

Abstract
While the lifespan of people with type 1 diabetes has increased progressively since the advent of insulin therapy, these patients still experience premature mortality, primarily from cardiovascular disease (CVD). However, a subgroup of those with type 1 diabetes survives well into old age without significant morbidity. It is the purpose of this review to explore the factors which may help in identifying these patients. It might be expected that hyperglycaemia plays a major role in explaining the increased incidence of CVD and mortality of these individuals. However, while a number of publications have associated poor long term glycaemic control with an increase in both all-cause mortality and CVD in those with type 1 diabetes, it is apparent that good glycaemic control alone cannot explain why some patients with type 1 diabetes avoid fatal CVD events. Lipid disorders may occur in those with type 1 diabetes, but the occurrence of elevated high-density lipoprotein-cholesterol is positively associated with longevity in this population. Non-renal hypertension, by itself is a significant risk factor for CVD but if adequately treated does not appear to mitigate against longevity. However, the presence of nephropathy is a major risk factor and its absence after 15-20 years of diabetes appears to be a marker of long-term survival. One of the major factors linked with long-term survival is the absence of features of the metabolic syndrome and more specifically the presence of insulin sensitivity. Genetic factors also play a role, with a family history of longevity and an absence of type 2 diabetes and hypertension in the family being important considerations. There is thus a complex interaction between multiple risk factors in determining which patients with type 1 diabetes are likely to live into older age. However, these patients can often be identified clinically based on a combination of factors as outlined above.
Keywords: Type 1 diabetes, Prognosis, Survival, Coronary artery disease, Cardiovascular disease, Lipids, Metabolic syndrome
Core tip: People with type 1 diabetes are generally assumed to have a shortened lifespan. This contention is supported by a number of epidemiological studies confirming a trend towards premature death, primarily due to cardiovascular disease. However, a subset of type 1 individuals survives for many years, living for over 50 years or more with type 1 diabetes. This review explores the clinical features that are linked to long-term survival in people with type 1 diabetes, allowing identification of these individuals. Recognising these individuals will aid in assessing prognosis, and treating the identified risk factors could improve survival.
INTRODUCTION
Prior to the discovery of insulin, patients with type 1 diabetes had an expected lifespan of less than 3 years[1]. With the advent of modern therapy, survival has increased progressively. However, those with type 1 diabetes remain with an increased incidence of coronary artery disease (CAD) and mortality compared to the general population. By 1991, reported standard mortality rates for those with type 1 diabetes under the age of 60 years were 9.1 for males and 13.5 for females[2]. Subsequently, a cohort of 23751 patients from the United Kingdom and diagnosed with diabetes under the age of 30 years between 1972 and 1993 were analysed for cardiovascular mortality up to 2000[3]. These results confirmed higher mortality rates at younger ages for those with type 1 diabetes (Figure 1). Of interest, not only are the mortality rates for women with diabetes considerably higher than for women without diabetes, but also higher than for men without diabetes. Soedamah-Muthu et al[4], utilizing the United Kingdom General Practice research database, have also confirmed that the risk of cardiovascular disease (CVD) remains high in patients with type 1 diabetes. Typically, patients with type 1 diabetes reach a 10-year risk of fatal CVD of 5% about 10 to 15 years before the general population. Furthermore, incidence rates of CAD in type 1 patients range between 1.2% and 2% per year, vs 0.1% and 0.5% in the general population[5]. The incidence of stroke is also increased in type 1 diabetes, with overall standardised incidence ratios being 17.94 for men and 26.11 for women[6].
Figure 1.
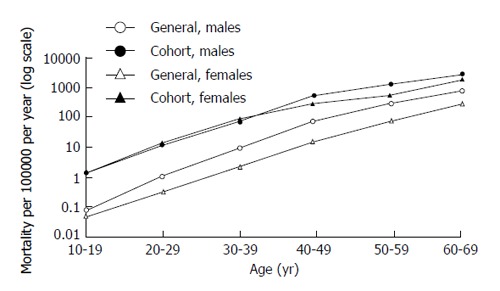
Ischaemic heart disease mortality rates in people with type 1 diabetes vs general population (from: Laing et al[3]).
