

Abstract
Appropriate management of temporomandibular disorders (TMD) requires an understanding of the underlying dysfunction associated with the temporomandibular joint (TMJ) and surrounding structures. A comprehensive examination process, as described in part 1 of this series, can reveal underlying clinical findings that assist in the delivery of comprehensive physical therapy services for patients with TMD. Part 2 of this series focuses on management strategies for TMD. Physical therapy is the preferred conservative management approach for TMD. Physical therapists are professionally well-positioned to step into the void and provide clinical services for patients with TMD. Clinicians should utilize examination findings to design rehabilitation programs that focus on addressing patient-specific impairments. Potentially appropriate plan of care components include joint and soft tissue mobilization, trigger point dry needling, friction massage, therapeutic exercise, patient education, modalities, and outside referral. Management options should address both symptom reduction and oral function. Satisfactory results can often be achieved when management focuses on patient-specific clinical variables.
Keywords: Conservative management, Review, Temporomandibular joint disorders
Physical therapists are trained in the utilization of multimodal approaches to address musculoskeletal dysfunction. Traditionally, this approach has been based on the biomedical model, which continues to play an important role in the management of temporomandibular disorders (TMD). It is paramount to ensure therapeutic interventions are selected based on their relevance to patient-centered findings that can be monitored over time for relative change. This impairment-based approach is known to the physical therapy profession and has been shown to be practical in the management of musculoskeletal conditions.1–3 Additionally, clinicians must evaluate and manage variables related to chronic pain such as hyperalgesia and allodynia when working with patients with TMD, though a sufficiently thorough review of this portion of management is beyond the scope of this paper. Part 1 of this two-part series reviewed the pathoanatomy and examination of TMD. Part 2 describes conservative management for TMD based on examination findings.
Research Informed Management
Clinicians often turn to systematic reviews and meta-analyses for definitive answers on management strategies but these publications provide insufficient guidance for TMD. A recent review of TMD-based systematic reviews and meta-analyses noted that too few published studies exist and that more research is needed before establishing global interpretations of management efficacy.4 This lack of the highest level of evidence does not mean physical therapists are without evidence-informed guidance for TMD management but it does signify that managing TMD requires a mixture of both art and science.
Irritability
During management, as it was the case with the physical examination, the clinician should consider the irritability level of the patient’s symptoms. For information on this topic see part 1 of the series. Failure to properly dose any given intervention could lead to undesirable effects such as unnecessarily high levels of symptom provocation. However, failure to provide sufficiently aggressive techniques may lead to insufficiently rapid or complete recovery. Providing a professionally dosed intervention thus requires the coordination of information from the patient history, clinical examination, and intervention phases. Precise follow-up during and immediately after performing an intervention as well as at follow-up sessions can assist in verifying the appropriateness of dosage decisions so that necessary modifications can be made.
Joint Mobilization
Joint mobilization is a central component of physical therapy and works well in treating a variety of dysfunctions. Joint mobilization techniques are both impairment centered and clinician controlled. The primary mechanisms through which joint mobilization facilitates improvement are inhibition of pain, improvement of range-of-motion (ROM), and inhibition of muscle spasm.5 Additionally, recent evidence demonstrates that joint mobilization may decrease spinal excitability of nociceptive pathways, indicating a down-modulation of central sensitization.6 Improving ROM and/or symptom generation through the application of joint mobilization demonstrates that the clinician can impart benefit on the patient, improve function, and promote patient confidence in the treating clinician. This is a useful early component of the rehabilitation process.
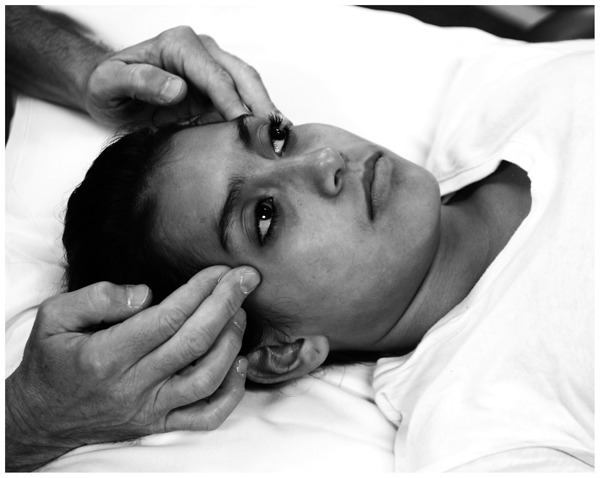
The implementation of joint mobilizations follows the same pattern as clinical examination for accessory joint restrictions, which was reviewed in part 1 of this series. Techniques of importance include distraction (Fig. 1), anterior glide (Fig. 2), anterior glide with pre-positioned mouth opening (Fig. 3), medial/lateral glides (Fig. 4), caudal-anterior-medial (CAM) glide (Fig. 5), and CAM glide with pre-positioned mouth opening (Fig. 6). Importantly, though not all shown here, each joint mobilization technique can be performed in various amounts of mouth opening or other active ranges. For an internal view of first digit placement on the mandibular teeth during certain joint mobilization techniques see Fig. 6 in part 1 of this series. Joint mobilization should be applied when a movement restriction is evident but should be avoided if joint hypermobility is suspected or verified unless a low-grade technique is utilized. It is clinically helpful to take ROM measurements and/or test symptom provocation both before and after the implementation of mobilization techniques. This test–treat–retest approach can assist in providing ongoing information about the patient’s condition and whether or not the selected intervention is appropriate and/or necessary. While many patients with TMD will require joint mobilization, hypermobility may be present in the joint so caution is advised.
Figure 1.
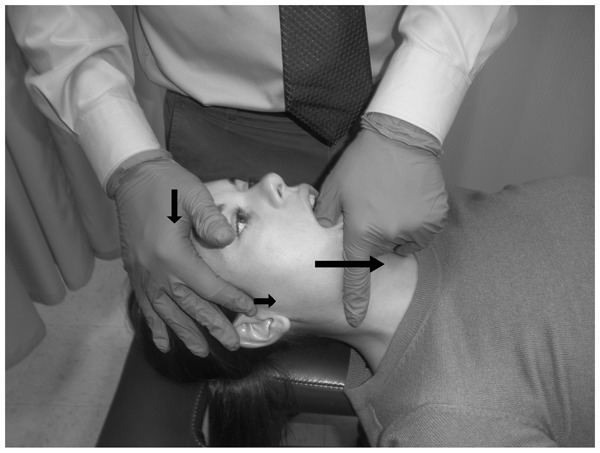
Distraction of the temporomandibular joint (TMJ); large arrow: distraction force placed through the ipsilateral lower molars and premolars with the first digit while the second and third digits provide a counterforce on the inferior aspect of the ipsilateral and contralateral mandibular bodies, respectively; medium arrow: posteriorly directed stabilization force applied through the ipsilateral aspect of the patient’s forehead; small arrow: the examiner palpates the joint line to assess for movement of the mandibular condyle.
Figure 2.

