

Abstract
Background:
Ratio of second and fourth digit (2D:4D) is known to be germane in analyzing utero concentrations of testosterone and estrogen in human and other vertebrates. 2D:4D had been linked to several traits like athletes’ abilities, reproductive success, risk of cancer and cardiovascular disease (CVD). Metabolic syndrome (MetS) is a clustering of several cardiovascular risk factors. Waist circumference (WC), neck circumference (NC), body mass index (BMI) and waist-to-height ratio (WHtR) are important in measuring MetS. This study investigated sexual dimorphism in 2D:4D and its relationship with MetS indices and CVD factors among adult residing in Ilorin, North central Nigeria.
Materials and Methods:
This is a cross-sectional, stratified multi-staged sampling study. Participants residing in different neighborhoods were visited at home where finger lengths and anthropometric traits were measured. Participants include 801 healthy adults aged 18-44 years (56% male) who had been living in the area for more than 3 years.
Results:
Males showed significantly lower 2D:4D than females (unpaired t-test; t [699] = 11.49, P = 0.001). A significant positive correlation was observed in MetS markers and 2D:4D. WHtR showed the highest correlation with 2D:4D in male (r = 0.461, P ≤ 0.001) and female (r = 0.408, P ≤ 0.001) when compared with BMI, NC and WC. All positive correlations recorded in this study were high in male and right hand.
Conclusion:
Our results showed that 2D:4D is sexual dimorphic and right hand 2D:4D as a predictor of MetS is better. We concluded that 2D:4D is a proxy for MetS and CVD risk factors in Ilorin.
Keywords: Cardiovascular disease, digit ratio, metabolic syndrome, sexual dimorphism
INTRODUCTION
The ratio of second and fourth digit lengths (2D:4D), has been highlighted as a potentially useful phenotypic marker of steroid exposure in utero of vertebrates.[1] It is generally postulated that the lower the individual 2D:4D, the higher testosterone but the lower estrogen levels experienced during fetal life. In humans, the evidence for this hypothesis comes from studies showing that 2D:4D is sexually dimorphic with lower ratios among males than females from the end of the first trimester of fetal development and remain relatively stable across the life span.[2,3,4,5,6,7] Congenital adrenal hyperplasia, which leads to excessive prenatal androgen production, has been shown to be related to low 2D:4D in both sexes.[8] Similarly, women with polycystic ovarian syndrome that presumably relates to increased prenatal testosterone (PT) level have lower than normal 2D:4D.[9] In addition, women from the opposite-sex twin pairs have also been reported to show masculinized 2D:4D.[10] Recent studies showed that 2D:4D is determined not by PT alone but by the balance of PT to prenatal estrogen signaling in a restricted time window of fetal digit development.[11,12]
A study by Gobrogge et al.[13] reported substantial additive genetic and non-shared environmental influences on digit ratios. Moreover, a recent study by Medland et al.[14] showed that a variant situated in the intron 2 of LIN28B gene (rs314277) was associated with 2D:4D. Variation in 2D:4D has been suggested to have evolutionary relevance because of its associations with fitness components. Evidence for an association between 2D:4D and reproductive success[15] and breast cancer risk and age at the onset of breast cancer[16] had been shown. Also, 2D:4D had been implicated in risk of cardiovascular disease (CVD),[17,18,19] because it had been suggested that prenatal androgen exposure might enhance the development of the cardiovascular system.[20,21] It is thus imperative to test the relationship between 2D:4D and CVD.
Metabolic syndrome (MetS), which connotes the clustering of known CVD risk factors including obesity, dyslipidemia, hyperglycemia and systemic hypertension, is a major public health challenge world-wide.[22] Obesity is now a pandemic condition, affecting approximately half a billion people world-wide.[23] A recent study by Adediran et al.[24] reported that MetS is a major health condition among rural and urban dwellers in Nigeria, prevalence of MetS is high among newly diagnosed hypertensive patients in Nnewi South East Nigeria[25] and a study by Wahab et al.[26] also reported a high prevalence of obesity in Northern Nigeria. Thus, MetS is also becoming a cause for a public health concern in Nigeria.