It is therefore clear, that despite a better understanding and treatment of appropriate risk factors and better general care, those with type 1 diabetes still have a tendency towards a shortened life span, primarily due to premature CVD. Yet a subgroup of individuals with type 1 diabetes survives well into old age in relatively good health. This review explores the factors that may help to identify these patients. This can be done either by identifying a group of long-surviving type 1 patients and analysing any unique clinical or biological features that may be specific to this cohort, or by assessing surrogate endpoints of vascular disease, such as carotid artery Intima-Media Thickness (IMT) measurement or arterial calcification and identifying those who appear to be “protected” from vascular disease.
THE ROLE OF GLYCAEMIC CONTROL
Type 1 diabetes is a condition of “pure” hyperglycaemia. The only abnormality is one of β-cell failure and insulin deficiency in an otherwise “normal” or “healthy” individual. It could therefore be expected that hyperglycaemia might play a major role in explaining the increased incidence of CVD and mortality seen in these individuals. A number of publications have associated poor long-term glycaemic control with an increase in both all-cause mortality and CVD in those with type 1 diabetes. Grauslund et al[7] demonstrated a direct relationship between HbA1c and survival. When patients were categorized into quartiles of HbA1c measurements, patients in the highest quartile had a significantly higher risk of all-cause mortality, cardiovascular mortality and ischaemic heart disease when compared to patients in the lowest quartile (Figure 2). While at the conclusion of the Diabetes Control and Complications Trial (DCCT) there was no significant difference between the conventional and intensive treatment groups regarding cardiovascular outcomes or death from CVD, the 10-year Epidemiology of Diabetes Interventions and Complications (EDIC) follow-up demonstrated a significant difference between the two groups with regard to both CV outcomes and death. An overall 42% risk reduction was seen in the previously intensively treated group[8]. This sustained effect of improved control in the DCCT years was ascribed to “metabolic memory”. Patients followed in the DCCT/EDIC cohort were also submitted to IMT measurements, and it was demonstrated that intensive therapy during the DCCT resulted in decreased progression of IMT six year after the end of the trial[9]. These findings imply that early glycaemic control is an important factor in preventing CVD in type 1 diabetes.
Figure 2.
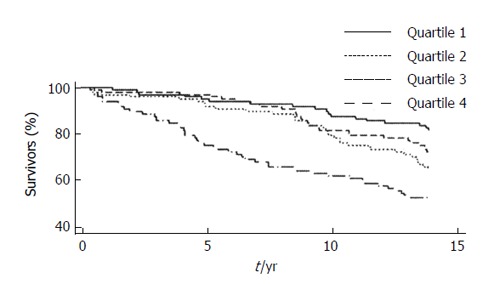
All-cause mortality and the association of glycaemic control (from: Grauslund et al[7]).
However, good blood glucose levels alone cannot explain why some patients with type 1 diabetes avoid fatal CVD events. In the “Golden Years Cohort” of 400 type 1 patients who survived for over 50 years with diabetes[10], the mean HbA1c was 7.6% (± 1.4), with some of these patients having HbA1c levels as high as 8.5%-9%. None had an HbA1c below 7%. In addition, a number of other publications have shown only a weak correlation between long-term glycaemic control, CVD and mortality. Larsen et al[11], performed coronary angiography on 29 asymptomatic patients with a mean duration of type 1 diabetes of 30.6 years. Of these, 34% had significant coronary artery stenosis. While a significant relationship existed between stenosis and glycaemic control (a 6.1% increase in vessel stenosis for every 1% increase in HbA1c over 18 years), glycaemic control was less significant as a risk factor than the age of the subjects and the effect of elevated serum cholesterol. In another cohort of 125 patients with a mean duration of diabetes of 22 years[12], IMT was compared to an index of lifetime glycaemic exposure. This demonstrated significantly increased IMT only on those at the highest tertile of glycaemic exposure. IMT measurements performed in 148 long-surviving patients with type 1 diabetes (duration > 15 years)[13] showed no significant correlation between HbA1c and IMT, although ordinal logistic regression showed that for every 1% increase in HbA1c, there was a 27% less chance of the IMT falling into the low-risk group (defined as an IMT below 0.6 mm and no plaque). A prospective observational study of a meta-analysis of the relationship between CVD and glycaemic control[14], revealed an only moderate increase in cardiovascular risk with increasing levels of glycated haemoglobin in persons with diabetes mellitus. However, this meta-analysis included patients with both type 1 and type 2 diabetes. The data suggested that there is an increased risk of CVD of 15% for every 1% increase in HbA1c (RR = 1.15; 95%CI: 0.92-1.43).
