

Abstract
Patient: Male, 64
Final Diagnosis: Lung pleomorphic carcinoma
Symptoms: Cough • fever
Medication: —
Clinical Procedure: —
Specialty: Oncology
Objective:
Unusual clinical course
Background:
The diagnosis of lung cancer is often made based on computed tomography (CT) image findings if it cannot be confirmed on pathological examinations, such as bronchoscopy. However, the CT image findings of cancerous lesions are similar to those of abscesses.We herein report a case of lung cancer that resembled a lung abscess on CT.
Case Report:
We herein describe the case of 64-year-old male who was diagnosed with lung cancer using surgery. In this case, it was quite difficult to distinguish between the lung cancer and a lung abscess on CT images, and a lung abscess was initially suspected due to symptoms, such as fever and coughing, contrast-enhanced CT image findings showing a ring-enhancing mass in the right upper lobe and the patient’s laboratory test results. However, a pathological diagnosis of lung cancer was confirmed according to the results of a rapid frozen section biopsy of the lesion.
Conclusions:
This case suggests that physicians should not suspect both a lung abscesses and malignancy in cases involving masses presenting as ring-enhancing lesions on contrast-enhanced CT.
MeSH Keywords: Lung Neoplasms – etiology, Lung Neoplasms – radiography, Lung Neoplasms – surgery
Background
The diagnosis of lung cancer is often made based on computed tomography (CT) image findings if it cannot be confirmed on pathological examinations, such as bronchoscopy. However, the CT image findings of cancerous lesions are similar to those of abscesses.
We herein report a case of lung cancer that resembled a lung abscess on CT.
Case Report
A 64-year-old male, a current smoker with a wet cough and fever lasting for one week followed by the spontaneous resolution of symptoms, presented to the outpatient clinic for an evaluation of an abnormal shadow on a chest X-ray. The chest X-ray showed an area of consolidation in the apex of the right lung (Figure 1A). In addition, laboratory tests revealed an elevated CRP level(3.86 mg/L) and white blood cell count (8,980 ml), although the levels of serum tumor markers such as CEA, CYFLA, and ProGRP were within the normal range. Contrast-enhanced CT showed a low-density lesion with thick ring-enhanced irregular walls in the right upper lobe. The mass measured 53×43 mm, and had poorly defined margins. The interface between the lesion and surrounding organs was not clear. No gas collection or calcification was indicated. Enlarged lymph nodes were not detected in the mediastinum(Figure 1B). A PET/CT scan demonstrated a high uptake in the lesion, with a maximum SUV of 8.7, and the mediastinal lymph node, with a maximum SUV of 3.7, suspicious for both lung cancer and lung abscess formation (Figure 1C). An abscess was initially suspected based on the patient’s symptoms, CT image findings and laboratory test results. Both a transbronchial lung biopsy (TBLB) and CT-guided fine-needle biopsy of the lesion showed inflammatory cells compatible with active inflammation, No malignant cells were seen, and all bacterial cultures were negative.
Figure 1.
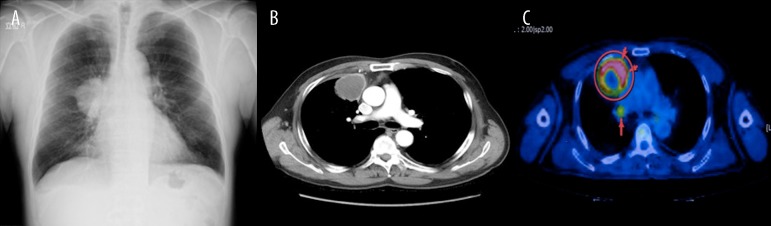
(A) An X-ray shows an abnormal shadow in the right upper lobe. (B) Chest CT with contrast enhancement shows a ring-enhancing solid mass measuring 53×43 mm in size in the right upper lobe with significant mediastinal lymphadenopathy. (C) A PET/CT scan reveals a high uptake in the mass, with a maximum SUV of 8.7, and the mediastional lymph node, with a maximum SUV of 3.7.
The patient was referred to our institution for management of the mass one month later. We suspected that the lesion indicated malignancy, as a follow-up CT scan showed an increase in the lesion in size to 59×49 mm (Figure 2) despite the absence of symptoms, such as fever. Therefore, we planned to perform surgery because there were no other signs of distant metastasis based on a CT scan of the chest, abdomen and pelvis, brain MRI and PET/CT.
Figure 2.

