

Abstract
Background. The aim of this study was to analyze complications of vestibular schwannoma (VS) microsurgery. Material and Methods. A retrospective study was performed in 333 patients with unilateral vestibular schwannoma indicated for surgical treatment between January 1997 and December 2012. Postoperative complications were assessed immediately after VS surgery as well as during outpatient followup. Results. In all 333 patients microsurgical vestibular schwannoma (Koos grade 1: 12, grade 2: 34, grade 3: 62, and grade 4: 225) removal was performed. The main neurological complication was facial nerve dysfunction. The intermediate and poor function (HB III–VI) was observed in 124 cases (45%) immediately after surgery and in 104 cases (33%) on the last followup. We encountered disordered vestibular compensation in 13%, permanent trigeminal nerve dysfunction in 1%, and transient lower cranial nerves (IX–XI) deficit in 6%. Nonneurological complications included CSF leakage in 63% (lateral/medial variant: 99/1%), headache in 9%, and intracerebral hemorrhage in 5%. We did not encounter any case of meningitis. Conclusions. Our study demonstrates that despite the benefits of advanced high-tech equipment, refined microsurgical instruments, and highly developed neuroimaging technologies, there are still various and significant complications associated with vestibular schwannomas microsurgery.
1. Introduction
Vestibular schwannomas (VS) are the most common tumors of the cerebellopontine angle (CPA; 80–95%). They are benign, slow growing tumors arising from the Schwann cells at the oligodendrocyte-Schwann cell junction (Obersteiner-Redlich zone). These tumors originate from the peripheral portion of the inferior and superior vestibular nerve and very rarely from the cochlear branch of the eighth cranial nerve. VS are rare, comprising approximately 10% of primary intracranial tumors, 85% of CPA tumors, and 90% of intracranial schwannomas [1].
The symptoms of VS include mainly sensorineural hearing loss (SNHL), tinnitus, and vestibular disorder and rarely other cranial nerve lesions and intracranial hypertension. Treatment options of VS depend on several factors (size and growth of the tumor, symptoms, and medical comorbidities) and require an active approach (surgical removal; stereotactic radiosurgery) or observation (wait and scan). VS represent histologically benign tumours, a significant proportion of which are either nongrowing or slow-growing; therefore, observation is commonly accepted option in case of small oligosymptomatic tumors (<2.5 cm in size) [2, 3]. Preservation of neurological function and elimination of complications is a principal goal of any therapeutic action. Although microsurgery represents a gold standard in VS management, there are strong proponents of stereoradiosurgical treatment for tumors ≤2.5–3 cm in diameter [4, 5]. Microsurgery is indicated mainly in the case of large tumors, the deterioration of useful hearing during observation with attempt for its preservation, and in the case of disabling symptoms [2, 3].
Removal of vestibular schwannomas may be performed using several approaches: the translabyrinthine [6], the retrosigmoid [7], or the middle fossa approach [8]. Prerequisites for the translabyrinthine approach include mainly the preoperative lack of serviceable hearing and the presence of larger tumors [9, 10]. The retrosigmoid (suboccipital) approach allows the removal of tumors of any size with the potential for hearing preservation; its main disadvantage is the need for cerebellar retraction [11, 12]. Lastly, the middle fossa approach is chosen for tumors limited to the internal auditory canal or with minimal CPA extension with an attempt to preserve hearing. Drawbacks of this approach are the limited access to CPA and the need for temporal lobe retraction [8].
Over the past several decades, the outcomes of treatment for patients with VS have significantly improved. The goal of the treatment in the early 20th century was to resect the tumor without perioperative mortality. However, with the improvement of diagnostic tools (early stage diagnosis), advances in anesthetic care, introduction of microsurgical techniques, and intraoperative monitoring, mortality and neurologic morbidity have been significantly reduced without compromising the radicality of tumor resection. Therefore, it became possible to preserve normal function of cranial nerves, including facial nerve and hearing preservation, whilst causing minimal injury to the cerebellum and brainstem.
Early diagnosis, advanced skull base surgery techniques, specific surgical approaches, tumor size, age of the patient, and the use of intraoperative monitoring have all been implicated as predictive factors for good postoperative recovery with a decreased complication rate [13]. However, complications may still occur, especially when treating large tumors. Precise information about these potential complications has to be given to the patient at the time of the surgical decision. There is also imminent need of their effective diagnosis, management, and prevention. The most common complications of VS microsurgery are CSF leak and meningitis, facial nerve paresis, headache, disordered vestibular compensation, cerebellar and brain stem injuries, and vascular complications [2, 3, 14–20].
Based on recent trends our goal was to analyze the complications encountered in a series of 333 consecutive patients undergoing microsurgical treatment over the last 15-year period. We also reviewed the international literature on the complications of vestibular schwannoma microsurgery and its prevention and management.
2. Material and Methods
A retrospective study was performed on 333 patients, with ages ranging from 12 to 74 years (48 ± 14 years): 144 male (43%) and 189 female (57%) patients with unilateral vestibular schwannoma indicated for surgical treatment based on a retrosigmoid-transmeatal approach, across the period between January 1997 and December 2012. All patients were operated on by the same team of neurotologists and a neurosurgeon. The design of the study was approved by the local ethical committee.
The data collected in each patient included the patient's age, gender, size of tumor, intraoperative findings (e.g., facial nerve structural and functional preservation and radicality of tumor resection), and postoperative complications (CSF leak, meningitis, vascular complications, headache, cranial nerve dysfunction, and altered vestibular compensation).
The size of the tumor was determined by preoperative magnetic resonance imaging (MRI). The diameter was measured from the extrameatal component on the axial scans in the plane parallel with the long axis of the internal auditory canal (IAC), which included both intra- and extrameatal portion of the tumor. Koos grading system was also used to classify the tumor grade based on tumor extension (G1: intrameatal tumors; G2: tumors extending to the cerebellopontine angle; G3: tumors filling the cerebellopontine angle; G4: tumors compressing the brainstem and cerebellum).
Facial nerve function was assessed according to the House-Brackmann (HB) grading system immediately after surgery and at the time of the last followup. Function was further classified into three categories: excellent (HB I-II), intermediate (HB III-IV), and poor (HB V-VI). Facial nerve monitoring was used to identify the facial nerve and confirm its function intraoperatively in all cases.
Postoperative complications were evaluated during the immediate postoperative recovery (within one week) and at the time of last followup (long-term or persistent complications). The follow-up period ranged from 12 to 178 months. Symptoms of vertigo, spontaneous nystagmus, and deviation of subjective visual vertical, which were persistent after six months following operation, were classified as disordered compensation of vestibular pathology.
3. Results
Primary microsurgical vestibular schwannoma removal was performed in 317 patients. Seven patients underwent revision surgery because of a growing tumor remnant following a primary surgery performed elsewhere. Five patients were operated on because of a growing tumor after previous stereoradiosurgical treatment (three patients were treated with Leksell's gamma knife and 1 with LINAC) and another four patients because of a growing tumor after previous partial tumor resection followed by stereoradiosurgery (all were treated with Leksell's gamma knife (LGK)). We employed the retrosigmoid-transmeatal approach in 325 (97%), translabyrinthine approach in six (2%), and combined translabyrinthine-retrosigmoid approach in two (1%) of the cases.
In our series grade one tumors were present in 12 patients (3.6%), grade two in 34 patients (10.2%), grade three in 62 patients (18.6%), and grade four in 225 patients (67.6%). In nine (3%) patients tumors caused hydrocephalus and intracranial hypertension. We would like to stress here the atypically high proportion of the grade four tumors.
