

Abstract
Background: The manual lymphatic drainage in lymphedema has proved to be successful; however, this method cannot be applied to millions of patients around the world. The only solution is to offer inexpensive, easily accessible mechanical devices for pneumatic compression (IPC). These devices should be designed on parameters of edema fluid hydromechanics. Recent data point to high pressures and long time of compression.
Aim: To validate the effects of 3 years daily high pressure, long inflation time IPC therapy in terms of decrease of limb circumference/volume, tissue elasticity, histological changes, and incidental complications.
Methods: A group of 18 patients with unilateral leg lymphedema stage II to IV was treated for a period of 3 years using an 8-chamber sleeve, sequential inflation of chambers to 100–120 mmHg for 50 sec (total 400 sec). Limb circumference and tissue tonicity were measured at monthly intervals. Correlation between decrease in calf and thigh circumference and increase in elasticity was done.
Results: The treatment revealed durable permanent decrease of limb circumference and increased elasticity of tissues. The improvement was most expressed in the calf above the ankle and mid-calf. No complications as thigh ring or chronic genital edema were observed. There was no direct correlation between the decrease in limb circumference and increase in elasticity, most likely due to different mass of fibrous tissue.
Conclusions: IPC takes over the permanently missing function of the obliterated lymphatics by squeezing edema tissue fluid to the regions with normal lymphatic drainage. The limb circumference is decreased or at least does not further increase, elasticity of tissue is increased and maintained. No complications in limb tissues were observed. The long-term, high pressure IPC, long inflation timed therapy can be safely be recommended to patients with lower limb lymphedema.
Introduction
Lymphedema of lower limbs is a consequence of obstruction of the main lymphatics caused by inflammation, trauma, excision of lymph nodes, and irradiation. In a percentage of cases, the etiology remains unknown and the term “idiopathic” is being used. Lymphedema has been defined as an abnormal accumulation of capillary filtrate with proteins, cytokines and chemokines, recirculating lymphocytes, products of parenchymatous cells, and debris of senescent cells. Edema of tissues develops once the intercellular space has been filled with stagnant fluid.
Persons afflicted with lymphedema have significant problems as impaired extremity function, recurrent episodes of soft tissue inflammation (dermatolymphangioadenitis), lymphorrhea, and unsatisfactory cosmesis, and a variety of psychological and social issues.
Therapeutic efforts remain focused on minimizing the edema, mitigating complications, and on reversing and restoring the functional and cosmetic nature of the limb. The therapies available for edema reduction are divided into three categories: rehabilitative interventions, pharmacologic therapies, and surgery. Among the conservative methods, external compression remains the mainstay modality. One of the most promising methods is intermittent pneumatic compression (IPC). The very high number of cases, estimated by WHO around 300 million, requires simple, inexpensive, and easily accessible compression devices all over the world. Although manual lymphatic drainage and its various modifications have proved to be successful, the problem of its accessibility for patients cannot be solved due to the insufficient number of therapists for those large cohorts of patients. The only solution is mechanization of the compression method using pneumatic devices. The construction and function of these devices should be based on the physiological parameters of tissue fluid (edema fluid) hydromechanics.1,2 We measured the tissue fluid (edema fluid) (TF) pressures and flow using various types pneumatic compression devices in a group of patients with lower limb lymphedema and estimated the most effective parameters for fluid movement.3
It was found that the highest flow of 20 to 120 mL/1 h cycle was obtained with compression pressures between 80 and 120 mmHg and inflation timing 6–7 min, sequentially from foot to groin. Devices with such technical parameters have been constructed by Biocompression.Co, Moonachie, NJ, USA.
The question arose how effective would be a long-term therapy with such a pneumatic compression device in terms of a decrease of limb circumference/volume, tissue elasticity, histological changes, and incidental complications. In this study, we tried its effectiveness in a group of randomly selected patients treated continuously for a period of 3 years. The changes in limb circumference and tissue tonicity were measured at monthly intervals. Correlation between decrease in calf and thigh circumference and increase in elasticity was carried out.