The evidence therefore suggests that while early good glycaemic control is important in the prevention of CVD and survival, the importance of glycaemic control may diminish as patients survive longer. While glycaemic control is clearly a risk factor for CAD and mortality in type 1 diabetes, this is not the major determinant of survival. Good glycaemic control alone cannot explain why some type 1 patients survive into old age.
LIPIDS IN TYPE 1 DIABETES
Patients with type 1 diabetes may show quantitative lipid disorders. There is a clear relationship between the level of glycaemic control and lipid abnormalities, with an independent correlation between HbA1c and low-density lipoprotein (LDL)-cholesterol, non-high-density lipoprotein (HDL) cholesterol and triglycerides[15]. Abnormal lipid levels are associated with worse cardiovascular outcomes[5]. The lipid profiles of patients with well-controlled type 1 diabetes are very different from those with poor glycaemic control[16], related possibly to the presence of adequate peripheral insulin levels in the better controlled subjects. There are direct metabolic consequences of administering insulin subcutaneously. Peripheral hyperinsulinemia is associated with increased lipoprotein lipase activity[17], which may account for reduced triglyceride levels. In addition, LDL-cholesterol may also be slightly reduced due to decreased very LDL production[18]. The more sensitive the individual is to insulin, the greater is this effect.
As might be expected, Serum LDL-cholesterol and non-HDL-cholesterol levels are positively associated with not only an increase in IMT[9], increased Arterial Stiffness[19] and coronary artery stenosis[11], but also CAD and mortality[5,7,20]. A major factor that appears to be associated with prolonged survival in patients with type 1 diabetes is elevated HDL-cholesterol. HDL levels are often elevated in those with type 1 diabetes. This is more marked with better glycaemic control and may be due to an elevated lipoprotein lipase/hepatic lipase ratio (Increased peripheral lipoprotein lipase activity due to peripheral hyperinsulinemia from subcutaneous insulin administration and normal hepatic lipase activity). Bain et al[10] reported a high mean HDL-level in those surviving over 50 years with diabetes (1.84 ± 0.057 mmol/L), and this was associated with lower triglyceride levels (1.49 ± 0.79 mmol/L). In long-surviving type 1 patients, IMT measurements showed a significant inverse association to HDL levels and computed tomography/HDL ratios for all measure of risk (IM thickness and/or plaque)[13]. A number of other studies have supported the protective effects of HDL-cholesterol with regard to CVD[5,7,9,11,20]. In addition to this direct association between HDL-cholesterol and CVD, higher HDL-cholesterol levels may provide protection against the development of albuminuria[21].
Therefore, it can be concluded that in addition to the expected effect of dyslipidaemia (high LDL and non-HDL-cholesterol), HDL-cholesterol itself exerts a significant protective effect on the development of CVD in patients with type 1 diabetes and elevated HDL-cholesterol levels appears to play a major role in longevity in these patients.
BLOOD PRESSURE AS A RISK FACTOR
Hypertension in those with type 1 diabetes is often a manifestation of underlying nephropathy. However, hypertension can also occur as a stand-alone risk factor (non-renal hypertension). A significant positive association between high blood pressure and arterial stiffness in youth with type 1 diabetes was demonstrated in the SEARCH CVD Study[19].
