Table 4).
Table 4.
National trends of hip replacements according to hospital types in Korea from 2007 to 2011
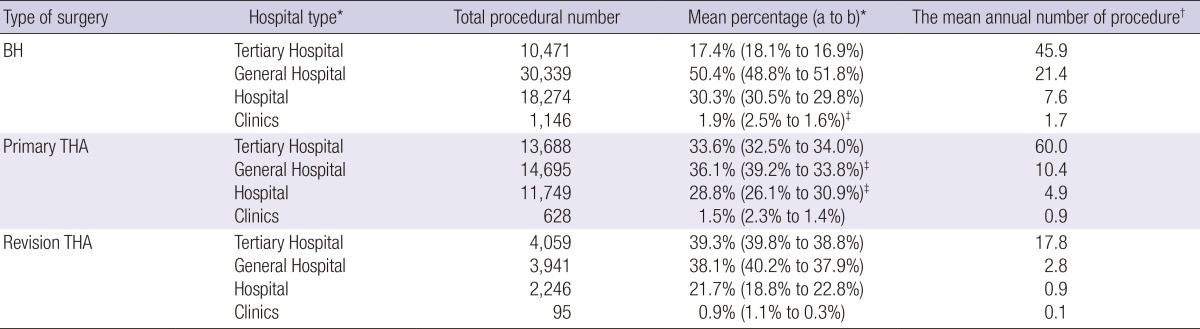
*a, percentage in 2007; b, percentage in 2011. ‡Calculated by dividing total number of each procedure by total number of each hospital type; ‡The change is statistically significant (P<0.05). BH, bipolar hemiarthropalsty; THA, total hip arthroplasty.
The average length of hospital stay for BH, primary THA, partial component revision THA, and all component revision THA was 23.7, 19.6, 23.7, and 26.5 days, respectively. The average inpatient hospital charges for each procedure were consistent during the study period: BH (US $5,947), primary THA (US $6,247), and partial component revision THA (US $5,866), and all component revision THA (US $8,272). The total inpatient hospital charges were increased by 42% (US $58,493,180 in 2007 to US $83,221,020 in 2011) for BH and by 25% (US $44,656,681 in 2007 to US $55,666,826 in 2011) for primary THA. However, that of revision THA remained relatively constant over time, with a mean US $7,582,408 (range, US $7,222,503 to US $8,126,854) The average exchange rate of the South Korean won to the US dollar for 2011 was $1 to ₩1,108, according to the Bank of Korea.
DISCUSSION
Most epidemiological studies from western countries have shown an increased annual incidence of primary THA over the past few decades (1, 2, 3, 4, 5, 6, 7, 17). Our results also indicate that the number and rate of primary THA increased substantially between 2007 and 2011 in Korea. However, the rate of primary THA of 17.8 per 100,000 in 2011 was similar to the annual incidence of primary THA in Taiwan (15 per 100,000 between 1996 and 2004) (12), lower than those reported for the United States (69 per 100,000 in 2002) (1), Iceland (43 per 100,000 in 1982) (2), Denmark (101 per 100,000 in 1996) (4), and England (87 per 100,000 in 1996) (18). Kim et al. (13) reported the rate of primary THA in Korea using a national database from 2002 to 2006 in a previous study. However, the total number and rate reported in their study were much lower than our data because their study focused mainly on primary THAs for osteoarthritis. Although many factors are associated with disparity in the rate of primary THA between western and Asian countries, one reason may be the different indications for primary THAs. Western epidemiological studies showed that more than 75% of primary THAs were performed for osteoarthritis (16, 19), while the most common indication for primary THA in Korea and Taiwan was osteonecrosis of the femoral head (12, 13), which is consistent with our findings. A few studies have reported that the prevalence of hip osteoarthritis in Asian countries (range, 1.2% to 5.4%) was much lower than that of western countries (13, 20, 21). The fact that osteonecrosis of the femoral head affects mostly young male adults within their 3rd to 5th decade may explain why the rate of primary THA in Korea was consistently higher for men than for women in contrast to western data, and why 66% of the patients treated with primary THA were <65-yr-of-age while the majority of patients in western countries were ≥65-yr-of-age (1, 3, 5, 16, 18).