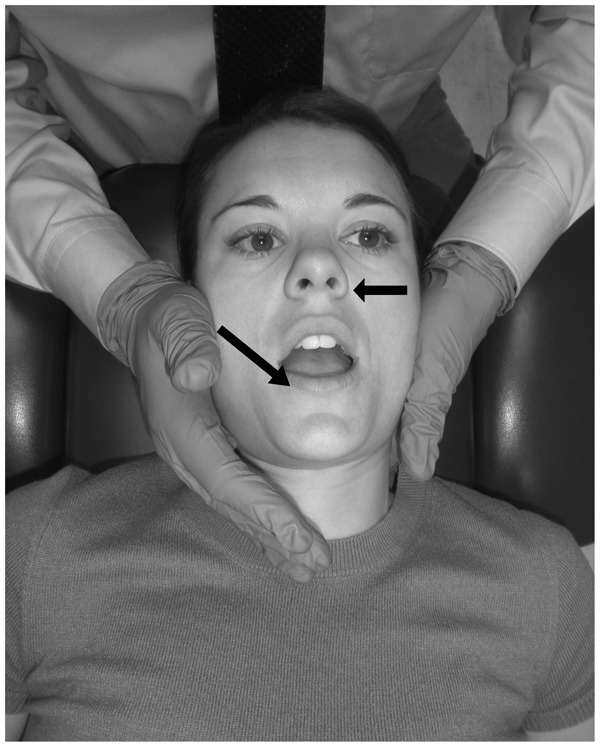
Anterior glide of the temporomandibular joint (TMJ); large arrow: anterior glide force with mild caudal bias placed through the mandible via gripping the ipsilateral lower molars and premolars with the first digit while the second and third digits provide a counterforce on the inferior aspect of the ipsilateral and contralateral mandibular bodies, respectively; medium arrow: posteriorly directed stabilization force applied through the ipsilateral aspect of the patient’s forehead; small arrow: the examiner palpates the joint line to assess for movement of the mandibular condyle.
Figure 3.

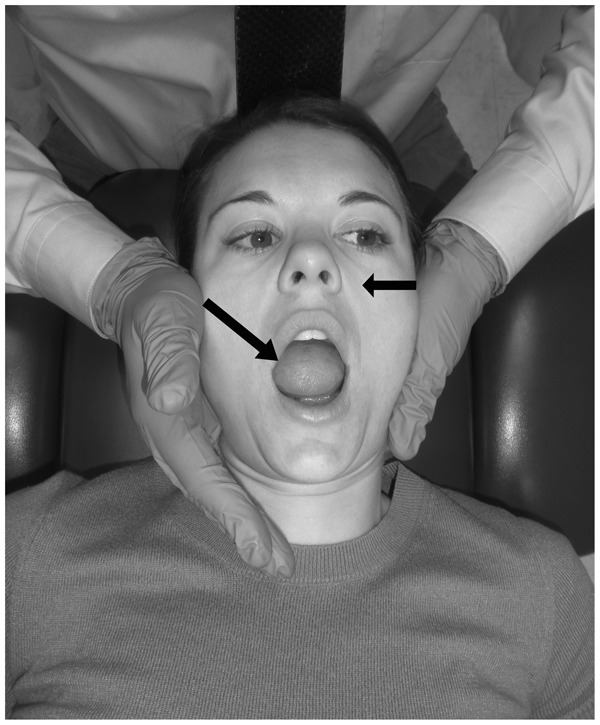
Anterior glide of the temporomandibular joint (TMJ) with pre-positioned mouth opening; large arrow: anterior-inferior glide force placed through the mandible via gripping the ipsilateral lower molars and premolars with the first digit while the second and third digits provide a counterforce on the inferior aspect of the ipsilateral and contralateral mandibular bodies, respectively; medium arrow: posteriorly directed stabilization force applied through the ipsilateral aspect of the patient’s forehead; small arrow: the examiner palpates the joint line to assess for movement of the mandibular condyle.
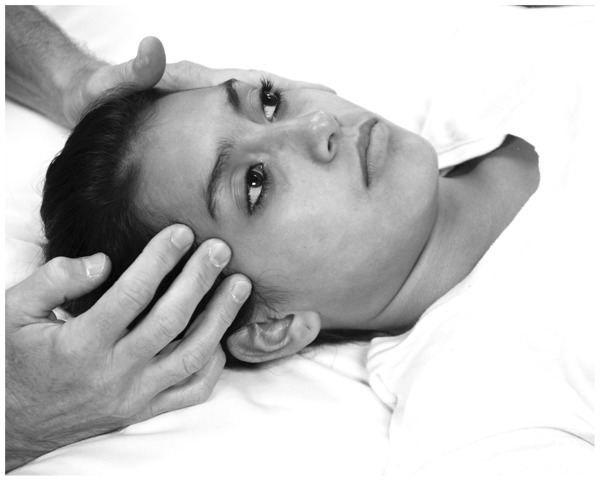
Figure 4.

Medial/lateral glide of the temporomandibular joint (TMJ); large arrow: medial glide force placed through the mandibular condyle and/or mandibular ramus; small arrow: the contralateral hand provides a stabilizing force either through the contralateral zygomatic arch of the temporal bone and/or the contralateral mandibular condyle, depending on the patient’s experience.
Figure 5.
Caudal-anterior-medial (CAM) glide of the temporomandibular joint (TMJ); large arrow: combined caudal, anterior, and medial glide force placed through the mandibular condyle and/or mandibular ramus; small arrow: the contralateral hand provides a stabilizing force either through the contralateral zygomatic arch of the temporal bone and/or the contralateral mandibular condyle, depending on the patient’s experience.
Figure 6.
Caudal-anterior-medial (CAM) glide of the temporomandibular joint (TMJ) with pre-positioned mouth opening; large arrow: medial glide force placed through the mandibular condyle and/or mandibular ramus; small arrow: the contralateral hand provides a stabilizing force either through the contralateral zygomatic arch of the temporal bone and/or the contralateral mandibular condyle, depending on the patient’s experience.
Joint mobilization dosage should be guided by an informed decision that takes into account the patient’s irritability level, the severity of the identified impairment, the chronicity of the symptom presentation, and the patient’s response rate. Assessment of tissue resistance and/or symptom provocation throughout the technique can help inform this process. There are no studies that verify the isolated usage of joint mobilizations for the management of temporomandibular joint (TMJ) restrictions. However, considerable evidence exists that supports the usage of joint mobilizations for improving joint restrictions.7–10
Additionally, self-mobilization can be useful as part of a comprehensive home program. In either sitting or supine, the patient can be instructed to mobilize one TMJ while, if necessary, stabilizing the contralateral joint. Figures 7 and 8 show positioning for self-mobilization. In the version with the mouth closed (Fig. 7), the patient’s mandibular teeth should not be in contact with the maxillary teeth. In most instances, the mobilizing and stabilizing forces should be directed through the mandibular ramus but for some patients stabilization through the zygomatic arch may be appropriate. Self-mobilization can be accomplished successfully either by teaching the patient to utilize a medially directed force or a combined approach, such as the force utilized during CAM mobilization.
Figure 7.

Self-mobilization of the temporomandibular joint (TMJ); large arrow: medial glide force placed through the mandibular condyle and/or mandibular ramus; small arrow: the contralateral hand provides a stabilizing force either through the contralateral zygomatic arch of the temporal bone and/or the contralateral mandibular condyle, depending on the patient’s experience.
Figure 8.

Self-mobilization of the temporomandibular joint (TMJ) with pre-positioned mouth opening; large arrow: medial glide force placed through the mandibular condyle and/or mandibular ramus; small arrow: the contralateral hand provides a stabilizing force either through the contralateral zygomatic arch of the temporal bone and/or the contralateral mandibular condyle, depending on the patient’s experience.
