

Abstract
The long-term social sequelae of adolescent depressive symptoms were examined in a multi-method, multi-reporter study of a diverse community sample of 179 adolescents followed from age 14 to 24. Even mild to moderate levels of early adolescent depressive symptoms strongly predicted loneliness, lower maternal relationship quality, and problematic interactions with romantic partners in adulthood, even after accounting for prior levels of social functioning and concurrent levels of adult depressive symptoms. Predictions were partially mediated via late adolescent avoidance of social interactions and poor maternal relationship quality. Results are interpreted as suggesting the potential impact of depressive symptoms on core tasks of adolescent social development, with potential implications for the need for treatment of even mild symptoms and their social concomitants.
A core challenge in developmental psychopathology is understanding the process by which development can lead to pathology; yet understanding the converse process—the way in which pathology may interfere with future development—has typically received far less attention. This study examines the sequelae of one potentially insidious form of pathology—mild depressive symptoms—experienced at a particularly sensitive period for social development in early adolescence, in terms of its long-term effects on adult social functioning.
Although almost all of the long-term outcome research in this area has focused on adolescents’ diagnosable major depression (Fergusson, 2007; Kasen, Cohen, Skodol et al., 2001; Lewinsohn, Rohde, Seeley et al., 2000), even more minor symptoms of depression may have significant consequences (Gotlib, Lewinsohn, & Seeley, 1995; Pine, Cohen, Cohen et al., 1999). Although the long-term social sequelae of milder depressive symptoms in early adolescence have received scant attention, there is good reason to believe that early adolescence is a period that is particularly sensitive to the negative effects of such symptoms.
Adolescence is a critical period for the development of adult-like social relationship skills with parents, peers, and romantic partners (Aquilino, 2006; Roisman, Masten, Coatsworth et al., 2004). In terms of neurological development, the world of adult-like relationships is first opening up to the early adolescent, as brain structures closely tied to adult social functioning (e.g., the prefrontal and parietal cortex) begin to take on their final form (Blakemore & Choudhury, 2006). The developmental tasks of learning to establish and maintain newly intense social relationships typically require and receive extreme levels of attention from the developing adolescent (Collins & Laursen, 2004) and are thus likely to be particularly susceptible to disruption by depressive symptoms that reduces the level of energy available for them.
Difficulties in first experiences with adult-like relationships are also likely to provide the adolescent with a template that will partly anchor expectations of relationships going forward. Yet, these experiences are likely to be particularly problematic for depressed adolescents (Connolly, Geller, Marton et al., 1992; Daley & Hammen, 2002; Stice, Ragan, & Randall, 2004). Depressed individuals tend to recall feedback from others more negatively (Gotlib, Lewinsohn, & Seeley, 1998) and may thus end up wanting to avoid relationships, which in turn may lead to further social deficits. A similar process has been observed in short-term studies (e.g., over a one-year period) in adolescents experiencing major depressive episodes (Rohde, Lewinsohn, & Seeley, 1994). Given the uniquely challenging social developmental tasks of early adolescence, however, even teens experiencing milder depressive symptoms would seem potentially vulnerable to substantial social impairment in both the short and long-term.
Beyond daily peer interactions, potential long-term sequelae of depressive symptoms seem likely to extend to more intimate and enduring relationships. Maintaining supportive relationships with parents, for example, is a complex and challenging task in adolescence (Allen, Hauser, Bell et al., 1994) that might easily be disrupted by depressive symptoms. These depressive symptoms create intense needs for symptom relief and reassurance that cannot be easily assuaged in close relationships (Hammen, 2000) and that potentially lead to disruption in adolescents’ underlying working models of attachment (Allen, McElhaney, Kuperminc et al., 2004). A similar process has been observed in intense romantic relationships, which depressed individuals appear particularly likely to seek out, but to then find dissatisfying (Gotlib, et al., 1998).
Although the long-term sequelae of sub-clinical levels of adolescent depressive symptoms have received scant attention to date, even relatively modest social impairments resulting from such symptoms can have surprisingly large costs if these impairments extend past adolescence. In adulthood, loneliness and social isolation predict not only a greater likelihood of future depression (Coyne, 1976; Joiner, 2002), but a host of deleterious outcomes including poorer immune functioning (Pressman, Cohen, Miller et al., 2005), elevated cortisol levels (Cacioppo, Ernst, Burleson et al., 2000), sleep disturbances (Hawkley, Burleson, Berntson et al., 2003), higher systolic blood pressure (Hawkley, Masi, Berry et al., 2006), and higher cholesterol levels (O’Reilly & Emerson Thomas, 1989). Alienation from parental relationships is equally problematic, as parent-adult child relationships have been found to be crucial to early adult individuation and adjustment (Aquilino, 2006; Lerner, Lerner, von Eye et al., 1996; Powers, Hauser, & Kilner, 1989). Numerous studies have linked global social isolation and loneliness to early mortality (Pennix, van Tilburg, Kriegsman et al., 1997; Seeman, 2000; Sugisawa, Liang, & Liu, 1994), with social isolation creating a greater potential risk for early mortality than even cigarette smoking (House, Landis, & Umberson, 1988). Despite the magnitude of these consequences, virtually no research has examined whether early adolescents experiencing subclinical levels of depressive symptoms might be vulnerable to such impairments over the longer term.
This study examined the role of depressive symptoms as predictors of long-term impairment in social functioning in a socio-economically diverse community sample followed from age 14 through 23. Five specific hypotheses were examined to assess the nature of the relation of early adolescent depressive symptoms to markers of social adaptation in early adulthood:
Early adolescent depressive symptoms will display long-term continuities with adult loneliness and with lower maternal and romantic relationship quality.
Predictions from depressive symptoms will obtain even after excluding adolescents with the highest levels of early adolescent symptoms (e.g., those above clinical screening cutoffs).
Predictions will exist even after accounting for baseline markers of peer and maternal relationship quality.
Predictions will be found over and above effects of concurrent depressive symptoms in early adulthood.
Predictions to early adulthood will be mediated via greater tendencies toward social avoidance and reduced quality of maternal relationships in late adolescence.
