

Abstract
Objective
To evaluate the impact of power assist wheels (PAWs) on the distance traveled by manual wheelchair users and analyze potential cofactors in the magnitude of response: To test the hypothesis that wheelers would travel significantly further with PAWs.
Design
A 16-week A (Pre-intervention)-B (Intervention)- A (Post-intervention) repeated measures design. Seven women and 13 men (age 43±15 years) full-time wheelers participated. During the pre-intervention and post-intervention phases (4 weeks each), participants used their own unaltered manual wheelchairs. During the 8-week intervention phase, the manual wheels were replaced with PAWs. Daily distance was measured with bicycle-style odometers. A composite score of laboratory wheelchair tasks was used to classify wheelchair performance. Mixed model repeated measures analysis of variance analyzed changes across phases of the trial. A post-hoc analysis tabulated the amount of days wheelers exceeded their individual daily averages in each phase by two standard deviations.
Results
Wheelers traveled significantly greater distances during the intervention phase compared to pre- or post-intervention phases regardless of baseline wheelchair performance . Wheelers who demonstrated higher baseline wheelchair performance traveled lesser average distances in the first two weeks after receiving PAWs than in the subsequent 6 weeks. Wheelers exceeded their individual daily averages per phase on a significantly greater number of days during the intervention phase.
Conclusions
PAWs enabled wheelers to travel farther and to travel beyond their usual distances on more days. Future studies may be strengthened by taking into account the two-week “adjustment phase” for PAWs.
Keywords: Pushrim-Activated Power Assist Wheelchairs, Wheelchair, Mobility, Disability
Until recently, there were essentially two systems of seated wheeled mobility: conventional manual wheelchairs that relied solely on the user or helper to propel the chair and power mobility (both wheelchairs and scooters) using motors to drive the wheels. Manual wheelchairs are relatively lightweight (typically 17-40 lbs for an adult), easy to manipulate, and can be transported in most vehicles without special adaptations. Yet by relying solely on the user's own physical power, many environments are not practically accessible. Carpets, rough terrain and even small inclines or slopes increase the effort and energy cost of mobility.1-4 A growing body of evidence suggests that the repetitive stress of manual wheeling has serious negative consequences.5-9 Cooper et al. concluded that manual wheelchair users are particularly susceptible to a variety of bone, joint, and repetitive motion injuries that may not have time to adequately heal when manual wheelchairs are the primary mode of mobility.8 Boninger et al. recommended that peak forces imposed on the upper limb during wheeling and push frequency be minimized in order to prevent or forestall the injury related to long term wheelchair use. 5
Power mobility demands very little of the user's strength and endurance, but this may not be desirable in all instances. 10 Physical inactivity appears to occur disproportionately among those with disabilities, contributing to obesity and a cycle of deconditioning and further decline. 8 Further limitations of power mobility include the weight of the devices (typically 150 lbs or greater) and difficulty in transporting the devices10, 11. Often, expensive vehicle modifications and mechanical lifts are required.
To address the limitations of conventional manual and power mobility, a third option has emerged, power-assist wheels (PAWs). When PAWs are attached to a manual wheelchair or in systems where the PAW is integral to the wheelchair, the term pushrim-activated power assist wheelchair (PAPAW) is often used. PAWs require users to stroke the pushrims to activate small, lightweight motors that drive the wheels for a brief period of time (seconds). To keep PAWs moving, users must continue to stroke the pushrim as they would if they were propelling a conventional manual chair. Compared to manual wheeling, use of PAWs requires less user strength and endurance to propel which is especially beneficial on inclines, uneven terrain, and carpeted surfaces.11,13,14 Compared to conventional power wheelchairs, PAWs are lighter and thus likely to be easier to transport.11 Laboratory studies have demonstrated that PAWs require less effort and energy compared to conventional manual mobility, as manifested by lower heart rate, less activation from upper limb and trunk muscles, reduced stroke frequency and range of motion, less perceived exertion, and less oxygen consumption. 11,13-18 It should be noted that PAPAWs are heavier than comparable manual wheelchairs, and thus more challenging to transport, and may not be as intuitive to propel. They are also more expensive than comparable manual wheelchairs, and require recharging and battery maintenance. Despite the apparent utility of PAWs, little is known about their actual impact on users' daily life experiences and events. Although there are many dimensions of enablement, it is appealing to use distance travelled as a primary outcome to measure the impact of PAWs on users' lives since the central purpose of wheeled mobility devices is to facilitate travel. In other words, a key question is whether wheelers travel farther when given an opportunity to use PAWs than when in their own conventional wheelchairs.
Except differences in participant sample, Fitzgerald el al (7 manual wheelers with paraplegia) and Ding et al (15 with tetraplegia) used similar methodology to investigate the impact of PAPAWs in wheelers' every-day lives. 19,20 Both studies employed a cross-over design with subjects acting as their own controls. During the 2-week baseline phase, wheelers' activity in their own manual wheelchairs was monitored with both a data logger and survey instruments. This was compared to the 2-week intervention phase, where users were given a Yamaha JWII PAPAW which was selected to be similar to the users' own chairs. During the experimental phase, the users were free to use either their own chair or the PAPAW.