An easy and affordable means of diagnosing this health challenge is thus imperative. A recent robust and extensive review that cut across several ethnic groups by Ashwell et al.[27] suggested that waist-to-height ratio (WHtR), waist circumference (WC) and body mass index (BMI) are germane in detecting cardiometabolic risk factor in both sexes, but WHtR was considered as the best predictor, although Onat et al.[28] reported that neck circumference (NC) contributes to MetS likelihood beyond WC. Studies by Fink et al.,[18,19] Abba et al.[29] have shown the relationship between 2D:4D and other predictors of MetS (NC, WC and BMI).
Thus, the goal of this study is to assess the relationship between sexually dimorphic traits established early in life (finger length) and putative marker for MetS amongst people living in Ilorin North Central Nigeria.
MATERIALS AND METHODS
Subjects
A stratified multi-staged sampling method was used to select participants for the study. A total of eight neighborhoods composed of four high density and the rest were low density areas were selected by simple random sampling. This cross-sectional study was conducted between February and July, 2012 in Ilorin among 801 adults comprising of 450 males and 351 females (age 18 and above). Sample size was determined for each neighborhood according to Cohen.[30] Data on socio-demographic characteristics and digits lengths were collected and recorded into structured questionnaire.
Finger length measurements
Digit length was measured as described by Manning et al.[2] Briefly, participants were asked to keep their hands supine on the table surface with the palm facing up and the digits straight in the same plane and fingers opened in a posture of ease (not kept together tight under artificial pressure). Care was taken to ensure that details of major creases could be seen on the hands by removing finger ornaments. Length of each digit was measured on the ventral aspect of hand from the proximal crease to the tip of the finger. In cases where there were two creases at the base of the ring finger, the most proximal crease was chosen for the measurement. The length on both left and right hands was measured using an FH electronic digital caliper (Model FH-150, China) measuring to 0.01 mm with the pointers on the caliper just touching the middle point of proximal crease and tip of the finger. All the measurements of digit length were made twice with digits completely protracted. The average of the two measurements was taken. The digit ratio (2D:4D) was calculated by dividing the length of the second digit by that of the fourth.
Anthropometric measurements
Weight was measured to nearest 0.1 kg using a well-calibrated, mechanical personal bathroom scale (Camry scale, model BR-9011). The subjects were weighed barefoot, wearing minimal clothing (T-shirt and trousers or blouse and skirt and underwear), with feet together in the center of the weighing scales and the head looking forward. The scales were checked before each measurement for zero adjustment and standardized.
Height was measured to the nearest 0.1 cm using a portable stadiometer (Seca 213), which consisted of an anthropometer with a simple headboard. During height taking subjects were made to stand upright without shoes and head held erect such that the external auditory metus and the lower border of the eye were in one horizontal plane (Frankfurt plane). Back of the subjects were positioned against the instrument and heels touching the floor plate of the stadiometer with knees and legs together and arms hanging naturally by the side. A movable headboard was brought against the crown of the head and the height measurement read off at maximum inspiration. BMI was calculated as weight (kg) divided by height (m) squared.
WC was measured midway between the lowest rib and the iliac crest after exhaling with the person standing without suppressing the skin using an inextensible tape (measured to the nearest 0.1 cm). The measurement of WC was performed one time for each subject. The WHtR was calculated as WC divided by height. NC was measured in the midway of the neck between the mid-cervical spine and mid-anterior neck to 0.5 cm, if palpable, just below the laryngeal prominence.[28]
The study was explained to potential participants and they were informed that the survey was completely voluntary. Their consents were sought before they were allowed to participate in the study. Subjects with injuries or deformities in any of the digits were left out of the study.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation and discrete variables as numbers and percentages. Differences were assessed by two tailed Student t-test and one-tailed Pearson correlation coefficients were used for assessing the relationship between 2D:4D and height, NC, WC, BMI and WHtR and partial correlations were calculated in order to remove confounding effects of body weight. Statistical significance was accepted at P value less than 0.05 (P < 0.05).
All statistical analyses were computed using PASW (Version 18, Chicago, Illinois) and Microsoft Excel (Microsoft Office Professional, 2007) Microsoft Corporation.