Soft Tissue Mobilization
Soft tissue mobilization is important to the management of patients with TMD because of its relevance to all TMD diagnostic classifications. However, the available evidence regarding soft tissue mobilization in patients with TMD is limited11,12 despite the fact that soft tissue mobilization has been a management component in studies utilizing multimodal approaches.13–15 Many TMD management studies completely ignore soft tissue techniques2,16,17 despite their near universal relevance. This is even the case in studies focusing on myogenous forms of TMD.18,19 Yet, due to other evidence that soft tissue mobilization is advantageous in the management of musculoskeletal disorders,20,21 these techniques should not be overlooked in the management of TMD. In each case, the clinician should determine which muscles to address based on patient-specific clinical findings. At a minimum, the temporalis, masseter, medial pterygoid, and lateral pterygoid muscles must be considered for soft tissue mobilization. Accessory muscles of mastication and cervical spine musculature may also require management through soft tissue mobilization.
When performing soft tissue mobilization, familiarity with a variety of techniques can be helpful. Utilizing one digit (Fig. 9) or one reinforced digit (Fig. 10) to contact a myofascial trigger point (MTrP) or the general muscle belly can be helpful. Utilizing multiple digits (Fig. 11) to simultaneously contact a muscle belly can be helpful as well. The application of the massage force can be accomplished utilizing a variety of techniques including friction massage or tissue techniques applied in a variety of directions. These techniques are easily applied to the masseter and temporalis muscle bellies either unilaterally with a contralateral stabilization hand to prevent inadvertent head motion (Fig. 9) or bilaterally such that a second treatment hand provides the counterforce (Fig. 10). Intraoral techniques directed at the medial (Fig. 12) and lateral pterygoid muscles are useful as well but are difficult to demonstrate based on the visual obstruction of the treating hand by perioral tissue. Additionally, stimulation of the patient’s gag reflex may prove to be an obstacle with intraoral techniques, especially with respect to the lateral pterygoid muscle.
Figure 9.
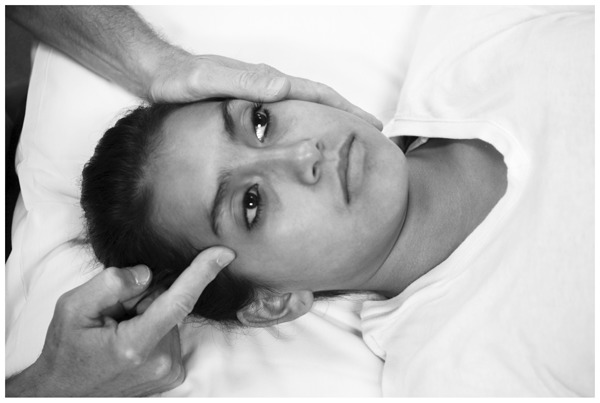
Soft tissue mobilization of the temporalis muscle utilizing one digit for contact and one hand for contralateral stabilization. Palpation of an MTrP or the general muscle belly by the tip of one digit (second digit shown) to apply soft tissue mobilization to the temporalis muscle. Switching between different digits can be helpful in prolonging technique application time before the onset of fatigue. Note that a contralateral hand provides a counterforce to stabilize the head and prevent inadvertent head motion. In this instance, the therapist begins at the anterior margin of the muscle and moves posteriorly while focusing on areas of the muscle that require treatment.
Figure 10.
Bilateral soft tissue mobilization of the temporalis muscle utilizing reinforced digits for contact. Palpation of an MTrP or the general muscle belly by the tips of the second digits with reinforcement by the third digits to apply soft tissue mobilization to the temporalis muscles. Note that both hands provide simultaneous treatment and therefore serve as both the treating and stabilizing forces. In this instance, the therapist begins at the anterior margin of the muscles and moves posteriorly.
Figure 11.
Soft tissue mobilization of the temporalis muscle utilizing three digits for contact and one hand for contralateral stabilization. Palpation of the muscle belly by the tips of three digits to apply soft tissue mobilization to the right temporalis muscle. Switching pressure and emphasis to different digits can be helpful in prolonging technique application time before the onset of fatigue. Note that the contralateral hand provides a counterforce to stabilize the head and prevent inadvertent head motion. In this instance, the therapist begins at the anterior margin of the muscle and moves posteriorly.
Figure 12.

Soft tissue mobilization of the medial pterygoid muscle. Palpation of the muscle belly by the tip of the second digit to apply soft tissue mobilization to the medial pterygoid muscle. For treatment purposes, having the patient relax so that the mouth is not opened widely can be advantageous. The open mouth position is utilized here for visualization purposes.
Trigger Point Dry Needling
When TMD associated muscle pain is related to MTrPs, trigger point dry needling should be considered for management.22 One disadvantage of this intervention is that a limited number of clinicians are sufficiently trained to implement it despite the fact that its utility was demonstrated as early as the 1970s.23 Over the years, a growing number of publications have added to our understanding of the topic. This body of evidence has shown that MTrPs can be a source of pain,24,25 that the prevalence of MTrPs, while not specifically known,26 is sufficiently high to create a need for effective management strategies,27,28 and that dry needling affects the symptom generating capabilities of MTrPs.28,29
Friction Massage
All clinicians can utilize friction massage in the management of TMD. At the cellular level, it has been demonstrated that mechanical stimulation can influence fibroblasts and other connective tissue components.30 The application of friction massage can stimulate tissues to respond such that they become stronger than untreated tissues.31 No studies have been published regarding the effectiveness of friction massage in the management of TMD, though the technique has been empirically demonstrated to be beneficial in the management of symptoms located at the lateral joint line, retrodiscal space, the temporalis insertion on the coronoid process, and over MTrPs, especially those located in the temporalis muscle.
Therapeutic Exercise
Perhaps the most widely known exercise routine for TMD is the Rocabado 6×6 program, which utilizes six exercises six times per day.32 These exercises are summarized in Table 1. Rocabado’s program has been widely utilized clinically and is present in scientific literature both as a group33 and as individual exercises.34,35 The collective 6×6 program has only been studied once for effectiveness, the results of which suggest the program adds no extra benefit to the rehabilitation process.33
Table 1. Rocabado’s 6×6 exercise program.
| Name | Exercise description/purpose |
| Rest position of the tongue | The anterior 1/3 of the tongue is placed at the palate with mild pressure, which rests the tongue and jaw musculature and promotes diaphragmatic breathing |
| Control of TMJ rotation | The jaw is repeatedly opened and closed with the anterior 1/3 of the tongue on the palate, which decreases initiating jaw movements (e.g. protrusive movement in opening, talking, or chewing) |
| Rhythmic stabilization technique | Gentle isometrics in the resting position are performed for jaw opening, closing, and lateral deviation to promote muscular relaxation via reciprocal inhibition, which promotes an improved resting position of the jaw through proprioceptive input |
| Axial extension of the neck | Combined upper cervical flexion with lower cervical extension, allowing reduction of tension in the cervical musculature |
| Shoulder posture | Shoulder girdle retraction and depression to facilitate postural corrections |
| Stabilized head flexion | Upper cervical spine distraction via chin tuck (without additional cervical flexion), during which it is recommended that the fingers be laced behind the neck to stabilize C2-7 while the head nods |
A different multiple-part approach has been proposed by Kraus.36 The first part is abbreviated TTBS because the exercises involve: tongue position at rest, teeth apart, (nasal-diaphragmatic) breathing, and swallowing. These exercises are intended to inhibit excessive masticatory muscle activity. In a later publication, Kraus removed the swallowing exercise and added wiggling, touch and bite, and strengthening exercises.37 The second part is intended to target both neuro-muscular control of mandibular movement. Part three involves isometric exercises, which are intended to address joint clicking, muscle asymmetry, deviations in active ROM patterns, and spasms that limit opening (Table 2). This collection of exercises has never been investigated as individual parts or as a whole.