Results of these 2 studies showed that users chose to use the PAPAWs and their personal wheelchairs at similar frequency during the PAPAW phase of the trial. The distances travelled were not significantly different between the PAPAW and manual chairs, although the participants travelled more quickly in the PAPAWs. The PAPAWs did not result in significantly greater community participation, satisfaction, or psychological impact compared to users' own manual wheelchairs.
Limitations to these studies acknowledged by the authors included a small sample size and the two-week time frame for each phase, which may not have been adequate to detect the effects of the intervention. The authors suggested that future studies should include larger, more diverse samples and measurements collected over longer periods of time.
With this in mind, we decided to investigate the impact of power assist wheels over 16-weeks and tested the following hypotheses:
Wheelers would travel significantly farther during the intervention phase than the baseline or follow-up periods.
Baseline wheelchair performance would not predict the response to the intervention.
Those with worse hand function would have more trouble controlling the PAWs, and therefore would see a significantly smaller change of distance in the intervention compared to baseline and follow-up than those with more normal hand function.
The distance travelled during the first two weeks after receiving the PAWS would be significantly less than in the following 6 weeks since wheelers would need a period to adjust to the PAWs.
The most functional wheelers (those with the highest ability to wheel in a test of wheelchair performance) would show the most difficulty adjusting, since their current manual wheelchair use was more likely to be satisfactory.
Methods
Design
This was part of a larger study to investigate the impact of PAWs on quality of life, participation, and psycho-social processes. A more detailed explanation of the study design has been reported elsewhere and will be briefly reviewed here. 21 The study was a 16-week A-Pre-intervention, B-Intervention, A-Post-Intervention repeated measures design with participants serving as their own controls. Participants propelled their own manual wheelchairs during an initial baseline period (4 weeks). This was followed by an 8-week intervention period where subjects used the PAWs, and then a 4-week post-intervention period, where participants returned to their own manual wheelchairs. All aspects of this project were approved in advanced by appropriate university institutional board and were conducted in accord with the Declaration of the World Medical Association.
Design Consideration 1) Choice of PAW
At the time of our study, there were two power assist systems available in the United States, the Yamaha JWII system (Yamaha Motor Corporation, Shizuoka, Japan) which is marketed as the Quickie Xtendertm (Sunrise Medical, Longmont, Colorado) in the U.S., and the Alber E.motion M-12 power assist wheels (Alber, Albstadt, Germany) marketed by Frank Mobility Systems in the U.S. (Oakdale, Pennsylvania). The Xtender is only available on selected Quickie wheelchairs, while the E.motion wheels can be attached to most existing manual wheelchairs with the addition of small mounting brackets. By choosing the E.motion wheels, we were able to allow users to stay in their own wheelchairs in different phases of the study, only exchanging the conventional manual wheels for PAWs in the intervention phase. This eliminated the potential confound of different wheelchairs in different phases. The E.motion wheels and batteries together added a total of 53 pounds (22 kg) to the users' wheelchairs and approximately 6 cm to the total width.
Design Consideration 2) Choice to Use Only the PAW during the Intervention Phase Rather Than Allowing Use of both Paws and Manual Wheels
This study was influenced by current U.S. Medicare policy which allows for reimbursement for one wheeled mobility device every five years (although some exceptions are permitted under special circumstances). This typically forces clinicians and wheelers to choose either a PAPAW or a manual wheelchair. In order to mimic patient and clinician choices, our design did not allow the use of the PAWs and manual wheels during the same phase of the trial. As a result, the design differed form that of Fitzgerald el al and Ding et al. 19,20
Design Consideration 3) Lengths of the Different Phases
At the time of the study, there was no set standard to determine the duration of each phase. Because only medically stable, experienced wheelers were recruited, it was expected that manual wheelchair performance would be relatively stable, and thus an initial four week period would be sufficient. In contrast, none of our participants had experience using PAWs. There was a question of how wheelers might react to receiving the PAWs. It was possible that some users might be either enthralled by or resistant to the new technology. We thought the longer 8 week intervention phase would be adequate to allow full adjustment to the PAWs.
Participants
Inclusion/exclusion criteria: To determine eligibility, participants were evaluated by the primary author, a physiatrist who gathered a medical and social history and examined the status of each participant's central and peripheral nervous systems, musculoskeletal system, cardiovascular system and pulmonary system. Individuals were excluded if they were judged to be cognitively impaired to the extent that cooperation with the study protocol might be compromised. In order to be eligible to enroll, potential participants must have been full-time wheelers who were medically and functionally stable, and at least 4 months post-injury/disorder, and without expectation of significant further recovery or loss of abilities during the study period, as based on the natural history of the injury/disorder. Wheelers were ≥ 18 years of age and able to propel their own wheelchairs independently with their upper limbs, and could not exceed 225lbs (the weight capacity of the E.motion wheels). Participants were required to demonstrate that their wheelchairs fitted with PAWs could be loaded into their usual mode of transportation. If the participant was accustomed to loading his or her own wheelchair independently, then he or she was required to do the same with the wheelchair fitted with PAWs. If the person relied on a helper to transport the chair, then the helper had to be able to transport the wheelchair equipped with PAWs; each participant received a total of $400 to compensate for their time, travel, and active participation in the study, in the form of monthly checks. Those who did not complete the study were paid a pro-rated amount proportional to their duration of participation.