Material and methods
Patients
The study was carried out on 18 patients, age 28–62 years, mean weight 72 kg (48–74), mean height of 156 cm (161–172), with diagnosis of unilateral lymphedema of lower limb, stage II to IV, duration of 3 to 12 years. They were included into the study in order as they appeared in the out-patients clinic. Thirteen patients reported foot skin infection episodes in the past, followed by transient foot and calf edema. Larger edema developed 1 to 5 years later, and in 5 cases was complicated by 1 to 3 attacks of dermato-lymphangio-adenitis. In 4 patients, edema developed without any detectable reason. Cases with acute inflammation, chronic venous insufficiency, and systemic etiology of edema were excluded from the study. The consent of patients was obtained and the study was approved by the Warsaw Medical University ethics committee.
Clinical diagnosis
Diagnosis and staging were based on clinical evaluation: level of edema embracing limb from foot to groin, and degree of skin keratosis and fibrosis. Briefly, in stage II, pitting edema affected foot and lower half of the calf; in stage III, foot and calf were involved, with hard foot and ankle area skin; in stage IV, the whole limb was edematous with foot and calf skin hyperkeratosis and papillomatosis of toes.4 Evaluation of lymphatic pathways was done on lymphoscintigraphic images. In stage II, there was spread of tracer in foot and lower part of calf, interrupted outline of a single lymphatic, and a few small inguinal nodes with irregular outline. In stage III, no draining lymphatics were seen, with some inguinal nodes of irregular outline appearing after 2 hours. Stage IV was characterized by spread of tracer in the foot and entire calf without visualization of collecting lymphatics and nodes. In the healthy contralateral limb, lymphoscintigraphy revealed a normal outline of superficial and deep lymphatics.
Compression device
We used a device produced for us by Biocompression (Moonachie, NJ) pneumatic compression appliance manufacturer. The device met the following conditions, proposed by us: multi-chamber, sequential inflation, gradient inflation pressure, time of inflation sufficient for translocation of tissue fluid to proximal region, no deflation of distal chambers to prevent fluid back-flow and venous stasis in the superficial limb system. It was composed of eight segments 9 cm long each, sequentially inflated, inflation pressures were regulated from 50 to 125 mmHg, gradient pressures decreasing proximally by 20%, inflation time of each chamber was 50 sec, total inflation time equaled 400 sec. There was no deflation of distal chambers, deflation time of all chambers was 50 sec at the end of each cycle. The inflation pressures were measured in chambers and compared with those on pumping device manometers. The differences ranged between 2 and 5 mmHg. The sleeve embraced the whole limb up to the inguinal crease.
Girth measurement
Limb circumference was measured at five levels as shown on Figure 1. The results were presented in percent of girth but not volume changes. Total volume change does not reflect changes at various limb levels with different soft tissue mass, from where most of the edema fluid is evacuated. False results are obtained as fluid accumulates in the space of the popliteal fossa and in the upper thigh loose tissue region. Presentation of girth changes provides a better picture of fluid translocation and the limb profile.
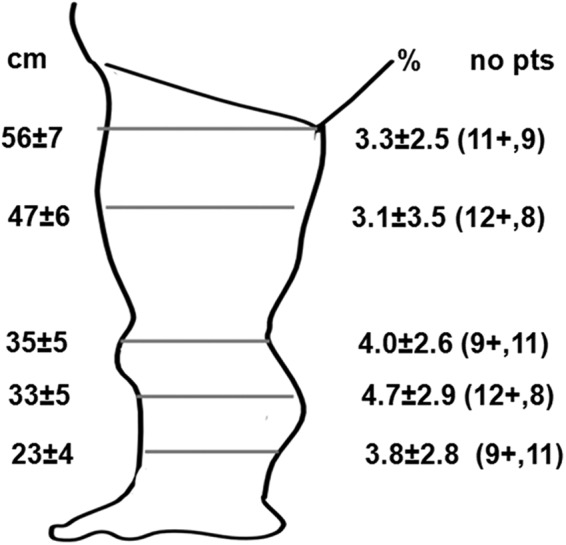
FIG. 1.