RESULTS
Re-measurement reliability of 2D:4D
There was strong significant correlation between 2D:4D calculated from first and second measurement of digit lengths (correlation coefficient: P < 0.0001; right hand r1 = 0.945; left hand r = 0.931). Also, differences in 2D:4D between-individuals were very much greater than the within-individual differences measurement error of 2D:4D (intra class correlation coefficients: right hand F (1,800) = 69.32, P < 0.0001; left hand F (1,800) = 42.98, P < 0.0001). We concluded that our measured 2D:4D reflected real differences between individuals and there was high re-measurement reliability in our data. All the 2D:4D ratios used in the analyses were mean values of the first and second measurements. Means of right and left 2D:4D recorded in this study were significantly correlated (r = 0.710, P < 0.0001).
Basic characteristics of the study subjects
The basic characteristics of the study population, anthropometric traits and MetS parameters stratified by gender, are shown in Table 1. The mean age of the study population was 29.19 and 25.90 years for male and female respectively. The subject's age ranged between 18 and 44 years, men were slightly older on average [Table 1].
Table 1.
Descriptive statistics, means and SDs, for age, MetS and CVD risk factors indices, left and right second and fourth digits and 2D:4D ratios
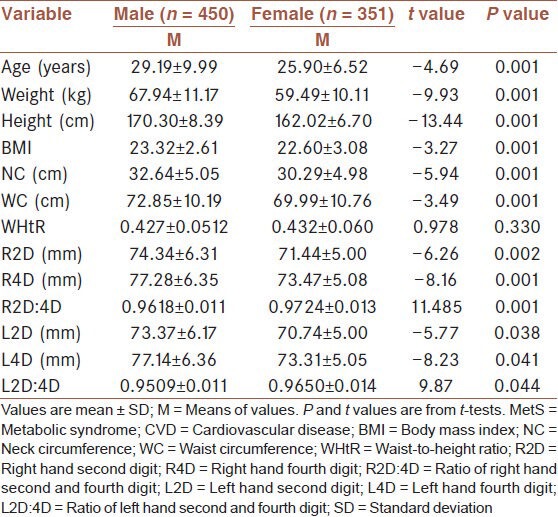
Mean BMI was low, less than 25, in both sexes, but higher in men (23.32) and ratio of digit ratio was higher in women. Considering all the variables studied the results indicated strong sexual dimorphism as shown in Table 1, with statistical significance difference (P < 0.05) in males and females, but there was no sex difference in WHtR (unpaired t-tests; t (699) = 0.978, P = 0.88). Also, there is a statistical difference (P < 0.055) in right and left 2D:4D ratio in male and female. Males showed significantly lower 2D:4D than females in the right hand (unpaired t-test; t (699) = 11.49, P = 0.001) and left hand (unpaired t-test; t (699) = 9.87, P = 0.044), but the significance is high in the right hand [Table 1].
Correlations between 2D:4D, anthropometric traits and MetS risk factors
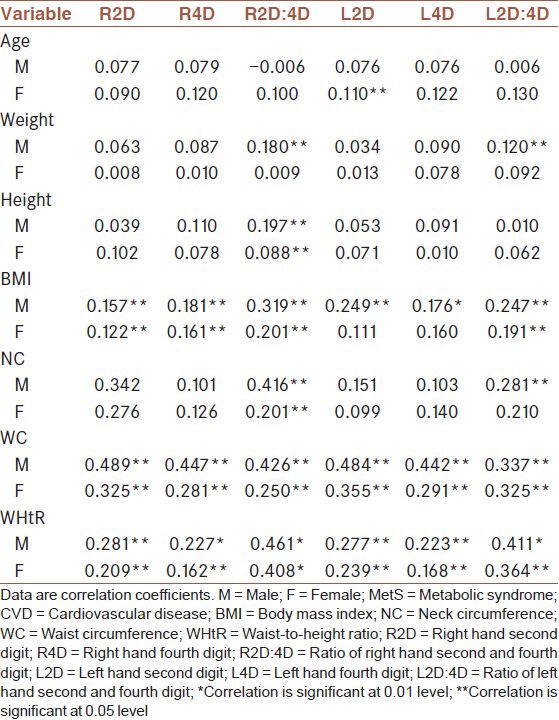
Pearson's correlation coefficients, as measured among the anthropometric indices and MetS surrogate marker tested in this study show a positive correlation with 2D and 4D digit length and ratios (2D:4D) in both males and females subjects [Table 2]. There was no significant correlation between age, weight and height and both right and left 2D, 4D and 2D:4D ratio in female and male [Table 2]. Digit ratio (2D:4D) in both hands failed to show any significant correlations with NC in female subjects, but a significant relationship was recorded in male. Also, MetS markers (BMI, WC and WHtR) were significantly correlate with both right and left 2D, 4D digit and ratios in male and female. WHtR showed the highest significant correlation with right 2D:4D in both male (r = 0.461, P ≤ 0.001) and female (r = 0.408, P ≤ 0.001) when compared with BMI, NC and WC.
