

Abstract
Objective. To evaluate the efficacy and safety of large dosage of Chishao in formulae for treatment of cholestatic hepatitis. Methods. The major databases (PubMed, Embase, Cochrane Library, Chinese Biomedical Database Wanfang, VIP medicine information system, and China National Knowledge Infrastructure) were searched until January 2014. Randomized controlled trials (RCTs) of large dosage of Chishao in formulae that reported on publications in treatment of cholestatic hepatitis with total efficacy rate, together with the biochemical indices including alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin (TBIL), and direct bilirubin (DBIL), were extracted by two reviewers. The Cochrane tool was used for the assessment of risk of bias included trials. Data were analyzed with RevMan 5.2.7 software. Results. 11 RCTs involving 1275 subjects with cholestatic hepatitis were included. Compared with essential therapy, large dosage of Chishao in formulae demonstrated more efficiently with down regulation of serum ALT, AST, TBIL, DBIL. Meanwhile, there were no obvious adverse events. Conclusion. As a promising novel treatment approach, widely using large dosage of Chishao in formulae may enhance the curative efficacy for cholestatic hepatitis. Considering being accepted by more and more practitioners, further rigorously designed clinical studies are required.
1. Introduction
Cholestatic hepatitis presents the symptoms as abnormal bile generation, secretion, and excretion that leads to the intrahepatic accumulation of bile acids (BA) and other toxic compounds with progression of liver pathology. It is one of the most common but devastating manifestations in many liver diseases, and without proper treatment, it will ultimately result in cirrhosis and hepatic failure [1, 2]. Presently, there are 350 million to 400 million HBV infected individuals worldwide, and 2 percent of them suffer from cholestatic hepatitis along the progress [3, 4]. Cholestatic hepatitis known for its severe and prolong jaundice characteristic brings heavy burden to patients and society [5]. Current therapy, aiming at symptoms and mechanism, generally takes several measures such as vitamin for adequate nutrition, albumin and plasma for supporting treatment, symptomatic treatment to cutaneous pruritus, ursodeoxycholic acid (UDCA) or adrenocortical hormone for removing jaundice, and even transplantation. However, several unsatisfactory aspects and side effects could be seen in clinics, and the alternative medicine or treatment is more necessary.
Along with development of medical science, complementary and alternative medicine displays its unique role in hepatitis treatment [6–8]. Traditional Chinese medicine (TCM), known for its holistic concept and treatment based on syndrome differentiation, emphasizes formulae employment more than single drug use in treatment of diseases. Increasing current studies demonstrate that formulae with definite efficacy for specific disease regulate function of multiple organs and tissues in a way of network [9, 10]. In TCM, Yin Chen Hao Decoction has been widely used in treatment of jaundice. However, Yin Chen Hao Decoction usually fails in severe jaundice with the symptom of blood stasis. Chishao, owing to its function of blood invigoration, has been used in severe cholestatic hepatitis for decades and obtained satisfactory effects. Chishao, the dried root of Paeonia lactiflora pall or Paeonia veitchii Lynch, has been used for blood stasis and hyperactivity of liver-Yang in more than 2000 years. In 1983, Wang et al. proposed a novel approach of severe jaundice treatment by using large dosage of Chishao [11]. Following clinical studies, it suggested significant effect of Chishao in large dosage for cholestatic hepatitis [12]. Besides, Chishao in large dosage could ameliorate cholestasis induced by ANIT and bile duct ligation in animals [13]. By now, it demonstrates a promising treatment to use large dosage of Chishao on severe cholestasis in clinic. However, the systematic review on Chishao used in large dosage has not been seen. Therefore, this meta-analysis of RCTs was conducted to assess the clinical value of large dosage of Chishao relevant formulae for the treatment of cholestatic hepatitis.
2. Materials and Methods
2.1. Inclusion Criteria
The inclusion criteria were as follows. (1) Randomized controlled trials (RCTs) of patients diagnosed with cholestatic hepatitis met the criteria of Viral Hepatitis Prevention and Treatment Programs, Guidance for Clinical Research on New Drugs of TCM [25, 26]. (2) Chishao with large dose (more than 25 g, 2 times larger than the prescribed maximum dose of Chinese Pharmacopeia 2010 version) serves as the main element in formulae alone or in combination with conventional therapy compared with placebo, conventional therapy as controls. (3) Outcome measurements included one or more indices as total efficacy rate, alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin (TBIL), and direct bilirubin (DBIL).
2.2. Exclusion Criteria
The exclusion criteria were (1) reviews, nonclinical studies, and case observations, (2) no RCTs, and (3) controlled interventions with TCM therapies as other Chinese herbs or acupuncture.
2.3. Search Strategy
Comprehensive searches were both performed in English and Chinese databases including PubMed, Embase, Cochrane Library, Chinese Biomedical Database (CBM), Wanfang, VIP medicine information system (VMIS), and China National Knowledge Infrastructure (CNKI) from their inception to January 2014. Search terms included traditional Chinese medicine, Chishao, Paeonia lactiflora pall, Paeonia veitchii Lynch, large dose, hepatitis, cholestatic hepatitis, cholestasis, randomized controlled trial, and clinical controlled trial.
2.4. Data Extraction and Risk of Bias Assessment
Data extraction and quality assessment were independently performed by two researchers (Ma Xiao and He Xuan) and disagreements were resolved by consensus. Detailed data as study design, participants' information, interventions, outcome measures, and adverse event report were extracted to a conclusive table. Assessment of symptom improvement was based on Guidance for Clinical Research on New Drugs of TCM or Disease Diagnosis and Efficacy Standards of Chinese Internal Medicine.