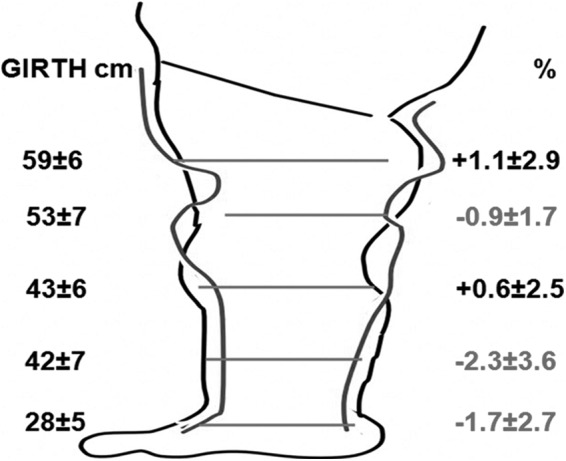
The effect of the initial 1 h intermittent pneumatic compression (IPC) on the limb circumference—the girth of limb in cm before and in percent of decrease after IPC. There was a statistically significant decrease in lower calf and thigh, and increase under the knee and in the groin. This last was brought about by translocation of edema fluid. Internal outline of the limb shows change of the limb shape. High standard deviation could be attributed to the large individual variations in individual circumferences and stiffness of tissues; n=18, *p<0.05.
Tonometry
Tissue tonometry was performed at the same levels as those of girth measurements. A deep tissue tonometer was used. It was composed of a manometer (Wagner, Seattle, USA) connected to a 10 mm long round bottom shape plunger of 1 sq.cm surface area. It was pressed against tissues to the depth of 10 mm within 5 sec. The applied force was read off on the manometer scale and expressed in g×103/sq.cm.
Study setting
The IPC was applied in each patient daily for 45 min for 24–36 months. The sleeve inflation pressure started at foot level with 120 mmHg with a gradual decrease by 20% in the groin. The inflation time was 50 sec/chamber amounting to 400 sec for the whole sleeve. It was followed by 50 sec deflation. Each compression procedure was composed of 9–10 cycles. The measurements were taken after the first use of IPC, then following 1, 12, and 24–36 months, at monthly intervals. All 1 to 36 months follow-up measurements were taken before starting daily IPC. Patients wore the same type semi-elastic noncustomized compression stockings grade 2, standard factory size fitting to limb dimensions, advised by an experienced fitter. They changed stockings every 6 months. The limb circumference was also measured in the contralateral healthy leg of each patient. Lack of lymphedema was confirmed on lymphoscintigraphy.
Statistical evaluation
Data were expressed in cm (circumference) and g/sq.cm (tonometry) as means±sd. For statistical evaluation of differences in circumference and tonometry of the same patient over various time periods, a double tail t-Student test was applied with significance at <0.05 level.
Results
The first one hour IPC showed: 1. decrease in circumference of lower parts of the calf and thigh with increase below knee and in the groin region. This was caused by TF translocation (Fig.1); 2. decrease of tissue stiffness measured by tonometry (Fig. 2). One month of IPC revealed: 1. decrease of circumferences at all limb levels (Fig. 3); 2. decrease of stiffness of tissues measured by tonometry (Fig. 4a.b), 3. In most cases stabilization of circumferences and tissue elasticity with no further decrease. In some others, gradual decrease lasted for another 1–2 months. One year of IPC showed: 1. further decrease of circumference in some cases (Fig. 3) and maintenance of decreased stiffness (Fig. 5). Three years of IPC showed: 1. maintenance of decreased circumferences (Fig. 6) and stiffness (Fig. 7a,b), with major fluctuations, most likely depending on patients' compliance to the daily application of IPC. No further decrease in parameters of edema was observed what can be accounted for by restoration of normal tissue (intercellular) fluid volume but not of cells and matrix structure (fibroblasts, collagen). The IPC in the third year did not further decrease the circumferences at all levels (Fig. 8); however, it increased tissue elasticity when measured immediately after pneumatic compression (Fig. 9). Major standard deviations in limb girth were due to individual reactions to IPC presumably depending on the degree of tissue induration. Interestingly, simultaneous measuring of the circumference of contralateral normal limbs (no stockings) revealed, at the end of the 3 years follow-up, a slight increase in 60% of cases (Fig. 10). There was no correlation between the decrease in limb circumference and increase in elasticity at specified levels, most likely due to different degree of subcutaneous fibrosis, not to be measured clinically without multiple biopsies.