Methods
Participants
This report is drawn from a larger longitudinal investigation of adolescent social development in familial and peer contexts. Initial participants included 184 seventh and eighth graders (86 male and 98 female) followed over a 10-year period from ages 14 to 24. Adolescents were first assessed annually over a three-year period in early adolescence (at ages 14.29 (SD=.75) at Wave 1; and 15.22 (SD = .80) at Wave 2; and 16.35 (SD=.87) at Wave 3). They were repeatedly assessed thereafter, up through the final two assessments at ages 22.8 (SD = .96) and 23.8 (SD =.97).
Adolescents were recruited from the 7th and 8th grades of a public middle school drawing from suburban and urban populations in the Southeastern United States. Students were recruited via an initial mailing to all romantic partners of students in the school along with follow-up contact efforts at school lunches. Families of adolescents who indicated they were interested in the study were contacted by telephone. Of all students eligible for participation, 63% agreed to participate either as either target participants or as peers providing collateral information. All participants provided informed assent before each interview session, and romantic partners provided informed consent. Interviews took place in private offices within a university academic building.
The sample was racially/ethnically and socioeconomically diverse: 107 adolescents (58%) identified themselves as Caucasian, 53 (29%) as African American, 15 (8%) as of mixed race/ethnicity and 9 (5%) as being from other minority groups. Adolescents’ parents reported a median family income in the $40,000 – $59,999 range.
Follow-up and Attrition Analyses
Follow-up data were obtained for 179 (97.3%) of the original 184 participants at ages 20 to 23 in early adulthood. For participants who were in a romantic relationship lasting 3 months or longer between ages 21 and 23, 92 romantic partners also participated with target participants in an observational discussion task. Participants’ mothers were surveyed when participants were in early adulthood and reports from 125 mothers were obtained.
Comparisons of the 179 participants from whom we had follow-up data vs. the 5 for whom we didn’t (one of whom was deceased and one of whom had become intellectually disabled) indicated that those not continuing had lower initial levels of family income but were otherwise statistically indistinguishable from continuing participants. Comparisons of baseline data for participants with and without observational data from romantic partners at follow-up indicated that those without observational data from romantic partners did not differ from those with such data on any baseline measures. Comparisons of baseline data for participants with and without maternal report data in early adulthood indicated that those without maternal report data had lower family incomes in early adolescence than those who had such data, but did not differ on any other baseline measures.
To best address any potential biases due to attrition in longitudinal analyses, full imputation maximum likelihood (FIML) methods were used with analyses including all variables that were linked to future missing data (i.e., where data were not missing completely at random). Because these procedures have been found to yield the least biased estimates when all available data are used for longitudinal analyses (vs. listwise deletion of missing data), the entire original sample of 184 was utilized for these analyses. This full sample thus provides the best possible estimates of long-term social outcomes, and was least likely to be biased by missing data. Alternative longitudinal analyses using just those participants without missing data (i.e., listwise deletion) yielded results that were substantially identical to those reported below. In sum, analyses suggest that, with the exception of romantic partner data, where substantial attrition would be expected but was not related to baseline measures, attrition was quite modest overall and not likely to have distorted any of the findings reported.
Procedure
In the initial introduction and throughout all sessions, confidentiality was assured to all study participants and adolescents were told that their parents, friends, and romantic partners would not be informed of any of the answers they provided. Participants’ data were covered by a Confidentiality Certificate issued by the U.S. Department of Health and Human Services, which protected information from subpoena by federal, state, and local courts. Transportation and childcare were provided if necessary. Adolescent/adult participants, their mothers, and their romantic partners were all paid for participation.
Measures
Depressive Symptoms (ages 14–16, 23–24)
Adolescents reported the degree of their depressive symptoms using the Child Depression Inventory (Kovacs & Beck, 1977). This 27-item inventory is based on the Beck Depression Inventory and has been well-validated as a measure of depressive symptomatology linked to poor self-esteem, hopelessness, and negative cognitive attributions (Kazdin, 1990). Scores were summed and then averaged across assessments at ages 14, 15 and 16 to produce an overall depressive symptoms score for early adolescence. Internal consistency for this measure was good (Cronbach’s α =.93).
At age 23 and 24, participants completed the Beck Depression Inventory, a 21-item measure designed to assess the degree of depressive symptoms in late adolescents and adults (BDI; Beck & Steer, 1987). Items were rated on a 0 to 3 scale and summed to yield a total depression score, with higher scores indicating more severe depressive symptoms. The BDI is a well-validated and widely accepted self-report measure of adult depressive symptomatology (Kazdin, 1990). Scores were summed and averaged across assessments at ages 23 and 24 to produce an overall depressive symptoms score for early adulthood. Internal consistency for this measure was good (Cronbach’s α =.91).
Both the CDI and BDI use a continuum/severity vs. a threshold approach, recognizing that higher levels of depressive symptoms that do not necessarily meet diagnostic thresholds may still be important in predicting future dysfunction (Lewinsohn, Solomon, Seeley, & Zeiss, 2000).
Adult Maternal Relationship Quality (Age 23) was assessed via maternal report from the Network of Relationships Inventory (Furman & Buhrmester, 1985), which obtains ratings on a series of five-point Likert scales. A total positivity score was obtained by summing six three-item scales for companionship, intimacy, nurturance, admiration, overall support and satisfaction. Internal consistency for this meta-scale was good (Cronbach’s α = .89 and reliability and validity have been previously documented (Furman, 1998).
Attachment to Mother (Ages 14–16, 18–20)
The Inventory of Parent and Peer Attachment (Armsden & Greenberg, 1987) was used to assess adolescents’ perceptions of the quality of their overall attachment to their mother in early and late adolescence. Total attachment quality is calculated as the sum of 14 5-point Likert-scale items capturing communication and trust and seven 5-point items (reverse-scored) capturing alienation in the relationship. Scores were summed and then averaged across assessments at ages 14, 15, and 16, and ages 18, 19, and 20 to produce overall scores for early and for late adolescence. Internal consistency was good at both points (Cronbach’s α’s =.92 and .97, respectively).