Table 2. Kraus’ temporomandibular joint exercises36,37.
| Name | Exercise description/purpose |
| Tongue position at rest | The patient is instructed to maintain a resting tongue position except during function, which involves the tip of the tongue sitting on the palate with the tip resting just posterior to the upper incisors |
| Teeth apart | The patient is educated that maintaining the teeth apart can be therapeutic, which facilitates the resting tongue position |
| Nasal-diaphragmatic breathing | The patient is instructed in nasal breathing to facilitate function of the diaphragm, which reinforces positioning of both the tongue and teeth |
| Tongue up and wiggle | Patients who brace but whose teeth do not touch or grind while doing so are instructed to routinely assume the resting position and gently oscillate the mandible side-to-side to interrupt the bracing contractions. If clicking or popping occurs, intensity is decreased |
| Strengthening | Resisted closing via self manual resistance of lower incisors: 5–10-second contractions, 10 repetitions, 3–5×/day |
| Touch and bite | Proprioceptive re-education: Lateral deviation – the patient touches the contralateral maxillary canine with the fingertip (with affected right lateral deviation touch left canine) and then bites the finger, which requires lateral deviation toward the finger. Protrusion – repeat with finger touching the outer surface of maxillary incisors. |
| Neuro-muscular control | When excessive anterior movement of the mandibular condyle is noted, instruct the patient to define end range opening by placing the tip of the tongue on the anterior palate while the fingers gently palpate the chin and mandibular condyle. Repeatedly open and close to that range. Progression: incrementally remove feedback. |
| Isometric exercises | Reciprocal click: isometrics are performed immediately before the closing click. Weakness or AROM deviations not believed to be from a structural anomaly: isometrics are performed in any position. Muscle inhibition to improve ROM: agonists or antagonists can be contracted gently. |
Other more generic exercises are generally included in clinical research. However, as a result of extreme variability in study designs and patient populations, it is impossible to draw general conclusions from their findings. Many of the studies even fail to sufficiently describe exercises to the extent that a clinician could reproduce them. Additionally, most studies utilize multimodal approaches and compare outcomes of different groups when one of the management strategies is modified or removed. These studies are discussed in the Multimodal Approaches section below. Generally speaking, no evidence exists to direct clinicians toward which exercises, if any, may be useful in the conservative management of TMD. Additionally, because many, if not most, patients with TMD over-recruit their muscles of mastication, it may be more advantageous to focus on relaxation techniques and patient education than therapeutic exercise. Either way, each case should be handled individually so that management decisions regarding therapeutic exercise are patient-specific and based upon identified variables.
Patient Education
Patient education is a central component of TMD management.38–40 Each patient should receive individualized education. Primary areas of focus include reducing parafunctional habits, addressing psychosocial factors, and providing pain science education. Relevant psychosocial factors may include both anxiety and stress management. Clinicians should reasonably address these variables during treatment sessions and consider outside referral if required.
Functional habits are generally limited to caloric intake, speaking, breathing, and yawning.41 Parafunctional habits can be defined as those activities not associated with routine oral function and are generally broken down into two categories: bruxism and other parafunctional habits. Bruxism is the most common and important parafunctional habit and has been the focus of many studies. Bruxism can be divided into two primary types: awake and nocturnal bruxism.42 Nocturnal bruxism, or teeth grinding while sleeping, has been estimated to occur in 20% of the general adult population and up to two-thirds of people with TMD.43 Awake bruxism can be defined as clenching or bracing of the jaw during non-sleeping periods and generally involves awareness that it is occurring. The process is primarily associated with nervousness or stress but the physiology and pathology of awake bruxism remains largely unknown.44 Awake bruxism is not generally associated with noise production by the grinding of teeth.
Normal daily function such as mastication and yawning can play an important role as well. As a result, the clinicians should educate the patient with respect to a spectrum of variables that include food consistency, laterality of chewing, symptom behavior, and pain variables as they relate to the clinical presentation. For example, the consistency of food can affect mastication. Harder, drier foods require an increased number of chewing cycles and longer times in the mouth before swallowing.45 For this reason, some patients with TMD may require a trial period of diet modification to soften foods in an attempt to reduce symptoms.40,46 For certain patients, this period could last from weeks to months depending on symptom progression.38 If successful, the modifications should be maintained sufficiently long to assist in the rehabilitation process. In less severe cases, some harder foods may still be tolerated. Once symptoms have decreased to a manageable level, harder foods can be periodically tested for provocation and reintroduced when appropriate. Educating the patient to both observe and potentially alter any one of these factors may be associated with successfully addressing patient complaints.
Patients with hypermobility, especially in mouth opening, may require education to avoid end range positions. For example, activities such as yawning could irritate joint structures and, as a result, patients with hypermobility may require strategies to modify their routine. A generally useful technique is to teach patients not to depress their mandible farther than the position that permits the tip of the tongue to maintain contact with the hard palate just posterior to the upper incisors. Additionally, clinicians should take note of any patients that are not initially aware of the role factors such as these contribute in their presentation. Subsequent follow-up may be required because patients often do not initially recognize significant clinical contributors.
Another approach, known as cognitive behavioral therapy (CBT), is utilized for the management of chronic pain and is based on the biopsychosocial model. This approach highlights the interactions among biological, psychological, and social variables.47 Studies are mixed in their results regarding the utility of CBT in the management of TMD, though it appears to be an advantageous component of comprehensive services.48,49 As with all interventions, CBT should be tailored to each case, monitored for effectiveness, utilized only when necessary, and implemented for as long as required. For some patients this could involve a brief period whereas for others it could include permanent modifications. Some relevant exercises pertaining to patient education and relaxation techniques were previously discussed in the exercise portion and will not be revisited here.
Modalities
Electrical stimulation has been recommended for the management of TMD.38,50 Both interferential current (IFC) and transcutaneous electrical nerve stimulation (TENS) have been shown to produce an analgesic effect in pain-free volunteers provoked by ischemic conditions.51 Both IFC and TENS have been shown to elevate heat pain thresholds in pain-free subjects as well, though the post-stimulation effects of IFC last longer than those of TENS.52 In these studies, stimulation was applied for 30 minutes, which may exceed dosage times commonly utilized in clinical settings. Additionally, based on these studies, the post-stimulation effects of IFC are likely only temporary, potentially lasting as little as 30 minutes. However, research indicates that electrical stimulation of patients with acute53 and chronic pain53,54 provides a significant though short-term decrease in symptoms and tends to help more with ROM than pain when utilized for patients with TMD.55 Bearing these findings in mind, it is reasonable to augment conservative TMD management with electrical stimulation but doing so should take a secondary role and may only be necessary in patients with irritable symptoms.
Investigators have recommended the utilization of biofeedback for the management of TMD,4,38,56 during which surface electrodes are typically placed either unilaterally or bilaterally over the masseter muscle. The anterior temporalis can sometimes be targeted as well, though the majority of the muscle belly is generally inaccessible for electrode placement. A variety of biofeedback techniques have been implemented including: muscle tension discrimination to increase perception of contractions (e.g. comparing involved vs uninvolved musculature), training progressively lower levels of muscle tension to obtain maximal relaxation, deactivation training to promote rapid recovery from contraction, and home practice to ensure carry-over to activities of daily living.57
A literature review analyzed six controlled trials and found that biofeedback was superior to both no intervention and placebo intervention in five of the six studies. Roughly 70% of the patients studied experienced significant improvement in the biofeedback group whereas only 35% did in the control groups.57 It is therefore advisable to attempt biofeedback training in patients with TMD who present with altered muscular activation, which is likely to be the majority of conservatively managed patients with TMD.