Participant flow is described in Figure 1. Twenty-six individuals were recruited to participate in the study via advertisements in local newspapers and fliers placed in rehabilitation facilities and regional wheelchair sports/recreational events. One individual was initially excluded at the initial laboratory assessment when it became clear that he exceeded the weight limit of PAWs. Five other individuals were secondarily excluded during the baseline monitoring phase due to unwillingness to follow-up, complications of chronic diabetes causing frequent hospitalizations, and unwillingness to keep up with the demands to collect and transmit data as required by the study. Data from these participants were incomplete, and thus were not included in the analyses. Thus the final sample consisted of 8 women and 12 men (M age = 43.1 years, SD = 14.5, M time since injury = 17.8 years, SD = 9.4) The primary diagnoses were 5 cervical spinal cord injuries, 7 thoracic spinal cord injuries, 2 lumbar spinal cord injuries as well as 1 individual with juvenile diabetes and a trans-tibial amputation, 1 individual with sepis of the knee and avascular necrosis of the hip, 2 individuals with multiple schlerosis, one with transverse myelitis, and one whose diagnosis was undetermined. A table with more demographic information is provided by Giacobbi et al21Appropriate permissions were granted from local institutional review boards, and all subjects gave their informed consent in writing before inclusion.
Figure 1. Participant flow.

Wheelchair Set Up: Each Wheelchair was fitted with special brackets (supplied by Frank Mobility) near the rear to allow attachment of the PAWs. A pair of commercially available bicycle computers (Cat Eye VDO Cytec C15, North America Cat Eye, Boulder, CO) was fitted to each chair. These devices used a magnet placed on each wheel and a corresponding sensor attached to the frame to monitor the number of revolutions completed by the wheel. Similar magnetic technology has been used in previous studies.22-4The distance traveled in kilometers was then calculated based on a calibration value relative to the diameter of the wheel. Participants recorded their daily distances by entering the value provided by the odometers into a daily log. The data from right and left wheels were averaged and used in subsequent analyses unless one of the units malfunctioned or was damaged. In that case, the data from the remaining unit were used. The logs were collected by staff members each week. In addition, participants emailed their data from each wheel to the investigators on a daily or weekly basis. Those without email access were contacted by telephone. Except in instances when there was obvious damage or malfunction, distances recorded by the left and right odometers showed very little difference.
Measures of Physical Function
The presence or absence of a movement disorder in the hands was assessed using 4 items of the Unified Parkinson's Disease Rating Scale (UPDRS) motor examination subscales with a total value ranging from 0-16.25,26 The items were “Handwriting,” “Fingertaps,” “Hand Movements,” (the subject opens and closes his or her hands in rapid succession with widest amplitude possible), and “Rapid Alternating Movements of the Hand” (the subject performs pronation-supination movements of hands vertically or horizontally, with as large an amplitude as possible, both hands simultaneously). The UPDRS depends on the rater's judgment of the participant's performance using a Likert Scale. A rating of 0 generally corresponds with no impairment, 1 = mild impairment, 2 = moderate impairment, 3 = severe impairment, while 4 generally corresponds to an inability to complete the task in a meaningful manner. The UPDRS items were chosen as a rapid method to characterize hand function, not to assess specifically for Parkinsin's Disease (although abnormal test performance of one individual with spinal cord injury ultimately led the participant to seek a neurological evaluation which confirmed Parkinson's Disease).
Wheelchair performance was assessed by the times to complete the following laboratory tasks in their own wheelchairs at a self-selected free speed: 1) Level propulsion over a flat surface for a distance of 100 m – four lengths of 25 m with three 180° turns around a traffic cone2) A 40 m level propulsion task without turns over a flat surface; 3) Level propulsion over a thick (3/4”) polyester carpet for a distance of 21 m – three lengths of 7 m with two 180° turns; 4) Propulsion up and down a 6-m ramp (5° in slope) three times with 180° turns made on level surfaces at the top and bottom of the ramp. A composite variable was formed that included each of these wheelchair performance variables. This composite technique was used due to high correlations among the measures (r's = .74 to .93). The composite variable was calculated by transforming actual completion times into z-scores and summing across the tasks. The composite variable was strongly correlated with each of the individual tasks (r's = .50 to .94). ‘High’ and ‘low’ functioning subgroups were created by splitting the sample at the median because the composite was normally distributed, no meaningful cutoff was evident in the data, and splitting at the median allowed equal sample sizes in between-group analyses that were performed.