Attachment to Peers (Age 14–16)
The Inventory of Parent and Peer Attachment (Armsden, et al., 1987) was used to assess adolescents’ perceptions of the quality of their overall attachment to their peers in early adolescence. Total attachment was calculated as the sum of 14 5-point Likert-scale items capturing communication and trust and seven 5-point items (reverse-scored) capturing alienation in the relationship. Scores were summed and then averaged across assessments at ages 14, 15, and 16 to produce an overall score for early adolescence. Internal consistency for this scale was good (Cronbach’s α = .96).
Social Avoidance (Age 19–21) was assessed from the four-item general social avoidance scale from the Social Anxiety Scale for Adolescents (La Greca & Lopez, 1998). This scale has good psychometric properties and has been related concurrently to broad peer group acceptance and close friendship competence (La Greca, et al., 1998). Scores were summed and averaged across assessments at ages 19, 20, and 21 to produce an overall score for late adolescence. Internal consistency for this scale was good (Cronbach’s α = .87).
Loneliness (Age 23–24) was assessed via the UCLA Loneliness Scale (Russell, Peplau, & Cutrona, 1980). This 20-item measure assesses loneliness using responses on a 4-point Likert-scale. Scores have been related to outcomes ranging from lower life satisfaction to attachment insecurity (Bowlby, 1969/1982; Goswick & Jones, 1982; Kobak & Sceery, 1988; Moore & Schultz, 1983). Scores were summed and then averaged across assessments at ages 23 and 24 to produce an overall score for early adulthood. Internal consistency for this scale was good (Cronbach’s α = .97).
Observed Negativity in Romantic Relationships
Target adult-romantic partner dyads (for relationships of at least three months duration) participated in an 8-minute videotaped task in which they were presented with a hypothetical ‘dating court’ scenario in which partners were asked to separately make judgments about which member of a dating couple was correct in each of a series of hypothetical disagreements over matters ranging from meeting parents to clothing choice to time spent with friends vs. partner. After making their decisions separately, target adults and their partners were then brought together in a revealed differences paradigm in which they could compare their answers and then try to come to a consensus (Strodtbeck, 1951).
The Autonomy-Relatedness Coding System was used to code these interactions (Allen, Porter, & McFarland, 2001; Allen, Porter, McFarland et al., 2007). This system yields a score for target adults’ behavior toward their partners in the interaction. Ratings are molar in nature, yielding overall scores for behavior across the entire the interaction; however, these molar scores are derived from an anchored coding system that considers both the frequency and intensity of each speech relevant to that behavior during the interaction in assigning the overall molar score. The score for observed negativity sums ratings of behaviors undermining the relationship by overtly expressing hostility toward one’s partner, or by rudely interrupting/ignoring the partner. Inter-rater reliability was calculated using intraclass correlation coefficients and was in what is considered “good” range (intraclass r =.66) (Cicchetti & Sparrow, 1981).
Results
Preliminary Analyses
Means and standard deviations for all variables examined in the study are presented in Table 1. Initial analyses examined the role of gender and family income in early adolescence on the primary substantive measures used in the study. Several substantive variables were related to income in the adolescent’s family of origin and to adolescent gender, hence these factors are considered and described as covariates in analyses below. We also examined possible moderating effects of these demographic factors on each of the relationships described in the primary analyses below. Moderation effects were assessed by creating interaction terms based on the product of the centered main effect variables. No moderating effects of adolescent gender or fmaily income were found beyond what would be expected by chance.
Table 1.
Means, Standard Deviations, and Intercorrelations of Substantive Variables
| Mean | SD | Depression (23–24) | Loneliness (23–24) | Maternal Relship. Quality (23) | Negativty Romantic Rels. (22) | Attch, To Peers (14–16) | Attch. To Mthr (14–16) | Social Avoidance (19–21) | Attch To Mthr (18–20) | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Depression (14–16) | 6.61 | 5.23 | 35*** | 52*** | −30*** | 23* | −29*** | −23** | 46*** | −41*** |
| 2. Depression (23–24) | 5.07 | 5.31 | -- | 54*** | 08 | 29** | −08 | 01 | 31*** | −21** |
| 3. Loneliness (23–24) | 12.3 | 11.9 | -- | −21* | −01 | −28*** | −09 | 51*** | −32*** | |
| 4. Maternal Rel Quality (23) | 73.9 | 12.2 | -- | 17 | 17 | 49*** | −13 | 38*** | ||
| 5. Negativity in Romantic Relationship (23) | 0.52 | 0.73 | -- | −14 | −06 | 16 | −16 | |||
| 6. Attachment to Peers (14–16) | 102.8 | 11.9 | -- | 16* | −32*** | 52*** | ||||
| 7. Attachment to Mother (14–16) | 104.1 | 9.3 | -- | −27*** | 69*** | |||||
| 8. Social Avoidance (19–21) | 6.63 | 2.41 | -- | −39*** | ||||||
| 9. Attachment to Mother (18–20) | 102.5 | 16.4 | -- |
Note: Correlations are multiplied by 100. Age of assessment is in parentheses.
Primary Analyses
Prediction of Early Adult Loneliness
Direct prediction
Simple correlational analysis, as presented in Table 1, indicated a quite strong (r = .52, p < .001) relationship between depressive symtpoms at ages 14–16 and early adult loneliness at ages 23–24.
Predictions after excluding the most depressed adolescents
Analyses then examined whether this relationship was primarily driven by adolescents experiencing high levels of depressive symptoms. Kovacs (1992) recommends that a score of 19 on the Childhood Depression Inventory be used as a screening cutoff suggesting need for further inquiry for individuals who may potentially be experiencing clinically diagnosable major depression. To eliminate the possibility that individuals above this cutoff were driving findings, we examined a reduced data set in which adolescents who reached this screening cutoff at any of our assessment points at ages 14, 15, or 16 (N = 19) were temporarily removed from analyses. In this reduced data set, the correlation between adolescent depressive symptoms and later loneliness remained, with the correlation only modestly reduced (r = .41, p < .001). This indicates that the relation of depressive symptoms to future loneliness existed and was moderately strong even among those indivduals who were clearly not observed experiencing extremely high levels of those symptoms in early adolescence.