Iontophoresis with dexamethasone has been recommended for use in the management of TMD.59–61 However, the evidence supporting this management approach is mixed. Basic scientific studies have shown that iontophoresis can deliver dexamethasone between eight and 17 mm deep62,63 and that long duration (3 hours) application via low current is more effective than more traditional delivery by higher currents over 10–30 minutes.63 Other studies have failed to demonstrate adequate absorption of dexamethasone.64,65 A plausible explanation for these discrepancies is that dexamethasone is not equally absorbed by all patients.66 However, in the clinical setting there is no way of determining which patients are likely to benefit from the application of iontophoresis with dexamethasone. For this reason, whenever iontophoresis is utilized, patients should be monitored for changes in their clinical presentation and the modality continued only as long as it appears beneficial.
One study found that after an average of eight sessions with dexamethasone, patients with juvenile idiopathic arthritis of the TMJ demonstrated improvements in both ROM and function. Pain did not improve and side effects ranged from transient erythema (86%) to metallic taste (4%) and blistering (4%).67 Another study found that dexamethasone applied to the TMJ can help improve function but does not reduce pain.68 Other investigations have shown that iontophoresis with dexamethasone is no more effective than a saline placebo in providing pain relief for patients with TMD.69 As a result, there is currently insufficient evidence to fully support or refute the utilization of iontophoresis with dexamethasone as a component of multimodal TMD management. Decisions regarding dexamethasone should therefore be made on a case-by-case basis.
Therapeutic ultrasound has been recommended for the management of TMD.38,39,50 However, despite the ubiquity of ultrasound in clinical practice, there is an abundance of evidence suggesting it is not warranted. A review that analyzed 38 studies concluded there was little evidence supporting the usage of ultrasound in the management of musculoskeletal disorders.70 Other reviews have reached the same conclusion.71,72 Additionally, ultrasound machines calibrated to Food and Drug Administration standards have been shown to produce unpredictable outputs.73 As a result, therapeutic ultrasound not only appears to be of little clinical value, it is likely impossible for a clinician to provide a targeted or consistent dosage even when equipment is calibrated to industry standards. For this reason, ultrasound it is not recommended for the management of TMD.
Oral Splints
Dentists commonly prescribe and fabricate a variety of oral splints for patients with TMD.74 Oral splints come in a variety of different materials and styles. One fabrication method involves obtaining impressions of the upper and lower teeth to make a custom splint. Others do not cover the teeth at all. Generally, splints are worn only while sleeping to protect the teeth, decrease nighttime bruxism, and/or reduce TMD symptoms.75 While it is not specifically the responsibility of clinicians such as physical therapists to participate in this process, it can be beneficial to both the patient and therapist if they are at least minimally aware of the relevant evidence.
Certain investigators have provided support for the usage of oral splints in the management of TMD.76,77 One proposed mechanism for the improvement of symptoms is a reduction in muscle activity as a result of using a splint,78 though evidence supporting this phenomenon is mixed. It has been demonstrated that, while the absolute EMG values can potentially decrease with splint usage, the standard deviation of measurements is so large that data may be of little practical use.79 Despite an initial decrease in muscle activity, the effects of splint usage appear both transient and insufficiently strong to reduce sleep bruxism, which is one of the primary intensions of their utilization.80
Other investigators have concluded that despite the lack of improvement in EMG results, TMD symptoms can improve as a result of splint usage.81 The bottom line question becomes whether or not splints are helpful in alleviating TMD symptoms. In an attempt to answer this question, two systematic reviews came to similar conclusions. Each found that there is insufficient evidence either in favor of or against the usage of splints in the management of TMD.74,82 As a result, decisions regarding splints should be made on a case-by-case basis and may be limited to the topic of protecting the structural integrity of teeth.
Multimodal Approaches
A series of studies demonstrated that over a minimum of five 30-minute sessions, multimodal management of TMD including soft tissue mobilization, muscle stretching, gentle isometric tension exercises against resistance, guided opening and closing, manual joint distraction, disc/condyle mobilization, postural corrections, and relaxation techniques are helpful in reducing symptoms associated with anterior disc displacement with reduction,13 anterior disc displacement without reduction,83 TMJ osteoarthritis,14,84 and myofascial pain dysfunction of the TMJ.85
One study demonstrated that manual jaw opening exercises with 30-second hold times promote a more rapid recovery than usage of a splint, though both groups received non-steroidal anti-inflammatory medication.17 Well-rounded manual therapy approaches that include exercise have been successful at promoting relief, though evidence in this area is still limited.2,86 Multimodal management has been shown to improve mandibular function over time.16 Others have combined exercise with manual therapy, medication, and splints to demonstrate long-term relief.87 Some have shown that the relationship between TMD and cervicogenic headache could mean treating both is required for maximal benefit.88 In fact, a thorough cervical spine evaluation and relevant management are advised for all patients with TMD, though the discussion of that process is beyond the scope of this series. Overall, these studies indicate that a multimodal approach is beneficial to patients with TMD, though the variability between studies does not assist in the clinical decision making process in terms of which intervention strategies are most effective.
Cervical Spine Management
Impairments identified during cervical spine examination should be addressed with appropriate intervention strategies. Management techniques should, at a minimum, address any cervical spine range deficits, accessory movement restrictions, and altered muscle recruitment patterns, though the description of these procedures is beyond the scope of this series. Failure to provide sufficiently thorough management of cervical spine impairments in patients with TMD may lead to limiting the patient’s rehabilitation potential.
Summary
Despite the prevalence of TMD, many patients are currently left without sufficient options for care. The aim of this two-part series was to review TMD relevant pathoanatomy and present an overview of examination and management strategies focused on clinical finding and addressing underlying causes of TMD. Satisfactory results can often be achieved when management focuses on addressing identified impairments. Physical therapists are positioned well to step into the current treatment void and provide comprehensive conservative management. In addition to familiarizing themselves with the content of this series and other sources, physical therapists should seek clinical guidance from colleagues experienced in evaluating and managing TMD.