FIG. 2.
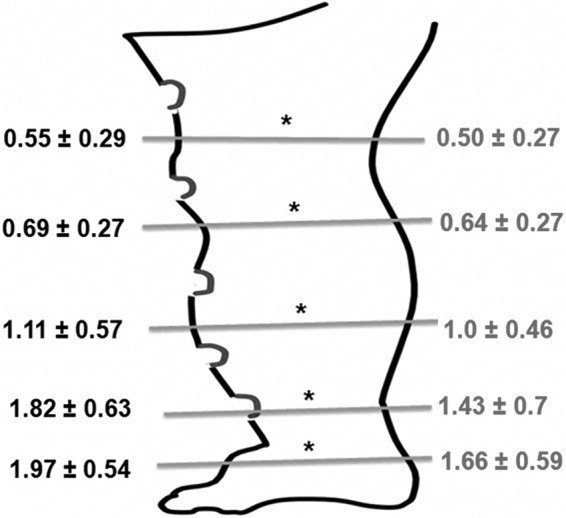
Tonometry of soft tissues after 1 h of IPC. Evident decrease of force required for producing 10 mm indentation of tissues, expressed in g/sq.cm×103, reflecting increased elasticity. It was less of 100–300 g/sq.cm in the calf. *Pre- vs. post-compression p<0.05, n=18.
FIG. 3.
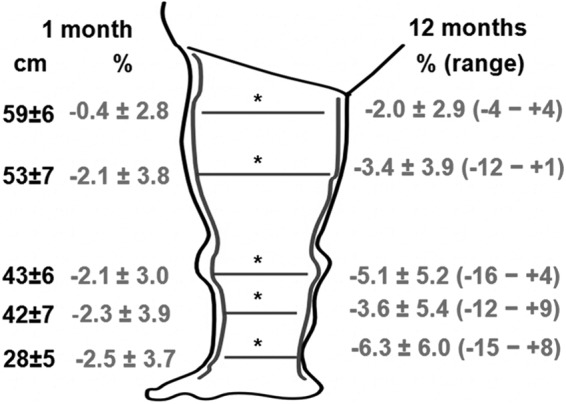
The effect of 1 and 12 months of IPC on the limb circumference. Data expressed in % and range (after 12 months). Statistically significant decrease compared to the pretreatment data for 1 month and 12 months therapy (*p<0.05). Expressed in cm, the 12 months decrease ranged between 1.2 and 2.2 cm. Internal outline of the limb shows change of the limb shape. High standard deviation could be ascribed to the large individual variations in individual circumferences and stiffness of tissues; n=18.
FIG. 4.

Tonometry of soft tissues after 1 month of IPC: (a) mean±sd, in g/sq.cm×103 and (b) in percent of change, range, and number of patients. Decrease of applied force by 220 to 170 g or 18%–14% in the calf of 80%–90% of patients; n=18.
FIG. 5.
Tonometry of soft tissues after 12 months of IPC. Evident decrease of force required for 10 mm indentation of calf tissues by 200–700 g, expressed as means±sd and range in g/sq.cm×103±; *p<0.05; n=18.
FIG. 6.
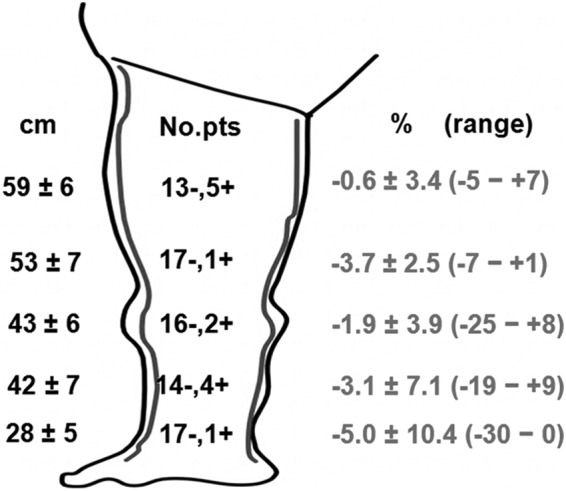
The effect of 24–36 months of IPC on the limb circumference. Data expressed in mean %±sd, range, and number of patients with decrease. Statistically significant decrease compared to the pretreatment data. High standard deviation could be ascribed to the large individual variations in individual circumferences and stiffness of tissues. Note that limb circumference decrease is most expressed in the calf, n=18.