Our results indicate that both the number and rate of BH increased substantially over the 5 yr. It is impossible to compare the nationwide trends and prevalence of BH in Korea with those in western countries because, to our knowledge, no previous epidemiological study focused on BH. The most common indication for BH was hip fractures, therefore our data concurs with the results of two nationwide epidemiological studies for the incidence of hip fractures and trends of surgical treatment in femoral neck fractures conducted in Korea. Two previous studies showed an increasing tendency of hip fractures, especially in women (14, 22), and another documented that the proportion of femoral neck fracture patients who underwent BH increased steadily in Korea from 2006 to 2011 (15). In contrast, the number of hip fractures and the proportion of BH for hip fractures remained nearly the same in the United States between 2000 and 2009 (23). Kannan et al. reported a relatively low revision rate of about 3% of BH over a 5-yr period in western countries, but the risk of revision increased in patients <75-yr-of-age (24). Considering the significant increasing rate of BH even in patients <75-yr-of-age, BH is likely to become a substantial socioeconomic burden due to its future revision in Korea.
In western countries, the rate of revision THA has increased substantially over the past few decades (1, 2, 4, 8), while during this 5-yr period, the rate of revision THA in Korea has remained nearly the same and even significantly decreased in those <65-yr-of-age. However, overall revision burden for primary THA (20.3%) in Korea from 2007 to 2011 was greater than those for western countries (6.4% to 18.3%), and the Korean revision burden of 18.9% in 2011 was comparable with the Australian (18.2% for 1999 through 2002) (25) and Finnish (17.1% for 1999 through 2003) (26) revision burdens. In Sweden, the revision burden of 6.4% for the elderly population (≥65-yr-of-age) was much lower than the 11% reported for the general population (27). In contrast, the revision burden from 2007 to 2011 for the elderly population (≥65-yr-of-age) in Korea (26.6%) was substantially greater than that for the general population (20.3%). This discrepancy between western and Korean revision burden may be partly explained by the different proportion of age groups undergoing primary and revision THAs. The relatively low revision burden for the elderly population in western countries is because the majority of patients undergoing primary THA are elderly (1, 5, 16, 19). Conversely, in Korea the proportion of the elderly population undergoing primary THA was only 34%, although the proportion of the elderly population undergoing revision THA is almost same as that of the other population.
In Korea, 32.2% of BHs and 30.3% of primary THAs were performed in hospitals and clinics, and the mean annual number of each procedure was fewer than 10 procedures. Similarly, 60.7% of revision THAs was performed in general hospitals, hospitals, and clinics that performed fewer than three procedures a year (Table 4). Although it is contentious whether or not hospital volume affects patient outcome (19), an association between higher volume and improved patient outcomes for hip replacements has been reported (8). Based on these data, there have been efforts to regionalize major surgical procedures, such as THA, to higher volume medical centers. A previous study reported minimal evidence of regionalization of THA in the United States between 1991 and 2005 (8). In contrast, we found that the proportion of primary THAs performed in low-volume hospitals substantially increased in Korea during the study period.
The average length of hospital stay for hip replacements in Korea was much longer than those reported in the United States (6.9 days for BH, 4.3 days for primary THA, and 5.9 days for revision THA). Nevertheless, it is noteworthy that the average inpatient hospital charges for each procedure was about 6-times lower than those reported in the United States (19). South Korea has a universal healthcare system controlled by the government and managed under the National Health Insurance Corporation. Since medical care costs are tightly controlled by government, a high supply of health and hospital services can be provided at low prices in Korea.
To our best knowledge, this is the second population-based epidemiological study in Asia, based on the nationwide database to document the longitudinal trends in use of BH, primary, and revision THA in terms of the procedural number and rate, stratified by age and gender (12). However, the present study is the first to document the annual revision burden and the year-to-year change in the burden in Asia stratified by both age and gender. We also reported the change of procedural rates according to type of hospital.
Several limitations in this study should be noted. First, our study was limited in terms of duration because HIRA limited the study period to a maximum of 6 yr. Therefore, our findings over the 5-yr period may not represent longitudinal trends of hip replacements in Korea over a longer period. Second, this was not a registry-based study and thus we could not provide all information associated with each procedure such as type of admission, surgical technique, and outcomes. Third, we could not exactly provide the trends of hospital choice of the patients because we did not exclude several populations in whom surgery is typically more emergent and hospital choice is more limited. Fourth, the comparative rates of primary and revision THAs between countries are not exactly reflected period because of no recent nationwide population-based data is lack at similar period. Fifth, HIRA data cannot explain the diagnosis of primary THA other than osteonecrosis and osteoarthritis and also the causes of revision THA other than infection and loosening, and number of repeated revision correctly. Sixth, the time for search is too short and did not explain the difference of rate of revision THA according to region or hospital.