A follow-up CT scan shows an increase in the size of the mass 59×49 mm.
Based on the intraoperative findings, the right middle lobe was found to be involved with the mass in the upper lobe. A pathological diagnosis of lung cancer was confirmed according to the results of a rapid frozen section biopsy of the lesion. Consequently, we performed the right upper and middle lobectomy. There were no intraoperative complications, and the patient had an uneventful recovery. The final results of the pathologic examination showed a pleomorphic carcinoma of pT2N0M0, stage A.
Discussion
A lung abscess is defined as necrosis of the pulmonary tissue with the formation of cavities containing necrotic debris or fluid caused due to microbial infection. CT with contrast enhancement is the most sensitive and specific imaging modality for diagnosing lung abscesses. On CT images, abscesses often appear as round radiolucent lesions with a thick wall and ill-defined irregular margin.
Pleomorphic carcinoma of the lung, the final diagnosis in this case, is rare, accounting for 0.3% to 1% of all lung malignancies [1]. The prognosis of affected patients is generally poorer than that of patients with other types of non-small cell lung cancer [2]. Pleomorphic carcinoma was first classified as a carcinoma with pleomorphic, sarcomatoid, or sarcomatous elements by the World Health Organization in 1999, and in the 2003 Classification of Lung Cancers was defined as a poorly differentiated non-small cell carcinoma, which includes squamous cell carcinoma, adenocarcinoma and large cell carcinoma that contains spindle cells or giant cells, and cancers that contain at least 10% spindle cells or giant cell areas [3]. Therefore, the preoperative diagnosis of these tumors is very difficult, because pleomorphic carcinoma is a biphasic tumor [4].
According to Kim et al. [5], pleomorphic carcinoma frequently exhibits a central area of low attenuation with substantial enhancement in the tumor periphery on contrast material-enhanced CT scans, and low-attenuation areas on contrast-enhanced CT scans were found to correspond to areas of myxoid degeneration, necrosis or hemorrhage in pathological specimens. Therefore, in the present case, the CT image findings were similar to those of a lung abscess.
In general, the CT image findings of lung cancer can be similar to those of lung abscesses, as bronchial obstruction and vascular involvement with resulting ischemia can lead to tumor necrosis in cases of malignancy. In addition, FDG-PET shows accumulation resulting from both inflammatory changes and malignancy.
Therefore, it can be difficult to distinguish between lung cancer lesions and lung abscesses on CT in case in which the patient has no symptoms, including fever, and the diagnosis cannot be confirmed on pathological examinations, such as TBLB or CT-guided fine-needle biopsy.
In the present case, we suspected malignancy because follow-up CT revealed an increase in tumor in size despite the patient’s lack of symptoms suggestive of a lung abscess.
Conclusions
In conclusion, this case suggests that physicians should suspect both lung abscesses and malignancy in cases involving masses as presenting as ring-enhancing lesions on contrast-enhanced CT.
Footnotes
Conflict of interest statement
Naohiro Taira and the other co-authors have no conflicts of interest to declare.
Reference:
- 1.Rossi G, Cavazaa A, Sturm N, et al. Pulmonary carcinomas with pleomorphic, sarcomatoid, or sarcomatous element: a clinicopathologic and immunohistochemical study of 75 cases. Am J Surg Pathol. 2003;27:311–24. doi: 10.1097/00000478-200303000-00004. [DOI] [PubMed] [Google Scholar]
- 2.Mochizuki T, Ishii G, Nagai K, et al. Pleomorphic carcinoma of the lung: clinicopathologic characteristics of 70 cases. Am J Surg Pathol. 2008;32:1727–35. doi: 10.1097/PAS.0b013e3181804302. [DOI] [PubMed] [Google Scholar]
- 3.The Japan Lung Cancer Society . General rule for clini- cal and pathological record of lung cancer. 6th ed. Tokyo: Kanehara Shuppan; 2003. pp. 128–29. [in Japanese] [Google Scholar]
- 4.Kakegawa S, Kawashima O, Sugano M, et al. Pleomorphic lung cancer; a clinicopathologic study. Kyobu Geka. 2006;59(2):110–13. [in Japanese] [PubMed] [Google Scholar]
- 5.Kim TH, Kim SJ, Ryu YH, et al. Pleomorphic carcinoma of lung: comparison of CT features and pathologic findings. Radiology. 2004;232(2):554–59. doi: 10.1148/radiol.2322031201. [DOI] [PubMed] [Google Scholar]