Statistical Analyses
T-test and chi square analyses were used to analyze univariate demographic, wheelchair performance variables, and distance traveled measures by the wheelchair performance composite variable (median-split). Mixed model repeated measures analysis of variance was used to analyze changes in daily distance traveled across phases of the trial to address each of the five stated hypotheses.27 Mixed model analyses were chosen because of the intensive repeated measures design and statistical power within this framework, which depends on the frequency of observations and between- and within-person change variances28. Over the length of the trial, individuals reported their travel each day, which resulted in a potential of 112 data points per participant. Mixed model analyses have been shown to be more robust to missing data than standard general linear model approaches where subjects are excluded listwise. 25 In other words, because so many points were collected and all available data are used, this method provides better estimates when data points were missing (e.g., the participant forgets to enter the data). If we had only collected the cumulative distance per phase, and that data point were lost, we would have lost the entire participant data for further analyses. Model building steps included entering stepwise into the model (a) phase (baseline, intervention, and follow-up phases) to assess differences in distance traveled; (b) physical performance status (composite physical function score discussed previously) to assess differences in distance traveled, regardless of phase; and (c) interaction effects of physical functioning status by phase, to assess differential effects of PAW use by level of physical function. To investigate whether there was a learning curve or an adjustment period for wheelers when they transitioned into their wheelchairs equipped with PAWs, a second analysis was conducted using similar model building steps to examine differences in distance traveled within the intervention phase (weeks 1-2, weeks 3-4, weeks 5-6, weeks 7-8). Full-information maximum likelihood estimation was used as part of the SPSS 15.0 softwarec to accommodate missing data in the models. The significance level for all statistical analysis was set at p < .05.
Results
Descriptive Analyses
Compliance with the study protocol was robust. The percentage of missing data was 15.1% for the daily distance traveled, with no notable differences across the three phases of the trial. There were no missing data for the demographic and physical functioning variables. No potential participants were excluded on the basis of limited cognitive function that might have precluded cooperation with the study.
Sample characteristics and univariate analyses of all study variables are presented in Table 1 by wheelchair performance status (‘high’ vs. ‘low’) using a median split. As would be expected, higher performing participants were younger (M difference = 16.70 years), and traveled greater distances during each phase of the trial (M difference range = 2.13 to 2.77 m/s km/day) compared to low performing participants. These groups were similar in gender distribution and no comparisons for race/ethnicity were performed due to small cell sizes (both groups were primarily Caucasian). Because age was moderately correlated with the wheelchair performance composite (r = -.424, p = .063) and distance traveled during the baseline phase (r = -.476, p = .034), it was controlled for in all subsequent statistical models.
Table 1.
Demographic, wheelchair performance measures, and distance traveled measures presented by wheelchair performance composite variable split at the median (n=20).
| Characteristic | High functioning | Low functioning | Total sample | t | p |
|---|---|---|---|---|---|
| N | 10 | 10 | 20 | ||
| Age (y) | 34.70± 8.65 | 51.40± 14.71 | 43.05± 14.54 | 3.10 | 0.01 |
| Female gender | 40% | 30% | 35% | X2 = 0.64 | 0.50 |
| Physical performance measures | |||||
| Flat (m/s) | 1.26± 0.20 | 0.88± 0.18 | 1.07± 0.27 | -4.44 | <.001 |
| Carpet (m/s) | 1.12± 0.19 | 0.69± 0.20 | 0.90± 0.29 | -5.12 | <.001 |
| Ramp (m/s) | 0.99± 0.17 | 0.45± 0.18 | 0.72± 0.33 | -6.95 | <.001 |
| 40m test (m/s) | 1.99± 0.79 | 1.30± 0.51 | 1.64± 0.74 | -2.35 | 0.03 |
| Functional Composite | 1.79± 1.15 | -1.79± 1.33 | 0.00± 2.19 | -6.44 | <.001 |
| Distance traveled (km/day) | |||||
| Baseline phase | 2.66± 1.77 | 0.30± 0.24 | 1.48± 1.72 | -4.19 | 0.00 |
| Intervention phase | 3.42± 4.27 | 0.65± 0.54 | 2.04± 3.29 | -2.03 | 0.07 |
| Follow-up phase | 2.54± 2.41 | 0.41± 0.23 | 1.42± 1.95 | -2.63 | 0.03 |
NOTE. Values are M ± SD unless noted otherwise.
Finally, the primary outcome measure (daily distance traveled) was found to not be normally distributed. This variable was therefore log-transformed for subsequent multivariate analyses and back-transformed for interpretability.
Hypotheses 1 and 2: Distance Traveled
Our primary research question was whether participants traveled on average a greater distance during the intervention phase (with PAW wheels) compared to baseline and follow-up phases after controlling for age. Wheelchair performance was entered into the model as a continuous variable and main effect and interactions with phase were tested. After testing for fixed effects, random effects for time (i.e., random slopes) were entered into the model, however the model was unable to converge (likely due to the relatively small sample size). Therefore, Model 1 in Table 2 presents the final fixed effects estimates excluding any random effects. Participants traveled significantly greater distance during the intervention phase compared to both baseline (M difference = 0.76 km•day-1) and follow-up (M difference = 0.88 km•day-1) phases.
Table 2.