In type 1 diabetes, hypertension without nephropathy has been shown to be a major risk factor for the development of carotid artery plaque [OR = 5.26 (P < 0.004)], but the effect of hypertension on IMT was moderate and not significant[13]. In the DCCT/EDIC at 6 years, the presence of hypertension and particularly systolic hypertension was significant, but had less of an effect on IMT than did smoking, lipids or glycaemic control[9]. In the Golden years cohort[10], 29% of the patients were receiving antihypertensive treatment but had nevertheless survived for over 50 years with diabetes.
It therefore appears as though hypertension itself, while a significant risk factor for CVD, if treated does not mitigate against longevity in this population.
MICROVASCULAR DISEASE AS A MARKER OF SURVIVAL
The presence of diabetic nephropathy, microalbuminuria or macroalbuminuria is a significant risk factor for CAD, cardiovascular mortality and all cause mortality, and there is a strong independent relationship between albuminuria and CAD (Table 1)[7]. The occurrence of stroke in subjects with type 1 diabetes is also increased by the presence of nephropathy [microalbuminuria: HR = 3.2 (1.9-5.6), macroalbuminuria: HR = 4.9 (2.9-8.2), End Stage Renal Disease: HR = 7.5 (4.2-13.3)][22]. The DCCT/EDIC Study showed a sustained effect of good glycaemic control[23] on the reduction in albumin excretion 7 years after the conclusion of the DCCT study, with an 83% risk reduction in those patients initially treated with intensive therapy, confirming the concept of “metabolic memory”. The long-term risk of a reduction in estimated glomerular filtration rate (eGFR) was also shown to be 50% lower among those who were treated early in the course of type 1 diabetes with intensive diabetes therapy than among those treated with conventional diabetes therapy[24]. The development of hypertension was also delayed in the intensively treated group. These effects appeared to be largely mediated by the levels of glycaemia achieved during the DCCT. However, as pointed out by the authors, a long time elapsed between treatment intensification during the DCCT early in the course of the diabetes and the effect on eGFR, and the advantages of improved glycaemic control in persons already with advanced complications may not apply. This further supports the contention that good glycaemic control in the early years of the diabetes may be more important achieved in those who have had the condition for some years.
Table 1.
Cox proportional hazard models for risk of cardiovascular disease from nephropathy (from: Grausland et al[7])
| All cause mortality | Cardiovascular mortality | IHD | |
| Creatinine > 120 μmol/L | 5.1 | 6.29 | 4.25 |
| Microalbuminuria | 1.32 | 1.44 | 1.40 |
| Macroalbuminuria | 2.4 | 2.57 | 1.77 |
IHD: Ischaemic heart disease.
In type 1 diabetes, the peak incidence of nephropathy occurs between 15 and 20 years after the development of the diabetes[25,26]. Progression from microalbuminuria to overt neuropathy has been shown to reduce from 45% in those with diabetes of less than 15 years, to 26% in those with diabetes of over 15 years duration. By the time someone has had diabetes for over 40 years, it drops to just 4% per year[25]. In this regard, none of the long surviving patient in the “Golden Years cohort”[10] had evidence of overt nephropathy.
It is therefore apparent, that those individuals with type 1 diabetes who are likely to survive, would remain free of any evidence of nephropathy.
No prospective studies in type 1 patients have found a strong independent relationship between retinopathy and CVD or mortality. However, the presence of retinopathy increases the risk of stroke[22]. Severe diabetic retinopathy was common in the “Golden Years Cohort”[10]. Forty-three percent of subjects had had laser therapy and 2% were blind. In relatively long-surviving people with type 1 diabetes, the presence of retinopathy had a significant association with the presence of plaque (OR = 3.65; P < 0.033), independent of glycaemic control[13]. However, there was no association between the presence of retinopathy and IMT measurements. It therefore appears as though retinopathy is not a major risk factor for CVD or mortality in those with type 1 diabetes, as opposed to those with type 2 diabetes where the presence of retinopathy may indicate CAD and mortality risk[27].