Cochrane risk of bias tool was used to assess methodological quality of included RCTs. There are six domains including random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome data (attrition bias), incomplete outcome data (attrition bias), and selective reporting (reporting bias). The judgment was marked as “high risk,” “unclear risk,” or “low risk.” Trials that met all the criteria were categorized as high risk of bias, whereas those that met none of the criteria were categorized as low risk of bias. The others were classified as unclear risk of bias if insufficient information was available to make a judgment.
2.5. Data Analysis
Statistical analysis was performed by Cochrane RevMan 5.2.7 (Cochrane Collaboration). Dichotomous data were presented as risk ratio (RR) and continuous variables as mean difference (MD), with 95% confidence intervals (95% CI). Statistical heterogeneity was assessed by Cochrane's Q test. Data with low heterogeneity (P ≥ 0.10 and I 2 ≤ 50%) were performed as fixed-effects model whereas others performed as as random-effects model. A funnel plot was used for assessing the potential publication bias.
3. Results
3.1. Characteristics of Included Trials
A total of 1437 publications were identified for initial screen and 516 duplicated citations were removed. In the remaining 921 reports, 119 reviews/commentaries and 753 records irrelevant to the study were excluded. 49 full-text articles were used for further assessment. Among them, 18 nonrandomized controlled studies, 5 animal studies, 4 inconsistent criteria, 9 Chinese herbs in control group and 2 low dosage of Chishao were excluded. The rest of 11 eligible studies were conformed to meta-analysis (Figure 1).
Figure 1.
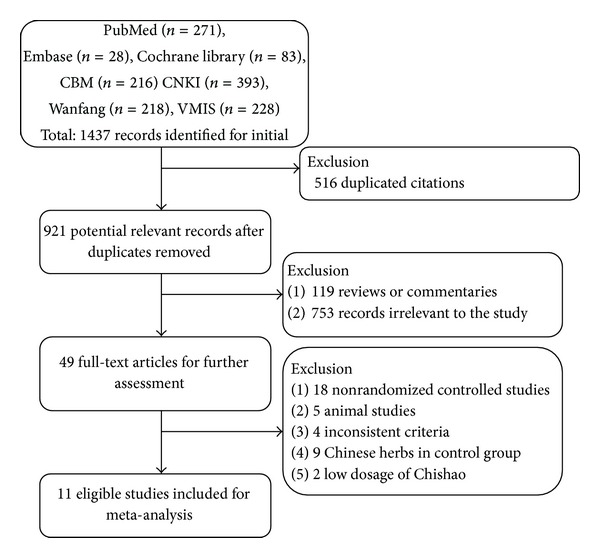
Flow diagram showing the trial selection process for the systematic review.
11 articles involving 1275 subjects with cholestatic hepatitis (751 cases in trials group, 524 cases in control group) were included in this study, and there was no significance in ages, sex, and course of disease between two groups (Table 1). Essential treatment with large dose Chishao formulae or single Chishao formulae was used in trials group, whereas essential treatment or single western medicine was applied in control group. 10 of 11 articles described treatment duration that ranged from 30 days to 2 months [14, 16–24] and 4 reported follow-up period from 2 weeks to 6 months [21–24]. Six articles reported advent events with or without slight side effect [14, 18, 21–24] (Table 2).
Table 1.
Characteristics of included studies.
| Author (reference) | Published year | Cases T/C |
Age (years) Range, mean |
Sex Male/female |
Course of disease (years) Range, mean |
|
|---|---|---|---|---|---|---|
| Tang et al. [14] | 2013 | 50/50 |
T: 24–65, 41.2 C: 23–67, 42.1 |
T: 37/13 C: 38/12 |
T: 0–0.7, 0.4 C: 0–0.8, 0.4 |
|
| Chen and Tu [15] | 2013 | 30/20 | NR | T: 20/10 C: 15/5 |
NR | |
| Wu [16] | 2012 | 45/45 |
T: 33–68, 47.9 C: 34–66, 48.4 |
T: 26/19 C: 23/22 |
T: 1–6, 3.4 C: 1–7, 3.1 |
|
| Xu et al. [17] | 2011 | 30/30 |
T: 18–53, 42.2 C: 16–58, 45.3 |
T: 18/12 C: 20/10 |
T: 0.1–3 C: 0.1–3.2 |
|
| Zhu [18] | 2010 | 45/45 |
T: 22–75, 44.6 C: 34–68, 46.1 |
T: 20/25 C: 22/23 |
T: 0.1–0.4 C: 0.1–0.3 |
|
| He et al. [19] | 2008 | 32/28 |
T: 16–61, 32 C: 17–59, 31 |
T: 19/13 C: 16/12 |
NR | |
| Xie et al. [20] | 2008 | 30/30 |
T: 22–61, 38.5 C: 19–65, 42.1 |
T: 22/8 C: 20/10 |
T: 0.1–6, 4.5 C: 0–10, 4.7 |
|
| Shu [21] | 2007 | 24/24 | 19–53 |
T: 36.2 C: 37.8 |
T: 20/4 C: 18/6 |
T: 0.2 C: 0.2 |
| Li [22] | 2006 | 32/31 |
T: 37.1 C: 37.3 |
T: 22/10 C: 17/14 |
T: 0.1 C: 0.1 |
|
| He et al. [23] | 2003 | 121/117 | NR | NR | NR | |
| He* et al. [24] | 2003 | 312/104 |
T: 39.8 C: 41.3 |
T: 233/79 C: 80/24 |
T: 0.1a, 3.1ch
C: 0.1a, 3.3ch |
|
Table 2.