FIG. 7.
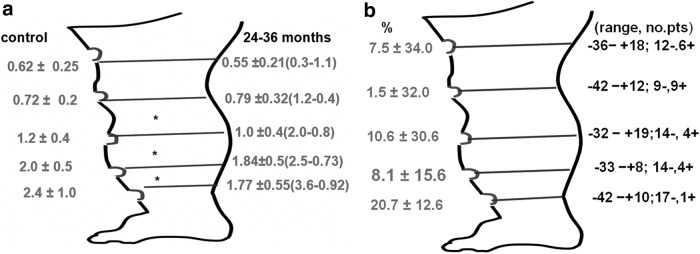
Tonometry of soft tissues after 24–36 months of IPC. Evident decrease of force required for 10 mm indentation of tissues expressed in (a) mean±sd, g/sq.cm. and (b) percent of changes, range, and number of patients with decreased data. High standard deviation and range of data could be ascribed to the large individual variations in individual circumferences and stiffness of tissues. Most evident decrease observed in the calf; *p<0.05, n=18.
FIG. 8.
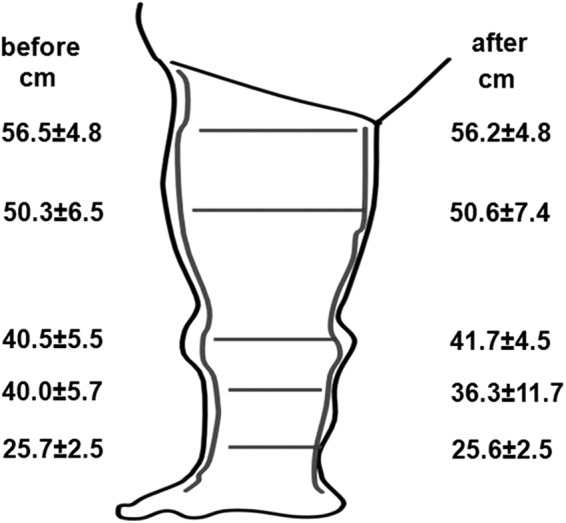
The effect of 1 h compression in patients after 24–36 months of therapy on limb circumference. Note lack of statistically significant differences. This may be accounted for by previous evacuation of tissue fluid (edema fluid) excess in course of long-term compression therapy. Data are cm, means±sd, n=12.
FIG. 9.
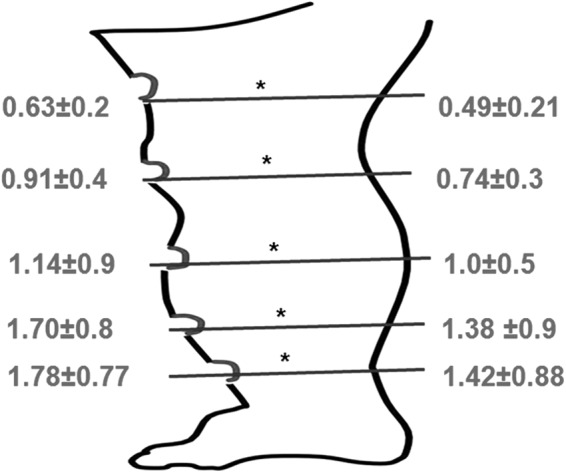
The effect of 1 h compression in patients after 24–36 months of therapy on limb tissue tonometry. Evident decrease of force required for 10 mm indentation of calf tissues by 200–360 g, expressed as means±sd, in g/sq.cm×103; *p<0.05, n=12.