Predictions over and above baseline functioning and current depressive symptoms
Analyses with the full sample were next used to examine whether predictions would obtain after accounting for both baseline levels of social functioning in adolescence and concurrent levels of depressive symptoms in early adulthood. Although concurrent levels of depressive symptoms and baseline adolescent functioning with peers were strongly related to adult reported loneliness in simple correlational analyses reported in Table 1, prior levels of symptoms in adolescence continued to predict loneliness over and above concurrent depressive symptoms and adolescent attachment to peers, and accounted for an additional 9% of the variance in loneliness even after accounting for these other factors (see Table 2). This indicates that the relation of adolescent depressive symptoms to adult loneliness existed over and above both baseline social functioning and also was to a significant degree present even over and above concurrent adult levels of depressive symptoms.
Table 2.
Predicting Young Adult Loneliness (Age 23–24)
| Loneliness (Age 23–24) | |||
|---|---|---|---|
| β | ΔR2 | Total R2 | |
| Step I. | |||
| Gender (1-M; 2=F) | −.08 | ||
| Total Family Income (13) | .06 | ||
| Statistics for Step | .00 | .00 | |
| Step II. | |||
| Attachment to Peers (14–16) | −.11+ | .070 | .070 |
| Step III. | |||
| Depression (23–24) | .43*** | .280*** | .350*** |
| Step IV. | |||
| Depression (14–16) | .34*** | .091*** | .441*** |
Note.
p < .001.
p < .01.
p < .05.
β’s are from final model.
Mediated Pathways
The extent to which predictions to future loneliness were mediated by a tendency toward avoidance of social interactions was examined in a path model that assessed the indirect effect of depressive symptoms on future loneliness via social avoidance in mid- to late-adolescence. This model (which was also used to simultaneously examine the relation of symptoms to maternal relationship quality, as described further below) is presented in Figure 1.
Figure 1.
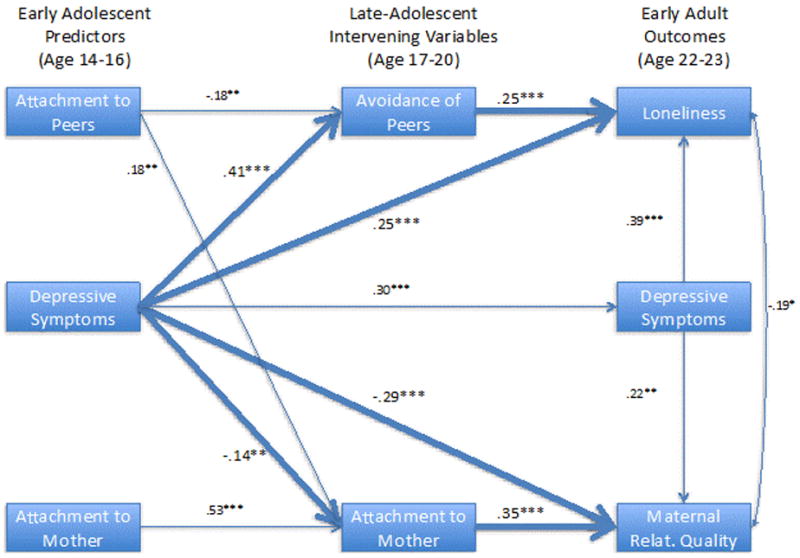
Mediated relationship between early adolescent depressive symptoms and adult social functioning
Results indicate that adolescent depressive symptoms have both an indirect effect on future loneliness as mediated via late adolescent social avoidance (βindirect effect = .10, p < .01) as well as a remaining direct effect as depicted in the model. The overall path model fit the data well, (CFI =.99, chisq (11) = 17.5, p > .05; RMSEA = .057).
Predictions of Maternal Relationship Quality
Direct prediction
Simple correlational analysis, as presented in Table 1, indicated a substantial (r = −.30, p < .001) relationship between depressive symtpoms at ages 14–16 and lower maternal relationship quality, as reported by mothers, in early adulthood.
Predictions excluding most depressed adolescents
Analyses next examined whether this relationship was primarily driven by adolescents experiencing high levels of depressive symptoms. Examining only adolescents who never had scores above 19 on the CDI, as described above, the correlation between adolescent depressive symptoms and poorer early adult maternal relationship quality remained, with the correlation actually slightly greater for this subsample (r = −.31, p < .001). This indicates that the relation of depressive symptoms to future maternal relationship quality was robust even among those indivduals who were clearly not observed experiencing extremely high levels of those symptoms in early adolescence.
Predictions over and above baseline functioning and current depressive symptoms
Analyses with the full sample were next used to examine whether predictions would obtain after accounting for both baseline levels of social functioning in adolescence and effects of concurrent levels of depressive symptoms in early adulthood. Although concurrent levels of depressive symptoms were strongly related to lower maternal relationship quality, prior levels of symptoms in adolescence continued to predict relationship quality over and above concurrent depressive symptoms and early adolescent maternal relationship quality, and accounted for an additional 11% of the variance in maternal relationship quality even after accounting for these factors as shown in Table 3. This indicates that the relation of adolescent depressive symptoms to poorer maternal relationship quality was not simply a reflection of baseline relationship quality and also was to a significant degree present even over and above concurrent adult levels of depressive symptoms.
Table 3.
Predicting Young Adult Maternal Relationship Quality (Age 23)
| Maternal Relationship Quality (Age 23) | |||
|---|---|---|---|
| β | ΔR2 | Total R2 | |
| Step I. | |||
| Gender (1-M; 2=F) | .22** | ||
| Total Family Income (13) | −.18* | ||
| Statistics for Step | .061 | .061 | |
| Step II. | |||
| Attachment to Mother (14– 16) | −.03 | .035 | .096 |
| Step III. | |||
| Depression (23–24) | .18* | .005 | .101 |
| Step IV. | |||
| Depression (14–16) | −.39*** | .110*** | .211** |
Note.
p < .001.
p < .01.
p < .05.
β’s are from final model.
Mediated Pathways
Lastly, the extent to which predictions to future loneliness were mediated by maternal relationship quality in mid- to late-adoelscence was examined in a path model that assessed the indirect effect of depressive symptoms on future loneliness via intervening maternal relationship quality. This model, as described in further detail above, is presented in Figure 1.
Results indicate that adolescent depressive symptoms have both a modest indirect effect on early adult maternal relationship quality as mediated via late adolescent maternal relationship quality (βindirect effect = −.05, p ≤ .05) as well as a remaining direct effect as depicted in the model.