Intervention and outcome measures of included studies.
| Study ID | Intervention | Duration/followup | Adverse events | Outcome measures | |
|---|---|---|---|---|---|
| Trials group (large dose Chishao formulae) |
Control group | ||||
| Tang et al. 2013 [14] | Yin Chen Xiao Dan decoction (Chishao 30 g) + Vitamin C + glucuronolactone + diammonium glycyrrhizinate Injection |
Vitamin C + glucuronolactone + diammonium glycyrrhizinate injection | 30 days/NR | NO | Total efficacy rate |
|
| |||||
| Chen and Tu 2013 [15] | Yin Chen Hao decoction jia wei (Chishao 60 g) + sparagin + diammonium glycyrrhizinate + vitamin C |
sparagin + diammonium glycyrrhizinate + vitamin C | NR | NR | Total efficacy rate, ALT, TBIL, γ-GT |
|
| |||||
| Wu 2012 [16] | Huo Xue Qing Dan decoction (Chishao 30 g) |
ademetionine injection | 2 months/NR | NR | Total efficacy rate, ALT, AST, TBIL, DBIL |
|
| |||||
| Xu et al. 2011 [17] | Chishao relevant formulae (Chishao 100 g) + essential treatment |
Essential treatment | Hospitalization time/NR | NR | Total efficacy rate, ALB, AST, TBIL, PT |
|
| |||||
| Zhu 2010 [18] | Chishao relevant formulae (Chishao 30 g–80 g) + diammonium glycyrrhizinate + vitamin K1 + sparagin + ademetionine or UDCA |
Diammonium glycyrrhizinate + vitamin K1 + sparagin + ademetionine or UDCA | 1-2 months/NR | NO | Total efficacy rate, ALT, TBIL, DBIL |
|
| |||||
| He et al. 2008 [19] | Chishao relevant formulae (Chishao 60 g) + diammonium glycyrrhizinate Injection + alprostadil injection + UDCA + vitamin C and vitamin BCO | diammonium glycyrrhizinate injection + alprostadil injection + UDCA + vitamin C and vitamin BCO | 4 weeks/NR | NR | Total efficacy rate, ALT, AST, TBIL, DBIL, TBA, CGT, ALP |
|
| |||||
| Xie et al. 2008 [20] | Chishao Tui Huang decoction (60–100 g) + diammonium glycyrrhizinate | diammonium glycyrrhizinate | 8 weeks/NR | NR | Total efficacy rate |
|
| |||||
| Shu 2007 [21] | Wen Li Huo Xue decoction (Chishao 25 g) + silymarine + Adenosine disodiu injection |
Galle Donau + silymarine + adenosine disodiu injection | 2 months/1-2 months | NO | Total efficacy rate, ALT, TBIL, GGT, ALP |
|
| |||||
| Li 2006 [22] | Jian Pi Li Dan decoction (Chishao 25 g) + vitamin K1 + vitamin BCO + glucuronolactone | Diammonium glycyrrhizinate injection + UDCA + vitamin K1 + vitamin BCO + Glucuronolactone | 40 days/3 months | T: 2 Cases/C: 4 Cases with light digestive tract side effect. | Total efficacy rate, TBIL, ALT, TBA, ALP |
|
| |||||
| He et al. 2003 [23] | Chi Dan Tui Huang granule | Galle Donau | 8 weeks/2 weeks–6 months | T: 2 Cases/C: 4 Cases with light digestive tract side effect. | Total efficacy rate, ALT, AST |
|
| |||||
| He* et al. 2003 [24] | Chi Dan Tui Huang granule | Galle Donau | 8 weeks/2 weeks–6 months | T: 13 Cases/C: 3 Cases with light digestive tract side effect. | Total efficacy rate, TBIL |
3.2. Methodological Quality of Included Trials
According to Cochrane risk of bias estimation, randomized allocation of participants was mentioned in all trials; however, 3 trials reported randomized methods [16, 23, 24] through number table and 2 through clinical sequence [14, 17]. Allocation concealment was performed in 2 of 11 articles [23, 24] and 1 mentioned blinding of participants and personnel and blinding of outcome assessment [23]. There were no incomplete outcome data or essential data missing in 6 reports [14, 18, 21–24], whereas others were unclear. Four articles mentioned systematic project in research [21–24] and others remained unclear (Figure 2).
Figure 2.