Our study demonstrates that both the number and rate of BH and primary THA have increased substantially from 2007 to 2011 in Korea. However, the overall rate of revision THA remained constant over time and significant decrease of the rate was found in the younger population. The revision burden for primary THA steadily decreased over the 5-yr period. However, it was still greater than that reported for western countries. In contrast to western countries, primary and revision THAs were performed more commonly in the younger male population, and the proportion of primary and revision THAs performed in low-volume hospitals substantially increased over time. To decrease revision burden in Korea, nationwide efforts should be made by using optimized bearing surfaces in terms of enhancing implant longevity, especially in younger male population at particular risk for mechanical wear of their hip replacements. In addition, a policy increasing regionalization of hip replacements as well as improving quality in lower volume hospitals might be helpful to decrease revision burden in Korea in the future.
ACKNOWLEDGMENTS
We thank Sohee Oh from Department of Biostatistics, Seoul National University Boramae Hospital for statistical advice.
Footnotes
This study was funded by the National Evidence-based Healthcare Collaborating Agency (NECA) (project no. NECA-B-12-003) and by a grant from the Seoul National University Hospital Research Fund (#3020130080).
The authors declare no potential conflicts of interest.
References
- 1.Kurtz S, Mowat F, Ong K, Chan N, Lau E, Halpern M. Prevalence of primary and revision total hip and knee arthroplasty in the United States from 1990 through 2002. J Bone Joint Surg Am. 2005;87:1487–1497. doi: 10.2106/JBJS.D.02441. [DOI] [PubMed] [Google Scholar]
- 2.Ingvarsson T, Hägglund G, Jónsson H, Jr, Lohmander LS. Incidence of total hip replacement for primary osteoarthrosis in Iceland 1982-1996. Acta Orthop Scand. 1999;70:229–233. doi: 10.3109/17453679908997798. [DOI] [PubMed] [Google Scholar]
- 3.Lohmander LS, Engesaeter LB, Herberts P, Ingvarsson T, Lucht U, Puolakka TJ. Standardized incidence rates of total hip replacement for primary hip osteoarthritis in the 5 Nordic countries: similarities and differences. Acta Orthop. 2006;77:733–740. doi: 10.1080/17453670610012917. [DOI] [PubMed] [Google Scholar]
- 4.Pedersen AB, Johnsen SP, Overgaard S, Søballe K, Sørensen HT, Lucht U. Total hip arthroplasty in Denmark: incidence of primary operations and revisions during 1996-2002 and estimated future demands. Acta Orthop. 2005;76:182–189. doi: 10.1080/00016470510030553. [DOI] [PubMed] [Google Scholar]
- 5.Melton LJ, 3rd, Stauffer RN, Chao EY, Ilstrup DM. Rates of total hip arthroplasty; a population-based study. N Engl J Med. 1982;307:1242–1245. doi: 10.1056/NEJM198211113072004. [DOI] [PubMed] [Google Scholar]
- 6.Wells VM, Hearn TC, McCaul KA, Anderton SM, Wigg AE, Graves SE. Changing incidence of primary total hip arthroplasty and total knee arthroplasty for primary osteoarthritis. J Arthroplasty. 2002;17:267–273. doi: 10.1054/arth.2002.30414. [DOI] [PubMed] [Google Scholar]
- 7.Järvholm B, From C, Lewold S, Malchau H, Vingård E. Incidence of surgically treated osteoarthritis in the hip and knee in male construction workers. Occup Environ Med. 2008;65:275–278. doi: 10.1136/oem.2007.033365. [DOI] [PubMed] [Google Scholar]
- 8.Cram P, Lu X, Callaghan JJ, Vaughan-Sarrazin MS, Cai X, Li Y. Long-term trends in hip arthroplasty use and volume. J Arthroplasty. 2012;27:278–285.e2. doi: 10.1016/j.arth.2011.04.043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fevang BT, Lie SA, Havelin LI, Engesaeter LB, Furnes O. Improved results of primary total hip replacement. Acta Orthop. 2010;81:649–659. doi: 10.3109/17453674.2010.537807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hoaglund FT, Oishi CS, Gialamas GG. Extreme variations in racial rates of total hip arthroplasty for primary coxarthrosis: a population-based study in San Francisco. Ann Rheum Dis. 1995;54:107–110. doi: 10.1136/ard.54.2.107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Oishi CS, Hoaglund FT, Gordon L, Ross PD. Total hip replacement rates are higher among Caucasians than Asians in Hawaii. Clin Orthop Relat Res. 1998;(353):166–174. doi: 10.1097/00003086-199808000-00019. [DOI] [PubMed] [Google Scholar]