Table 2.
The coefficient of correlation in MetS and CVD risk factors indices and age, 2D:4D and lengths of the index and ring fingers for both hands in males and females
Consequently, we controlled for the effect of body weight by calculating partial correlations (rp) between body weight and MetS indices. In male, non-significant positive correlations between both hands 2D:4D and BMI (right hand: rp = 0.13, P = 0.06; left hand: rp = 0.08, P = 0.091) was observed. While there was a significant positive association between other MetS and CVD risks factors (WC, NC and WHtR) and mean 2D:4D ratio, but these correlations were higher in the right hand. Similar results were recorded in female, though the correlations were lower when compared with their male counterparts Table 3.
Table 3.
Partial correlation coefficients between MetS and CVD risk factors indices and 2D:4D in males and females
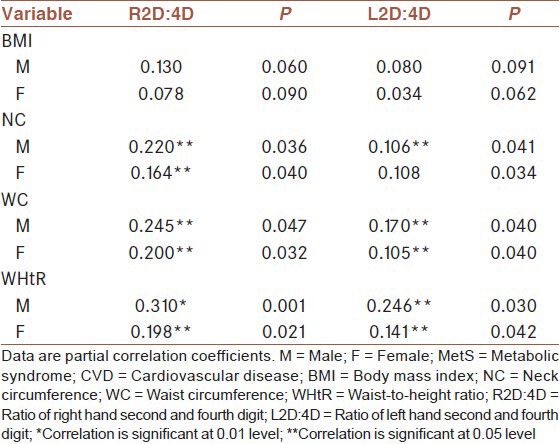
All positive correlations recorded in this study were higher in male and right hand.
DISCUSSION
In this cross-sectional study, a significant positive correlation was observed in MetS markers (BMI, WC, NC and WHtR) and 2D:4D. Individuals residing in different neighborhoods in Ilorin (aged between 18 and 35) were recruited for this study to establish the sexual dimorphism, left and right hand asymmetry in 2D:4D. The result shows that females 2D:4D was statistically higher (P = 0.001) than male 2D:4D. This finding is congruent with previous studies in Nigeria,[31,32,33,34] Uganda[29] and other parts of the world.[7,16] This difference was more pronounced in right digit ratios than left digit ratios. This is in line with the previous study.[7,35] Studies have shown that right hand 2D:4D is dependable than left hand in estimating human phenotypic behaviors and activities, thus the right hand 2D:4D is a better predictor of PT levels.[2,35,36,37] Thus, sex difference in the right hand 2D:4D is more pronounced than that in the left hand. Invariably, right hand show stronger correlation with predicted variables than that in the left hand.[7,38] The insignificant correlation between age and 2D:4D for both sexes observed in this study was similar to the recent report by Zhao et al.[7] and Fink et al.[19] The previous reports have shown that 2D:4D is sexually dimorphic with lower ratios among males than females from the end of the first trimester of fetal development and remain relatively stable across the life span.[2,3,4,5,6,7]
Sexual dimorphism in 2D:4D recorded in this study might be influenced by PT concentration. This hormone has been implicated in its role as modifier of developmental rate like epidermal ridges of the digits.[39] Elevated quantities of fetal testosterone denote a low 2D:4D ratio, which therefore indicates high prenatal testicular activity because development of genitals and digit are influenced by the same directive actions of the homeobox gene complex, in particular HoxA and HoxD.[40] Conversely, 2D:4D is positively associated with estrogen in both sexes. High level of estrogen indicates high digit ratio in both men and women.[2] Our result reported a significant positive relationship between digit lengths (second and fourth) and BMI, WC and WHtR, this is not in-tandem with the earlier study by Abba et al.[29]
The outcome of this study suggests there may be a link between early-life androgen exposure and the risk of MetS that is related with diabetes and heart relation health condition. Perhaps, as well as predicting some anthropometric traits at any stage in life of an individual because 2D:4D has been reported to be determined in-utero and relatively stable throughout the life span.[4,5]