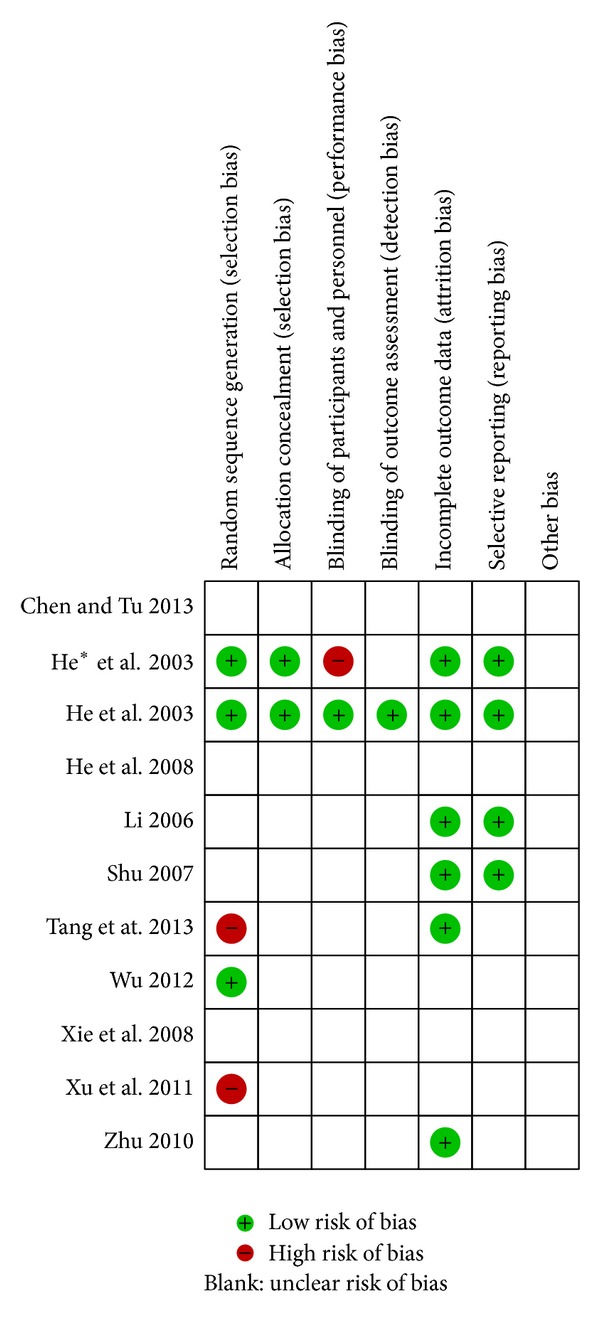
Methodological quality assessment for risk of bias for each included study.
3.3. Outcome Measures
3.3.1. Formulae with or without Essential Treatment versus Essential Treatment
Three of 11 articles described trials group with only Chishao formulae treatment, whereas the rest 8 RCTs reported combination treatment of Chishao formulae and essential drugs in trials group. No heterogeneity was displayed in both analyses and fixed effects model was used (P > 0.10). The results displayed RR with 95% CI in single application and combinations were 1.23 (1.13, 1.34) and 1.43 (1.29, 1.58). It revealed that formulae with large dosage of Chishao did demonstrate an exact efficacy in cholestatic hepatitis treatment whether combined application or not (Figure 3).
Figure 3.
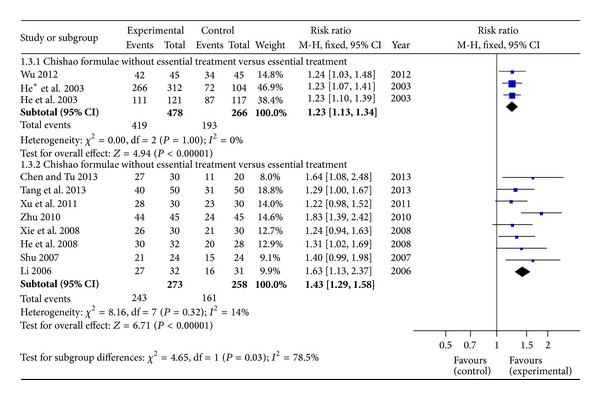
Forest plot of large dosage of Chishao relevant formulae with or without essential treatment versus essential treatment in patients with cholestatic hepatitis.
3.3.2. Serum Indices of Cholestatic Hepatitis Pathology
Serum ALT level was measured in 6 articles whereas 4 reported AST. TBIL level, the direct index of cholestatic hepatitis, was described in 9 trials and 4 displayed serum DBIL level. Heterogeneity occurred in indices of ALT, AST, TBIL, and DBIL (P < 0.10). Therefore, random effects model was adopted for analysis. The MDs with 95% CI of serum ALT, AST, TBIL, and DBIL level were −24.96 (−34.02, −15. 90), −22.84 (−31.60, −14.08), −30.28 (−42.55, −18.02), and −15.13 (−25.21, −5.04), respectively, indicating a significant pathologic indices decrease in trials group (Figure 4).
Figure 4.
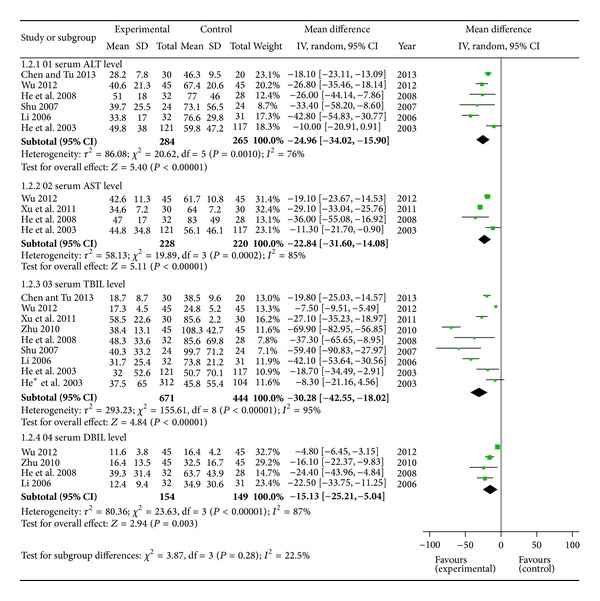
Forest plot of serum indices of cholestatic hepatitis pathology.