Fixed effects for age, intervention phase, and physical function predicting distance traveled and days exceeding distance threshold criterion.
| Beta estimate | SE | df | t | 95% CI | p | |
|---|---|---|---|---|---|---|
| Model 1. Distance Traveled | ||||||
| Age | -0.011 | 0.035 | 19.776 | -0.330 | -0.083 to 0.061 | 0.745 |
| Phase† | ||||||
| BL Phase | -0.382 | 0.145 | 2000.185 | -2.640 | -0.666 to -0.098 | 0.008 |
| FU Phase | -0.404 | 0.153 | 1999.918 | -2.635 | -0.704 to -0.103 | 0.008 |
| Function | 0.593 | 0.230 | 20.280 | 2.583 | 0.115 to 1.072 | 0.018 |
| Function * BL Phase | -0.023 | 0.065 | 1998.153 | -0.355 | -0.151 to 0.105 | 0.723 |
| Function * FU Phase | -0.082 | 0.072 | 2001.004 | -1.130 | -0.224 to 0.060 | 0.259 |
| Model 2. Distance threshold (2+SDs) | ||||||
| Age | 0.002 | 0.002 | 19.708 | 0.971 | -0.002 to 0.005 | 0.343 |
| Phase† | ||||||
| BL Phase | -0.102 | 0.016 | 2010.424 | -6.506 | -0.133 to -0.071 | < 0.001 |
| FU Phase | -0.070 | 0.017 | 2010.030 | -4.218 | -0.102 to -0.037 | < 0.001 |
| Function | -0.016 | 0.011 | 22.470 | -1.454 | -0.039 to 0.007 | 0.160 |
| Function * BL Phase | 0.019 | 0.007 | 2003.165 | 2.697 | 0.005 to 0.033 | 0.007 |
| Function * FU Phase | 0.025 | 0.008 | 2013.183 | 3.134 | 0.009 to 0.040 | 0.002 |
NOTE. BL = Baseline; FU = Follow-up.
Phases were compared to the intervention (PAW) phase.
The main effect for wheelchair performance was also significant, indicating participants with higher scores on the composite performance variable, travelled greater distances across all phases of the investigation To illustrate this point, high performing participants (using the median-split convention; n = 10) traveled, on average, 2.23 km•day-1 greater distance than low performing participants (n = 10). Wheelchair performance did not moderate the effect of the intervention on distance traveled across different phases of the investigation (baseline vs. intervention and intervention vs. follow-up). Figure 2 displays these trends graphically with physical functioning dichotomized at the median for ease of interpretation.
Figure 2.
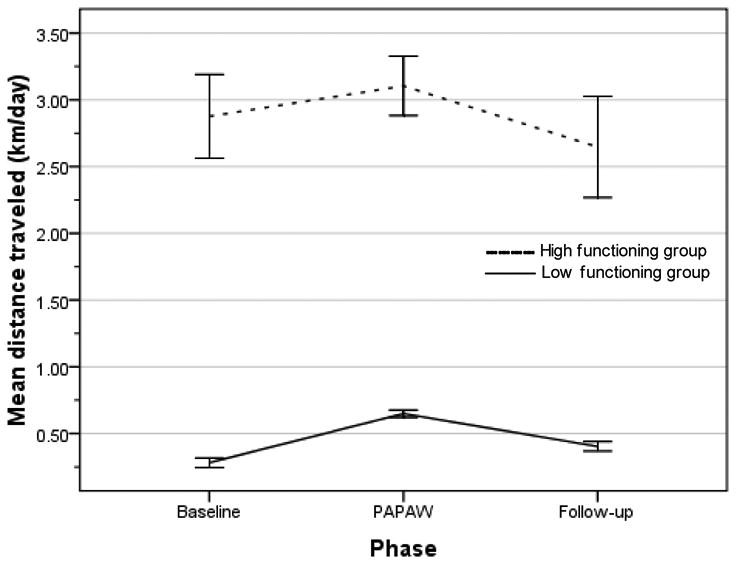
Mean distance traveled adjusted for age by phase for high and low performing groups. Note: Wheelchair performance is displayed here dichotomously (median split) to aid interpretation of the data.
Hypothesis 3: Differences in Distance Traveled Based Upon Hand-Function
The range for the sum of all four UPDRS tasks was 0-9. Seventy percent of the summed scores were 4 or less (an average score of ≤1 per task) which corresponds to no more than mild impairment. It was felt that this did not represent a meaningful clinical or statistical range. Additionally, better hand function was correlated with higher scores on the functional composite variable (r = -0.46, p < .05), indicating that variability in hand function was reasonably captured in the functional composite. Therefore, hand function was not used in subsequent analyses and the related hypothesis was not tested.
Hypothesis 4: Sub-Phase Differences in Distance Traveled During Paw Use
This analysis described the course of change in distance traveled through the intervention phase and addressed questions related to participant adjustment to the PAW wheels. The 8-week intervention phase was divided into four equal sub-phases (weeks 1-2, weeks 3-4, weeks 5-6, and weeks 7-8). Model building steps followed the same plan as in the previous analyses, controlling for age and exploring main effect and interactions for wheelchair performance. The final model revealed significant sub-phase differences in distance traveled (F(3,914.13) = 3.04, p = .03), with exploratory analyses revealing weeks 1-2 significantly lower than weeks 3-4 (M difference = 0.63 km•day-1, p = .03) and weeks 7-8 (M difference = 0.73 km•day-1, p = .01), and trending lower than weeks 5-6 (M difference = 0.45 km•day-1, p = .11). No other differences were observed between sub-phases. As observed in the previous model of distance traveled, the main effect for wheelchair performance was also significant (p = .03), indicating participants with greater performance, across all sub-phases, traveled greater distances.