With regard to peripheral neuropathy, no prospective trials link the presence of neuropathy to either CAD or mortality other than the EURODIAB study, which did detect peripheral and autonomic neuropathy as risk markers for future mortality[20].
TYPE 1 DIABETES AND THE METABOLIC SYNDROME
There is no reason to expect patients with type 1 diabetes to have a lower prevalence of obesity and the metabolic syndrome (MetS) than the general population and a MetS frequency in type 1 patients of over 30% has been reported[28]. A significant relationship exists between mortality and central obesity in those with type 1 diabetes[20] and type 1 subjects with the MetS have been shown to have an increased prevalence of macrovascular disease[29]. The presence of MetS features in patients with type 1 diabetes is associated with risk factors similar to many patients with type 2 diabetes, and the superimposition of the insulin resistance due to obesity or the MetS in a patient who already has type 1 diabetes has been termed “Double diabetes”[30].
Identifying patients with the MetS in the presence of type 1 diabetes is difficult. Of the diagnostic criteria, the presence of dysglycaemia is a foregone conclusion and cannot be used. Hypertension should only be included if it is non-renal as nephropathy-induced hypertension has other implications as outlined above. Quantifying insulin resistance is also difficult and requires a euglycaemic clamp study to document it properly. A derived estimate of glucose disposal rate has been suggested to measure of insulin resistance[31] but this includes the presence of hypertension and waist-hip ratio in the formula and therefore cannot be used in assessing insulin resistance in the context of the MetS, since both of these variables are separate components of the MetS in their own right. Insulin dosage provides a surrogate measurement of insulin resistance in these patients, and in their series of long-surviving type 1 patients, Distiller et al[32] arbitrarily chose insulin doses in the top quartile of their series of patients (0.75 U/kg body weight), to be a measure of insulin resistance. In this series, a multiple linear regression analysis showed a significant relationship between waist circumference and insulin dose and carotid artery IMT when corrected for age of onset, current age and duration of diabetes. Interestingly, neither body mass index (BMI) nor HbA1c were significantly associated with carotid artery IMT. Overall, there was a significant increase in IMT in type 1 subjects with the MetS (Figure 3). A significant association was demonstrated between IMT risk and the number of features of the MetS (P = 0.01). Fifty percent of patients with 0-1 features had low risk IMT, whereas 60% of patients with 3-4 features had high risk IMT measures. This finding was confirmed by the SEARCH CVD Study[16], a longitudinal study of 298 youth with diabetes, where those with the MetS had consistently increased arterial wall stiffness when compared to type 1 patients without the Syndrome and with the same duration of diabetes. This was born out by the “Golden Years Cohort”[10], where the patients were generally on low doses of insulin. The mean daily insulin dose was 37.5 U (± 16.2) (0.52 U/kg body weight), the mean BMI of these long surviving patients was 25 kg/m2, and HDL-cholesterol was high and triglycerides were low. These features could be considered the antithesis of the MetS.
Figure 3.
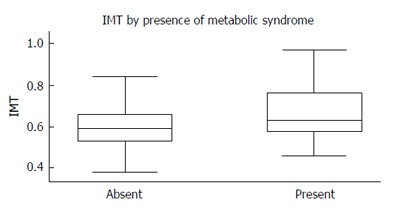
A significant increase in Intima-Media Thickness is seen in patients s with the metabolic syndrome (P = 0.003) (adapted from: Distiller et al[32]).
GENETIC FACTORS
The best predictor of old age is the age one’s parents achieved. This adage was supported by the “Golden Years Cohort”[10], where on average, both parents of those surviving 50 years with diabetes lived to over 70 years. Furthermore, a family history of either type 2 diabetes or hypertension has been shown to result in significantly increased IMT in type 1 diabetes subjects[12].
Clearly, a complex interaction exists between multiple risk factors in determining which patients with type 1 diabetes are likely to live into older age (Figure 4). However, these patients can often be identified clinically based on a combination of factors (Table 2).
Figure 4.