3.3.3. Efficacy Rate of Different Course of Disease
Cholestatic hepatitis was divided into two kinds of subtype according to the course of disease. In this study, the course of cholestatic hepatitis beyond 1 year was defined as long-term disease. Otherwise, cholestatic hepatitis within 1 year was classified to short term disease. There were 4 articles ascribed as short-term subtype and 3 as long-term subtype. On the basis of fixed effects model (P > 0.10), both of the results showed a significant difference between trials and control. RR with 95% CI was 1.53 (1.31,1.77) in shortterm and 1.23 (1.08,1.40) in long term (Figure 5).
Figure 5.
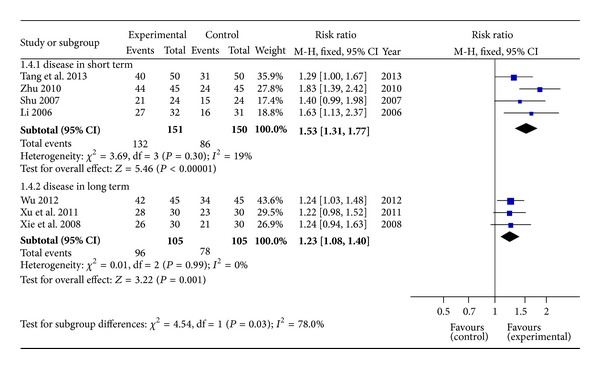
Forest plot of different course of cholestatic hepatitis.
3.4. Adverse Events
Among 11 RCTs, 3 [14, 18, 21] reported no side effect occurring in clinical trials. Another 3 [22–24] observed totally 28 cases of side effect presenting as light digestive tract symptom, but there was no causality assessment for this adverse event. In spite of no difference between trials and controls, systematic safety assessment of Chishao relevant formulae needed further investigation (Table 2).
3.5. Publication Bias
A funnel plot of large dosage of Chishao relevant formulae with essential treatment verses essential treatment in patients with cholestatic hepatitis was applied with RR as the x-axis and SE(RR) as the y-axis, respectively. The plot was symmetric, suggesting that the publication bias was little (Figure 6).
Figure 6.
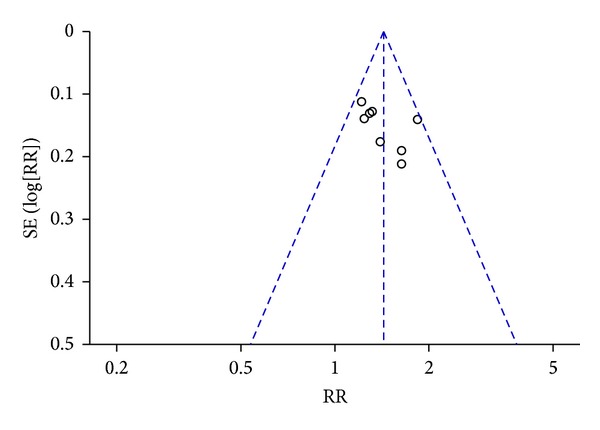
Funnel plot of large dosage of Chishao relevant formulae with essential treatment versus essential treatment in patients with cholestatic hepatitis.
4. Discussion
Cholestasis is defined as an impairment of bile secretion and flow followed by a lack of bile in intestine and accumulation of potentially toxic BA in the liver and the systemic circulation. Cholestasis results in intrahepatic retention of cytotoxic BA which can thus lead to liver injury or liver fibrosis [27, 28]. In cholestatic hepatitis, serum TBIL and DBIL are regarded as the sensitive diagnosis indices of cholestatic hepatitis, meanwhile, ALT and AST represent the liver function along with disease. It is well known that a variety of definite factors including infection, drug abuse, autoimmunity, heredity, gestation, and operation cause intrahepatic cholestasis. As for the mechanism of cholestatic hepatitis, more focus is localized on oxidative stress [29], inflammatory response [30], and relevant hepatocyte transporters [31, 32]. However, a systematic explanation still remains vague. At present, UDCA is recognized as the specific and potent medicine for cholestasis [33] and often combined with glucocorticoid [34]. But for long duration therapy, glucocorticoid may lead to several side effects, meanwhile UDCA will not always present stable efficacy. Transplantation, as the ultimate treatment, may result in severe immune rejection which is a devastating problem affecting quality of life. As one kind of alternative and complementary medicine, TCM shows the absolutely advantages in chronic diseases treatment. The integrated modulation to disease always involves in network style distributed to targets of molecules, tissues, and organs level [35, 36]. There are a variety of herbs and formulae in TCM that represent obvious effect of removing jaundice. Although different herbs and formulae may display different mechanisms [37], the ultimate manifestation in macro view reaches the same.