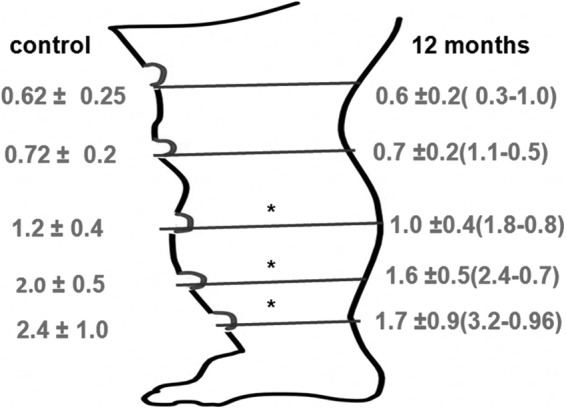
FIG. 10.
The changes in the circumference of the contralateral healthy limb in the 24–36 months follow-up. Note that around 50% of limbs had increase of the girth by a mean of 3%–4%; in another 50% there was no change; n=18.
Discussion
Results of our 3 years treatment of lower limb lymphedema by daily IPC revealed permanent decrease of limb circumference and increased elasticity of tissues. The improvement was most expressed in the calf above the ankle and mid-calf. No complications as thigh ring or genital edema were observed. Our findings corroborate the data from the 2004–2011 literature on the use of IPC.5 Well controlled studies have documented its usefulness in the treatment of lower limb lymphedema, thereby supporting their continued use.5–20 However, no long-term observations have so far been documented. The difference between our and others' studies relied mainly on that we applied long inflation times and relatively high pressures, based on our previously published tissue fluid pressure/flow data.4 Moreover, we measured not only the limb circumference but also tissue elasticity using a deep tissue tonometry. This gave us an indirect information of a decreased tissue fluid pressure, so important for prevention of fibroblast stimulation and subsequent fibrosis.21,22
We found that measuring circumference changes at various levels of the limb better illustrates the dynamics of TF translocation during IPC than calculation of the total volume, since there is translocation of fluid to the popliteal fossa containing loose connective tissue and to the groin region with lax skin and fat layer. This makes the volume change data questionable. We also followed the effect of IPC on tissue elasticity, using a deep tissue tonometer measuring force necessary to produce a 10 mm deep indentation. Edema fluid accumulates deep in the subcutaneous tissue and perifascial space, and is responsible, along with fibrous structures, for tissue stiffness. The tonometer plunger should then reach deep tissues. Not only fluid accumulating in tissues and generating increased pressure but also the recoil force of mechanically strong matrix (collagen and elastic fibers) create resistance to the tonometer. The situation resembles that of a water-soaked sponge. This requires high force in order to mobilize TF. We reported previously that tonometry-measured force of 2000 g/sq.cm in stage III of lymphedematous calf generates tissue fluid pressures of only 30–60 mmHg.4 This pressure level could be obtained in the subcutaneous tissue of the same patients by applying IPC pressure of 120 mmHg. The tonometry findings justified using high IPC pressures in our group of patients.
Furthermore, tonometry studies showed that elasticity of lower limbs tissue is lower in the calf with more hard skin than in the thigh, and that most efforts for improvement using IPC should be directed at the regions above the ankle, the site of common dermatitis, ulcers, and lymphorrhea. Indeed, the pre-and post-IPC recordings showed most decrease of stiffness (or increase in elasticity) in the calf in 100% of patients, including the 3-year follow-up patients. Thus, tonometry provided objective evidence of the effectiveness of long-term IPC.