Anthropometric indices such as NC, WC, BMI and WHtR have been shown to be germane in screening for CVD risk factors and MetS.[28,41,42] But studies have shown that WHtR was strongly associated with visceral adipose tissue[43] and recently Ashwell et al.[27] in robust reviews reported that WHtR should be considered as a screening tool for cardiomatabolic risk factor in male and female because it was shown to be better than others (BMI and WC). This was supported by other studies in different parts of the world,[44,45,46] though Guasch-Ferrι et al.[47] reported no significant differences between the predictive abilities of WHtR and WC on metabolic disease. Therefore, WHtR could be the most useful anthropometric variable for predicting MetS and CVD risk factor in a population because it is not dependent on age or sex and it is easy to use.[41]
Earlier researches[18,19,29,31,48,49] have established relationship between 2D:4D and anthropometric traits (height, weight, NC, WC and BMI). But none have shown its relationship with WHtR, thus to the best of our knowledge this is the first study that finds a relationship between 2D:4D and WHtR in any population. Our result presented a significant relationship between 2D:4D and these traits either in right or left hands, which agrees with other reports.[18,19,29,48]
Significant positive correlations in both hands between 2D:4D and BMI, WC, NC and WHtR reported in this study implies that 2D:4D could be a surrogate marker for these important MetS and CVD risk factors, in that they could be used as predictors for MetS and CVD risk factors in Ilorin, North central Nigeria. Lastly, this study results showed that these relationships were stronger in the right hand and male 2D:4D. Thus right hand 2D:4D would be a better predictor of these traits.
CONCLUSION
This study confirmed sexual dimorphism of 2D:4D in Ilorin and showed that it could be a proxy for heart related disease. A routine measure of 2D, 4D and 2D:4D as a simple and practical measure of abdominal obesity will thus be useful in providing information on MetS and CVD risk factors among individuals in Ilorin North central Nigeria.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Berenbaum SA, Bryk KK, Nowak N, Quigley CA, Moffat S. Fingers as a marker of prenatal androgen exposure. Endocrinology. 2009;150:5119–24. doi: 10.1210/en.2009-0774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Manning JT, Scutt D, Wilson J, Lewis-Jones DI. The ratio of 2 nd to 4 th digit length: A predictor of sperm numbers and concentrations of testosterone, luteinizing hormone and oestrogen. Hum Reprod. 1998;13:3000–4. doi: 10.1093/humrep/13.11.3000. [DOI] [PubMed] [Google Scholar]
- 3.Malas MA, Dogan S, Evcil EH, Desdicioglu K. Fetal development of the hand, digits and digit ratio (2D:4D) Early Hum Dev. 2006;82:469–75. doi: 10.1016/j.earlhumdev.2005.12.002. [DOI] [PubMed] [Google Scholar]
- 4.Trivers R, Manning J, Jacobson A. A longitudinal study of digit ratio (2D:4D) and other finger ratios in Jamaican children. Horm Behav. 2006;49:150–6. doi: 10.1016/j.yhbeh.2005.05.023. [DOI] [PubMed] [Google Scholar]