Gross total removal (GTR) of tumors was achieved in 328 (98.5%) of cases. In five patients we decided to perform near total tumor removal (NTR) leaving residual tumor capsules of ≤1-2 mm either at the root exit zone of CN VII (as in one case) or at CN VII in the region of porus of IAC (four cases). We did not observe any tumor regrowth on the repeated annual MRI scans. We encountered only two cases of tumor recurrence in the group of GTR (one in the region of the fundus of IAC and one in the labyrinth extending to the IAC).
CN VII function preservation noted immediately after surgery was deemed “excellent” in 175 patients (55%), “intermediate” in 96 patients (30%), and “poor” in 48 patients (15%). CN VII function at the last followup was “excellent” in 214 patients (67%), “intermediate” in 98 patients (31%), and “poor” in 15 patients (2%). Overall facial nerve injury leading to discontinuation was present in 22 patients (6.6%) after primary surgery and in all but one patient after previous primary stereoradiosurgery or stereoradiosurgery preceded by partial tumor resection (PTR) (Table 1). In all such cases we performed facial nerve reconstruction. Direct neurorrhaphy in the IAC without grafting was possible in only two patients. In 12 patients we performed CN VII-VII anastomosis with grafting in the IAC/CPA, employing the graft from the greater auricular nerve, and in four patients we performed extra-intracranial CN VII-VII anastomosis according to the Norman-Dott method, using the sural nerve graft. In one patient we employed transpetrous CN VII-VII anastomosis with sural nerve according to Samii. Cross-anastomosis CN VII–CN XII end to side according to the technique described by Darrouzet et al. [21] was employed in cases of proximal stump of CN VII absence (two patients from the group of primary microsurgery and nine patients in the group of revision microsurgery following previous stereoradiosurgery and eventual PTR) and in one patient with preserved facial nerve following previous LGK treatment, but the patient had persistent HB VI function even after 18 months postoperatively without any sign of ongoing reinnervation based on electromyography (Table 2).
Table 1.
Complications of vestibular schwannoma microsurgery.
| Type of complication | Number of patients | % |
|---|---|---|
| CN VII discontinuity | 31 | 10% |
| Permanent CN V dysfunction | 3 | 1% |
| Transient CN V dysfunction | 7 | 2% |
| CN VI palsy | 1 | 0.3% |
| Transient CN IX–XI dysfunction | 20 | 6% |
| Disordered vestibular compensation | 43 | 13% |
| Lateral variant of CSF leak | 208 | 62.5% |
| Medial variant of CSF leak | 2 | 0.6% |
| Headache | 29 | 9% |
| Intracranial hemorrhage | 12 | 4% |
| Epidural hematomas | 3 | 1% |
| Mortality | 3 | 3% |
CN: cranial nerve.
Table 2.
Facial nerve function assessed immediately after surgery and at the last follow up.
| CN VII function (House-Brackmann) | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| Nm. immediately/last follow-up | 140/195 | 35/19 | 64/89 | 32/9 | 25/6 | 23/0 |
| % immediately/last follow-up | 44/61 | 11/6 | 20/28 | 10/3 | 8/2 | 7/0 |
Transient postoperative dysfunction of the trigeminal nerve was observed in seven patients (2%) and the permanent lesion in three patients (1%). One patient (0.3%) had an iatrogenic lesion of the CN VI after accidental VII-VI anastomosis. Transient postoperative dysfunction of lower cranial nerves (CN IX–XI) occurred in 20 patients (6%) with giant VS (>4 cm extrameatal tumor component).
Disordered vestibular compensation was observed in 43 patients (13%).
A lateral variant of CSF leakage (pseudomeningocele) (Figure 1) occurred in 208 patients (62.5%). In 205 patients it was managed conservatively using a puncture, aspiration, with or without tissue glue injection (84 patients, one to six applications), and wound compression. A medial variant of CSF leakage (Figure 2) occurred in two patients (0.6%) and was managed by wound revision and leak sealing. During the follow-up period (1–15 years in all 333 patients after surgery), neither infection nor meningitis occurred.
Figure 1.
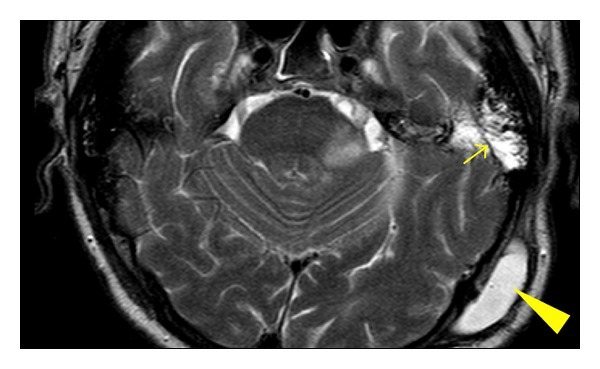
Lateral variant of CSF leak/pseudomeningocele (T2W MRI). Arrowhead: pseudomeningocele, arrow demonstrates CSF filled pneumatic system of the temporal bone.
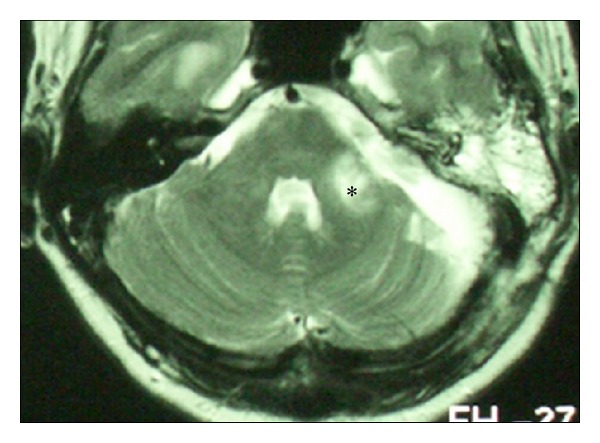
Figure 2.
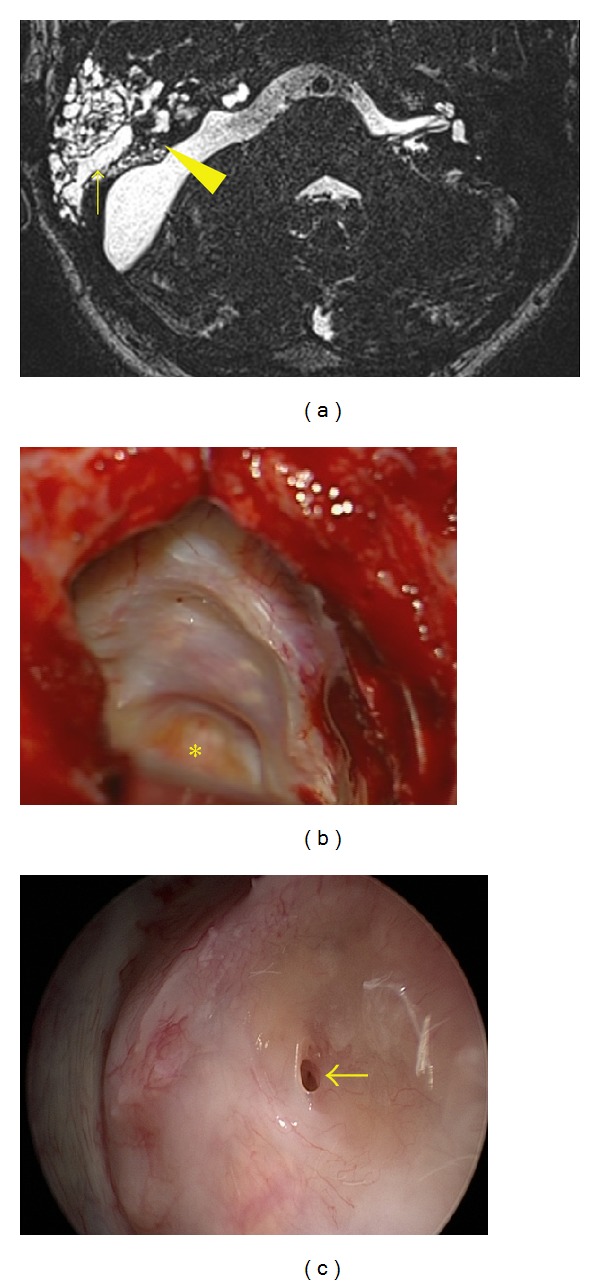
Medial variant of CSF leak. (a) T2W MRI, arrowhead pointing to the fistula; arrow demonstrates CSF filled pneumatic system of temporal bone. (b) Wound revision with identification of fistula in the posterior rim of meatotomy; asterisk shows the closed IAC. (c) Endoscopic view of the fistula.