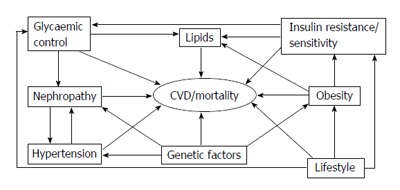
Complex interactions exist between multiple risk factors in determining the outcome for patients with type 1 diabetes. CVD: Cardiovascular disease.
Table 2.
Identifying features of long-surviving patients with type 1 diabetes
| Reasonable (not necessarily ideal) glycaemic control |
| High HDL-cholesterol levels |
| Low daily insulin requirements (“insulin sensitive”) |
| Normal body weight |
| Non-smokers |
| Lower blood pressures |
| Microalbumin negative after 15-20 yr of diabetes |
| Family history of longevity |
HDL: High density lipoprotein.
CONCLUSION
While the longevity of those with type 1 diabetes has improved considerably over the past century, these patients remain with a reduced life expectancy compared to the non-diabetic population. Nevertheless, a subgroup of these individuals may survive into older age despite their diabetes. Certain clinical and biochemical features can identify these people. This understanding may provide clinicians with further evidence that correction of modifiable risk factors like glycaemic control, blood pressure control, avoidance of excessive weight gain and lipid control is vital in ensuring the ongoing longevity of patients with type 1 diabetes.
ACKNOWLEDGMENTS
I would like to thank Michael Brown for his invaluable assistance in editing and preparing this manuscript.
Footnotes
P- Reviewers: Masuo K, PIzawa K S- Editor: Song XX L- Editor: A E- Editor: Liu SQ
References
- 1.Gale EAM. Historical aspects of type 1 diabetes [internet] Available from: http: //www.diapedia.org/type-1-diabetes-mellitus/2104085134/historical-aspects-of-type-1-diabetes.
- 2.Moss SE, Klein R, Klein BE. Cause-specific mortality in a population-based study of diabetes. Am J Public Health. 1991;81:1158–1162. doi: 10.2105/ajph.81.9.1158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Laing SP, Swerdlow AJ, Slater SD, Burden AC, Morris A, Waugh NR, Gatling W, Bingley PJ, Patterson CC. Mortality from heart disease in a cohort of 23,000 patients with insulin-treated diabetes. Diabetologia. 2003;46:760–765. doi: 10.1007/s00125-003-1116-6. [DOI] [PubMed] [Google Scholar]
- 4.Soedamah-Muthu SS, Fuller JH, Mulnier HE, Raleigh VS, Lawrenson RA, Colhoun HM. High risk of cardiovascular disease in patients with type 1 diabetes in the U.K.: a cohort study using the general practice research database. Diabetes Care. 2006;29:798–804. doi: 10.2337/diacare.29.04.06.dc05-1433. [DOI] [PubMed] [Google Scholar]
- 5.Soedamah-Muthu SS, Chaturvedi N, Toeller M, Ferriss B, Reboldi P, Michel G, Manes C, Fuller JH. Risk factors for coronary heart disease in type 1 diabetic patients in Europe: the EURODIAB Prospective Complications Study. Diabetes Care. 2004;27:530–537. doi: 10.2337/diacare.27.2.530. [DOI] [PubMed] [Google Scholar]
- 6.Sundquist K, Li X. Type 1 diabetes as a risk factor for stroke in men and women aged 15-49: a nationwide study from Sweden. Diabet Med. 2006;23:1261–1267. doi: 10.1111/j.1464-5491.2006.01959.x. [DOI] [PubMed] [Google Scholar]
- 7.Grauslund J, Jørgensen TM, Nybo M, Green A, Rasmussen LM, Sjølie AK. Risk factors for mortality and ischemic heart disease in patients with long-term type 1 diabetes. J Diabetes Complications. 2010;24:223–228. doi: 10.1016/j.jdiacomp.2009.05.003. [DOI] [PubMed] [Google Scholar]