Prediction to Romantic Relationship Behavior
Direct prediction
Simple correlational analysis, as presented in Table 1, indicated a moderate (r = .23 p = .03) relationship between depressive symtpoms at ages 14–16 and greater observed negativity in romantic relationships at age 23.
Predictions excluding most depressed adolescents
Analyses next examined whether this relationship was primarily driven by adolescents experiencing high levels of depressive symptoms. Examining only adolescents who never had scores above 19 on the CDI, as described above, the correlation between adolescent depressive symptoms and later loneliness remained, with the correlation somewhat greater for this sample (r = .33, p = .003). This indicates that the relation of depressive symptoms to future romantic relationship behavior was robust even among those indivduals who were clearly not observed experiencing extremely high levels of those symptoms in early adolescence.
Predictions over and above baseline functioning and current depressive symptoms
No prediction of early adolescent depressive symptoms to negativity in romantic relationships was observed after accounting for early adolescent attachment to peers and concurrent depressive symptoms. Given the lack of predictions of depressive symptoms to romantic relationship behavior in models that included these variables, further analyses of potential mediated pathways in models that also included these variables were not explored.
Post-hoc Categorical Analyses
Post-hoc analyses examined early adolescents who on average displayed levels of depressive symptoms that were above the broadest, most inclusive screening criteria (CDI scores 13 or greater) (Matthey & Petrovski, 2002) designed to capture individuals who might potentially warrant further evaluation (N = 24). When this cutoff was used to predict individuals above vs. below the median score for adult loneliness, results indicated a striking relationship, as shown in Table 4. Every single one of the 24 adolescents who were above even the loosest published screening criteria for depressive symptoms in early adolescence was above the sample median for loneliness by early adulthood (χ2 = 24.25, p < .0001). A similar, though far less striking pattern was seen for predictions of individuals above vs. below the median scores for maternal relationship quality (χ2 = 6.68, p < .01, not depicted). No such effect was observed for romantic relationship negativity.
Table 4.
Categorical Analysis of Early Depressive Symptoms and Young Adult Loneliness
| Loneliness (Age 23–24) | ||||
|---|---|---|---|---|
| Below Median | Above Median | |||
| Average Depression Score (Age 14–16) | CDI > 13 | N | 80 | 68 |
| Row % | 54% | 46% | ||
| CDI > 13 | N | 0 | 24 | |
| Row % | 0% | 100% | ||
χ2 = 24.25, p < .0001.
Discussion
The results of this study show that even depressive symptoms in early adolescence that do not exceed clinical screening cutoffs can predict a surprisingly large risk for substantial social difficulty nearly a decade later in early adulthood. Future social difficulties appeared across a variety of domains, including overall levels of loneliness and deficits in specific family and romantic relationships. Difficulties were observed from a variety of perspectives from self-report to maternal report to direct observation. Two key predictions—from early adolescent depressive symptoms to overall adult loneliness and low maternal relationship quality—were observed even after accounting for both concurrent depressive symptoms in adulthood and prior levels of functioning in early adolescence. Although lay conceptions of adolescence as being associated with ‘moodiness’ might lead to a tendency to minimize the importance of milder depressive symptoms during this period, these findings suggest that such symptoms warrant serious attention as potential markers of substantial future social difficulties.
Although even longitudinal data cannot establish the presence of causal pathways, these findings are consistent with a role for depressive symptoms in early adolescence as interfering with processes of social development at a critical point in such development to create long-term risks of dysfunction. Consistent with this perspective, predictive effects of depressive symptoms appeared partially mediated by intervening qualities of social functioning in late adolescence. In terms of predictions of adult loneliness, links from adolescent depressive symptoms appeared partially mediated by a tendency toward avoidance of social interactions in late adolescence. Predictions to lower quality adult-maternal relationships were partially mediated via quality of these relationships in late adolescence. Predictions to qualities of romantic relationships, though somewhat less robust, were also clearly present in both simple correlational analyses and in analyses examining only early adolescents who had never crossed screening thresholds for high levels of depressive symptoms. Together, these findings are consistent with the perspective that early adolescent depressive symptoms may alter social-developmental trajectories in ways that forecast longer-term problems in social functioning.
The types of difficulties predicted by early adolescent depressive symptoms were not trivial. Loneliness and social isolation in adulthood have been related to outcomes ranging from higher cholesterol and adverse changes in blood pressure management to early morbidity and mortality (Hawkley, et al., 2006; House, et al., 1988; O’Reilly, et al., 1989). In addition, it is noteworthy that in adulthood social difficulties are likely to contribute to future depressive symptoms and may in fact be an important factor underlying the observed chronicity of depressive symptoms (Fergusson, 2007; Joiner, 2000; Pine, et al., 1999). Although depressive symptoms no doubt have their own endogenous sources of stability, the present results suggest that stability may also be maintained in part via a cumulative continuity process (Caspi, Bem, & Elder, 1989) in which early depressive symptoms impair future social relationship qualities which in turn increase the likelihood of future depressive symptoms. In adulthood, major depression is substantially (25–30%) comorbid w/social phobia and avoidant personality disorder (Alpert, Uebelacker, McLean et al., 1997) and the finding that depressive symptoms predict long-term social impairment may partly help to explain this comorbidity.
Notably, this study found predictions even when the sample excluded adolescents displaying higher levels (i.e., above a standard clinical screening cutoff) of depressive symptoms at any one of the three assessment points from ages 14 to 16. This is consistent with the notion that depressive symptoms in adolescence are best viewed on a continuum, with even individuals well below clinical diagnostic thresholds vulnerable to long-term impairment in addition to short-term distress (Gotlib, et al., 1995; Lewinsohn, Solomon, Seeley et al., 2000).
Nor can these findings be explained as simply reflecting the ongoing effects of a stable depressive pattern from adolescence to adulthood. Not only does the observed instability of adolescent depressive symptoms across this period mitigate against this explanation (Lewinsohn, Petit, Joiner et al., 2003), but predictions to future loneliness and poor maternal relationships were robust even after accounting for concurrent levels of depressive symptoms in adulthood. In terms of simple direct correlations, adolescent depressive symptoms actually displayed substantial heterotypic continuity, serving as stronger predictors of social functioning than of future depressive symptoms.