Postoperative headache was reported by 29 patients (9%).
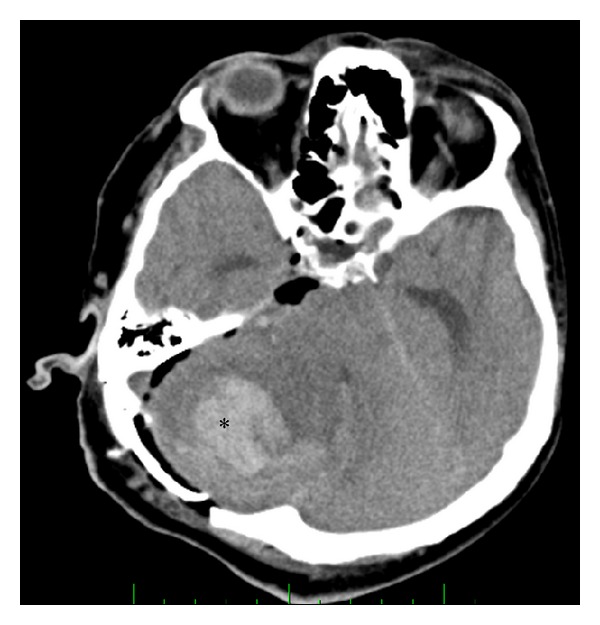
Hemorrhage after VS microsurgery occurred in 15 patients (5%). Intracerebellar haematomas (Figure 3) were observed in four patients (1.2%) and CPA haematomas (Figure 4) in eight patients (2.4%). All of these were managed with immediate wound revision and decompression. We also encountered epidural haematoma in three patients (1%). Two of these epidural haematomas were managed with wound revision and one case with puncture and aspiration only. In one patient supratentorial ischemia caused by microembolization (Figure 5) occurred and one patient suffered peduncular venous infarction caused by superior petrous vein injury (Figure 6). Both of them suffered from transient organic psychosyndrome.
Figure 3.
CT scan of patient with intracerebellar haematoma.
Figure 4.

CT scan of patient with haematoma of the cerebellopontine angle.
Figure 5.
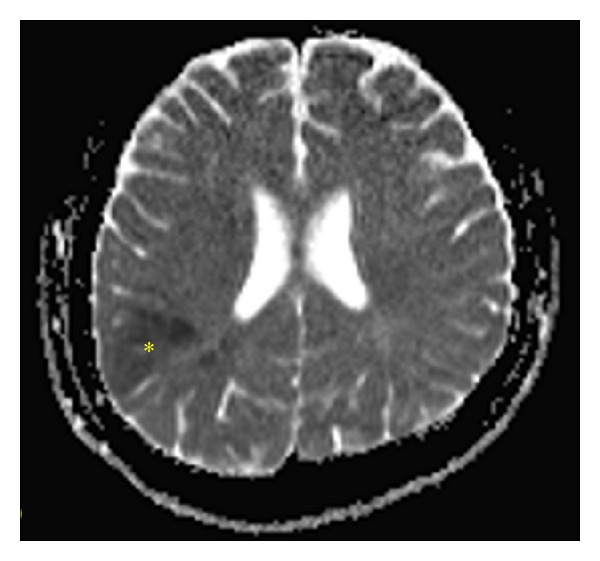
MRI of patient with the supratentorial ischemia as a consequence of microembolisation (paradox embolisation excluded).
Figure 6.
MRI of patient with peduncular venous infarction (asterisk) due to superior petrous vein injury.
The mortality rate in our study was approximately 3%. The cause of death in two patients was intracerebellar haemorrhage and pulmonary embolism in one case.
We also encountered one case of myelopathy related to cervical disc herniation as a consequence of unexpected intraoperative patient arousal from general anaesthesia. Other rare nonsurgical complications, for example, displacement of central venous catheter, phlebitis, transitory lesion of the ulnar (two cases), and peroneal (one case) nerve, were also observed.
Postoperative hearing loss/deafness was not considered a complication; therefore, it is not evaluated in this series.
4. Discussion
Morbidity and mortality rates associated with the surgical treatment of vestibular schwannomas have changed significantly during the past century. In the early 1900s Harvey Cushing developed techniques to reduce the surgical mortality rate from 80% to 20% [20, 22–24] and during the 1960s major advances in anaesthesia, pharmacology, and especially surgical techniques were developed to a large extent by William House [22]. As mortality and morbidity have been reduced dramatically in the recent years, preservation of quality of life postoperatively has become the generally accepted goal of VS management.
In the case of microsurgical treatment, gross total tumor removal with the preservation of neurologic functions is the newest benchmark. Despite this some works support near total and subtotal removal in large tumors as suitably viable treatment options to maintain good postoperative facial nerve and even hearing functions [14, 25].
The reduced complication rate is a result of the introduction of modern methods and materials into the surgical treatment of VS. In general, the increased visualization of the surgical field, through the use of endoscopes, helps to identify possible CSF leakage and also decreases the chance of residual tumor, especially intrameatally. Faster tumor removal is managed by the use of ultrasonic aspirators, shavers, or fibre lasers. The position of craniotomy according to sigmoid sinus and avoidance of its injury can be improved by CT navigation. Diffusion tensor imaging (DTI) of facial nerves helps in easier identification of its course. New materials used for dura mater and skull reconstruction should help to prevent CSF leakage as well as the adhesion of nuchal muscles that cause headaches.
The most common complications of microsurgical treatment are CSF leak and meningitis, facial paresis, headache, vestibular disorders, cerebellar and brain stem injuries, and vascular complications. These postoperative complications can be divided into two groups: neurological and nonneurological.
4.1. Nonneurological Complications
4.1.1. CSF Leak and Meningitis
CSF leaks and meningitis are the most common complications following vestibular schwannoma resection. The literature reports a range of postoperative CSF leak rates from 2% to 30% [26–29] but the average leak rate appears to be approximately 10% [30].
CSF leakage can be classified as either of a medial (via petrous air cells or eventual labyrinth) or lateral variant (wound leak/pseudomeningocele). The most difficult to manage are the medial variants that usually require revision surgery and leak closure.
4.1.2. Medial CSF Leak
Many reports have discussed different factors leading to postoperative CSF leaks. Both Slattery et al. [20] and Brennan et al. [31] found a significant relationship between tumor size and the prevalence of CSF leakage; according to Brennan et al., larger tumors appeared to lead to a greater risk of CSF leak; however, Slattery et al. [20] showed a correlation between surgical approach and CSF leakage rate, with a retrosigmoid approach having the highest frequency (15%) and middle fossa approach the lowest (5.7%). Lüdemann et al. [32] observed that only large tumors with severe dislocation of the brainstem, causing hydrocephalus, showed a higher incidence of CSF; otherwise, they showed inverse correlation (smaller tumors had a higher risk of CSF leak). Sanna et al. [15] did not demonstrate any relationship and medial CSF leak in the case of the translabyrinthine approach. Based on these findings, it can be concluded that tumor size and type of surgical approach are the main factors affecting postoperative CSF leakage.