- 5.Galis F, Ten Broek CM, Van Dongen S, Wijnaendts LC. Sexual dimorphism in the prenatal digit ratio (2D:4D) Arch Sex Behav. 2010;39:57–62. doi: 10.1007/s10508-009-9485-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Manning JT. Digit ratio (2D:4D), sex differences, allometry, and finger length of 12-30-year olds: Evidence from the British Broadcasting Corporation (BBC) Internet study. Am J Hum Biol. 2010;22:604–8. doi: 10.1002/ajhb.21051. [DOI] [PubMed] [Google Scholar]
- 7.Zhao D, Li B, Yu K, Zheng L. Digit ratio (2D:4D) and handgrip strength in subjects of Han ethnicity: Impact of sex and age. Am J Phys Anthropol. 2012;149:266–71. doi: 10.1002/ajpa.22130. [DOI] [PubMed] [Google Scholar]
- 8.Ciumas C, Lindén Hirschberg A, Savic I. High fetal testosterone and sexually dimorphic cerebral networks in females. Cereb Cortex. 2009;19:1167–74. doi: 10.1093/cercor/bhn160. [DOI] [PubMed] [Google Scholar]
- 9.Cattrall FR, Vollenhoven BJ, Weston GC. Anatomical evidence for in utero androgen exposure in women with polycystic ovary syndrome. Fertil Steril. 2005;84:1689–92. doi: 10.1016/j.fertnstert.2005.05.061. [DOI] [PubMed] [Google Scholar]
- 10.Voracek M, Dressler SG. Digit ratio (2D:4D) in twins: Heritability estimates and evidence for a masculinized trait expression in women from opposite-sex pairs. Psychol Rep. 2007;100:115–26. doi: 10.2466/pr0.100.1.115-126. [DOI] [PubMed] [Google Scholar]
- 11.Manning JT. Resolving the role of prenatal sex steroids in the development of digit ratio. Proc Natl Acad Sci U S A. 2011;108:16143–4. doi: 10.1073/pnas.1113312108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zheng Z, Cohn MJ. Developmental basis of sexually dimorphic digit ratios. Proc Natl Acad Sci U S A. 2011;108:16289–94. doi: 10.1073/pnas.1108312108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gobrogge KL, Breedlove SM, Klump KL. Genetic and environmental influences on 2D:4D finger length ratios: A study of monozygotic and dizygotic male and female twins. Arch Sex Behav. 2008;37:112–8. doi: 10.1007/s10508-007-9272-2. [DOI] [PubMed] [Google Scholar]
- 14.Medland SE, Zayats T, Glaser B, Nyholt DR, Gordon SD, Wright MJ, et al. A variant in LIN28B is associated with 2D:4D finger-length ratio, a putative retrospective biomarker of prenatal testosterone exposure. Am J Hum Genet. 2010;86:519–25. doi: 10.1016/j.ajhg.2010.02.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Auger J, Eustache F. Second to fourth digit ratios, male genital development and reproductive health: A clinical study among fertile men and testis cancer patients. Int J Androl. 2011;34:e49–58. doi: 10.1111/j.1365-2605.2010.01124.x. [DOI] [PubMed] [Google Scholar]
- 16.Muller DC, Baglietto L, Manning JT, McLean C, Hopper JL, English DR, et al. Second to fourth digit ratio (2D:4D), breast cancer risk factors, and breast cancer risk: A prospective cohort study. Br J Cancer. 2012;107:1631–6. doi: 10.1038/bjc.2012.418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Manning JT, Bundred PE. The ratio of 2 nd to 4 th digit length and age at first myocardial infarction in men: A link with testosterone? Br J Cardiol. 2001;8:720–3. [Google Scholar]
- 18.Fink B, Neave N, Manning JT. Second to fourth digit ratio, body mass index, waist-to-hip ratio, and waist-to-chest ratio: Their relationships in heterosexual men and women. Ann Hum Biol. 2003;30:728–38. doi: 10.1080/03014460310001620153. [DOI] [PubMed] [Google Scholar]
- 19.Fink B, Manning JT, Neave N. The 2 nd -4 th digit ratio (2D:4D) and neck circumference: Implications for risk factors in coronary heart disease. Int J Obes (Lond) 2006;30:711–4. doi: 10.1038/sj.ijo.0803154. [DOI] [PubMed] [Google Scholar]