A developmental psychopathology perspective offers perhaps the most satisfying explanation of these findings (Cicchetti & Toth, 1998). From this perspective, depressive symptoms may have specific, deleterious effects on critical ongoing social processes—the efforts to establish adult-like social relationships with peers and family—that comprise a key developmental task of adolescence. By interfering with this task at a sensitive point in development, even symptoms that will themselves display only modest stability going forward may profoundly alter the adolescent’s developmental trajectory—by interfering with a related developmental process—in ways that predict long-term social impairment. The magnitude of some of the reported findings bears out the potential strength of these effects. For example, when adolescents who met only the loosest screening criteria for possible depression were followed into adulthood, 100% (24 out of 24) were found to be above the sample median in adult loneliness. This suggests a remarkably powerful correspondence between early adolescent depressive symptoms and future social difficulties.
These findings clearly suggest the importance of early detection and treatment of even milder depressive symptoms in adolescence. By 2020, after ischemic heart disease, depression is predicted to be the second largest cause of disability worldwide (Murray & Lopez, 1996), but these cost analyses do not even include many of the secondary social effects of early depression identified in this study. The findings of this study clearly suggest that even so-called ‘minor’ levels of depressive symptoms are anything but minor. These findings also suggest the potential importance of interpersonal therapies for adolescent depression (Mufson, Weissman, Moreau et al., 1999). Addressing the social sequelae of adolescent depressive symptoms within these therapies may in fact be as important as addressing the symptoms of themselves in terms of enhancing long-term outcomes.
Notably there were no gender differences observed in these data. Whereas major depressive disorder gradually evinces a clear gender difference in prevalence primarily beginning in mid- to late-adolescence (Hankin, Abramson, Moffitt et al., 1998), gender effects on symptom level reports are typically far more modest. Even by age 16, females are typically only about 10% above males (e.g., 1 scale point on the CDI) in reported symptom levels (Twenge & Nolen-Hoeksema, 2002). This study found that the pattern of long-term social impairment predicted by adolescent depressive symptoms did not differ significantly for males vs. females.
Several limitations to these findings warrant note. As already mentioned, although this study can address causal hypotheses, its design only allows it to potentially disconfirm, but not to directly support such hypotheses. In addition, diagnostic interviews were not conducted with this sample. Although, as a community sample, we would expect the incidence of confirmed major depressive disorder to be quite modest, this cannot be definitively ascertained. In any case, future research would be needed to make generalizations to more severely impaired samples. Findings regarded reported loneliness may be somewhat inflated given the common method variance from use of self-reports to assess both adolescent symptoms and adult loneliness. Although, by covarying adult reports of depressive symptoms, much of this methods confound is likely removed from results, and in any case, quite similar findings were obtained for other-report and observational assessments of adult social functioning where no methods confounds are present. Finally, our understanding of the mediators of these long-term predictions from depressive symptoms is still at a quite rudimentary phase. Further research examining micro-processes that occur within early- to mid-adolescence for depressed individuals is needed to flesh out precisely how long-term links to social difficulties are established and maintained.
Acknowledgments
This study and its write-up were supported by grants from the National Institute of Child Health and Human Development and the National Institute of Mental Health (9R01HD058305-11A1 & R01-MH58066).
References
- Allen JP, Hauser ST, Bell KL, O’Connor TG. Longitudinal assessment of autonomy and relatedness in adolescent-family interactions as predictors of adolescent ego development and self-esteem. Child Development. 1994;65(1):179–194. doi: 10.1111/j.1467-8624.1994.tb00743.x. [DOI] [PubMed] [Google Scholar]
- Allen JP, McElhaney KB, Kuperminc GP, Jodl KM. Stability and change in attachment security across adolescence. Child Development. 2004;75:1792–1805. doi: 10.1111/j.1467-8624.2004.00817.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allen JP, Porter MR, McFarland CF. The Autonomy and Relatedness Coding System for Peer Interactions. University of Virginia; Charlottesville, Virginia: 2001. [Google Scholar]
- Allen JP, Porter MR, McFarland FC, McElhaney KB, Marsh PA. The relation of attachment security to adolescents’ paternal and peer relationships, depression, and externalizing behavior. Child Development. 2007;78:1222–1239. doi: 10.1111/j.1467-8624.2007.01062.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alpert JE, Uebelacker LA, McLean NE, Nierenberg AA. Social phobia, avoidant personality disorder and atypical depression: Co-occurrence and clinical implications. Psychological Medicine. 1997;27(3):627–633. doi: 10.1017/s0033291797004765. [DOI] [PubMed] [Google Scholar]
- Aquilino WS. Family Relationships and Support Systems in Emerging Adulthood. In: Arnett JJ, Tanner JL, editors. Emerging adults in America: Coming of age in the 21st century. Washington, DC, US: American Psychological Association; 2006. pp. 193–217. [Google Scholar]