Merkus et al. [33] in their long term study of 1803 cases operated via translabyrinthine approach reported only 0.8% of postoperative CSF leaks and stressed meticulous sealing of petrous bone air cells. The same is true for the retrosigmoid-transmeatal approach in which the most common pathways of leak formation are perimeatal air cells of petrous bone; therefore, their sealing is crucial for CSF leak prevention. The addition of endoscopic and endoscopy-assisted vestibular schwannoma surgery seems to be beneficial for improved identification of potential pathways of CSF leakage [34]. The material used for petrous bone air cells sealing can also be considered a significant factor. The work of Lüdemann et al. [32] supports a fat implantation as superior to muscle implantation for the prevention of CSF leakage. Their study on 420 patients undergoing tumor removal via retrosigmoid-transmeatal approach reports the incidence of postoperative CSF leaks at 2.2% with the use of fat implantation compared to 5.7% if muscle grafts were employed for petrous air cell sealing. Furthermore, women had less postoperative CSF leakage (3.4%) than men (5.6%).
Our results show that with meticulous sealing of opened air cells following IAC opening, medial variant of CSF leakage can be reduced to a minimum even in cases with high proportions of large tumors. We have observed only two such cases and both of them were managed surgically. Suspicion can be based on intraoperative findings (e.g., significant perimeatal pneumatisation) and the absence of pseudomeningocele. MRI can be helpful in confirming and localizing the pathologic pathway. Despite the majority of experts recommending the horizontal positioning of patient with elevated head and lumbar drainage for cases of leakage persisting for more than 24 hours, we are proponents of early leak sealing as the first leaving surgical revision for cases of leaks persisting more than three days.
4.1.3. Lateral CSF Leak
The study by Mangus et al. [35] showed a correlation between the surgical approach and type of CSF leak [26], in which wound leak was most commonly present in the use of translabyrinthine (54%), whereas rhinorrhea was most common in the cases of the suboccipital (68%) and middle fossa (70%) approach. Incidence of wound leak in our study was much higher than in the published studies. This could be related to the technique of wound closure, avoidance of lumbar drainage in the perioperative period, and our active approach in identifying wound leak. Moreover, our results show that management of the lateral variant of CSF leak is relatively straightforward (sole puncture, aspiration, and wound compression and in cases of recurrence the application of tissue glue). Wound revision for CSF leak was needed in less than 1% of all these cases when an anatomical obstacle preventing optimal closure of the dead space, created by bone and soft tissue removal, was identified intraoperatively (e.g., bony overhang over the dura mater).
Our recommendation for wound leak prevention is the use of the watertight multilayer-tissue closure technique, with a preferred primary suture of dura mater and the use of muscle, fat, tissue glue, and pressure dressing for several days. Under such conditions, we did not observe any prolonged wound healing or postoperative wound infection; however, our frequency rate of CSF wound leak is relatively high.
4.1.4. Meningitis
Postoperative meningitis is a well described complication of skull based surgery. Although mortality is rare [15–17, 20, 36], early diagnosis and treatment are important in the management of these patients. Postoperative CSF leak is associated with an increased risk of meningitis that is raised from 3% to 14% [30]. Allen et al. [37] also reported an increased risk associated with the suboccipital approach. In contrast, Selesnick et al. [30] reported that a CSF leak was not associated with surgical approach, although the meningitis was significantly associated with cerebrospinal fluid leak. However, Kourbeti et al. [38] reported that presence of CSF leak was not significant in developing of meningitis. In general, CSF leak seems to be an obvious risk factor of meningitis.
Despite the high rate of the lateral variant of CSF leak in our series that were managed actively without lumbar drainage, we did not encounter neither wound infection nor meningitis. Thus, we can only speculate whether or not perioperative employment of lumbar drainage represents a risk of meningitis.
Our recommendations for the avoidance of meningitis are the prevention of wound contamination by the aseptic surgical field, perioperative antibiotic coverage, meticulous sealing of all potential pathways of CSF leaks, and active management of all types of CSF leaks.
4.1.5. Headache
The incidence of chronic headache after VS surgery in the literature is widely variable ranging from 0 to 73% and depends on surgical approach as well as postoperative evaluation period [39–44]. The occurrence of postoperative headache has been reported mainly in patients undergoing tumor resection via the retrosigmoid approach [45]; however, the origin of postoperative headache in relation to surgical approach remains unclear. Many different factors may cause symptom: incision, dural adhesions to nuchal muscles or to subcutaneous tissues, dural tension, or muscle spasm [46]. A high-arching skin incision crossing the occipital nerves at its terminal branches is less likely to cause chronic postoperative headache compared to a straight incision. Schaller and Baumann [47] informed that the prevention of postoperative headache may include the replacement of the bone flap at the end of surgery, duraplasty instead of direct dural closure, and prevention of the use of fibrin glue. Catalano et al. [48] reported that free circulation of bone dust into the posterior fossa during intradural drilling of the IAC may be the most important factor in the development of headache after the retrosigmoid approach.
Our results fit to the published data with prevalence of postoperative headache being 9%. The vast majority of such cases were tension type headaches managed conservatively.
To prevent postoperative headache in our patients, we promote meticulous cleaning of the bone dust by continuous irrigation and suction, duraplasty as needed, cranioplasty to prevent dural adhesion to nuchal muscles, and proper placement of the incision [45]. In the case of postoperative headaches, multidisciplinary management in cooperation with a physiotherapist, neurologist, pain clinic, and even alternative approaches (e.g., acupuncture) are helpful.
4.1.6. Intracranial Vascular Complications
Vascular complications of the VS surgery can have devastating consequences. These complications occur as an intracranial haemorrhage (intraparenchymal hematomas and subdural or epidural hematomas) or ischemia. Such complications can cause death if not immediately treated. Samii and Matthies [18] reported their acute and subacute postoperative haemorrhage cases as 2.2% and 1.5%, respectively. Sade et al. [49] concluded that the incidence of vascular complications in VS surgery was similar for retrosigmoid and translabyrinthine approaches (2.7%). The middle fossa approach has the highest occurrence of epidural haematomas.
The major consequences of the acute intracranial haemorrhage are mainly caused by increased intracranial pressure leading to loss of consciousness, hemiparesis, fixed or dilated pupil, respiratory distress, bradycardia, or systolic hypertension. The recognition of any of these signs should lead to early intervention. The majority of intracranial haemorrhages necessitate immediate wound revision following CT scanning.
Ischemic complications may be of arterial or venous origin and may affect the brain stem or the cerebellar hemisphere. Adhesion of the tumor with the brainstem and cerebellum is the cause of microtraumatism of the small vessels that course at the tumor-brain interface. Consequently, meticulous care to preserve the arachnoid plane during tumor removal is crucial for preservation of subpial vessels. Coagulation of small arterial perforators must be avoided to prevent brainstem infarction. Major injury of cerebellar vessels is rare because these vessels are usually well identified and safely dissected from the tumor. Care should also be taken to preserve large veins (e.g., greater petrosal vein) as their closure can have serious consequences [50]. Similarly transverse and sigmoid sinus thrombosis can also lead to severe complications [19].