- 8.Nathan DM, Cleary PA, Backlund JY, Genuth SM, Lachin JM, Orchard TJ, Raskin P, Zinman B. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med. 2005;353:2643–2653. doi: 10.1056/NEJMoa052187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nathan DM, Lachin J, Cleary P, Orchard T, Brillon DJ, Backlund JY, O’Leary DH, Genuth S. Intensive diabetes therapy and carotid intima-media thickness in type 1 diabetes mellitus. N Engl J Med. 2003;348:2294–2303. doi: 10.1056/NEJMoa022314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bain SC, Gill GV, Dyer PH, Jones AF, Murphy M, Jones KE, Smyth C, Barnett AH. Characteristics of Type 1 diabetes of over 50 years duration (the Golden Years Cohort) Diabet Med. 2003;20:808–811. doi: 10.1046/j.1464-5491.2003.01029.x. [DOI] [PubMed] [Google Scholar]
- 11.Larsen J, Brekke M, Sandvik L, Arnesen H, Hanssen KF, Dahl-Jorgensen K. Silent coronary atheromatosis in type 1 diabetic patients and its relation to long-term glycemic control. Diabetes. 2002;51:2637–2641. doi: 10.2337/diabetes.51.8.2637. [DOI] [PubMed] [Google Scholar]
- 12.Mäkimattila S, Ylitalo K, Schlenzka A, Taskinen MR, Summanen P, Syvänne M, Yki-Järvinen H. Family histories of Type II diabetes and hypertension predict intima-media thickness in patients with Type I diabetes. Diabetologia. 2002;45:711–718. doi: 10.1007/s00125-002-0817-6. [DOI] [PubMed] [Google Scholar]
- 13.Distiller LA, Joffe BI, Melville V, Welman T, Distiller GB. Carotid artery intima-media complex thickening in patients with relatively long-surviving type 1 diabetes mellitus. J Diabetes Complications. 2006;20:280–284. doi: 10.1016/j.jdiacomp.2005.07.012. [DOI] [PubMed] [Google Scholar]
- 14.Selvin E, Marinopoulos S, Berkenblit G, Rami T, Brancati FL, Powe NR, Golden SH. Meta-analysis: glycosylated hemoglobin and cardiovascular disease in diabetes mellitus. Ann Intern Med. 2004;141:421–431. doi: 10.7326/0003-4819-141-6-200409210-00007. [DOI] [PubMed] [Google Scholar]
- 15.Marcovecchio ML, Dalton RN, Prevost AT, Acerini CL, Barrett TG, Cooper JD, Edge J, Neil A, Shield J, Widmer B, et al. Prevalence of abnormal lipid profiles and the relationship with the development of microalbuminuria in adolescents with type 1 diabetes. Diabetes Care. 2009;32:658–663. doi: 10.2337/dc08-1641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Guy J, Ogden L, Wadwa RP, Hamman RF, Mayer-Davis EJ, Liese AD, D’Agostino R, Marcovina S, Dabelea D. Lipid and lipoprotein profiles in youth with and without type 1 diabetes: the SEARCH for Diabetes in Youth case-control study. Diabetes Care. 2009;32:416–420. doi: 10.2337/dc08-1775. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Nikkilä EA, Huttunen JK, Ehnholm C. Postheparin plasma lipoprotein lipase and hepatic lipase in diabetes mellitus. Relationship to plasma triglyceride metabolism. Diabetes. 1977;26:11–21. doi: 10.2337/diab.26.1.11. [DOI] [PubMed] [Google Scholar]
- 18.Taskinen MR. Quantitative and qualitative lipoprotein abnormalities in diabetes mellitus. Diabetes. 1992;41 Suppl 2:12–17. doi: 10.2337/diab.41.2.s12. [DOI] [PubMed] [Google Scholar]
- 19.Dabelea D, Talton JW, D’Agostino R, Wadwa RP, Urbina EM, Dolan LM, Daniels SR, Marcovina SM, Hamman RF. Cardiovascular risk factors are associated with increased arterial stiffness in youth with type 1 diabetes: the SEARCH CVD study. Diabetes Care. 2013;36:3938–3943. doi: 10.2337/dc13-0851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Soedamah-Muthu SS, Chaturvedi N, Witte DR, Stevens LK, Porta M, Fuller JH. Relationship between risk factors and mortality in type 1 diabetic patients in Europe: the EURODIAB Prospective Complications Study (PCS) Diabetes Care. 2008;31:1360–1366. doi: 10.2337/dc08-0107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Molitch ME, Rupp D, Carnethon M. Higher levels of HDL cholesterol are associated with a decreased likelihood of albuminuria in patients with long-standing type 1 diabetes. Diabetes Care. 2006;29:78–82. doi: 10.2337/diacare.29.01.06.dc05-1583. [DOI] [PubMed] [Google Scholar]