- Armsden GC, Greenberg MT. The Inventory of Parent and Peer Attachment: Individual differences and their relationship to psychological well-being in adolescence. Journal of Youth & Adolescence. 1987;16(5):427–454. doi: 10.1007/BF02202939. [DOI] [PubMed] [Google Scholar]
- Blakemore SJ, Choudhury S. Development of the adolescent brain: implications for executive function and social cognition. [Research Support, Non-U.S. Gov’t Review] Journal of child psychology and psychiatry, and allied disciplines. 2006;47(3–4):296–312. doi: 10.1111/j.1469-7610.2006.01611.x. [DOI] [PubMed] [Google Scholar]
- Bowlby J. Attachment and loss. Vol. 1. New York: Basic Books; 1969/1982. [Google Scholar]
- Cacioppo JT, Ernst JM, Burleson MH, McClintock MK, Malarkey WB, Hawkley LC, Hugdahl K. Lonely traits and concomitant physiological processes: The MacArthur social neuroscience studies. International Journal of Psychophysiology. 2000;35(2–3):143–154. doi: 10.1016/s0167-8760(99)00049-5. [DOI] [PubMed] [Google Scholar]
- Caspi A, Bem DJ, Elder GH. Continuities and consequences of interactional styles across the life course. Journal of Personality. 1989;57(2):375–406. doi: 10.1111/j.1467-6494.1989.tb00487.x. [DOI] [PubMed] [Google Scholar]
- Cicchetti D, Toth SL. The development of depression in children and adolescents. American Psychologist. 1998;53(2):221–241. doi: 10.1037//0003-066x.53.2.221. [DOI] [PubMed] [Google Scholar]
- Cicchetti DV, Sparrow SA. Developing criteria for establishing interrater reliability of specific items: Applications to assessment of adaptive behavior. American Journal of Mental Deficiency. 1981;86:127–137. [PubMed] [Google Scholar]
- Collins WA, Laursen B. Changing Relationships, Changing Youth: Interpersonal Contexts of Adolescent Development. Journal of Early Adolescence. 2004;24(1):55–62. [Google Scholar]
- Connolly J, Geller S, Marton P, Kutcher S. Peer responses to social interaction with depressed adolescents. Journal of Clinical Child Psychology. 1992 Dec;21(4):365–370. 1992. [Google Scholar]
- Coyne JC. Toward an interactional description of depression. Psychiatry: Journal for the Study of Interpersonal Processes. 1976;39(1):28–40. doi: 10.1080/00332747.1976.11023874. [DOI] [PubMed] [Google Scholar]
- Daley SE, Hammen C. Depressive symptoms and close relationships during the transition to adulthood: Perspectives from dysphoric women, their best friends, and their romantic partners. Journal of Consulting & Clinical Psychology. 2002;70(1):129–141. doi: 10.1037//0022-006x.70.1.129. [DOI] [PubMed] [Google Scholar]
- Fergusson DMB, Joseph M, Horwood L John. Recurrence of major depression in adolescence and early adulthood, and later mental health, educational and economic outcomes. British Journal of Psychiatry. 2007 doi: 10.1192/bjp.bp.107.036079. [DOI] [PubMed] [Google Scholar]
- Furman W. The measurement of friendship perceptions: Conceptual and methodological issues. In: Bukowski WM, Newcomb AF, editors. The company they keep: Friendship in childhood and adolescence. Cambridge studies in social and emotional development. New York, NY, USA: Cambridge University Press; 1998. pp. 41–65. [Google Scholar]
- Furman W, Buhrmester D. Childrens’ perceptions of the personal relationships in their social networks. Developmental Psychology. 1985;21:1016–1024. [Google Scholar]
- Goswick RA, Jones WH. Components of loneliness during adolescence. Journal of Youth and Adolescence. 1982;11(5):373. doi: 10.1007/BF01540375. [DOI] [PubMed] [Google Scholar]
- Gotlib IH, Lewinsohn PM, Seeley JR. Symptoms versus a diagnosis of depression: Differences in psychosocial functioning. Journal of Consulting and Clinical Psychology. 1995;63(1):90. doi: 10.1037//0022-006x.63.1.90. [DOI] [PubMed] [Google Scholar]
- Gotlib IH, Lewinsohn PM, Seeley JR. Consequences of depression during adolescence: Marital status and marital functioning in early adulthood. Journal of Abnormal Psychology. 1998;107(4):686–690. doi: 10.1037//0021-843x.107.4.686. [DOI] [PubMed] [Google Scholar]
- Hammen C. Interpersonal factors in an emerging developmental model of depression. In: Johnson SL, Hayes AM, Field TM, Schneiderman N, McCabe PM, editors. Stress, coping and depression. Mahwah, NJ: Lawrence Erlbaum Associates; 2000. pp. 71–88. [Google Scholar]
- Hankin BL, Abramson LY, Moffitt TE, Silva PA, McGee R, Angell KE. Development of depression from preadolescence to young adulthood: Emerging gender differences in a 10-year longitudinal study. Journal of Abnormal Psychology. 1998;107(1):128–140. doi: 10.1037//0021-843X.107.1.128. [DOI] [PubMed] [Google Scholar]
- Hawkley LC, Burleson MH, Berntson GG, Cacioppo JT. Loneliness in everyday life: Cardiovascular activity, psychosocial context, and health behaviors. Journal of Personality and Social Psychology. 2003;85(1):105. doi: 10.1037/0022-3514.85.1.105. [DOI] [PubMed] [Google Scholar]
- Hawkley LC, Masi CM, Berry JD, Cacioppo JT. Loneliness is a unique predictor of age-related differences in systolic blood pressure. Psychology and Aging. 2006;21(1):152. doi: 10.1037/0882-7974.21.1.152. [DOI] [PubMed] [Google Scholar]
- House JS, Landis KR, Umberson D. Social relationships and health. Science. 1988;241(4865):540–545. doi: 10.1126/science.3399889. [DOI] [PubMed] [Google Scholar]
- Joiner TE. Depression in its interpersonal context. In: Gotlib IH, Hammen CL, editors. Handbook of depression. New York, NY: Guilford Press; 2002. pp. 295–313. [Google Scholar]
- Joiner TE., Jr Depression’s vicious scree: Self-propagating and erosive processes in depression chronicity. Clinical Psychology: Science & Practice. 2000;7(2):203–218. [Google Scholar]
- Kasen S, Cohen P, Skodol AE, Johnson JG, Smailes E, Brook JS. Childhood Depression and Adult Personality Disorder: Alternative Pathways of Continuity. Arch Gen Psychiatry. 2001;58(3):231–236. doi: 10.1001/archpsyc.58.3.231. [DOI] [PubMed] [Google Scholar]