4.2. Neurological Complications
4.2.1. Facial Nerve Injury
The risk of facial nerve dysfunction after VS surgery cannot be entirely eliminated. A significant incidence of transient facial nerve dysfunction is still present after VS surgical removal [22, 51]. The type of surgical approach and tumor size are the main factors significantly affecting postoperative facial nerve function [52–54]. The anatomical facial nerve preservation rate has been reported to be 80–90% [55–59]. The preservation of facial nerve function has been reported to be 70–80% for tumors greater than 3 cm in diameter, removed either by the retrosigmoid [18, 43, 60] or by translabyrinthine approaches [55–59]. The HB evaluation of facial nerve function can be modified to “excellent” (HB grade 1/2), “intermediate” (HB grade 3/4), or “poor” (HB grade 5/6). The reported preservation rate of “excellent” function after the removal of large tumors is 42–52.6% [55–59].
Surgical techniques for preserving facial nerve function include the early identification of the root entry/exit zone and maximum caution during removal of the intrameatal tumor portion. If facial nerve function does not return after several months or the return of the function is not expected the cross-anastomosis is provided as the best measure and the most widely used technique for reanimation of facial nerve paralysis with no proximal stump [61–66]. Many different types of cross-anastomosis of damaged facial nerves have been described (accessory, phrenic, and glossopharyngeal nerves). The advantages of CN XII–CN VII anastomosis in general are improved facial tone with better cosmetic result, protection of the eye, intentional facial movements controlled by the tongue, and movements associated with physiological function of the tongue. The disadvantages are hemiatrophy of the tongue, mass movement of the face, and, in some instances, facial hypertonia [61]. This technique has been modified by May and subsequently Darrouzet who support side to end CN XII–CN VII anastomosis to preserve tongue function [21, 67]. We found this technique to be an excellent option for cases with an absence of the proximal stump of the CN VII. All patients were able to gain normal tonus of the face with voluntary movements and only transient dysarthria.
4.2.2. Injury of Other Cranial Nerves
The facial numbness caused by trigeminal paresis (incidence 0–4.7%) [16, 43, 57, 68, 69] and the dysfunction of the abducens nerve are very rare complications of VS surgery on large tumors.
The lower cranial nerves can be injured during removal of large vestibular schwannomas, which should impinge on jugular foramen contents and CN IX, X, and XI. Acute lower cranial nerve deficits could result in dysphagia and aspiration. In some cases, it is necessary to provide nutrition through a nasogastric feeding tube or to prevent the risk of aspiration. Reeducation and rehabilitation of swallowing techniques and manoeuvres are crucial for management. In cases with severe problems and risk of aspiration pneumonia, tracheostomy and percutaneous endoscopic gastrostomy can be an option. In our study we encountered only transitory lower cranial nerve injury.
4.2.3. Disordered Vestibular Compensation
Balance problems are a common complication of VS pre- as well as postoperatively [70–72]. Preoperative vertigo can be caused by a peripheral lesion (inner ear or neural origin); however, it can also have a central (cerebellar) origin [73]. Small tumors are more commonly associated with vertigo of peripheral origin because of missing deafferentation [74, 75], whereas large tumors, especially those that are slow-growing, will cause compression of the cerebellum or brainstem [74] and therefore central origin of vertigo. The preoperative diagnosis of a vestibular lesion is important for predicting the postoperative compensation outcome. Patients with a central lesion would be expected to have prolonged compensation [76], whereas in patients with hypofunction of the inner ear the development of compensation prior to surgery would be expected. It can be concluded that the severity of the patient's vestibular symptomatology is related to the level of residual vestibular function present; therefore, prehabituation (preoperative chemical labyrinthectomy with intratympanic application of gentamicin followed by vestibular rehabilitation) to improve vestibular compensation seems to be a promising method to alleviate postoperative problems [77]. Postoperative vertigo is in general caused by acute deafferentation originating from the transection of vestibular nerves. It has been reported in the majority of cases; however, it has a tendency to gradually improve over time [72, 78]. The prolonged postoperative vertigo, or disbalance, can be attributed to several factors: brainstem or cerebellum injuries, incorrect or insufficient rehabilitation, orthopedic and neurological factors, impairment of vision, anxiety and depression, and the persistence of the vestibular nerve [79, 80]. Nonaka et al. [14] described the influence of different surgical approaches on prolonged vertigo (in 12% of patients treated with the retrosigmoid approach, in 11.7% of patients with the middle fossa approach, and in 5% of patients undergoing the translabyrinthine approach). Overall incidences of persisting postoperative vertigo and disequilibrium in VS microsurgery have ranged from 1% to as high as 30% [16, 69, 81]. In our previous study [34], the patient's age was identified as the only important factor associated with disordered vestibular compensation following retrosigmoid VS microsurgery. Thus, new methods including prehabituation and biofeedback seem to be a logical step of outcome improvement [72, 77]. Intraoperative avoidance of cerebellar injury is crucial for the prevention of disordered vestibular compensation.
5. Conclusions
Despite the atypically high proportion of large tumors in this series, our rates of VS microsurgery complications are comparable with the reviewed literature, with the exception of the lateral CSF leak. Overall, during the last decades the rate of VS microsurgery complications has drastically decreased. However, the information about possible complications should be clearly given to the patient when the benefit/risk ratio is to be evaluated at the time of treatment decision. It can be concluded that most complications are the consequence of inadequate surgical maneuvers, with vascular complications carrying the most significant rate of severe morbidity and potential mortality. Appropriate selection of cases, meticulous surgical technique, and careful postoperative care are crucial to lower the rate of all complications of vestibular schwannoma microsurgery.
Acknowledgments
The authors are grateful for funding by the Ministry of Health of the Czech Republic (IGA MZ CR NT/11543-6 a NT/12459-5) and Charles University (Projects PRVOUK/LF1/P27, Specific University Research (SVV UK) 266513, and UNCE 204013).
Conflict of Interests
None of the authors has a conflict of interests with the submission of this paper.