Hypothesis 5: More functional wheelers will show the most difficulty adjusting
Finally, wheelchair performance also moderated sub-phase differences in distance traveled during weeks 1-2 only (beta estimate = -0.39, SE = 0.13, df = 914.51, t = -2.95, p = .003). The negative direction of this effect indicates that distance traveled was lower during weeks 1-2 compared with weeks 3-8 for those participants with higher wheelchair performance scores only. Participants of lower wheelchair performance traveled equal distances across all sub-phases of the intervention phase. Collectively these findings suggest an adjustment effect for the PAW wheels for those of higher wheelchair performance only, with no observable drop-off in distance traveled during the latter sub-phases of the intervention regardless of wheelchair performance.
Model 2: Secondary Post-Hoc Analyses
We encountered many anecdotal reports from participants indicating that PAW use did not uniformly impact distance traveled across all days; rather, during the intervention phase participants were able to opportunistically travel greater distance on select days. This led us to perform a set of secondary, posthoc analyses. Individual standard deviations (ISD) were calculated for each subject based upon normal distance traveled during the baseline phase. A distance threshold criterion of two ISDs above the participant's individual mean was set to represent days with “above-average” travel. The two ISD threshold was chosen as a strict criterion (p = .05) in order to minimize “chance” occasions of high distance travel. Daily distances were converted into a binary indicator (1 if participant met criterion, 0 otherwise) and this new variable was used as the dependent variable.
Model 2 in Table 2 shows that participants traveled significantly more days above the distance threshold in the intervention phase (14.7% of days) compared to both baseline (4.8% of days) and follow-up (7.7% of days) phases. The magnitude of this effect appeared greater than the raw distance traveled model presented previously. The main effect for wheelchair performance was not significant, indicating that participants of varying performance status, across all phases, were equally able to exceed the two ISD threshold. Wheelchair performance did, however, moderate phase differences in the distance threshold, such that lower performing participants displayed greater increase in the proportion of days above the distance threshold in the intervention phase compared to baseline and follow-up phases than higher performing subjects. To illustrate this point (using the median-split), lower performing participants exceeded the distance threshold on 16.1% and 11.1% more days during the intervention phase compared to the baseline and follow-up phases respectively, while higher performing participants exceeded the threshold only 5.8% and 3.3% more days respectively. Figure 3 displays this statistical interaction graphically.
Figure 3.
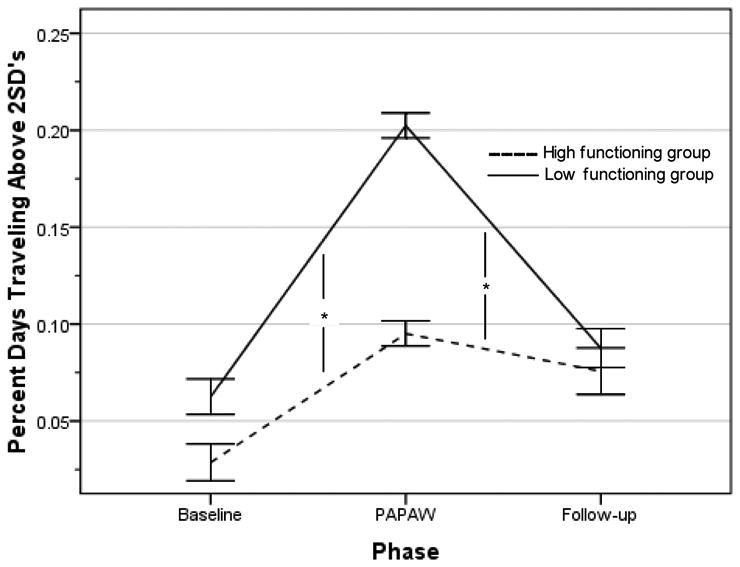
Percent days traveling above two baseline individual standard deviations by phase for high and low performing groups. *Interaction effects significant at p < .01. Note. Wheelchair performance is displayed here dichotomously (median split) to aid interpretation of the data.
Discussion
Wheelers in our study traveled significantly farther when they used wheelchairs equipped with PAWs than when they used their conventional manual wheelchairs. This was noted for both wheelers with higher and those with lower baseline wheelchair performance. Moreover, the increased distance wheeled by participants in PAWs was not so much realized on a daily basis, but occurred on selected days when opportunities to travel further presented themselves. This is consistent with the results of our qualitative interviews with this cohort14 where the majority of participants perceived positive experiences with the PAWs including access to new and different activities, and felt that PAWs provided more independence and social opportunities compared to their manual wheelchairs.
Our findings are somewhat at odds with those of Fitzgerald et al. and Ding et al.19, 20 Several differences in the experimental design may account for the discrepancy. The first is that their wheelers only had access to the PAPAWs for 2 weeks, a period that our more able wheelers appeared to be adjusting to the new technology. Second, in contrast to their wheelers, our participants had no choice but to adjust to the PAWs, since they did not have the option of continuing to use the manual wheels during our intervention phase. Although efforts were made to match the PAPAW with user's own manual chairs, there is a possibility that comfort or familiarity issues influenced users' choices in their cohorts. Finally, it is possible that differences between the Xtender PAPAW and the E.motion PAW played a role.
A limitation of this study is that there was not a direct measurement of participation or activity. Although the finding of increased distance traveled during the intervention phase suggest increased participation and activity, and is supported by the qualitative reports of our participants.21 Direct measurement that would quantify these effects would strengthen future studies. Although our sample size allowed meaningful within-person associations over time 28, between-person analyses regarding wheelchair performance should be interpreted with caution given the relatively small sample size.