- Kazdin AE. Childhood depression. Journal of Child Psychology & Psychiatry & Allied Disciplines. 1990;31(1):121–160. doi: 10.1111/j.1469-7610.1990.tb02276.x. [DOI] [PubMed] [Google Scholar]
- Kobak RR, Sceery A. Attachment in late adolescence: Working models, affect regulation and representations of self and others. Child Development. 1988;59:135–146. doi: 10.1111/j.1467-8624.1988.tb03201.x. [DOI] [PubMed] [Google Scholar]
- Kovacs M. Children’s Depression Inventory Manual. New York: Multi-Health Systems; 1992. [Google Scholar]
- Kovacs M, Beck AT. An empirical clinical approach toward a definition of childhood depression. New York: Raven Press; 1977. [Google Scholar]
- La Greca AM, Lopez N. Social anxiety among adolescents: Linkages with peer relations and friendships. Journal of Abnormal Child Psychology. 1998;26(2):83–94. doi: 10.1023/a:1022684520514. [DOI] [PubMed] [Google Scholar]
- Lerner RM, Lerner JV, von Eye A, Ostrom CW, Nitz K, Talwar-Soni R, Tubman J. Continuity and discontinuity across the transition of early adolescence: A developmental contextual perspective. Transitions through adolescence: Interpersonal domains and context. 1996:3–22. [Google Scholar]
- Lewinsohn PM, Petit JW, Joiner TE, Jr, Seeley JR. The symptomatic expression of major depressive disorder in adolescents and young adults. Journal of Abnormal Psychology. 2003;112(2):244–252. doi: 10.1037/0021-843x.112.2.244. [DOI] [PubMed] [Google Scholar]
- Lewinsohn PM, Rohde P, Seeley JR, Klein DN, Gotlib IH. Natural course of adolescent major depressive disorder in a community sample: Predictors of recurrence in young adults. American Journal of Psychiatry. 2000;157(10):1584–1591. doi: 10.1176/appi.ajp.157.10.1584. [DOI] [PubMed] [Google Scholar]
- Lewinsohn PM, Solomon A, Seeley JR, Zeiss A. Clinical implications of “subthreshold” depressive symptoms. Journal of Abnormal Psychology. 2000;109(2):345–351. [PubMed] [Google Scholar]
- Matthey S, Petrovski P. The Children’s Depression Inventory: Error in cutoff scores for screening purposes. Psychological Assessment. 2002;14(2):146–149. doi: 10.1037//1040-3590.14.2.146. [DOI] [PubMed] [Google Scholar]
- Moore D, Schultz NR. Loneliness at adolescence: Correlates, attributions, and coping. Journal of Youth and Adolescence. 1983;12(2):95. doi: 10.1007/BF02088307. [DOI] [PubMed] [Google Scholar]
- Mufson L, Weissman MM, Moreau D, Garfinkel R. Efficacy of interpersonal psychotherapy for depressed adolescents. Archives of General Psychiatry. 1999;56(6):573–579. doi: 10.1001/archpsyc.56.6.573. [DOI] [PubMed] [Google Scholar]
- Murray CJ, Lopez AD. Evidence-based health policy--lessons from the Global Burden of Disease Study. Science. 1996;274(5288):740–743. doi: 10.1126/science.274.5288.740. [DOI] [PubMed] [Google Scholar]
- O’Reilly P, Emerson Thomas H. Role of support networks in maintenance of improved cardiovascular health status. Social Science & Medicine. 1989;28(3):249–260. doi: 10.1016/0277-9536(89)90268-2. [DOI] [PubMed] [Google Scholar]
- Pennix BW, van Tilburg T, Kriegsman DM, Deeg DJ, Boeke AJ, van Eijk JT. Effects of social support and personal coping resources on mortality in older age: the Longitudinal Aging Study Amsterdam. Am Journal of Epidemiology. 1997;146:510–519. doi: 10.1093/oxfordjournals.aje.a009305. [DOI] [PubMed] [Google Scholar]
- Pine DS, Cohen E, Cohen P, Brook J. Adolescent depressive symptoms as predictors of adult depression: Moodiness or mood disorder? The American Journal of Psychiatry. 1999 doi: 10.1176/ajp.156.1.133. [DOI] [PubMed] [Google Scholar]
- Powers SI, Hauser ST, Kilner LA. Adolescent mental health. American Psychologist. 1989;44(2):200. doi: 10.1037//0003-066x.44.2.200. [DOI] [PubMed] [Google Scholar]
- Pressman SD, Cohen S, Miller GE, Barkin A, Rabin BS, Treanor JJ. Loneliness, social network size, and immune response to influenza vaccination in college freshmen. Health Psychology. 2005;24(3):297–306. doi: 10.1037/0278-6133.24.3.297. [DOI] [PubMed] [Google Scholar]
- Rohde P, Lewinsohn PM, Seeley JR. Are adolescents changed by an episode of major depression? Journal of the American Academy of Child & Adolescent Psychiatry. 1994;33(9):1289–1298. doi: 10.1097/00004583-199411000-00010. [DOI] [PubMed] [Google Scholar]
- Roisman GI, Masten AS, Coatsworth JD, Tellegen A. Salient and emerging developmental tasks in the transition to adulthood. Child Development. 2004;75(1):123–133. doi: 10.1111/j.1467-8624.2004.00658.x. [DOI] [PubMed] [Google Scholar]
- Russell D, Peplau LA, Cutrona CE. The revised UCLA Loneliness Scale: Concurrent and discriminant validity evidence. J Pers Soc Psychol. 1980;39(3):472–480. doi: 10.1037//0022-3514.39.3.472. [DOI] [PubMed] [Google Scholar]
- Seeman TE. Health promoting effects of friends and family on health outcomes in older adults. American Journal of Health Promotion. 2000 doi: 10.4278/0890-1171-14.6.362. [DOI] [PubMed] [Google Scholar]
- Stice E, Ragan J, Randall P. Prospective Relations Between Social Support and Depression: Differential Direction of Effects for Parent and Peer Support? Journal of Abnormal Psychology. 2004;113(1):155–159. doi: 10.1037/0021-843X.113.1.155. [DOI] [PubMed] [Google Scholar]
- Strodtbeck F. Husband-wife interaction over revealed differences. American Sociology Review. 1951;16:463–473. [Google Scholar]
- Sugisawa H, Liang J, Liu X. Social networks, social support, and mortality among older people in Japan. Journal of Gerontology. 1994;49(1):S3–S13. doi: 10.1093/geronj/49.1.s3. [DOI] [PubMed] [Google Scholar]
- Twenge JM, Nolen-Hoeksema S. Age, gender, race, socioeconomic status, and birth cohort difference on the children’s depression inventory: A meta-analysis. Journal of Abnormal Psychology. 2002;111(4):578–588. doi: 10.1037//0021-843x.111.4.578. [DOI] [PubMed] [Google Scholar]