References
- 1.Lanser MJ, Sussman SA, Frazer K. Epidemiology, pathogenesis, and genetics of acoustic tumors. Otolaryngologic Clinics of North America. 1992;25(3):499–520. [PubMed] [Google Scholar]
- 2.Myrseth E, Pedersen P-H, Møller P, Lund-Johansen M. Treatment of vestibular schwannomas. Why, when and how? Acta Neurochirurgica. 2007;149(7):647–660. doi: 10.1007/s00701-007-1179-0. [DOI] [PubMed] [Google Scholar]
- 3.Zverina E. Acoutic neuroma—vestibular schwannoma—personal experience of up-to-date management. Casopis Lekaru Ceskych. 2010;149(6):269–276. [PubMed] [Google Scholar]
- 4.Somers T, Van Havenbergh T. Multidisciplinary management of vestibular schwannomas: state of the art. B-ENT. 2012;8(4):235–240. [PubMed] [Google Scholar]
- 5.Kondziolka D, Mousavi SH, Kano H, Flickinger JC, Lunsford LD. The newly diagnosed vestibular schwannoma: radiosurgery,resection, or observation? Neurosurgical Focus. 2012;33(3):p. E8. doi: 10.3171/2012.6.FOCUS12192. [DOI] [PubMed] [Google Scholar]
- 6.Arriaga MA, Lin J. Translabyrinthine approach: indications, techniques, and results. Otolaryngologic Clinics of North America. 2012;45(2):399–415. doi: 10.1016/j.otc.2011.12.009. [DOI] [PubMed] [Google Scholar]
- 7.Elhammady MS, Telischi FF, Morcos JJ. Retrosigmoid approach: indications, techniques, and results. Otolaryngologic Clinics of North America. 2012;45(2):375–397. doi: 10.1016/j.otc.2012.02.001. [DOI] [PubMed] [Google Scholar]
- 8.Angeli S. Middle fossa approach: indications, technique, and results. Otolaryngologic Clinics of North America. 2012;45(2):417–438. doi: 10.1016/j.otc.2011.12.010. [DOI] [PubMed] [Google Scholar]
- 9.Brackmann DE, Green JD., Jr. Translabyrinthine approach for acoustic tumor removal (Reprinted from Otolaryngologic Clinics of NA vol 25, pg 311–330, 1992) Otolaryngologic Clinics of North America. 2008;19(2):p. 251. [PubMed] [Google Scholar]
- 10.Day JD, Chen DA, Arriaga M, et al. Translabyrinthine approach for acoustic neuroma. Neurosurgery. 2004;54(2):391–396. doi: 10.1227/01.neu.0000103668.26590.5a. [DOI] [PubMed] [Google Scholar]
- 11.de Freitas MR, Russo A, Sequino G, Piccirillo E, Sanna M. Analysis of hearing preservation and facial nerve function for patients undergoing vestibular schwannoma surgery: the middle cranial fossa approach versus the retrosigmoid approach-personal experience and literature review. Audiology and Neurotology. 2012;17(2):71–81. doi: 10.1159/000329362. [DOI] [PubMed] [Google Scholar]
- 12.Kutz JW, Jr., Scoresby T, Isaacson B, et al. Hearing preservation using the middle fossa approach for the treatment of vestibular schwannoma. Neurosurgery. 2012;70(2):334–341. doi: 10.1227/NEU.0b013e31823110f1. [DOI] [PubMed] [Google Scholar]
- 13.Isaacson B, Telian SA, El-Kashlan HK. Facial nerve outcomes in middle cranial fossa vs translabyrinthine approaches. Otolaryngology-Head and Neck Surgery. 2005;133(6):906–910. doi: 10.1016/j.otohns.2005.08.021. [DOI] [PubMed] [Google Scholar]
- 14.Nonaka Y, Fukushima T, Watanabe K, et al. Contemporary surgical management of vestibular schwannomas: analysis of complications and lessons learned over the past decade. Neurosurgery. 2013;72(6):103–115. doi: 10.1227/NEU.0b013e3182752b05. [DOI] [PubMed] [Google Scholar]
- 15.Sanna M, Taibah A, Russo A, Falcioni M, Agarwal M. Perioperative complications in acoustic neuroma (vestibular schwannoma) surgery. Otology and Neurotology. 2004;25(3):379–386. doi: 10.1097/00129492-200405000-00029. [DOI] [PubMed] [Google Scholar]
- 16.Darrouzet V, Martel J, Enée V, Bébéar J, Guérin J. Vestibular schwannoma surgery outcomes: our multidisciplinary experience in 400 cases over 17 years. Laryngoscope. 2004;114(4):681–688. doi: 10.1097/00005537-200404000-00016. [DOI] [PubMed] [Google Scholar]
- 17.Dubey A, Sung W, Shaya M, et al. Complications of posterior cranial fossa surgery-an institutional experience of 500 patients. Surgical Neurology. 2009;72(4):369–375. doi: 10.1016/j.surneu.2009.04.001. [DOI] [PubMed] [Google Scholar]
- 18.Samii M, Matthies C. Management of 1000 vestibular schwannomas (acoustic neuromas): surgical management and results with an emphasis on complications and how to avoid them. Neurosurgery. 1997;40(1):11–21. doi: 10.1097/00006123-199701000-00002. [DOI] [PubMed] [Google Scholar]
- 19.Roche P-H, Ribeiro T, Fournier H-D, Thomassin J-M. Vestibular schwannomas: complications of microsurgery. Progress in Neurological Surgery. 2008;21:214–221. doi: 10.1159/000157169. [DOI] [PubMed] [Google Scholar]
- 20.Slattery WH, III, Francis S, House KC. Perioperative morbidity of acoustic neuroma surgery. Otology and Neurotology. 2001;22(6):895–902. doi: 10.1097/00129492-200111000-00031. [DOI] [PubMed] [Google Scholar]
- 21.Darrouzet V, Dutkiewicz J, Chambrin A, Stoll D, Bebear JP. Hypoglosso-facial anastomosis: results and technical development towards end-to-side anastomosis with rerouting of the intra-temporal facial nerve (modified May technique) Revue de Laryngologie Otologie Rhinologie. 1997;118(3):203–210. [PubMed] [Google Scholar]
- 22.Sampath P, Holliday MJ, Brem H, Niparko JK, Long DM. Facial nerve injury in acoustic neuroma (vestibular schwannoma) surgery. Etiology and prevention. Journal of Neurosurgery. 1997;87(1):60–66. doi: 10.3171/jns.1997.87.1.0060. [DOI] [PubMed] [Google Scholar]
- 23.Ojemann RG. Management of acoustic neuromas (vestibular schwannomas) (honored guest presentation) Clinical Neurosurgery. 1993;40:498–535. [PubMed] [Google Scholar]
- 24.Kaylie DM, Gilbert E, Horgan MA, Delashaw JB, McMenomey SO. Acoustic neuroma surgery outcomes. Otology and Neurotology. 2001;22(5):686–689. doi: 10.1097/00129492-200109000-00022. [DOI] [PubMed] [Google Scholar]
- 25.Schwartz MS, Kari E, Strickland BM, et al. Evaluation of the increased use of partial resection of large vestibular schwanommas: facial nerve outcomes and recurrence/regrowth rates. Otology & Neurotology: Official Publication of the American Otological Society, American Neurotology Society & European Academy of Otology and Neurotology. 2013;34(8):1456–1464. doi: 10.1097/MAO.0b013e3182976552. [DOI] [PubMed] [Google Scholar]
- 26.Fishman AJ, Hoffman RA, Roland JT, Lebowitz RA, Cohen NL. Cerebrospinal fluid drainage in the management of CSF leak following acoustic neuroma surgery. Laryngoscope. 1996;106(8):1002–1004. doi: 10.1097/00005537-199608000-00017. [DOI] [PubMed] [Google Scholar]
- 27.Fishman AJ, Marrinan MS, Golfinos JG, Cohen NL, Roland JT., Jr. Prevention and management of cerebrospinal fluid leak following vestibular schwannoma surgery. Laryngoscope. 2004;114(3):501–505. doi: 10.1097/00005537-200403000-00022. [DOI] [PubMed] [Google Scholar]
- 28.Glasscock ME, III, Kveton JF, Jackson CG. A systematic approach to the surgical management of acoustic neuroma. Laryngoscope. 1986;96(10):1088–1094. doi: 10.1288/00005537-198610000-00008. [DOI] [PubMed] [Google Scholar]
