

A 51-year-old man, whose history included an unspecified early-childhood valvular procedure, presented with shortness of breath. An echocardiogram revealed normal left ventricular function and mild-to-moderate pulmonary regurgitation with turbulent flow, but we were unable to further characterize the pulmonary valve on the basis of those images. Cardiac magnetic resonance (CMR) images (Figs. 1 and 2) showed a quadricuspid pulmonary valve with 3 equal-sized cusps and a rudimentary 4th cusp, incomplete cusp coaptation with a jet of mild pulmonary regurgitation, marked aneurysmal enlargement in the main and left pulmonary artery, no evidence of a prosthetic pulmonary valve, and normal biventricular function.
Fig. 1.

Cardiovascular magnetic resonance steady-state free-precession sequence shows closure (arrow) of 3 pulmonary valve cusps of equal size and 1 smaller, poorly formed cusp. Pulmonary valvular motion was also apparent throughout the cardiac cycle.
Supplemental motion image (2.4MB, m1v) is available for Figure 1.
Fig. 2.
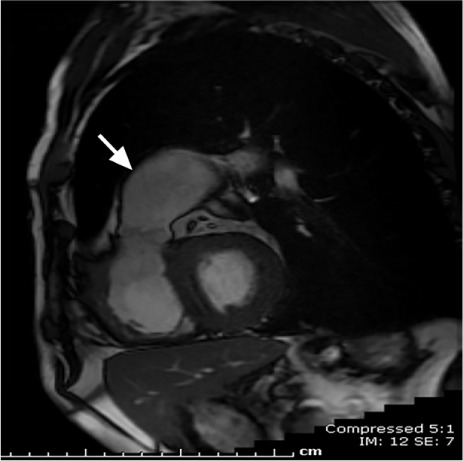
Cardiovascular magnetic resonance steady-state free-precession sequence of the pulmonary outflow tract shows the pulmonary artery aneurysm (arrow). Pulmonary valvular motion was also apparent.
Supplemental motion image (1.6MB, m1v) is available for Figure 2.
Comment
Quadricuspid pulmonary valve is a rarely identified abnormality occurring in isolation or with other congenital cardiovascular malformations. Descriptions have variously included 2 small and 2 large cusps; 4 cusps of equal size; and a rudimentary, deformed, shrunken, or fenestrated accessory cusp interposed between 3 cusps of equal size.1,2 In isolation, this malformation is not generally associated with significant clinical manifestations. Reported prevalences in postmortem specimens range from 1 in 400 to 1 in 1,000.1,3 Case reports have described a quadricuspid valve with documented severe pulmonary regurgitation4 and a quadricuspid valve with evidence of stenosis and severe regurgitation.5 In yet another report, CMR showed a quadricuspid pulmonary valve with 2 equally sized valves and 2 smaller, equal-sized valves, together with a pulmonary artery aneurysm.6
In regard to surgical therapy, there has been a report of surgical repair of a quadricuspid valve in association with severe pulmonary regurgitation and pulmonary artery aneurysm.7 In that case, the quadricuspid morphology of the valve (2 normal cusps, a sparrow-nest-shaped cusp, and a severely hypoplastic cusp) was discovered during surgery for severe pulmonary regurgitation and pulmonary artery aneurysm. Tricuspidization via annular plication at the level of the hypoplastic cusp was performed, together with pulmonary arterioplastic reduction.
The pulmonary valve's anatomic location renders the valve difficult to see by means of most noninvasive diagnostic methods. Our case shows that CMR can be useful for detailed noninvasive depiction of quadricuspid pulmonary valve abnormalities.
Footnotes
Section Editor: Raymond F. Stainback, MD, Department of Adult Cardiology, Texas Heart Institute, 6624 Fannin St., Suite 2480, Houston, TX 77030
References
- 1.Berdajs D, Lajos P, Zund G, Turina M. The quadricuspid pulmonary valve: its importance in the Ross procedure. J Thorac Cardiovasc Surg. 2003;125(1):198–9. doi: 10.1067/mtc.2003.115. [DOI] [PubMed] [Google Scholar]
- 2.Becker AE. Quadricuspid pulmonary valve. Anatomical observations in 20 hearts. Acta Morphol Neerl Scand. 1972;10(3):299–309. [PubMed] [Google Scholar]
- 3.Jashari R, Van Hoeck B, Goffin Y, Vanderkelen A. The incidence of congenital bicuspid or bileaflet and quadricuspid or quadrileaflet arterial valves in 3,861 donor hearts in the European Homograft Bank. J Heart Valve Dis. 2009;18(3):337–44. [PubMed] [Google Scholar]
- 4.Ascione L, Iengo R, Tuccillo B, D'Andrea A, De Michele M, Porto A et al. Quadricuspid pulmonary valve diagnosed by cardiac magnetic resonance. J Cardiovasc Med (Hagerstown) 2009;10(12):944–5. doi: 10.2459/jcm.0b013e328330306a. [DOI] [PubMed] [Google Scholar]
- 5.Kotani A, Nakagawa K, Yamamoto T, Hirano Y, Kimura H, Yamada S et al. Quadricuspid pulmonary valve with valvular stenosis and regurgitation identified by transthoracic echocardiography: a case report [in Japanese] J Cardiol. 2002;39(6):313–9. [PubMed] [Google Scholar]
- 6.Gentille Lorente DI. The pulmonary valve and the pulmonary artery. Eur Heart J. 2009;30(19):2326. doi: 10.1093/eurheartj/ehp289. [DOI] [PubMed] [Google Scholar]
- 7.Iosifescu AG, Dorobantu LF, Anca TM, Iliescu VA. Surgical treatment of a pulmonary artery aneurysm due to a regurgitant quadricuspid pulmonary valve. Interact Cardiovasc Thorac Surg. 2012;14(6):880–2. doi: 10.1093/icvts/ivs088. [DOI] [PMC free article] [PubMed] [Google Scholar]