Conclusions
Power assist wheels appear to have enabled wheelers to travel farther overall, and to travel beyond their usual distances on more days. This was particularly likely in those whose manual wheelchair performance was more greatly impaired. Future studies may be strengthened by considering the adjustment phase” for PAWs that occurs for at least some wheelers. The number of days travelled above a pre-determined threshold may be a more sensitive measure of PAW impact than distance measured over different phases of an experiment.
Acknowledgments
Funded by 1 R21 HDO46540-01A1 “The Impact of Power Assist Wheelchair on QOL”: NIH/National Institute of Child Health and Human Development.
Footnotes
Disclosures: Financial disclosure statements have been obtained, and no conflicts of interest have been reported by the authors or by any individuals in control of the content of this article.
SUPPLIER: The E.motion PAWs were built in Albstadt, Germany and distributed in the U.S. by Frank Mobility Systems, Inc, 1003 International Drive, Oakdale, PA 15071.
The last author was paid room and board (650.00) to present information about mixed-methods of inquiry for disability and rehabilitation researchers by Frank Mobility Systems. This was an invited conference hosted by the Rehabilitation Engineering Research Center (RERC), the National Institutes of Disability and Rehabilitation Research, and the Georgia Institute of Technology on September 17th, 2006.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Chow JW, Millikan TA, Carlton LG, Chae WS, Y L, Morse M. Kinematic and electromyographic analysis of wheelchair propulsion on ramps of different slopes for young men with paraplegia. Archives of Physical Medicine and Rehabilitation. 2009;90:271–8. doi: 10.1016/j.apmr.2008.07.019. [DOI] [PubMed] [Google Scholar]
- 2.Glaser RM, Barr SA, Lauback CC, et al. Relative stress of wheelchair activity. Human Factors. 1980;(22):177–81. doi: 10.1177/001872088002200206. [DOI] [PubMed] [Google Scholar]
- 3.Glaser RM, Sawka MN, Wilde SW, et al. Energy cost and cardiopulmonary responses for wheelchair locomotion and walking on tile and carpet. Paraplegia. 1981;19:220–6. doi: 10.1038/sc.1981.45. [DOI] [PubMed] [Google Scholar]
- 4.Waters RL, Lunsford BR. Energy cost of paraplegic locomotion. Journal of Bone & Joint Surgery in America. 1985;67:1245–50. [PubMed] [Google Scholar]
- 5.Bonninger ML, Koontz AM, Sisto SA, Dyson-Hudson TA, Chang M, Price R, et al. Pusrim biomechanics and injury prevention in spinal cord injury: Recommendations based on CULP-SCI investigations. Journal of Rehabilitation Research and Development. 2005;42 supplement:9–20. doi: 10.1682/jrrd.2004.08.0103. [DOI] [PubMed] [Google Scholar]
- 6.Cooper RA. Wheelchairs and related technology for the millennium. Journal of Rehabilitation Research and Development. 2000;37:xiii–xvi. [PubMed] [Google Scholar]
- 7.Cooper RA, Fitzgerald SG, Boninger ML, Prins K, Rentschler AJ, Arva J, et al. Evaluation of pushrim-activated power-assisted wheelchair. Archives of Physical Medicine and Rehabilitation. 2001;82:702–8. doi: 10.1053/apmr.2001.20836. [DOI] [PubMed] [Google Scholar]
- 8.Cooper RA, Quatrano LA, Axelson PW, Harlan W, Stineman M, Franklin B, et al. Research on physical activity and health among people with disabilities: A consensus statement. Journal of Rehabilitation Research and Development. 1999;36(2):142–54. [PubMed] [Google Scholar]
- 9.Gellman H, Chandler DR, Petrasek J, Sie I, Adkins R, Waters RL. Carpal tunnel syndrome in paraplegic patients. Journal of Bone & Joint Surgery in America. 1988;70:517–9. [PubMed] [Google Scholar]
- 10.Geisbrecht EM, Ripat JD, Quanbury AO, Cooper JE. Participation in community-based activities of daily living: COmparison of a pushrim-activated power-assisted wheelchair and a power wheelchair. Disability and Rehabiliation: Assistive technology. 2009;4:198–207. doi: 10.1080/17483100802543205. [DOI] [PubMed] [Google Scholar]
- 11.Levy CE, Chow JW, Tillman MD, Hanson C, Donohue T, Mann WC. Variable Ratio Power Assist Wheelchair Eases Wheeling Over a Variety of Terrains for Elders. Arch Phys Med Rehabil: Arch Phys Med Rehabil. 2004;85:104–12. doi: 10.1016/s0003-9993(03)00426-x. [DOI] [PubMed] [Google Scholar]
- 12.Levy CE, Chow JW. Pushrim-activated power assist wheelchairs: Elegance in motion. American Journal of Physical Medicine and Rehabilitation. 2001;83(2):166–7. doi: 10.1097/01.PHM.0000107500.89679.8E. [DOI] [PubMed] [Google Scholar]