- 22.Hägg S, Thorn LM, Putaala J, Liebkind R, Harjutsalo V, Forsblom CM, Gordin D, Tatlisumak T, Groop P-H; on behalf of the FinnDiane Study Group. Incidence of Stroke According to Presence of Diabetic Nephropathy and Severe Diabetic Retinopathy in Patients With Type 1 Diabetes. American Diabetes Association. 2013;36:4140–4146. doi: 10.2337/dc13-0669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Writing Team for the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group. Sustained effect of intensive treatment of type 1 diabetes mellitus on development and progression of diabetic nephropathy: the Epidemiology of Diabetes Interventions and Complications (EDIC) study. JAMA. 2003;290:2159–2167. doi: 10.1001/jama.290.16.2159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.de Boer IH, Sun W, Cleary PA, Lachin JM, Molitch ME, Steffes MW, Zinman B. Intensive diabetes therapy and glomerular filtration rate in type 1 diabetes. N Engl J Med. 2011;365:2366–2376. doi: 10.1056/NEJMoa1111732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Rossing P, Hougaard P, Parving HH. Progression of microalbuminuria in type 1 diabetes: ten-year prospective observational study. Kidney Int. 2005;68:1446–1450. doi: 10.1111/j.1523-1755.2005.00556.x. [DOI] [PubMed] [Google Scholar]
- 26.Rossing P. Prediction, progression and prevention of diabetic nephropathy. The Minkowski Lecture 2005. Diabetologia. 2006;49:11–19. doi: 10.1007/s00125-005-0077-3. [DOI] [PubMed] [Google Scholar]
- 27.Liew G, Wong TY, Mitchell P, Cheung N, Wang JJ. Retinopathy predicts coronary heart disease mortality. Heart. 2009;95:391–394. doi: 10.1136/hrt.2008.146670. [DOI] [PubMed] [Google Scholar]
- 28.Studies to Treat or Prevent Pediatric Type 2 Diabetes Prevention Study Group. Prevalence of the metabolic syndrome among a racially/ethnically diverse group of U.S. eighth-grade adolescents and associations with fasting insulin and homeostasis model assessment of insulin resistance levels. Diabetes Care. 2008;31:2020–2025. doi: 10.2337/dc08-0411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ghosh S, Collier A, Hair M, Malik I, Elhadd T. MetS in type 1 diabetes. Int J Diabetes Mellitus. 2010;2:38–42. [Google Scholar]
- 30.Cleland SJ, Fisher BM, Colhoun HM, Sattar N, Petrie JR. Insulin resistance in type 1 diabetes: what is ‘double diabetes’ and what are the risks? Diabetologia. 2013;56:1462–1470. doi: 10.1007/s00125-013-2904-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Williams KV, Erbey JR, Becker D, Arslanian S, Orchard TJ. Can clinical factors estimate insulin resistance in type 1 diabetes? Diabetes. 2000;49:626–632. doi: 10.2337/diabetes.49.4.626. [DOI] [PubMed] [Google Scholar]
- 32.Distiller LA, Joffe BI, Brown V, Distiller GB. The effect of features of the metabolic syndrome on atherosclerotic risk in relatively long-surviving patients with type 1 diabetes. Metab Syndr Relat Disord. 2010;8:539–543. doi: 10.1089/met.2010.0036. [DOI] [PubMed] [Google Scholar]