- 29.Becker SS, Jackler RK, Pitts LH. Cerebrospinal fluid leak after acoustic neuroma surgery: a comparison of the translabyrinthine, middle fossa, and retrosigmoid approaches. Otology and Neurotology. 2003;24(1):107–112. doi: 10.1097/00129492-200301000-00021. [DOI] [PubMed] [Google Scholar]
- 30.Selesnick SH, Liu JC, Jen A, Newman J. The incidence of cerebrospinal fluid leak after vestibular schwannoma surgery. Otology and Neurotology. 2004;25(3):387–393. doi: 10.1097/00129492-200405000-00030. [DOI] [PubMed] [Google Scholar]
- 31.Brennan JW, Rowed DW, Nedzelski JM, Chen JM. Cerebrospinal fluid leak after acoustic neuroma surgery: influence of tumor size and surgical approach on incidence and response to treatment. Journal of Neurosurgery. 2001;94(2):217–223. doi: 10.3171/jns.2001.94.2.0217. [DOI] [PubMed] [Google Scholar]
- 32.Lüdemann WO, Stieglitz LH, Gerganov V, Samii A, Samii M. Fat implant is superior to muscle implant in vestibular schwannoma surgery for the prevention of cerebrospinal fluid fistulae. Neurosurgery. 2008;63(1):ONS38–ONS42. doi: 10.1227/01.neu.0000335009.53122.a3. [DOI] [PubMed] [Google Scholar]
- 33.Merkus P, Taibah A, Sequino G, Sanna M. Less than 1% cerebrospinal fluid leakage in 1,803 translabyrinthine vestibular schwannoma surgery cases. Otology and Neurotology. 2010;31(2):276–283. doi: 10.1097/MAO.0b013e3181cc06ad. [DOI] [PubMed] [Google Scholar]
- 34.Chovanec M, Zvěřina E, Profant O, et al. Impact of video-endoscopy on the results of retrosigmoid-transmeatal microsurgery of vestibular schwannoma: prospective study. European Archives of Oto-Rhino-Laryngology. 2013;270(4):1277–1284. doi: 10.1007/s00405-012-2112-6. [DOI] [PubMed] [Google Scholar]
- 35.Mangus BD, Rivas A, Yoo MJ, et al. Management of cerebrospinal fluid leaks after vestibular schwannoma surgery. Otology and Neurotology. 2011;32(9):1525–1529. doi: 10.1097/MAO.0b013e318232e4a4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Sanchez GB, Kaylie DM, O’Malley MR, Labadie RF, Jackson CG, Haynes DS. Chemical meningitis following cerebellopontine angle tumor surgery. Otolaryngology-Head and Neck Surgery. 2008;138(3):368–373. doi: 10.1016/j.otohns.2007.10.038. [DOI] [PubMed] [Google Scholar]
- 37.Allen KP, Isaacson B, Kutz JW, Purcell PL, Roland PS. The association of meningitis with postoperative cerebrospinal fluid fistula. Journal of Neurological Surgery Part B-Skull Base. 2012;73(6):401–404. doi: 10.1055/s-0032-1329618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kourbeti IS, Jacobs AV, Koslow M, Karabetsos D, Holzman RS. Risk factors associated with postcraniotomy meningitis. Neurosurgery. 2007;60(2):317–325. doi: 10.1227/01.NEU.0000249266.26322.25. [DOI] [PubMed] [Google Scholar]
- 39.Ryzenman JM, Pensak ML, Tew JM., Jr. Headache: a quality of life analysis in a cohort of 1,657 patients undergoing acoustic neuroma surgery, results from the Acoustic Neuroma Association. Laryngoscope. 2005;115(4):703–711. doi: 10.1097/01.mlg.0000161331.83224.c5. [DOI] [PubMed] [Google Scholar]
- 40.Wiegand DA, Fickel V. Acoustic neuroma-the patient’s perspective: subjective assessment of symptoms, diagnosis, therapy, and outcome in 541 patients. Laryngoscope. 1989;99(2):179–187. doi: 10.1288/00005537-198902000-00010. [DOI] [PubMed] [Google Scholar]
- 41.Parving A, Tos M, Thomsen J, Moller H, Buchwald C. Some aspects of life quality after surgery for acoustic neuroma. Archives of Otolaryngology-Head and Neck Surgery. 1992;118(10):1061–1064. doi: 10.1001/archotol.1992.01880100053013. [DOI] [PubMed] [Google Scholar]
- 42.Pedrosa CA, Ahern DK, McKenna MJ, Ojemann RG, Acquadro MA. Determinants and impact of headache after acoustic neuroma surgery. American Journal of Otology. 1994;15(6):793–797. [PubMed] [Google Scholar]
- 43.Ebersold MJ, Harner SG, Beatty CW, Harper CM, Jr., Quast LM. Current results of the retrosigmoid approach to acoustic neurinoma. Journal of Neurosurgery. 1992;76(6):901–909. doi: 10.3171/jns.1992.76.6.0901. [DOI] [PubMed] [Google Scholar]
- 44.Cohen NL, Lewis WS, Ransohoff J. Hearing preservation in cerebellopontine angle tumor surgery: the NYU experience 1974–1991. American Journal of Otology. 1993;14(5):423–433. doi: 10.1097/00129492-199309000-00002. [DOI] [PubMed] [Google Scholar]
- 45.Harner SG, Beatty CW, Ebersold MJ. Headache after acoustic neuroma excision. American Journal of Otology. 1993;14(6):552–555. [PubMed] [Google Scholar]
- 46.Ruckenstein MJ, Harris JP, Cueva RA, Prioleau G, Alksne J. Pain subsequent to resection of acoustic neuromas via suboccipital and translabyrinthine approaches. American Journal of Otology. 1996;17(4):620–624. [PubMed] [Google Scholar]
- 47.Schaller B, Baumann A. Headache after removal of vestibular schwannoma via the retrosigmoid approach: a long-term follow-up-study. Otolaryngology-Head and Neck Surgery. 2003;128(3):387–395. doi: 10.1067/mhn.2003.104. [DOI] [PubMed] [Google Scholar]
- 48.Catalano PJ, Jacobowitz O, Post KD. Prevention of headache after retrosigmoid removal of acoustic tumors. American Journal of Otology. 1996;17(6):904–908. [PubMed] [Google Scholar]
- 49.Sade B, Mohr G, Dufour J. Vascular complications of vestibular schwannoma surgery: a comparison of the suboccipital retrosigmoid and translabyrinthine approaches. Journal of Neurosurgery. 2006;105(2):200–204. doi: 10.3171/jns.2006.105.2.200. [DOI] [PubMed] [Google Scholar]
- 50.Ebner FH, Roser F, Shiozawa T, et al. Petrosal vein occlusion in cerebello-pontine angle tumour surgery: an anatomical study of alternative draining pathways. European Journal of Surgical Oncology. 2009;35(5):552–556. doi: 10.1016/j.ejso.2008.06.011. [DOI] [PubMed] [Google Scholar]
- 51.Lalwani AK, Butt FY-S, Jackler RK, Pitts LH, Yingling CD. Facial nerve outcome after acoustic neuroma surgery: a study from the era of cranial nerve monitoring. Otolaryngology-Head and Neck Surgery. 1994;111(5):561–570. doi: 10.1177/019459989411100505. [DOI] [PubMed] [Google Scholar]
- 52.Arriaga MA, Chen DA. Facial function in hearing preservation acoustic neuroma surgery. Archives of Otolaryngology-Head and Neck Surgery. 2001;127(5):543–546. doi: 10.1001/archotol.127.5.543. [DOI] [PubMed] [Google Scholar]
- 53.Jacob A, Robinson LL, Jr., Bortman JS, Yu L, Dodson EE, Welling DB. Nerve of origin, tumor size, hearing preservation, and facial nerve outcomes in 359 vestibular schwannoma resections at a tertiary care academic center. Laryngoscope. 2007;117(12):2087–2092. doi: 10.1097/MLG.0b013e3181453a07. [DOI] [PubMed] [Google Scholar]
- 54.Grey PL, Moffat DA, Palmer CR, Hardy DG, Baguley DM. Factors which influence the facial nerve outcome in vestibular schwannoma surgery. Clinical Otolaryngology. 1996;21(5):409–413. doi: 10.1046/j.1365-2273.1996.00816.x. [DOI] [PubMed] [Google Scholar]