- 13.Algood SD, Cooper RA, Fitzgerald SG, Cooper R, Bonninger ML. Impact of pushrim-activated power-assisted wheelchair on the metabolic demands, stroke frequency, and range of motion among subjects with tetraplegia. Archives of Physical Medicine and Rehabilitation. 2004;85:1865–71. doi: 10.1016/j.apmr.2004.04.043. [DOI] [PubMed] [Google Scholar]
- 14.Algood SD, Cooper RA, Fitzgerald SG, Cooper R, Bonninger ML. Effect of a pushrim-activated power-assist wheelchair on the functional capabilities of persons with tetraplegia. Archives of Physical Medicine and Rehabilitation. 2005;86(380-386) doi: 10.1016/j.apmr.2004.05.017. [DOI] [PubMed] [Google Scholar]
- 15.Arva J, SG F, RA C, ML B. Mechanical efficiency and user power requirement with a pushrim activated power assisted wheelchair. Medical Engineering and Physics. 2001;23(10):699–705. doi: 10.1016/s1350-4533(01)00054-6. [DOI] [PubMed] [Google Scholar]
- 16.Corfman TA, RA C, ML B, AM K, SG F. Range of motion and stroke frequency differences between manual wheelchair propulsion and pushrim-activated power-assisted wheelchair propulsion. Journal of Spinal Cord Medicine. 2003;26:135–40. doi: 10.1080/10790268.2003.11753673. [DOI] [PubMed] [Google Scholar]
- 17.Love JA, J B. Community use of a pushrim activated power-assisted wheelchair by an individual with facioscapulohumeral muscular dystrophy. Physiotherapy Theory and Practice. 2006;22:207–18. doi: 10.1080/09593980600822784. [DOI] [PubMed] [Google Scholar]
- 18.Nash MS, Koppens D, Hv M, S AL, L JP, L JE. Power-assisted wheels ease energy costs and perceptual responses to wheelchair propulsion in persons with shoulder pain and spinal cord injury. Archives of Physical Medicine and Rehabilitation. 2008;89:2080–5. doi: 10.1016/j.apmr.2008.05.018. [DOI] [PubMed] [Google Scholar]
- 19.Ding D, Souza A, Cooper RA, Fitzgerald SG, Cooper R, Kelleher A, et al. A preliminary study on the impact of pushrim-activated power-assist wheelchairs among individuals with tetraplegia. Journal of Physical Medicine and Rehabilitation. 2008;87:821–9. doi: 10.1097/PHM.0b013e318186bd1a. [DOI] [PubMed] [Google Scholar]
- 20.Fitzgerald SG, Arva J, Cooper RA, Dvorznak MJ, Spaeth DM, Bonninger ML. A pilot study of community usage of a pushrim-activated power assisted wheelchair. Assistive technology. 2003;15(2):113–9. doi: 10.1080/10400435.2003.10131895. [DOI] [PubMed] [Google Scholar]
- 21.Giacobbi PR, Jr, Levy CE, Dietrich FD, Hubbard-Winkler S, Tillman MD, Chow LC. Wheelchair users' perceptions of and experiences with power assist wheels. Am J Phys Med Rehabil. 2010;89:225–34. doi: 10.1097/PHM.0b013e3181c9d7df. [DOI] [PubMed] [Google Scholar]
- 22.Tolerica ML, Ding D, Cooper RA, Spaeth DM, Fitzgerald SG, Cooper R, Kelleher A, Boninger ML. Assessing mobility characteristics and activity levels of manual wheelchair users. Journal of Rehabilitation Research & Development. 2007;44(4):561–572. doi: 10.1682/jrrd.2006.02.0017. [DOI] [PubMed] [Google Scholar]
- 23.Sonenblum SE, Sprigle S, Harris FH, Maurer CL. Characterization of power wheelchair use in the home and community. Archives of Physical Medicine and Rehabilitation. 2008;89:486–491. doi: 10.1016/j.apmr.2007.09.029. [DOI] [PubMed] [Google Scholar]
- 24.Bussman JBJ, Kikkert MA, Sluis TAR, Bergen MP, Stam HJ, van den Berg-Emons HJG. Effect of wearing an activity monitor on the amount of daily manual wheelchair propulsion in persons with spinal cord injury. Spinal Cord. 2010;48(2):128–33. doi: 10.1038/sc.2009.72. [DOI] [PubMed] [Google Scholar]
- 25.Siderowf A. Test-retest reliability of the unified Parkinson's disease rating scale in patients with early Parkinson's disease: Results from a multicenter clinical trial. Movement Disorders. 2002;17(4):758–63. doi: 10.1002/mds.10011. [DOI] [PubMed] [Google Scholar]
- 26.Siderowf A, McDermott M, Kieburtz K, Blindauer K, Plumb S, Shoulson I. The unified Parkinson's disease rating scale (UPDRS): Status and recommendations. Movement Disorders. 2003;18(7):738–50. doi: 10.1002/mds.10473. [DOI] [PubMed] [Google Scholar]
- 27.Singer JB, Willett JB. Applied longitudinal data analysis: Modeling change and event occurence. New York: Oxford University Press; 2003. [Google Scholar]
- 28.Raudenbush SW, Xiao-Feng L. Effects of study duration, frequency of observation, and sample size on power in studies of group differences in polynomial change. Psychological Methods. 2001;6(4):387–401. [PubMed] [Google Scholar]