Conflict of Interest
None
References
- 1.Young B, Walker MJ, Strunce J, Boyles R. A combined treatment approach emphasizing impairment-based manual physical therapy for plantar heel pain: a case series. J Orthop Sports Phys Ther. 2004;34:725–33. doi: 10.2519/jospt.2004.34.11.725. [DOI] [PubMed] [Google Scholar]
- 2.Furto ES, Cleland JA, Whitman JM, Olson KA. Manual physical therapy interventions and exercise for patients with temporomandibular disorders. Cranio. 2006;24:283–91. doi: 10.1179/crn.2006.044. [DOI] [PubMed] [Google Scholar]
- 3.Walker MJ, Boyles RE, Young BA, Strunce JB, Garber MB, Whitman JM, et al. The effectiveness of manual physical therapy and exercise for mechanical neck pain: a randomized clinical trial. Spine. 2008;33:2371–8. doi: 10.1097/BRS.0b013e318183391e. [DOI] [PubMed] [Google Scholar]
- 4.List T, Axelsson S. Management of TMD: evidence from systematic reviews and meta-analyses. J Oral Rehabil. 2010;37:430–51. doi: 10.1111/j.1365-2842.2010.02089.x. [DOI] [PubMed] [Google Scholar]
- 5.Bialosky JE, Bishop MD, Price DD, Robinson ME, George SZ. The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Man Ther. 2009;14:531–8. doi: 10.1016/j.math.2008.09.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Courtney CA, Witte PO, Chmell SJ, Hornby TG. Heightened flexor withdrawal response in individuals with knee osteoarthritis is modulated by joint compression and joint mobilization. J Pain. 2010;11:179–85. doi: 10.1016/j.jpain.2009.07.005. [DOI] [PubMed] [Google Scholar]
- 7.Olson VL. Evaluation of joint mobilization treatment. A method. Phys Ther. 1987;67:351–6. doi: 10.1093/ptj/67.3.351. [DOI] [PubMed] [Google Scholar]
- 8.Threlkeld AJ. The effects of manual therapy on connective tissue. Phys Ther. 1992;72:893–902. doi: 10.1093/ptj/72.12.893. [DOI] [PubMed] [Google Scholar]
- 9.Michlovitz SL, Harris BA, Watkins MP. Therapy interventions for improving joint range of motion: a systematic review. J Hand Ther. 2004;17:118–31. doi: 10.1197/j.jht.2004.02.002. [DOI] [PubMed] [Google Scholar]
- 10.Bronfort G, Haas M, Evans R, Leininger B, Triano J. Effectiveness of manual therapies: the UK evidence report. Chiropr Osteopat [Internet]. 2010 [cited 2013 Jan 22];18:3. Available from: http://chiromt.com/content/18/1/3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Capellini VK, de Souza GS, de Faria CR. Massage therapy in the management of myogenic TMD: a pilot study. J Appl Oral Sci. 2006;14:21–6. doi: 10.1590/S1678-77572006000100005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Pierson MJ. Changes in temporomandibular joint dysfunction symptoms following massage therapy: a case report. Int J Ther Massage Bodywork. 2011;4:37–47. doi: 10.3822/ijtmb.v4i4.110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Nicolakis P, Erdogmus B, Kopf A, Djaber-Ansari A, Piehslinger E, Fialka-Moser V. Exercise therapy for craniomandibular disorders. Arch Phys Med Rehabil. 2000;81:1137–42. doi: 10.1053/apmr.2000.6282. [DOI] [PubMed] [Google Scholar]
- 14.Nicolakis P, Burak EC, Kollmitzer J, Kopf A, Piehslinger E, Wiesinger GF, et al. An investigation of the effectiveness of exercise and manual therapy in treating symptoms of TMJ osteoarthritis. Cranio. 2001;19:26–32. doi: 10.1080/08869634.2001.11746148. [DOI] [PubMed] [Google Scholar]
- 15.De Laat A, Stappaerts K, Papy S. Counseling and physical therapy as treatment for myofascial pain of the masticatory system. J Orofac Pain. 2003;17:42–9. [PubMed] [Google Scholar]
- 16.Bakke M, Hansdottir R. Mandibular function in patients with temporomandibular joint pain: a 3-year follow-up. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106:227–34. doi: 10.1016/j.tripleo.2007.12.034. [DOI] [PubMed] [Google Scholar]
- 17.Haketa T, Kino K, Sugisaki M, Takaoka M, Ohta T. Randomized clinical trial of treatment for TMJ disc displacement. J Dent Res. 2010;89:1259–63. doi: 10.1177/0022034510378424. [DOI] [PubMed] [Google Scholar]
- 18.Ekberg E, Vallon D, Nilner M. The efficacy of appliance therapy in patients with temporomandibular disorders of mainly myogenous origin. A randomized, controlled, short-term trial. J Orofac Pain. 2003;17:133–9. [PubMed] [Google Scholar]
- 19.La Touche R, Fernández-de-las-Peñas C, Fernández-Carnero J, Escalante K, Angulo-Díaz-Parreño S, Paris-Alemany A, et al. The effects of manual therapy and exercise directed at the cervical spine on pain and pressure pain sensitivity in patients with myofascial temporomandibular disorders. J Oral Rehabil. 2009;36:644–52. doi: 10.1111/j.1365-2842.2009.01980.x. [DOI] [PubMed] [Google Scholar]
- 20.Kalichman L. Massage therapy for fibromyalgia symptoms. Rheumatol Int. 2010;30:1151–7. doi: 10.1007/s00296-010-1409-2. [DOI] [PubMed] [Google Scholar]
- 21.Dhanani NM, Caruso TJ, Carinci AJ. Complementary and alternative medicine for pain: an evidence-based review. Curr Pain Headache Rep. 2011;15:39–46. doi: 10.1007/s11916-010-0158-y. [DOI] [PubMed] [Google Scholar]
- 22.Dommerholt J. Dry needling – peripheral and central considerations. J Man Manip Ther. 2011;19:223–7. doi: 10.1179/106698111X13129729552065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lewit K. The needle effect in the relief of myofascial pain. Pain. 1979;6:83–90. doi: 10.1016/0304-3959(79)90142-8. [DOI] [PubMed] [Google Scholar]
- 24.Melzack R, Stillwell DM, Fox EJ. Trigger points and acupuncture points for pain: correlations and implications. Pain. 1977;3:3–23. doi: 10.1016/0304-3959(77)90032-X. [DOI] [PubMed] [Google Scholar]
- 25.Lavelle ED, Lavelle W, Smith HS. Myofascial trigger points. Anesthesiol Clin. 2007;25:841–51. doi: 10.1016/j.anclin.2007.07.003. [DOI] [PubMed] [Google Scholar]
- 26.Gerwin RD. Classification, epidemiology, and natural history of myofascial pain syndrome. Curr Pain Headache Rep. 2001;5:412–20. doi: 10.1007/s11916-001-0052-8. [DOI] [PubMed] [Google Scholar]
- 27.Skootsky SA, Jaeger B, Oye RK. Prevalence of myofascial pain in general internal medicine practice. West J Med. 1989;151:157–60. [PMC free article] [PubMed] [Google Scholar]
- 28.Srbely JZ, Dickey JP, Lee D, Lowerison M. Dry needle stimulation of myofascial trigger points evokes segmental anti-nociceptive effects. J Rehabil Med. 2010;42:463–8. doi: 10.2340/16501977-0535. [DOI] [PubMed] [Google Scholar]
- 29.Fernández-Carnero J, La Touche R, Ortega-Santiago R, Galan-del-Rio F, Pesquera J, Ge HY, et al. Short-term effects of dry needling of active myofascial trigger points in the masseter muscle in patients with temporomandibular disorders. J Orofac Pain. 2010;24:106–12. [PubMed] [Google Scholar]
- 30.Ingber DE. Cellular mechanotransduction: putting all the pieces together again. FASEB J. 2006;20:811–27. doi: 10.1096/fj.05-5424rev. [DOI] [PubMed] [Google Scholar]