We did not stratify our patients and IPC results according to the stage and degree of fibrosis, although fibrosis of tissue adversely affects the IPC results. This was caused by a low number of investigated cases. Richmand et al. showed that more than 80% of patients in both the poor-response and partial-response groups had long-lasting lymphedema with subcutaneous fibrosis.11
We suggest that the decrease of the mobile tissue fluid volume and pressure prevents secondary tissue changes. Thus, the IPC therapy is aimed not only at evacuation of excess tissue (edema fluid) to decrease limb volume/weight but also, and probably more importantly, at prevention of secondary tissue changes developing mainly in the lower part of the calf as hardening of skin and subcutis, lymph leakage, ulceration, all seen in advanced stages of lymphedema. Daily repeated hydraulic decompression of leg soft tissues should eliminate the pressure on fibroblasts and tension on keratinocytes, maintain normal intercellular fluid chemistry, decrease the distance between blood capillaries and tissue cells, preventing their malnutrition, and evacuate stagnant immune cell products responsible for formation of fibrosis.22,23
After months of IPC therapy, stabilization of limb girth and elasticity occurred. There was no further decrease of limb volume. This can be explained by the poroelastic structure of the subcutaneous tissue resembling that that of a sponge. The skeleton is built of the intercellular matrix, mostly collagen. Fluid accumulates between the collagen bundles. During compression, edema fluid is squeezed to the non-compressed regions; however, the collagen fibers recoil force remains unchanged. Therefore, after compression, the tissue skeleton regains its pre-massage shape, although there is less edema fluid in between the fibers. This partly explains why decrease of limb circumference does not correlate with increase of limb tissue elasticity.
All patients wore semi-elastic compression stockings. Some investigators may ascribe the observed decrease in limb circumference and increase in tissue elasticity to the elastic material. However, evident large change in circumference and elasticity during each IPC procedure proved that this modality is responsible for edema fluid evacuation, whereas stockings do compress tissues preventing re-accumulation of fluid.
It has been also been reported that pumps may be ineffective and perhaps dangerous. However, extensive clinical experience does not support these claims, and the therapy-specific adverse effects (not edema) occur in less than 1% of patients. Some researchers have suggested that lower limb users may be at risk of developing genital lymphedema.23 We did not observe chronic lymphedema of genitals during long-term IPC application. Neither did we come across formation of a thigh ring. Recent experimental studies could not prove induction of fibrosis by tissue fluid proteins in short-term observations.24 The IPC increase of tissue elasticity, measured immediately after pneumatic compression, even in the 3-year-treated patients, proved that warnings that IPC may cause development of a thigh fibrous ring remain unjustified.
Interestingly, evaluation of contralateral healthy limbs' circumference showed that in 60% of cases, a girth increase was observed. This strengthens the importance of IPC in decreasing the size of the edematous limbs, which could become larger without compression therapy, as it happened in course of time to the apparently normal contralateral limb.
In conclusion, IPC takes over the permanently missing function of the obliterated lymphatics by squeezing TF to the regions with normal lymphatic drainage. The limb circumference is decreased or at least does not increase, and elasticity of tissue is increased and maintained.
Author Disclosure Statement
No competing financial interests exist.
This work was supported by grants from the National Science Center (Poland) NN 404113139 and National Center for Research and Development (Poland) NR 18002606.
References
- 1.Olszewski WL, Jain P, Ambujam G, Zaleska M, Cakala M. Topography of accumulation of stagnant lymph and tissue fluid in soft tissues of human lymphedematous lower limbs. Lymphat Res Biol 2009;7:239–245 [DOI] [PubMed] [Google Scholar]
- 2.Olszewski WL, Jain P, Ambujam G, Zaleska M, Cakala M, Gradalski T. Tissue fluid pressure and flow during pneumatic compression in lymphedema of lower limbs. Lymphat Res Biol 2011;9:77–83 [DOI] [PubMed] [Google Scholar]