Chishao serves as an important drug of TCM. The main components are monoterpene glycosides, flavonoids, tannins, and phenolic acids [38, 39]. The herb and its active component consistently exhibit many pharmacological effects such as vasodilatation of thoracic aorta [40], antiallergic effect [41], liver protection [2], anti-inflammation, and immunoregulation [42]. However, application of large dosage of Chishao treating cholestatic hepatitis is a novel clinical practice in the recent 30 years [11]. Due to its unique efficacy, the therapeutic form is accepted by increasing practitioners. But from the safety and reasonable aspect, it brings about an essential question in TCM. Why can Chishao or even others as Rheum palmatum (Dahuang) and Coptis (Huanglian) be applied with such a large dosage? A recent study may reveal this answer related to the fact that different organic status represent different tolerance to drugs [43]. An experiment of Rheum palmatum extraction (RE) also indicates that RE, ranged certain dose, displays curative function in fibrosis animal but induces liver damage in normal [44]. Therefore, tolerance of pathologic status is relatively higher than normal one. Except that, the metabolism characteristic of Chishao is possibly another reason. The bioavailability of paeoniflorin and albiflorin in Chishao is also distinct, manifested as normal rats' bioavailability being lower compared with cholestasis hepatitis rats' [45]. Therefore, in specific pathologic status, large dosage of Chishao shall present the specific dose-effect relationship which will not be discovered in normal condition. According to both of the assumptions and examples, organic status may be the crucial and specific point to the therapy.
This systematic review included 11 randomized controlled trials and a total of 1275 participants. Large dosage of Chishao relevant formulae served as the key subject. It demonstrated a specific and potent effect for cholestasis hepatitis. As indices of hepatic pathology, the formulae led to a significant decrease in ALT, AST, TBIL, and DBIL compared with essential treatment. In addition, trials' serum level of TBIL presented the most dramatic decline, indicating a stronger removing jaundice effect than controls. Subgroup study of formulae without essential treatment manifested potent effect and formulae combined with essential treatment did also enhance the efficacy rate. The course of disease is another important factor which affects prognosis [46]. Different course of disease was investigated. The result illustrated that formulae were effective to the disease in short term or long term and acquired stronger effect than controls. Except Chishao, other herbs such as Dahuang, Yinchen, Danshen, and Gegen may also serve as important ingredients (see Supplementary Material available online at http://dx.doi.org/10.1155/2014/328152). Effects of liver protection and jaundice removing existed in these herbs. Six articles also proved that there were no obvious severe advent events occurring in RCTs. Light digestive tract symptom was observed, but there was no causality assessment for this adverse event. From the systematic analysis, large dosage of Chishao relevant formulae exhibits a promising therapy for cholestasis hepatitis.
As the requirement for medical research in translational medicine, conventional drug discovery, as style of single target to animals, faces many challenges [47]. On the contrary, TCM presents abundant experiences in clinical treatment. Fundamental research can also be sustained or indicated through this treasure. Although clinical application is mature, the mechanism of Chishao relevant formulae's effect remains far from explicit. Therefore, further focus ought to be localized on internal relationship between the formulae and their effect through the model of “clinic-experiment-clinic.”
5. Conclusions
Large dosage of Chishao relevant formulae may promote the curative efficacy of cholestasis hepatitis, which is a promising novel treatment approach. Considering being accepted by widespread practitioners, more rigorously designed multicenter, double-blind, randomized, and large-scale controlled trials are required.
Supplementary Material
Affiliated Table in supplementary information showed the study ID, formulae name, dosage of Chishao and other Chinese herbal medicine in formula.
Acknowledgments
The current work was supported by the Major Projects of the National Science and Technology (no. 2012ZX10005010-002-002) and the National Natural Science Foundation Project of China (nos. 81303120 and 81173571).
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
Authors' Contribution
Xiao Ma and Ji wang contributed equally to this paper.
References
- 1.Jin F, Cheng D, Tao JY, et al. Anti-inflammatory and anti-oxidative effects of corilagin in a rat model of acute cholestasis. BMC Gastroenterology. 2013;13(1, article 79) doi: 10.1186/1471-230X-13-79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Zhao Y, Zhou G, Wang J, et al. Paeoniflorin protects against ANIT-induced cholestasis by ameliorating oxidative stress in rats. Food and Chemical Toxicology. 2013;58:242–248. doi: 10.1016/j.fct.2013.04.030. [DOI] [PubMed] [Google Scholar]