- 31.Loghmani MT, Warden SJ. Instrument-assisted cross-fiber massage accelerates knee ligament healing. J Orthop Sports Phys Ther. 2009;39:506–14. doi: 10.2519/jospt.2009.2997. [DOI] [PubMed] [Google Scholar]
- 32.Rocabado M, Iglarsh ZA.Musculoskeletal approach to maxillofacial pain Philadelphia, PA: JB Lippincott; 1991. p. 187–92. [Google Scholar]
- 33.Mulet M, Decker KL, Look JO, Lenton PA, Schiffman EL. A randomized clinical trial assessing the efficacy of adding 6×6 exercises to self-care for the treatment of masticatory myofascial pain. J Orofac Pain. 2007;21:318–28. [PubMed] [Google Scholar]
- 34.Magnusson T, Syrén M. Therapeutic jaw exercises and interocclusal appliance therapy. A comparison between two common treatments of temporomandibular disorders. Swed Dent J. 1999;23:27–37. [PubMed] [Google Scholar]
- 35.Wright EF, Domenech MA, Fischer JR., Jr Usefulness of posture training for patients with temporomandibular disorders. J Am Dent Assoc. 2000;131:202–10. doi: 10.14219/jada.archive.2000.0148. [DOI] [PubMed] [Google Scholar]
- 36.Kraus SL.Management of the craniomandibular complex New York: Churchill Livingstone; 1988. p. 139–74. [Google Scholar]
- 37.Kraus SL.Temporomandibular Disorders In: Saunders HD, Ryan RS editors. Evaluation, treatment and prevention of musculoskeletal disorders volume 1 spine, 4th ednChaska, MN: The Saunders Group; 2004. p. 173–210. [Google Scholar]
- 38.Friction J. Myogenous temporomandibular disorders: diagnostic and management considerations. Dent Clin North Am. 2007;51:61–83. doi: 10.1016/j.cden.2006.10.002. [DOI] [PubMed] [Google Scholar]
- 39.Wright EF, North SL. Management and treatment of temporomandibular disorders: a clinical perspective. J Man Manip Ther. 2009;17:247–54. doi: 10.1179/106698109791352184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Dym H, Israel H. Diagnosis and treatment of temporomandibular disorders. Dent Clin North Am [Internet]. 2012 [cited 2013 Jan 22];56:149–61. Available from: http://www.sciencedirect.com/science/article/pii/S0011853211001236. [DOI] [PubMed] [Google Scholar]
- 41.Benoliel R, Svensson P, Heir GM, Sirois D, Zakrzewska J, Oke-Nwosu J, et al. Persistent orofacial muscle pain. Oral Dis. 2011;17:23–41. doi: 10.1111/j.1601-0825.2011.01790.x. [DOI] [PubMed] [Google Scholar]
- 42.Lobbezoo F, Naeije M. Bruxism is mainly regulated centrally, not peripherally. J Oral Rehabil. 2001;28:1085–91. doi: 10.1046/j.1365-2842.2001.00839.x. [DOI] [PubMed] [Google Scholar]
- 43.De Laat A, Macaluso GM. Sleep bruxism is a motor disorder. Mov Disord. 2002;17:S67–69. doi: 10.1002/mds.10064. [DOI] [PubMed] [Google Scholar]
- 44.Lavigne GJ, Khoury S, Abe S, Yamaguchi T, Raphael K. Bruxism physiology and pathology: an overview for clinicians. J Oral Rehabil. 2008;35:476–94. doi: 10.1111/j.1365-2842.2008.01881.x. [DOI] [PubMed] [Google Scholar]
- 45.Pereira LJ, Duarte Gaviao MB, Van Der Bilt A. Influence of oral characteristics and food products on masticatory function. Acta Odontol Scand. 2006;64:193–201. doi: 10.1080/00016350600703459. [DOI] [PubMed] [Google Scholar]
- 46.de Souza RF, Lovato da Silva CH, Nasser M, Fedorowicz Z, Al-Muharraqi MA. Interventions for the management of temporomandibular joint osteoarthritis. Cochrane Database Syst Rev [Internet]. 2012 [cited 2013 Jan 22];4:CD007261. Available from: http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD007261.pub2/abstract. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Day MA, Thorn BE, Kapoor S. A qualitative analysis of a randomized controlled trial comparing a cognitive-behavioral treatment with education. J Pain. 2011;12:941–52. doi: 10.1016/j.jpain.2011.02.354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Orlando B, Manfredini D, Salvetti G, Bosco M. Evaluation of the effectiveness of biobehavioral therapy in the treatment of temporomandibular disorders: a literature review. Behav Med. 2007;33:101–18. doi: 10.3200/BMED.33.3.101-118. [DOI] [PubMed] [Google Scholar]
- 49.Aggarwal VR, Tickle M, Javidi H, Peters S. Reviewing the evidence: can cognitive behavioral therapy improve outcomes for patients with chronic orofacial pain? J Orofac Pain. 2010;24:163–71. [PubMed] [Google Scholar]
- 50.Kraus S. Temporomandibular disorders, head and orofacial pain: cervical spine considerations. Dent Clin North Am. 2007;51:161–93. doi: 10.1016/j.cden.2006.10.001. [DOI] [PubMed] [Google Scholar]
- 51.Johnson MI, Tabasam G. An investigation into the analgesic effects of interferential currents and transcutaneous electrical nerve stimulation on experimentally induced ischemic pain in otherwise pain-free volunteers. Phys Ther. 2003;83:208–23. [PubMed] [Google Scholar]
- 52.Cheing GL, Hui-Chan CW. Analgesic effects of transcutaneous electrical nerve stimulation and interferential currents on heat pain in healthy subjects. J Rehabil Med. 2003;35:15–9. doi: 10.1080/16501970306101. [DOI] [PubMed] [Google Scholar]
- 53.Fuentes JP, Armijo Olivo S, Magee DJ, Gross DP. Effectiveness of interferential current therapy in the management of musculoskeletal pain: a systematic review and meta-analysis. Phys Ther. 2010;90:1219–38. doi: 10.2522/ptj.20090335. [DOI] [PubMed] [Google Scholar]
- 54.Johnson M, Martinson M. Efficacy of electrical nerve stimulation for chronic musculoskeletal pain: a meta-analysis of randomized controlled trials. Pain. 2007;130:157–65. doi: 10.1016/j.pain.2007.02.007. [DOI] [PubMed] [Google Scholar]
- 55.McNeely ML, Armijo Olivo S, Magee DJ. A systematic review of the effectiveness of physical therapy interventions for temporomandibular disorders. Phys Ther. 2006;86:710–25. [PubMed] [Google Scholar]
- 56.Goldstein BH. Temporomandibular disorders: a review of current understanding. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:379–85. doi: 10.1016/s1079-2104(99)70048-x. [DOI] [PubMed] [Google Scholar]
- 57.Crider A, Glaros AG, Gevirtz RN. Efficacy of biofeedback-based treatments for temporomandibular disorders. Appl Psychophysiol Biofeedback. 2005;30:333–45. doi: 10.1007/s10484-005-8420-5. [DOI] [PubMed] [Google Scholar]
- 58.Crider AB, Glaros AG. A meta-analysis of EMG biofeedback treatment of temporomandibular disorders. J Orofac Pain. 1999;13:29–37. [PubMed] [Google Scholar]
- 59.DuPont JS., Jr Clinical use of iontophoresis to treat facial pain. Cranio. 2004;22:297–303. doi: 10.1179/crn.2004.037. [DOI] [PubMed] [Google Scholar]
- 60.Cameron MH. Fighting inflammation. Rehab Manag. 2005;18(6):26–8. [PubMed] [Google Scholar]
- 61.Buescher JJ. Temporomandibular joint disorders. Am Fam Physician. 2007;76:1477–82. [PubMed] [Google Scholar]
- 62.Glass JM, Stephen RL, Jacobson SC. The quantity and distribution of radiolabeled dexamethasone delivered to tissue by iontophoresis. Int J Dermatol. 1980;19:519–25. doi: 10.1111/j.1365-4362.1980.tb00380.x. [DOI] [PubMed] [Google Scholar]