- 55.Mamikoglu B, Wiet RJ, Esquivel CR. Translabyrinthine approach for the management of large and giant vestibular schwannomas. Otology and Neurotology. 2002;23(2):224–227. doi: 10.1097/00129492-200203000-00020. [DOI] [PubMed] [Google Scholar]
- 56.Briggs RJS, Luxford WM, Atkins JS, Jr., Hitselberger WE, Sekhar LN, Al-Mefty O. Translabyrinthine removal of large acoustic neuromas. Neurosurgery. 1994;34(5):785–791. doi: 10.1227/00006123-199405000-00001. [DOI] [PubMed] [Google Scholar]
- 57.Lanman TH, Brackmann DE, Hitselberger WE, Subin B. Report of 190 consecutive cases of large acoustic tumors (vestibular schwannoma) removed via the translabyrinthine approach. Journal of Neurosurgery. 1999;90(4):617–623. doi: 10.3171/jns.1999.90.4.0617. [DOI] [PubMed] [Google Scholar]
- 58.Sluyter S, Graamans K, Tulleken CAF, Van Veelen CWM. Analysis of the results obtained in 120 patients with large acoustic neuromas surgically treated via the translabyrinthine-transtentorial approach. Journal of Neurosurgery. 2001;94(1):61–66. doi: 10.3171/jns.2001.94.1.0061. [DOI] [PubMed] [Google Scholar]
- 59.Sterkers J-M, Morrison GAJ, Sterkers O, Badr El-Dine MMK. Preservation of facial, cochlear, and other nerve functions in acoustic neuroma treatment. Otolaryngology-Head and Neck Surgery. 1994;110(2):146–155. doi: 10.1177/019459989411000202. [DOI] [PubMed] [Google Scholar]
- 60.Jung S, Kang S, Kim T, et al. Current surgical results of retrosigmoid approach in extralarge vestibular schwannomas. Surgical Neurology. 2000;53(4):370–378. doi: 10.1016/s0090-3019(00)00196-8. [DOI] [PubMed] [Google Scholar]
- 61.Linnet J, Madsen FF. Hypoglosso-facial nerve anastomosis. Acta Neurochirurgica. 1995;133(3-4):112–115. doi: 10.1007/BF01420060. [DOI] [PubMed] [Google Scholar]
- 62.Pellat JL, Bonnefille E, Zanaret M, Cannoni M. Hypoglossal-facial anastomosis. A report of 60 cases. Annales de Chirurgie Plastique et Esthetique. 1997;42(1):37–43. [PubMed] [Google Scholar]
- 63.Pitty LF, Tator CH. Hypoglossal-facial nerve anastomosis for facial nerve palsy following surgery for cerebellopontine angle tumors. Journal of Neurosurgery. 1992;77(5):724–731. doi: 10.3171/jns.1992.77.5.0724. [DOI] [PubMed] [Google Scholar]
- 64.Rosenwasser RH, Liebman E, Jimenez DF, Buchheit WA, Andrews DW. Facial reanimation after facial nerve injury. Neurosurgery. 1991;29(4):568–574. doi: 10.1097/00006123-199110000-00014. [DOI] [PubMed] [Google Scholar]
- 65.Samii M, Matthies C. Indication, technique and results of facial nerve reconstruction. Acta Neurochirurgica. 1994;130(1–4):125–139. doi: 10.1007/BF01405512. [DOI] [PubMed] [Google Scholar]
- 66.Sawamura Y, Abe H. Hypoglossal-facial nerve side-to-end anastomosis for preservation of hypoglossal function: results of delayed treatment with a new technique. Journal of Neurosurgery. 1997;86(2):203–206. doi: 10.3171/jns.1997.86.2.0203. [DOI] [PubMed] [Google Scholar]
- 67.May M, Sobol SM, Mester SJ. Hypoglossal-facial nerve interpositional-jump graft for facial reanimation without tongue atrophy. Otolaryngology-Head and Neck Surgery. 1991;104(6):818–825. doi: 10.1177/019459989110400609. [DOI] [PubMed] [Google Scholar]
- 68.Wiet RJ, Raslan W, Kazan RP, Herzon GD. Complications in the approach to acoustic tumor surgery. Annals of Otology, Rhinology and Laryngology. 1986;95(1):28–31. doi: 10.1177/000348948609500106. [DOI] [PubMed] [Google Scholar]
- 69.Harner SG, Beatty CW, Ebersold MJ. Retrosigmoid removal of acoustic neuroma: experience 1978–1988. Otolaryngology-Head and Neck Surgery. 1990;103(1):40–45. doi: 10.1177/019459989010300106. [DOI] [PubMed] [Google Scholar]
- 70.Breivik CN, Nilsen RM, Myrseth E, Finnkirk MK, Lund-Johansen M. Working disability in Norwegian patients with vestibular schwannoma: vertigo predicts future dependence. World Neurosurgery. 2013;80(6):E301–E305. doi: 10.1016/j.wneu.2013.03.069. [DOI] [PubMed] [Google Scholar]
- 71.Uehara N, Tanimoto H, Nishikawa T, et al. Vestibular dysfunction and compensation after removal of acoustic neuroma. Journal of Vestibular Research: Equilibrium and Orientation. 2011;21(5):289–295. doi: 10.3233/VES-2011-0429. [DOI] [PubMed] [Google Scholar]
- 72.Cakrt O, Chovanec M, Funda T, et al. Exercise with visual feedback improves postural stability after vestibular schwannoma surgery. European Archives of Oto-Rhino-Laryngology. 2010;267(9):1355–1360. doi: 10.1007/s00405-010-1227-x. [DOI] [PubMed] [Google Scholar]
- 73.Giannuzzi AL, Merkus P, Falcioni M. The use of intratympanic gentamicin in patients with vestibular schwannoma and disabling vertigo. Otology & Neurotology: Official Publication of the American Otological Society, American Neurotology Society & European Academy of Otology and Neurotology. 2013;34(6):1096–1098. doi: 10.1097/MAO.0b013e3182804c41. [DOI] [PubMed] [Google Scholar]
- 74.Wagner JN, Glaser M, Wowra B, et al. Vestibular function and quality of life in vestibular schwannoma: does size matter? Frontiers in Neurology. 2011;2:p. 55. doi: 10.3389/fneur.2011.00055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Parietti-Winkler C, Gauchard GC, Simon C, Perrin PP. Sensorimotor postural rearrangement after unilateral vestibular deafferentation in patients with acoustic neuroma. Neuroscience Research. 2006;55(2):171–181. doi: 10.1016/j.neures.2006.02.016. [DOI] [PubMed] [Google Scholar]
- 76.Aw ST, Todd MJ, Lehnen N, et al. Electrical vestibular stimulation after vestibular deafferentation and in vestibular schwannoma. Plos ONE. 2013;8(12) doi: 10.1371/journal.pone.0082078.e82078 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Magnusson M, Kahlon B, Karlberg M, Lindberg S, Siesjö P. Preoperative vestibular ablation with gentamicin and vestibular ’prehab’ enhance postoperative recovery after surgery for pontine angle tumours-first report. Acta Oto-Laryngologica. 2007;127(12):1236–1240. doi: 10.1080/00016480701663433. [DOI] [PubMed] [Google Scholar]
- 78.Chovanec M, Zverina E, Cakrt O, et al. Factors influencig vestibular compensation following vestibular schwannoma microsurgery. Otolaryngology-Head and Neck Surgery. 2014 [Google Scholar]
- 79.Lynn SG, Driscoll CLW, Harner SG, Beatty CW, Atkinson EJ. Assessment of dysequilibrium after acoustic neuroma removal. American Journal of Otology. 1999;20(4):484–494. [PubMed] [Google Scholar]
- 80.Saman Y, Bamiou D, Gleeson M. A contemporary review of balance dysfunction following vestibular schwannoma surgery. Laryngoscope. 2009;119(11):2085–2093. doi: 10.1002/lary.20648. [DOI] [PubMed] [Google Scholar]
- 81.Wiegand DA, Ojemann RG, Fickel V. Surgical treatment of acoustic neuroma (vestibular schwannoma) in the United States: report from the acoustic neuroma registry. Laryngoscope. 1996;106(1):58–66. doi: 10.1097/00005537-199601000-00012. [DOI] [PubMed] [Google Scholar]