- 3.Zhu C, Cao H, Zhou X, et al. Meta-analysis of the clinical value of danshen injection and huangqi injection in liver cirrhosis. Evidence-Based Complementary and Alternative Medicine. 2013;2013:8 pages. doi: 10.1155/2013/842824.842824 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Yang D, Gao GJ, Wei K, Wang XJ, Sun FX. Clinical analysis of cholestatic hepatitis characteristic. Chinese Journal of Clinicians. 2011;5(24):7423–7424. [Google Scholar]
- 5.Yang D, Sun FX, Gao GJ, Wei K, Wang XJ. Evaluation on herbal Yudan decoction on treatment of acute cholestatic hepatitis. Chinese Journal of Liver Diseases. 2013;5(3):9–11. [Google Scholar]
- 6.Zhang L, Wang G, Hou W, Li P, Dulin A, Bonkovsky HL. Contemporary clinical research of traditional chinese medicines for chronic hepatitis B in china: an analytical review. Hepatology. 2010;51(2):690–698. doi: 10.1002/hep.23384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Xia Y, Luo H, Liu JP, Gluud C. Phyllanthus species for chronic hepatitis B virus infection. Cochrane Database of Systematic Reviews. 2011;(4) doi: 10.1002/14651858.CD008960.pub2.CD008960 [DOI] [PubMed] [Google Scholar]
- 8.Liu HM, Wang XB, Chang YJ, Gu LL. Systematic review and meta-analysis of randomized controlled trials of integrative medicine therapy for treatment of chronic severe hepatitis. Journal of Chinese Integrative Medicine. 2012;10(11):1211–1228. doi: 10.3736/jcim20121104. [DOI] [PubMed] [Google Scholar]
- 9.Li S, Zhang B. Traditional Chinese medicine network pharmacology: theory, methodology and application. Chinese Journal of Natural Medicines. 2013;11(2):110–120. doi: 10.1016/S1875-5364(13)60037-0. [DOI] [PubMed] [Google Scholar]
- 10.Li S, Zhang ZQ, Wu LJ, Zhang XG, Li YD, Wang YY. Understanding ZHENG in traditional Chinese medicine in the context of neuro-endocrine-immune network. IET Systems Biology. 2007;1(1):51–60. doi: 10.1049/iet-syb:20060032. [DOI] [PubMed] [Google Scholar]
- 11.Wang CB, He JP, Lei ZY, Chen JM. Treating cholestatic hepatitis with large dosage of Chishao for cooling blood and promoting blood flow—13 cases report. Journal of Traditional Chinese Medicine. 1983;(6):30–32. [Google Scholar]
- 12.He JP, Wang CB. Treatment of severe cholestatic hepatitis by integrative medicines. Chinese Journal of Integrative Medicine. 1998;4(1):18–21. [Google Scholar]
- 13.Wei SS, Zhao YL, Jiang FJ, et al. Investigation of high dosage of Paeoniae Radix Rubra against ANIT-induced acute cholestasis hepatitis in rats. Chinese Journal of Experimental Traditional Medical Formulae. 2012;18(12):151–155. [Google Scholar]
- 14.Tang XQ, Xu WQ, Cheng XJ. Yinchen Xiaodan method combined with western medicine in treatment of chronic hepatitis B with intrahepatic cholestasis randomized parallel controlled study. Journal of Practical Traditional Chinese Internal Medicine. 2013;27(3):79–80. [Google Scholar]
- 15.Chen ZQ, Tu YY. Clinical observation of 30 cases of cholestatic hepatitis treating with ancient Jiawei prescription. Inner Mongol Journal of Traditional Chinese Medicine. 2013;12:18–19. [Google Scholar]
- 16.Wu QB. control observation of Huoxue Qingdan decoction in treating chronic cholestatic hepatitis. Journal of Practical Traditional Chinese Internal Medicine. 2012;26(8):49–51. [Google Scholar]
- 17.Xu CJ, Guo WS, Xie YF. Clinical observation of 30 cases of severe cholestatic hepatitis treating with combined tratitional Chinsese medicine and western medicine. Modern Journal of Integrated Traditional Chinese and Western Medicine. 2011;20(20):2531–2532. [Google Scholar]
- 18.Zhu XJ. Clinical observation of cholestatic hepatitis treated with large dose Chishao. Clinical Journal of Traditional Chinese Medicine. 2010;22(2):144–145. [Google Scholar]
- 19.He SM, Huang B, Deng X. 32 Cases of severe cholestatic hepatitis treated with Chi Yin Tui Huang decoction combined with western medicine. Shaanxi Journal of Traditional Chinese Medicine. 2008;29(5):564–566. [Google Scholar]
- 20.Xie CJ, Ma WB, Li RC, Wang SY. 60 Cases of cholestatic hepatitis treated with Chishao Tuihuang decoction research. Capital Medicine. 2008;6:p. 49. [Google Scholar]
- 21.Shu ZE. Clinical Observation of Chronic Cholestatic Hepatitis Treated with Wen Li Huo Xue Decoction. Hubei University of Chinese Medicine; 2007. [Google Scholar]
- 22.Li YF. Clinical Observation of Chronic Viral Cholestatic Hepatitis After Treatment with Jian Pi Li Dan Decoction. Hubei University of Chinese Medicine; 2006. [Google Scholar]
- 23.He JP, Wang CB, Ding JB, et al. Comparison of Chidan Tuihuang granule and Galle-Donau in the treatment of acute and chronic viral cholestatic hepatitis. Chinese Journal of New Drugs. 2003;12(3):209–212. [Google Scholar]
- 24.He JP, Wang CB, Ding JB, et al. Open comparative study of Chidan Tuihuang granule in treating acute and chronic viral cholestatie hepatitis. Chinese Journal of Integrated Traditional and Wetern Medicine. 2003;23(7):498–500. [Google Scholar]
- 25.Chinese Medical Association. Viral hepatitis prevention and treatment programs. Infectious Disease Information. 2000;13(4):141–150. [Google Scholar]
- 26.Zheng XY. Guidance for Clinical Research on New Drugs of TCM. China Medical Science Press; 2002. [Google Scholar]