- 63.Anderson CR, Morris RL, Boeh SD, Panus PC, Sembrowich WL. Effects of iontophoresis current magnitude and duration on dexamethasone deposition and localized drug retention. Phys Ther. 2003;83:161–70. [PubMed] [Google Scholar]
- 64.Blackford J, Doherty TJ, Ferslew KE, Panus PC. Iontophoresis of dexamethasone-phosphate into the equine tibiotarsal joint. J Vet Pharmacol Ther. 2000;23:229–36. [PubMed] [Google Scholar]
- 65.Smutok MA, Mayo MF, Gabaree CL, Ferslew KE, Panus PC. Cathodic iontophoresis of dexamethasone-phosphate in human volunteers. J Orthop Sports Phys Ther. 2002;32:461–8. doi: 10.2519/jospt.2002.32.9.461. [DOI] [PubMed] [Google Scholar]
- 66.Gurney AB, Wascher DC. Absorption of dexamethasone sodium phosphate in human connective tissue using iontophoresis. Am J Sports Med. 2008;36:753–9. doi: 10.1177/0363546507311597. [DOI] [PubMed] [Google Scholar]
- 67.Mina R, Melson P, Powell S, Rao M, Hinze C, Passo M, et al. Effectiveness of dexamethasone iontophoresis for temporomandibular joint involvement in juvenile idiopathic arthritis. Arthritis Care Res (Hoboken). 2011;63:1511–6. doi: 10.1002/acr.20600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Schiffman EL, Braun BL, Lindgren BR. Temporomandibular joint iontophoresis: a double-blind randomized clinical trial. J Orofac Pain. 1996;10:157–65. [PubMed] [Google Scholar]
- 69.Reid KI, Dionne RA, Sicard-Rosenbaum L, Lord D, Dubner RA. Evaluation of iontophoretically applied dexamethasone for painful pathologic temporomandibular joints. Oral Surg Oral Med Oral Pathol. 1994;77:605–9. doi: 10.1016/0030-4220(94)90319-0. [DOI] [PubMed] [Google Scholar]
- 70.van der Windt DA, van der Heijden GJ, van den Berg SG, ter Riet G, de Winter AF, Bouter LM. Ultrasound therapy for musculoskeletal disorders: a systematic review. Pain. 1999;81:257–71. doi: 10.1016/S0304-3959(99)00016-0. [DOI] [PubMed] [Google Scholar]
- 71.Robertson VJ, Baker KG. A review of therapeutic ultrasound: effectiveness studies. Phys Ther. 2001;81:1339–50. [PubMed] [Google Scholar]
- 72.Shanks P, Curran M, Fletcher P, Thompson R. The effectiveness of therapeutic ultrasound for musculoskeletal conditions of the lower limb: a literature review. Foot (Edinb). 2010;20:133–9. doi: 10.1016/j.foot.2010.09.006. [DOI] [PubMed] [Google Scholar]
- 73.Straub SJ, Johns LD, Howard SM. Variability in effective radiating area at 1 MHz affects ultrasound treatment intensity. Phys Ther. 2008;88:50–7. doi: 10.2522/ptj.20060358. [DOI] [PubMed] [Google Scholar]
- 74.Gray RJ, Davies SJ. Occlusal splints and temporomandibular disorders: why, when, how? Dent Update. 2001;28:194–9. doi: 10.12968/denu.2001.28.4.194. [DOI] [PubMed] [Google Scholar]
- 75.Al-Ani MZ, Davies SJ, Gray RJ, Sloan P, Glenny AM.Stabilisation splint therapy for temporomandibular pain dysfunction syndrome. Cochrane Database Syst Rev [Internet]. 2004 [cited 2013 Jan 22];CD002778. Available from http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD002778.pub2/abstract [DOI] [PubMed] [Google Scholar]
- 76.Tsuga K, Akagawa Y, Sakaguchi R, Tsuru H. A short-term evaluation of the effectiveness of stabilisation therapy for specific symptoms of temporomandibular joint dysfunction syndrome. J Prosthet Dent. 1989;61:610–3. doi: 10.1016/0022-3913(89)90286-2. [DOI] [PubMed] [Google Scholar]
- 77.Davies SJ, Gray RJ. The pattern of splint usage in the management of two common temporomandibular disorders. Part II: the stabilisation splint in the treatment of pain dysfunction syndrome. Br Dent J. 1997;183:247–51. doi: 10.1038/sj.bdj.4809478. [DOI] [PubMed] [Google Scholar]
- 78.Landulpho AB, e Silva WA, e Silva FA, Vitti M. The effect of the occlusal splints on the treatment of temporomandibular disorders – a computerized electromyographic study of masseter and anterior temporalis muscles. Electromyogr Clin Neurophysiol. 2002;42:187–91. [PubMed] [Google Scholar]
- 79.Shi CS, Wang HY. Influence of an occlusal splint on integrated electromyography of the masseter muscles. J Oral Rehabil. 1991;18:253–6. doi: 10.1111/j.1365-2842.1991.tb00054.x. [DOI] [PubMed] [Google Scholar]
- 80.Harada T, Ichiki R, Tsukiyama Y, Koyano K. The effect of oral splint devices on sleep bruxism: a 6-week observation with an ambulatory electromyographic recording device. J Oral Rehabil. 2006;33:482–8. doi: 10.1111/j.1365-2842.2005.01576.x. [DOI] [PubMed] [Google Scholar]
- 81.Nascimento LL, Amorim CF, Giannasi LC, Oliveira CS, Nacif SR, Silva Ade M, et al. Occlusal splint for sleep bruxism: an electromyographic associated to Helkimo Index evaluation. Sleep Breath. 2008;12:275–80. doi: 10.1007/s11325-007-0152-8. [DOI] [PubMed] [Google Scholar]
- 82.Türp JC, Komine F, Hugger A. Efficacy of stabilization splints for the management of patients with masticatory muscle pain: a qualitative systematic review. Clin Oral Investig. 2004;8:179–95. doi: 10.1007/s00784-004-0265-4. [DOI] [PubMed] [Google Scholar]
- 83.Nicolakis P, Erdogmus B, Kopf A, Ebenbirchler G, Kollmitzer J, Piehslinger E, et al. Effectiveness of exercise therapy in patients with internal derangement of the temporomandibular joint. J Oral Rehabil. 2001;28:1158–64. doi: 10.1046/j.1365-2842.2001.00784.x. [DOI] [PubMed] [Google Scholar]
- 84.Nicolakis P, Erdogmus CB, Kollmitzer J, Kerschan-Schindi K, Sengstbrati M, Nuhr M, et al. Long-term outcome after treatment of temporomandibular joint osteoarthritis with exercise and manual therapy. Cranio. 2002;20:23–7. doi: 10.1080/08869634.2002.11746186. [DOI] [PubMed] [Google Scholar]
- 85.Nicolakis P, Erdogmus B, Kopf A, Nicolakis M, Piehslinger E, Fialka-Moser V. Effectiveness of exercise therapy in patients with myofascial pain dysfunction syndrome. J Oral Rehabil. 2002;29:362–8. doi: 10.1046/j.1365-2842.2002.00859.x. [DOI] [PubMed] [Google Scholar]
- 86.Cleland J, Palmer J. Effectiveness of manual physical therapy, therapeutic exercise, and patient education on bilateral disc displacement without reduction of the temporomandibular joint: a single-case design. J Orthop Sports Phys Ther. 2004;34:535–48. doi: 10.2519/jospt.2004.34.9.535. [DOI] [PubMed] [Google Scholar]
- 87.Murakami K, Kaneshita S, Kanoh C, Yamamura I. Ten-year outcome of nonsurgical treatment for the internal derangement of the temporomandibular joint with closed lock. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94:572–5. doi: 10.1067/moe.2002.126891. [DOI] [PubMed] [Google Scholar]
- 88.von Piekartz H, Lüdtke K. Effect of treatment of temporomandibular disorders (TMD) in patients with cervicogenic headache: a single-blind, randomized controlled study. Cranio. 2011;29:43–56. doi: 10.1179/crn.2011.008. [DOI] [PubMed] [Google Scholar]