- 20.English KM, Mandour O, Steeds RP, Diver MJ, Jones TH, Channer KS. Men with coronary artery disease have lower levels of androgens than men with normal coronary angiograms. Eur Heart J. 2000;21:890–4. doi: 10.1053/euhj.1999.1873. [DOI] [PubMed] [Google Scholar]
- 21.Pokrywka L, Rachoń D, Suchecka-Rachoń K, Bitel L. The second to fourth digit ratio in elite and non-elite female athletes. Am J Hum Biol. 2005;17:796–800. doi: 10.1002/ajhb.20449. [DOI] [PubMed] [Google Scholar]
- 22.Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet. 2005;365:1415–28. doi: 10.1016/S0140-6736(05)66378-7. [DOI] [PubMed] [Google Scholar]
- 23.Finucane MM, Stevens GA, Cowan MJ, Danaei G, Lin JK, Paciorek CJ, et al. National, regional, and global trends in body-mass index since 1980: Systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9·1 million participants. Lancet. 2011;377:557–67. doi: 10.1016/S0140-6736(10)62037-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Adediran O, Akintunde AA, Edo AE, Opadijo OG, Araoye AM. Impact of urbanization and gender on frequency of metabolic syndrome among native Abuja settlers in Nigeria. J Cardiovasc Dis Res. 2012;3:191–6. doi: 10.4103/0975-3583.98890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Osuji CU, Omejua EG. Prevalence and characteristics of the metabolic syndrome among newly diagnosed hypertensive patients. Indian J Endocrinol Metab. 2012;16(Suppl 1):S104–9. doi: 10.4103/2230-8210.94256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Wahab KW, Sani MU, Yusuf BO, Gbadamosi M, Gbadamosi A, Yandutse MI. Prevalence and determinants of obesity - A cross-sectional study of an adult Northern Nigerian population. Int Arch Med. 2011;4:10. doi: 10.1186/1755-7682-4-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ashwell M, Gunn P, Gibson S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: Systematic review and meta-analysis. Obes Rev. 2012;13:275–86. doi: 10.1111/j.1467-789X.2011.00952.x. [DOI] [PubMed] [Google Scholar]
- 28.Onat A, Hergenç G, Yüksel H, Can G, Ayhan E, Kaya Z, et al. Neck circumference as a measure of central obesity: Associations with metabolic syndrome and obstructive sleep apnea syndrome beyond waist circumference. Clin Nutr. 2009;28:46–51. doi: 10.1016/j.clnu.2008.10.006. [DOI] [PubMed] [Google Scholar]
- 29.Abba IS, Gabriel O, Domnic M, Godfery M, Dare SS, Mohammed YG, et al. Assessment of the relationship between digit lengths and circumferences of the waist and hip amongst Ugandans. Asian J Med Sci. 2012;4:113–6. [Google Scholar]
- 30.Cohen JA. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Associates; 1988. Statistical Power Analysis for the Behavioural Sciences. [Google Scholar]
- 31.Danborno B, Adebisi SS, Adelaiye AB, Ojo SA. Sexual dimorphism and relationship between chest, hip and waist circumference with 2D, 4D and 2D:4D in Nigerians. Internet J Biol Anthropol. 2008;1:2. [Google Scholar]
- 32.Oladipo G, Fawehinmi H, Edibamode E, Osunwoke E, Ordu KS. Second to fourth digit ratio in Nigerian Igbos and Yorubas. Sci Res Essay. 2009;4:1146–8. [Google Scholar]
- 33.Gwunireama IU, Ihemelandu EC. Geographical influence on digit ratio (2D:4D): A case study of Andoni and Ikwerre ethnic groups in Niger delta, Nigeria. J Appl Biosci. 2010;27:1736–41. [Google Scholar]
- 34.Ibegbu AO, Danjuma ZC, Hamman WO, Umana UE, Ikyembe D, Musa SA. Association of the index (2nd) and ring (4th) digit ratios with some physical attributes in Ebira Ethnic Group of Nigeria. Appl Technol Innov. 2012;7:46–54. [Google Scholar]