- 27.Poupon R, Chazouilleres O, Poupon RE. Chronic cholestatic diseases. Journal of Hepatology. 2000;32(1, supplement):129–140. doi: 10.1016/s0168-8278(00)80421-3. [DOI] [PubMed] [Google Scholar]
- 28.Kakizaki S, Takizawa D, Tojima H, Horiguchi N, Yamazaki Y, Mori M. Nuclear receptors CAR and PXR; therapeutic targets for cholestatic liver disease. Frontiers in Bioscience. 2011;16(7):2988–3003. doi: 10.2741/3893. [DOI] [PubMed] [Google Scholar]
- 29.Anthérieu S, Azzi PB, Dumont J, et al. Oxidative stress plays a major role in chlorpromazine-induced cholestasis in human HepaRG cells. Hepatology. 2013;57(4):1518–1529. doi: 10.1002/hep.26160. [DOI] [PubMed] [Google Scholar]
- 30.Allen K, Jaeschke H, Copple BL. Bile acids induce inflammatory genes in hepatocytes: a novel mechanism of inflammation during obstructive cholestasis. The American Journal of Pathology. 2011;178(1):175–186. doi: 10.1016/j.ajpath.2010.11.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Geier A, Wagner M, Dietrich CG, Trauner M. Principles of hepatic organic anion transporter regulation during cholestasis, inflammation and liver regeneration. Biochimica et Biophysica Acta—Molecular Cell Research. 2007;1773(3):283–308. doi: 10.1016/j.bbamcr.2006.04.014. [DOI] [PubMed] [Google Scholar]
- 32.Keppler D. Cholestasis and the role of basolateral efflux pumps. Zeitschrift für Gastroenterologie. 2011;49(12):1553–1557. doi: 10.1055/s-0031-1281755. [DOI] [PubMed] [Google Scholar]
- 33.Buryova H, Chalupsky K, Zbodakova O, et al. Liver protective effect of ursodeoxycholic acid includes regulation of ADAM17 activity. BMC Gastroenterology. 2013;13(1, article 155) doi: 10.1186/1471-230X-13-155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Arenas F, Hervias I, Úriz M, Joplin R, Prieto J, Medina JF. Combination of ursodeoxycholic acid and glucocorticoids upregulates the AE2 alternate promoter in human liver cells. Journal of Clinical Investigation. 2008;118(2):695–709. doi: 10.1172/JCI33156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Fang Z, Lu B, Liu M, et al. Evaluating the pharmacological mechanism of Chinese medicine Si-Wu-Tang through multi-level data integration. PLoS ONE. 2013;8(11) doi: 10.1371/journal.pone.0072334.e72334 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Liu J, Pei M, Zheng C, et al. A systems-pharmacology analysis of herbal medicines used in health improvement treatment: predicting potential new drugs and targets. Evidence-Based Complementary and Alternative Medicine. 2013;2013:17 pages. doi: 10.1155/2013/938764.938764 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Zhang A, Sun H, Qiu S, Wang X. Advancing drug discovery and development from active constituents of Yinchenhao Tang, a famous traditional Chinese medicine formula. Evidence-Based Complementary and Alternative Medicine. 2013;2013:6 pages. doi: 10.1155/2013/257909.257909 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Wang YZ, Feng WS, Shi RB, Liu B, Jiang YY. Monoterpenes of Paeonia lactiflora Pall. Chinese Pharmaceutical Journal. 2008;43(9):669–671. [Google Scholar]
- 39.Yang YY, Zhou G, Ma XK, et al. Research progress of Paeonia lactiflora Pall. Herald of Medicine. 2008;27(1):67–69. [Google Scholar]
- 40.Jin SN, Wen JF, Wang TT, Kang DG, Lee HS, Cho KW. Vasodilatory effects of ethanol extract of Radix Paeoniae Rubra and its mechanism of action in the rat aorta. Journal of Ethnopharmacology. 2012;142(1):188–193. doi: 10.1016/j.jep.2012.04.035. [DOI] [PubMed] [Google Scholar]
- 41.Lee B, Shin YW, Bae EA, et al. Antiallergic effect of the root of Paeonia lactiflora and its constituents paeoniflorin and paeonol. Archives of Pharmacal Research. 2008;31(4):445–450. doi: 10.1007/s12272-001-1177-6. [DOI] [PubMed] [Google Scholar]
- 42.He DY, Dai SM. Anti-inflammatory and immunomodulatory effects of Paeonia lactiflora Pall., a traditional Chinese herbal medicine. Frontiers in Pharmacology. 2011;2, article 10 doi: 10.3389/fphar.2011.00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Bourbonnais É, Raymond V, Éthier C, et al. Liver fibrosis protects mice from acute hepatocellular injury. Gastroenterology. 2012;142(1):130.e4–139.e4. doi: 10.1053/j.gastro.2011.09.033. [DOI] [PubMed] [Google Scholar]
- 44.Wang JB, Zhao HP, Zhao YL, et al. Hepatotoxicity or hepatoprotection? pattern recognition for the paradoxical effect of the chinese herb Rheum palmatum L. in treating rat liver injury. PLoS ONE. 2011;6(9) doi: 10.1371/journal.pone.0024498.e24498 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Jiang F, Zhao Y, Wang J, et al. Comparative pharmacokinetic study of paeoniflorin and albiflorin after oral administration of Radix Paeoniae Rubra in normal rats and the acute cholestasis hepatitis rats. Fitoterapia. 2012;83(2):415–421. doi: 10.1016/j.fitote.2011.12.009. [DOI] [PubMed] [Google Scholar]
- 46.Liaw YF. Impact of therapy on the outcome of chronic hepatitis B. Liver International. 2013;33(supplement 1):111–115. doi: 10.1111/liv.12057. [DOI] [PubMed] [Google Scholar]
- 47.Marincola FM. Translational medicine: a two-way road. Journal of Translational Medicine. 2003;1(1, article 1) doi: 10.1186/1479-5876-1-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Affiliated Table in supplementary information showed the study ID, formulae name, dosage of Chishao and other Chinese herbal medicine in formula.