- 12.Lai YS, Wei HW, Cheng CK. Incidence of hip replacement among national health insurance enrollees in Taiwan. J Orthop Surg Res. 2008;3:42. doi: 10.1186/1749-799X-3-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kim HA, Koh SH, Lee B, Kim IJ, Seo YI, Song YW, Hunter DJ, Zhang Y. Low rate of total hip replacement as reflected by a low prevalence of hip osteoarthritis in South Korea. Osteoarthritis Cartilage. 2008;16:1572–1575. doi: 10.1016/j.joca.2008.04.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Yoon HK, Park C, Jang S, Jang S, Lee YK, Ha YC. Incidence and mortality following hip fracture in Korea. J Korean Med Sci. 2011;26:1087–1092. doi: 10.3346/jkms.2011.26.8.1087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lee YK, Ha YC, Park C, Koo KH. Trends of surgical treatment in femoral neck fracture: a nationwide study based on claim registry. J Arthroplasty. 2013;28:1839–1841. doi: 10.1016/j.arth.2013.01.015. [DOI] [PubMed] [Google Scholar]
- 16.Malchau H, Herberts P, Eisler T, Garellick G, Söderman P. The Swedish total hip replacement register. J Bone Joint Surg Am. 2002;84-A:2–20. doi: 10.2106/00004623-200200002-00002. [DOI] [PubMed] [Google Scholar]
- 17.Abbott KC, Bucci JR, Agodoa LY. Total hip arthroplasty in chronic dialysis patients in the United States. J Nephrol. 2003;16:34–39. [PubMed] [Google Scholar]
- 18.Birrell F, Johnell O, Silman A. Projecting the need for hip replacement over the next three decades: influence of changing demography and threshold for surgery. Ann Rheum Dis. 1999;58:569–572. doi: 10.1136/ard.58.9.569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Zhan C, Kaczmarek R, Loyo-Berrios N, Sangl J, Bright RA. Incidence and short-term outcomes of primary and revision hip replacement in the United States. J Bone Joint Surg Am. 2007;89:526–533. doi: 10.2106/JBJS.F.00952. [DOI] [PubMed] [Google Scholar]
- 20.Nevitt MC, Xu L, Zhang Y, Lui LY, Yu W, Lane NE, Qin M, Hochberg MC, Cummings SR, Felson DT. Very low prevalence of hip osteoarthritis among Chinese elderly in Beijing, China, compared with whites in the United States: the Beijing osteoarthritis study. Arthritis Rheum. 2002;46:1773–1779. doi: 10.1002/art.10332. [DOI] [PubMed] [Google Scholar]
- 21.Lau EM, Lin F, Lam D, Silman A, Croft P. Hip osteoarthritis and dysplasia in Chinese men. Ann Rheum Dis. 1995;54:965–969. doi: 10.1136/ard.54.12.965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kim SR, Ha YC, Kim JR, Kim R, Kim SY, Koo KH. Incidence of hip fractures in Jeju Island, South Korea: a prospective study (2002-2006) Clin Orthop Surg. 2010;2:64–68. doi: 10.4055/cios.2010.2.2.64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kim SH, Meehan JP, Lee MA. Surgical treatment of trochanteric and cervical hip fractures in the United States: 2000-2009. J Arthroplasty. 2013;28:1386–1390. doi: 10.1016/j.arth.2012.09.007. [DOI] [PubMed] [Google Scholar]
- 24.Kannan A, Kancherla R, McMahon S, Hawdon G, Soral A, Malhotra R. Arthroplasty options in femoral-neck fracture: answers from the national registries. Int Orthop. 2012;36:1–8. doi: 10.1007/s00264-011-1354-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Australian Orthopaedic Association National Joint Replacement Registry: annual report 2003. [accessed on 1 March 2014]. Available at https://aoanjrr.dmac.adelaide.edu.au/documents/10180/75178/Annual%20Report%202003?version=1.1&t=1349407014597.
- 26.National Agency for Medicines. The 2002-2003 implant yearbook on orthopaedic endoprostheses: Finnish Arthroplasty Register. [accessed on 15 May 2014]. Available at: http://www.fimea.fi/instancedata/prime_product_julkaisu/fimea/embeds/fimeawwwstructure/19717_julkaisut_Orthopaedic_Endoprostheses_2003_v.pdf.pdf.
- 27.Malchau H, Herberts P, Garellick G, Söderman P, Eisler T. Prognosis of total hip replacement: update of results and risk-ratio analysis for revision and re-revision from the Swedish National Hip Arthroplasty Register 1979-2000. [accessed on 1 March 2014]. Available at http://www.shpr.se/Libraries/Documents/AAOS2002.sflb.ashx.