- 35.Hönekopp J, Watson S. Meta-analysis of digit ratio 2D:4D shows greater sex difference in the right hand. Am J Hum Biol. 2010;22:619–30. doi: 10.1002/ajhb.21054. [DOI] [PubMed] [Google Scholar]
- 36.Williams TJ, Pepitone ME, Christensen SE, Cooke BM, Huberman AD, Breedlove NJ, et al. Finger-length ratios and sexual orientation. Nature. 2000;404:455–6. doi: 10.1038/35006555. [DOI] [PubMed] [Google Scholar]
- 37.Coates JM, Gurnell M, Rustichini A. Second-to-fourth digit ratio predicts success among high-frequency financial traders. Proc Natl Acad Sci U S A. 2009;106:623–8. doi: 10.1073/pnas.0810907106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Manning JT. New Brunswick, NJ: Rutgers University Press; 2002. Digit Ratio: A Pointer to Fertility, Behavior, and Health. [Google Scholar]
- 39.Geschwind N, Galaburda AM. Cerebral lateralization. Biological mechanisms, associations, and pathology: I. A hypothesis and a program for research. Arch Neurol. 1985;42:428–59. doi: 10.1001/archneur.1985.04060050026008. [DOI] [PubMed] [Google Scholar]
- 40.Kondo T, Zákány J, Innis JW, Duboule D. Of fingers, toes and penises. Nature. 1997;390:29. doi: 10.1038/36234. [DOI] [PubMed] [Google Scholar]
- 41.Fujita Y, Kouda K, Nakamura H, Iki M. Cut-off values of body mass index, waist circumference, and waist-to-height ratio to identify excess abdominal fat: Population-based screening of Japanese school children. J Epidemiol. 2011;21:191–6. doi: 10.2188/jea.JE20100116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.He YH, Chen YC, Jiang GX, Huang HE, Li R, Li XY, et al. Evaluation of anthropometric indices for metabolic syndrome in Chinese adults aged 40 years and over. Eur J Nutr. 2012;51:81–7. doi: 10.1007/s00394-011-0195-2. [DOI] [PubMed] [Google Scholar]
- 43.Lee S, Kuk JL, Hannon TS, Arslanian SA. Race and gender differences in the relationships between anthropometrics and abdominal fat in youth. Obesity (Silver Spring) 2008;16:1066–71. doi: 10.1038/oby.2008.13. [DOI] [PubMed] [Google Scholar]
- 44.Wu HY, Xu SY, Chen LL, Zhang HF. Waist to height ratio as a predictor of abdominal fat distribution in men. Chin J Physiol. 2009;52:441–5. doi: 10.4077/cjp.2009.amh064. [DOI] [PubMed] [Google Scholar]
- 45.Al-Odat AZ, Ahmad MN, Haddad FH. References of anthropometric indices of central obesity and metabolic syndrome in Jordanian men and women. Diabetes Metab Syndr. 2012;6:15–21. doi: 10.1016/j.dsx.2012.05.012. [DOI] [PubMed] [Google Scholar]
- 46.Dong X, Liu Y, Yang J, Sun Y, Chen L. Efficiency of anthropometric indicators of obesity for identifying cardiovascular risk factors in a Chinese population. Postgrad Med J. 2011;87:251–6. doi: 10.1136/pgmj.2010.100453. [DOI] [PubMed] [Google Scholar]
- 47.Guasch-Ferré M, Bulló M, Martínez-González MÁ, Corella D, Estruch R, Covas MI, et al. Waist-to-height ratio and cardiovascular risk factors in elderly individuals at high cardiovascular risk. PLoS One. 2012;7:e43275. doi: 10.1371/journal.pone.0043275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Manning JT, Henzi P, Venkatramana P, Martin S, Singh D. Second to fourth digit ratio: Ethnic differences and family size in English, Indian and South African populations. Ann Hum Biol. 2003;30:579–88. doi: 10.1080/0301446032000112689. [DOI] [PubMed] [Google Scholar]
- 49.Neave N, Laing S, Fink B, Manning JT. Second to fourth digit ratio, testosterone and perceived male dominance. Proc Biol Sci. 2003;270:2167–72. doi: 10.1098/rspb.2003.2502. [DOI] [PMC free article] [PubMed] [Google Scholar]