- 3.Zaleska M, Olszewski WL, Jain P, Gogia S, Arun Rekha , Mishra S, Durlik M. Pressures and timing of intermittent pneumatic compression devices for efficient tissue fluid and lymph flow in limbs with lymphedema. Lymphat Res Biol 2013;11:227–232 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Olszewski WL, Zaleska M, Cakala M, Victor J, Tripathi M. Tissue fluid and lymph space pressure/volume relationship in obstructive lymphedema of lower limbs. Lymphology 2007;40:395 [Google Scholar]
- 5.Feldman JL, Stout NL, Wanchai A, Stewart BR, Cormier JN, Armer JM. Intermittent pneumatic compression therapy: A systemic review. Lymphology 2012;45:13–25 [PubMed] [Google Scholar]
- 6.Special report: Comparative efficacy of different types of pneumatic compression pumps for the treatment of lymphedema. Technologica MAP Suppl 1998:42–43 [PubMed] [Google Scholar]
- 7.Centers for Medicare and Medicaid Services (CMS). National Coverage Determination for Pneumatic Compression Devices, Publication number 100-3, Manual section number 280.6
- 8.Blue Cross and Blue Shield Association Technology Assessment Program (TEC). Special report: Comparative efficacy of different types of pneumatic compression pumps for the treatment of lymphedema. 1998:2. [PubMed]
- 9.Palmetto GBA-Statistical Analysis Durable Medical Equipment Carrier (SADMERC). Durable Medical Equipment Coding System (DMECS) Product Search for HCPCS codes E0650, E0651, E0652. Retrieved from http://www3.palmettogba.com/dmecs/do/productsearch
- 10.National Lymphedema Network (NLN). Position statement of the national lymphedema network. Treatment. 2006August10 Retrieved from http://www.lymphnet.org/pdf Docs/nlntreatment
- 11.Richmand DM, O'Donnell TR, Jr, Zelikovski A. Sequential pneumatic compression for lymphedema. A controlled trial. Arch Surg 1985;120:1116–1119 [DOI] [PubMed] [Google Scholar]
- 12.Klein MJ, Alexander MA, Wright JM, Redmond CK, LaGasse AA. Treatment of adult lower extremity lymphedema with the Wright Linear pump: Statistical analysis of a clinical trial. Arch PMR 1988;69:202–206 [PubMed] [Google Scholar]
- 13.Yamazaki Z, Idezuki Y, Nemoto T, Togawa T. Clinical experiences using pneumatic massage therapy for edematous limbs over the last 10 years. Angiology 1988;39:154–163 [DOI] [PubMed] [Google Scholar]
- 14.Pappas CJ, O'Donnell TF., Jr.Long-term results of compression treatment for lymphedema. J Vasc Surg 1992;16:555–562 [DOI] [PubMed] [Google Scholar]
- 15.Rockson SG, Miller LT, Senie R, et al. American cancer society lymphedema workshop. Workgroup III: Diagnosis and management of lymphedema. Cancer 1998;83:2882–2885 [DOI] [PubMed] [Google Scholar]
- 16.Mayrovitz HN. Interface pressures produced by two different types of lymphedema therapy devices. Phys Ther 2007;87;1379–1388 [DOI] [PubMed] [Google Scholar]
- 17.Ridner S, McMahon E, Dietrich MS, Hoy S. Home-based lymphedema treatment in patients with cancer-related lymphedema or noncancer-related lymphedema. Oncol Nurs Forum 2008;35:671–680 [DOI] [PubMed] [Google Scholar]
- 18.Adams KE, Rasmussen JC, et al. Direct evidence of lymphatic function improvement after advanced pneumatic compression device treatment of lymphedema. Biomed Opt Express 2010;1:114–125 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Oremus M, Dayes I. Diagnosis and treatment of secondary lymphedema. McMaster University Evidence-based Practice Center under contract to the Agency for Healthcare Research and Quality Technology Assessment, Blue Cross of Idaho MP 1.01.18 Pneumatic Compression Pumps for Treatment of Lymphedema [Google Scholar]
- 20.Rockson SG. Accruing evidence for a beneficial role of pneumatic biocompression in lymphedema. Lymphat Res Biol 2010;8:4. [DOI] [PubMed] [Google Scholar]
- 21.Chunyi LI. Exploration of the mechanism underlying neogenesis and regeneration of postnatal mammalian skin. IJMBF 2010;16;1–17 [Google Scholar]
- 22.Agrawal K, Agrawal S. Tissue regeneration during tissue expansion and choosing an expander. Indian J Plast Surg 2012;46:7–15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Boris M, Weindorf S, Lasinski BB. The risk of genital edema after external pump compression for lower limb lymphedema. Lymphology 1998;31:15–20 [PubMed] [Google Scholar]
- 24.Markhus CE, Karlsen TV, Wagner M, Svendsen ØS, Tenstad O, Alitalo K, Wiig H. Increased interstitial protein because of impaired lymph drainage does not induce fibrosis and inflammation in lymphedema. Arterioscler Thromb Vasc Biol 2013;33:266–274 [DOI] [PubMed] [Google Scholar]